
Association of Socioeconomic Factors and Physical Activity with Health-Related Quality of Life in Italian Middle School Children: An Exploratory Cross-Sectional Study

 ,
,  ,
,  , , ,
, , , 
Abstract
1. Introduction
Research Question and Purpose of the Study
2. Materials and Methods
2.1. Study Design and Participant
2.2. Instruments
2.3. Main Outcome Measure: Health-Related Quality of Life
2.4. Physical Activity Questionnaire for Older Children
2.5. Cardio-Fitness Performance Measurements
2.6. Socioeconomic Variables
2.7. Covariates
2.8. Data Analysis
3. Results
3.1. Study Population
3.2. Correlation Analysis
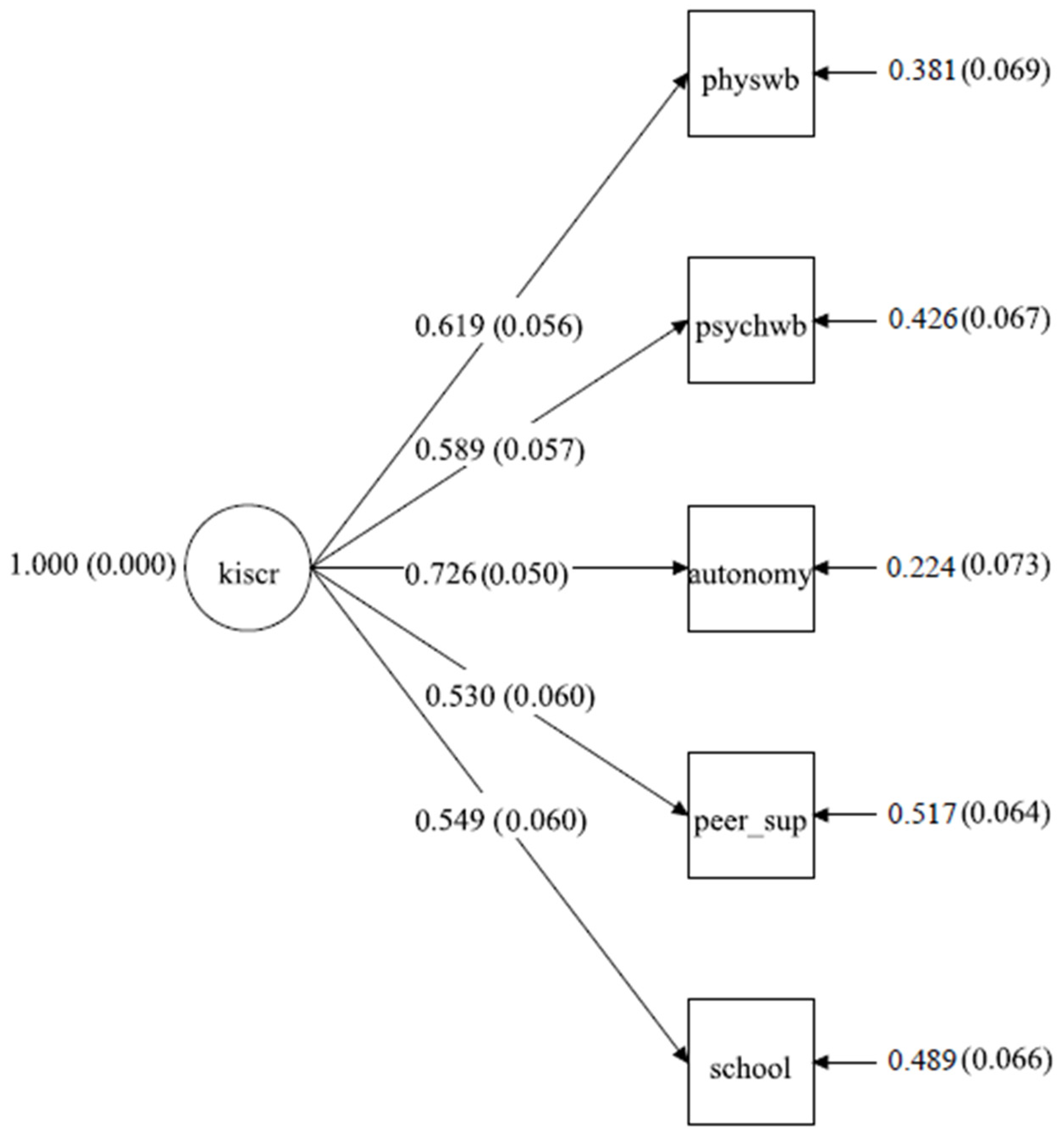
3.3. Path Model
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Whoqol Group. Development of the WHOQOL: Rationale and current status. Int. J. Ment. Health 1994, 23, 24–56. [Google Scholar] [CrossRef]
- Wang, H.; Shen, B.; Bo, J. Profiles of Health-related uality of lLife and their relationships with happiness, physical activity, and fitness. Res. Q. Exerc. Sport 2022, 93, 260–269. [Google Scholar] [CrossRef] [PubMed]
- Harding, L. Children’s quality of life assessments: A review of generic and health related quality of life measures completed by children and adolescents. Clin. Psychol. Psychother. 2001, 8, 79–96. [Google Scholar] [CrossRef]
- Spieth, L.E.; Harris, C.V. Assessment of health-related uality of life in children and adolescents: An integrative review. J. Pediatr. Psychol. 1996, 21, 175–193. [Google Scholar] [CrossRef]
- Petracci, E.; Cavrini, G. The effect of weight status, lifestyle, and body image perception on health-related quality of life in children: A quantile approach. Qual. Life Res. 2013, 22, 2607–2615. [Google Scholar] [CrossRef]
- Zhang, L.; Fos, P.J.; Johnson, W.D.; Kamali, V.; Cox, R.G.; A Zuniga, M.; Kittle, T. Body mass index and health related quality of life in elementary school children: A pilot study. Health Qual. Life Outcomes 2008, 6, 77. [Google Scholar] [CrossRef]
- Wang, J.; Jin, W.; Shi, L.; Geng, Y.; Zhu, X.; Hu, W. Health-related uality of life in children: The roles of age, gender and interpersonal trust. Int. J. Environ. Res. Public Health 2022, 19, 15408. [Google Scholar] [CrossRef]
- Sitaresmi, M.N.; Indraswari, B.W.; Rozanti, N.M.; Sabilatuttaqiyya, Z.; Wahab, A. Health-related quality of life profile of Indonesian children and its determinants: A community-based study. BMC Pediatr. 2022, 22, 103. [Google Scholar] [CrossRef]
- Ow, N.; Mayo, N.E. Health-related quality of life scores of typically developing children and adolescents around the world: A meta-analysis with meta-regression. Qual. Life Res. 2020, 29, 2311–2332. [Google Scholar] [CrossRef]
- Kalyva, E.; Malakonaki, E.; Eiser, C.; Mamoulakis, D. Health-related quality of life (HRQoL) of children with type 1 diabetes mellitus (T1DM): Self and parental perceptions. Pediatr. Diabetes 2011, 12, 34–40. [Google Scholar] [CrossRef]
- Rothmund, M.; Sodergren, S.; Rohde, G.; de Rojas, T.; Paratico, G.; Albini, G.; Mur, J.; Darlington, A.-S.; Majorana, A.; Riedl, D.; et al. Updating our understanding of health-related quality of life issues in children with cancer: A systematic review of patient-reported outcome measures and qualitative studies. Qual. Life Res. 2023, 32, 965–976. [Google Scholar] [CrossRef]
- Fardell, J.E.; Vetsch, J.; Trahair, T.; Mateos, M.K.; Grootenhuis, M.A.; Touyz, L.M.; Marshall, G.M.; Wakefield, C.E. Health-related quality of life of children on treatment for acute lymphoblastic leukemia: A systematic review. Pediatr. Blood Cancer 2017, 64, e26489. [Google Scholar] [CrossRef]
- Hubert-Dibon, G.; Bru, M.; Le Guen, C.G.; Launay, E.; Roy, A. Health-related quality of life for children and adolescents with specific language impairment: A cohort study by a learning disabilities reference center. PLoS ONE 2016, 11, e0166541. [Google Scholar] [CrossRef] [PubMed]
- Klassen, A.F.; Miller, A.; Fine, S. Health-related quality of life in children and adolescents who have a diagnosis of attention-deficit/hyperactivity disorder. Pediatrics 2004, 114, e541–e547. [Google Scholar] [CrossRef]
- Ravens-Sieberer, U.; Erhart, M.; Wille, N.; Bullinger, M.; BELLA study group. Health-related quality of life in children and adolescents in Germany: Results of the BELLA study. Eur. Child Adolesc. Psychiatry 2008, 17, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Ferrans, C.E.; Zerwic, J.J.; Wilbur, J.E.; Larson, J.L. Conceptual model of health-related quality of life. J. Nurs. Sch. 2005, 37, 336–342. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. The Ecology of human development: Experiments by nature and design; Harvard University Press: Cambridge, MA, USA, 1979. [Google Scholar]
- Wallander, J.L.; Schmitt, M.; Koot, H.M. Quality of life measurement in children and adolescents: Issues, instruments, and applications. J. Clin. Psychol. 2001, 57, 571–585. [Google Scholar] [CrossRef] [PubMed]
- Calzada-Rodríguez, J.I.; Denche-Zamorano, M.; Pérez-Gómez, J.; Mendoza-Muñoz, M.; Carlos-Vivas, J.; Barrios-Fernandez, S.; Adsuar, J.C. Health-related quality of life and frequency of physical activity in Spanish students Aged 8–14. Int. J. Environ. Res. Public Health 2021, 18, 9418. [Google Scholar] [CrossRef]
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar] [PubMed]
- Pascoe, M.; Bailey, A.P.; Craike, M.; Carter, T.; Patten, R.; Stepto, N.; Parker, A. Physical activity and exercise in youth mental health promotion: A scoping review. BMJ Open Sport Exerc. Med. 2020, 6, e000677. [Google Scholar] [CrossRef]
- Poitras, V.J.; Gray, C.E.; Borghese, M.M.; Carson, V.; Chaput, J.-P.; Janssen, I.; Katzmarzyk, P.T.; Pate, R.R.; Connor Gorber, S.; Kho, M.E.; et al. Systematic review of the relationships between objectively measured physical activity and health indicators in school-aged children and youth. Appl. Physiol. Nutr. Metab. 2016, 41, S197–S239. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Ayllon, M.; Cadenas-Sánchez, C.; Estévez-López, F.; Muñoz, N.E.; Mora-Gonzalez, J.; Migueles, J.H.; Molina-García, P.; Henriksson, H.; Mena-Molina, A.; Martínez-Vizcaíno, V.; et al. Role of physical activity and sedentary behavior in the mental health of preschoolers, children and adolescents: A systematic review and meta-analysis. Sports Med. 2019, 49, 1383–1410. [Google Scholar] [CrossRef] [PubMed]
- Biddle, S.J.; Ciaccioni, S.; Thomas, G.; Vergeer, I. Physical activity and mental health in children and adolescents: An updated review of reviews and an analysis of causality. Psychol. Sport Exerc. 2019, 42, 146–155. [Google Scholar] [CrossRef]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef]
- Kim, B.K.W.; Wallander, J.L.; Peskin, M.; Cuccaro, P.; Elliott, M.N.; A Schuster, M. Associations between parental SES and children’s health-related quality of life: The role of objective and subjective social status. J. Pediatr. Psychol. 2018, 43, 534–542. [Google Scholar] [CrossRef]
- von Rueden, U.; Gosch, A.; Rajmil, L.; Bisegger, C.; Ravens-Sieberer, U. Socioeconomic determinants of health related quality of life in childhood and adolescence: Results from a European study. J. Epidemiol. Community Health 2006, 60, 130–135. [Google Scholar] [CrossRef]
- Williams, J.; Wake, M.; Hesketh, K.; Maher, E.; Waters, E. Health-related quality of life of overweight and obese children. JAMA 2005, 293, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Keating, C.L.; Moodie, M.L.; Swinburn, B.A. The health-related quality of life of overweight and obese adolescents—A study measuring body mass index and adolescent-reported perceptions. Pediatr. Obes. 2011, 6, 434–441. [Google Scholar] [CrossRef]
- Costa, D.; Cunha, M.; Ferreira, C.; Gama, A.; Machado-Rodrigues, A.M.; Rosado-Marques, V.; Mendes, L.L.; Nogueira, H.; Pessoa, M.; Silva, M.G.; et al. Socioeconomic inequalities in children’s health-related quality of life according to weight status. Am. J. Hum. Biol. 2021, 33, e23453. [Google Scholar] [CrossRef]
- Drukker, M.; Kaplan, C.; Feron, F.; van Os, J. Children’s health-related quality of life, neighbourhood socio-economic deprivation and social capital. A contextual analysis. Soc. Sci. Med. 2003, 57, 825–841. [Google Scholar] [CrossRef]
- Marmot, M. The status syndrome: How social standing affects our health and longevity; Henry Holt and Company: New York, NY, USA, 2004. [Google Scholar]
- Masini, A.; Gori, D.; Marini, S.; Lanari, M.; Scrimaglia, S.; Esposito, F.; Campa, F.; Grigoletto, A.; Ceciliani, A.; Toselli, S.; et al. The determinants of health-related quality of life in a sample of primary school children: A cross-sectional analysis. Int. J. Environ. Res. Public Health 2021, 18, 3251. [Google Scholar] [CrossRef] [PubMed]
- Guevara, R.M.; Moral-García, J.E.; Urchaga, J.D.; López-García, S. Relevant factors in adolescent well-being: Family and parental relationships. Int. J. Environ. Res. Public Health 2021, 18, 7666. [Google Scholar] [CrossRef] [PubMed]
- Kowalski, K.C.; Crocker, P.R.; Faulkner, R.A. Validation of the physical activity questionnaire for older children. Pediatr. Exerc. Sci. 1997, 9, 174–186. [Google Scholar] [CrossRef]
- Ravens-Sieberer, U.; Auquier, P.; Erhart, M.; Gosch, A.; Rajmil, L.; Bruil, J.; Power, M.; Duer, W.; Cloetta, B.; Czemy, L.; et al. The KIDSCREEN-27 quality of life measure for children and adolescents: Psychometric results from a cross-cultural survey in 13 European countries. Qual. Life Res. 2007, 16, 1347–1356. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef]
- The KIDSCREEN Group Europe. The KIDSCREEN Questionnaires–Quality of Life Questionnaires for Children and Adolescents: Handbook; Pabst Science Publishers: Lengerich, Germany, 2006. [Google Scholar]
- McDonald, R.P. Theoretical foundations of principal factor analysis and alpha factor analysis. Br. J. Math. Stat. Psychol. 1970, 23, 1–21. [Google Scholar] [CrossRef]
- Crocker, P.R.E.; Bailey, D.A.; Faulkner, R.A.; Kowalski, K.C.; McGRATH, R. Measuring general levels of physical activity: Preliminary evidence for the Physical Activity Questionnaire for Older Children. Med. Sci. Sports Exerc. 1997, 29, 1344–1349. [Google Scholar] [CrossRef] [PubMed]
- Mannocci, A.; Masala, D.; Mei, D.; Tribuzio, A.M.; Villari, P.; LA Torre, G. International Physical Activity Questionnaire for Adolescents (IPAQ A): Reliability of an Italian version. Minerva Pediatr. 2021, 73, 383–390. [Google Scholar] [CrossRef]
- Gobbi, E.; Elliot, C.; Varnier, M.; Carraro, A. Psychometric properties of the physical activity questionnaire for older children in italy: Testing the validity among a general and clinical pediatric population. PLoS ONE 2016, 11, e0156354. [Google Scholar] [CrossRef]
- Ayán, C.; Cancela, J.M.; Romero, S.; Alonso, S. Reliability of two field-based tests for measuring cardiorespiratory fitness in preschool children. J. Strength Cond. Res. 2015, 29, 2874–2880. [Google Scholar] [CrossRef]
- Bolonchuk, W.W. The accuracy of the six minute run test to measure cardiorespiratory fitness; North Dakota University: Grand Forks, ND, USA, 1975. [Google Scholar]
- Čillík, I.; Kollár, R.; Kremnický, J.; Pivovarniček, P.; Mandzáková, M. The level of general physical performance and physical development of 7 and 10-year-old boys and girls. J. Hum. Sport Exerc. 2015, 10, S259–S268. [Google Scholar] [CrossRef]
- Secchi, J.D.; García, G.C.; España-Romero, V.; Castro-Piñero, J. Physical fitness and future cardiovascular risk in Argentine children and adolescents: An introduction to the ALPHA test battery. Arch. Argent. Pediatr. 2014, 112, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Castro-Piñero, J.; Ortega, F.B.; Artero, E.G.; Girela-Rejón, M.J.; Mora, J.; Sjöström, M.; Ruiz, J.R. Assessing muscular strength in youth: Usefulness of standing long jump as a general index of muscular fitness. J. Strength Cond. Res. 2010, 24, 1810–1817. [Google Scholar] [CrossRef]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjöström, M. Physical fitness in childhood and adolescence: A powerful marker of health. Int. J. Obes. 2008, 32, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Blair, S.N.; Cheng, Y.; Holder, J.S. Is physical activity or physical fitness more important in defining health benefits? Med. Sci. Sports Exerc. 2001, 33 (Suppl. S6), S379–S399. [Google Scholar] [CrossRef] [PubMed]
- Katzmarzyk, P.T.; Malina, R.M.; Bouchard, C. Physical activity, physical fitness, and coronary heart disease risk factors in youth: The Québec Family Study. Prev. Med. 1999, 29 Pt 1, 555–562. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- R Core Team. R: A language and environment for statistical computing; R Foundation for Statistical Computing: Vienna, Austria, 2022; Available online: https://www.r-project.org/ (accessed on 10 June 2023).
- Muthén, L.K.; Muthén, B.O. Mplus Users’ Guide, 8th ed.; Muthén & Muthén: Los Angeles, CA, USA, 1998–2017. [Google Scholar]
- Steiger, J.H.; Lind, J.C. Statistically-based tests for the number of common factors. In Proceedings of the Meeting of the Psychometric Society, Iowa City, IA, USA, 27–29 May1980. [Google Scholar]
- Taasoobshirazi, G.; Wang, S. The performance of the SRMR, RMSEA, CFI, and TLI: An examination of sample size, path size, and degrees of freedom. J. Appl. Quant. Methods 2016, 11, 31–39. [Google Scholar]
- Kenny, D.A.; Kaniskan, B.; McCoach, D.B. The performance of RMSEA in models with small degrees of freedom. Sociol. Methods Res. 2015, 44, 486–507. [Google Scholar] [CrossRef]
- MacCallum, R.C.; Browne, M.W.; Sugawara, H.M. Power analysis and determination of sample size for covariance structure modeling. Psychol. Methods 1996, 1, 130–149. [Google Scholar] [CrossRef]
- Gaspar, T.; Ribeiro, J.P.; De Matos, M.G.; Leal, I.; Ferreira, A. Health-related quality of life in children and adolescents: Subjective well being. Span. J. Psychol. 2012, 15, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Wallander, J.L.; Fradkin, C.; Chien, A.T.; Mrug, S.; Banspach, S.W.; Davies, S.; Elliott, M.N.; Franzini, L.; Schuster, M.A. Racial/ethnic disparities in health-related quality of life and health in children are largely mediated by family contextual differences. Acad. Pediatr. 2012, 12, 532–538. [Google Scholar] [CrossRef] [PubMed]
- Berchick, E.R. The relationship between maternal education and reported childhood conditions. Soc. Sci. Med. 2016, 170, 170–179. [Google Scholar] [CrossRef]
- Bicego, G.T.; Boerma, J.T. Maternal education and child survival: A comparative study of survey data from 17 countries. Soc. Sci. Med. 1993, 36, 1207–1227. [Google Scholar] [CrossRef] [PubMed]
- Hallal, P.C.; Victora, C.G.; Azevedo, M.R.; Wells, J.C.K. Adolescent physical activity and health: A systematic review. Sports Med. 2006, 36, 1019–1030. [Google Scholar] [CrossRef] [PubMed]
- Esteban-Cornejo, I.; Hallal, P.C.; Mielke, G.I.; Menezes, A.M.B.; Gonçalves, H.; Wehrmeister, F.; Ekelund, U.; Rombaldi, A.J. Physical activity throughout adolescence and cognitive performance at 18 years of age. Med. Sci. Sports Exerc. 2015, 47, 2552–2557. [Google Scholar] [CrossRef]
- Eime, R.M.; Young, J.A.; Harvey, J.T.; Charity, M.J.; Payne, W.R. A systematic review of the psychological and social benefits of participation in sport for children and adolescents: Informing development of a conceptual model of health through sport. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 98. [Google Scholar] [CrossRef]
- Longmuir, P.E.; Colley, R.C.; Wherley, V.A.; Tremblay, M.S. Canadian Society for Exercise Physiology position stand: Benefit and risk for promoting childhood physical activity. Appl. Physiol. Nutr. Metab. 2014, 39, 1271–1279. [Google Scholar] [CrossRef]
- Anderson, E.; Durstine, J.L. Physical activity, exercise, and chronic diseases: A brief review. Sports Med. Health Sci. 2019, 1, 3–10. [Google Scholar] [CrossRef]
- Masini, A.; Marini, S.; Gori, D.; Leoni, E.; Rochira, A.; Dallolio, L. Evaluation of school-based interventions of active breaks in primary schools: A systematic review and meta-analysis. J. Sci. Med. Sport 2020, 23, 377–384. [Google Scholar] [CrossRef]
- Watson, A.; Timperio, A.; Brown, H.; Best, K.; Hesketh, K.D. Effect of classroom-based physical activity interventions on academic and physical activity outcomes: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 114. [Google Scholar] [CrossRef]
- E Neil-Sztramko, S.; Caldwell, H.; Dobbins, M. School-based physical activity programs for promoting physical activity and fitness in children and adolescents aged 6 to 18. Cochrane Database Syst. Rev. 2021, 2021, CD007651. [Google Scholar] [CrossRef]
- Álvarez-Bueno, C.; Pesce, C.; Cavero-Redondo, I.; Sánchez-López, M.; Martínez-Hortelano, J.A.; Martínez-Vizcaíno, V. The Effect of Physical Activity Interventions on Children’s Cognition and Metacognition: A Systematic Review and Meta-Analysis. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 729–738. [Google Scholar] [CrossRef]
- Ardoy, D.N.; Fernández-Rodríguez, J.M.; Jiménez-Pavón, D.; Castillo, R.; Ruiz, J.R.; Ortega, F.B. A Physical Education trial improves adolescents’ cognitive performance and academic achievement: The EDUFIT study. Scand. J. Med. Sci. Sports 2014, 24, e52–e61. [Google Scholar] [CrossRef] [PubMed]
- Kvalø, S.E.; Bru, E.; Brønnick, K.; Dyrstad, S.M. Does increased physical activity in school affect children’s executive function and aerobic fitness? Scand. J. Med. Sci. Sports 2017, 27, 1833–1841. [Google Scholar] [CrossRef] [PubMed]
- Infantes-Paniagua, Á.; Silva, A.F.; Ramirez-Campillo, R.; Sarmento, H.; González-Fernández, F.T.; González-Víllora, S.; Clemente, F.M. Active school breaks and students’ attention: A systematic review with meta-analysis. Brain Sci. 2021, 11, 675. [Google Scholar] [CrossRef]
- Dallolio, L.; Gallè, F.; Masini, A.; Valeriani, F.; Ceciliani, A.; di Cagno, A.; Galeone, D.; Pecoraro, P.; Valerio, G.; Liguori, G.; et al. Active breaks: A strategy to counteract sedentary behaviors for health promoting schools: A discussion on their implementation in Italy. Ann. Ig. 2023, 35, 202–212. [Google Scholar] [CrossRef]
- MacCallum, R. Specification searches in covariance structure modeling. Psychol. Bull. 1986, 100, 107–120. [Google Scholar] [CrossRef]


{kind=link}
| Population Characteristics | Overall, n= 370 | Females, n = 182 | Males, n = 188 | p-Value 3 |
|---|---|---|---|---|
| Age (years, mean ± SD) | 12.76 ± 0.94 | 12.89 ± 0.91 | 12.63 ± 0.95 | 0.009 |
| IOTF category | 0.725 | |||
| Underweight/Normal weight | 170 (76%) | 98 (77%) | 72 (74%) | |
| Overweight/Obese | 54 (24%) | 29 (23%) | 25 (26%) | |
| Missing | 146 | 55 | 91 | |
| Live with both parents | 0.512 | |||
| No | 28 (13%) | 18 (14%) | 10 (10%) | |
| Yes | 194 (87%) | 108 (86%) | 86 (90%) | |
| Missing | 146 | 56 | 92 | |
| Nationality | 0.07 | |||
| Italian | 186 (83%) | 111 (87%) | 75 (77%) | |
| Other | 38 (17%) | 16 (13%) | 22 (23%) | |
| Missing | 146 | 55 | 91 | |
| Mother citizenship | 0.181 | |||
| Italian | 179 (81%) | 106 (84%) | 73 (76%) | |
| Other | 43 (19%) | 20 (16%) | 23 (24%) | |
| Missing | 146 | 56 | 92 | |
| Father citizenship | 0.7 | |||
| Italian | 193 (87%) | 111 (88%) | 82 (85%) | |
| Other | 29 (13%) | 15 (12%) | 14 (15%) | |
| Missing | 146 | 56 | 92 | |
| Parents citizenship | 0.228 | |||
| Both Italians | 173 (78%) | 103 (82%) | 70 (73%) | |
| One Italian-One other | 26 (12%) | 11 (8.7%) | 15 (16%) | |
| Both other | 23 (10%) | 12 (9.5%) | 11 (11%) | |
| Missing | 146 | 56 | 92 | |
| Parents citizenship dichotomic | 0.159 | |||
| Both Italians | 173 (78%) | 103 (82%) | 70 (73%) | |
| Other | 49 (22%) | 23 (18%) | 26 (27%) | |
| Missing | 146 | 56 | 92 | |
| Mother educational level | 0.651 | |||
| Middle school or lower | 44 (20%) | 26 (21%) | 18 (19%) | |
| High school | 109 (49%) | 64 (51%) | 45 (47%) | |
| University degree or higher | 69 (31%) | 36 (29%) | 33 (34%) | |
| Missing | 146 | 56 | 92 | |
| Father educational level | 0.442 | |||
| Middle school or lower | 60 (27%) | 35 (28%) | 25 (26%) | |
| High school | 111 (50%) | 66 (52%) | 45 (47%) | |
| University degree or higher | 51 (23%) | 25 (20%) | 26 (27%) | |
| Missing | 146 | 56 | 92 | |
| Parents highest educational level | 0.651 | |||
| Middle school or lower | 39 (18%) | 23 (18%) | 16 (17%) | |
| High school | 114 (51%) | 67 (53%) | 47 (49%) | |
| University degree or higher | 69 (31%) | 36 (29%) | 33 (34%) | |
| Missing | 148 | 56 | 92 | |
| Mother employed | >0.999 | |||
| Yes | 34 (15%) | 19 (15%) | 15 (16%) | |
| No | 188 (85%) | 107 (85%) | 81 (84%) | |
| Missing | 146 | 56 | 92 | |
| Mother employment status | 0.105 | |||
| Unemployed | 34 (15%) | 19 (15%) | 15 (16%) | |
| Part time | 70 (32%) | 47 (37%) | 23 (24%) | |
| Full time | 117 (53%) | 60 (48%) | 57 (60%) | |
| Missing | 146 | 56 | 93 | |
| Father employed | >0.999 | |||
| Yes | 5 (2.3%) | 3 (2.4%) | 2 (2.1%) | |
| No | 217 (98%) | 123 (98%) | 94 (98%) | |
| Missing | 148 | 56 | 92 | |
| Family working status | 0.981 | |||
| One employed or less | 38 (17%) | 21 (17%) | 17 (18%) | |
| Both employed | 184 (83%) | 105 (83%) | 79 (82%) | |
| Missing | 148 | 56 | 92 | |
| Physical Well-Being (5) 1 | 18.51 ± 3.38 | 18.02 ± 3.46 | 19.16 ± 3.19 | 0.013 |
| Missing | 146 | 56 | 92 | |
| Psychological Well-Being (7) | 27.66 ± 4.25 | 26.65 ± 4.47 | 28.94 ± 3.58 | <0.001 |
| Missing | 146 | 61 | 93 | |
| Parents and Autonomy (7) | 28.09 ± 4.59 | 27.33 ± 4.92 | 29.07 ± 3.93 | 0.005 |
| Missing | 146 | 56 | 92 | |
| Social Support and Peers (4) | 16.73 ± 2.59 | 16.64 ± 2.58 | 16.85 ± 2.60 | 0.548 |
| Missing | 146 | 56 | 92 | |
| School Environment (4) | 14.27 ± 2.30 | 14.34 ± 2.20 | 14.19 ± 2.42 | 0.622 |
| Missing | 146 | 56 | 92 | |
| KIDSCREEN 27 total score | 105.79 ± 12.20 | 103.77 ± 12.38 | 108.37 ± 11.53 | 0.006 |
| Missing | 146 | 61 | 93 | |
| Long jump (cm) 2 | 154.22 ± 33.08 | 144.13 ± 30.69 | 164.18 ± 32.43 | <0.001 |
| Missing | 67 | 42 | 46 | |
| Shuttle run (s) 2 | 12.13 ± 1.54 | 12.51 ± 1.38 | 11.77 ± 1.59 | <0.001 |
| Missing | 96 | 49 | 47 | |
| 6 min Cooper test (m) 2 | 1807.28 ± 378.68 | 1645.75 ± 313.79 | 1977.64 ± 367.35 | <0.001 |
| Missing | 105 | 47 | 60 | |
| PAQ-A score | 2.25 ± 0.62 | 2.08 ± 0.58 | 2.48 ± 0.58 | <0.001 |
| Missing | 146 | 56 | 92 |
| Variable | Physical WB | Psych WB | Parents and Autonomy | Social Support and Peers | School Env. | KIDSCR. 27 | PAQ-A Score | Long Jump | Shuttle Run | Cooper Test | Age |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Physical WB | - | 0.481 | 0.435 | 0.362 | 0.358 | 0.714 | 0.579 | 0.352 | −0.408 | 0.361 | −0.116 |
| Psychological WB | - | 0.536 | 0.349 | 0.453 | 0.824 | 0.141 | 0.181 | −0.095 | 0.169 | −0.210 | |
| Parents and Autonomy | - | 0.422 | 0.375 | 0.805 | 0.206 | 0.073 | −0.162 | 0.112 | −0.070 | ||
| Social Support and Peers | - | 0.256 | 0.595 | 0.189 | 0.119 | −0.073 | 0.146 | −0.074 | |||
| School Environment | - | 0.606 | 0.075 | −0.029 | −0.092 | 0.082 | −0.163 | ||||
| KIDSCREEN 27 | - | 0.313 | 0.192 | −0.200 | 0.230 | −0.158 | |||||
| PAQ-A score | - | 0.263 | −0.349 | 0.339 | −0.092 | ||||||
| Long jump | - | −0.727 | 0.496 | 0.144 | |||||||
| Shuttle run | - | −0.569 | −0.062 | ||||||||
| Cooper test | - | −0.022 | |||||||||
| Age | - |
| Structural Path Coefficients | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Univariate Model 1 | Multivariate Model | Fully Adjusted Model 3 | |||||||
| Measure | b | p-Value | 95% CI | b | p-Value | 95% CI | b | p-Value | 95% CI |
| Covariates | |||||||||
| Age | −0.136 | 0.064 | −0.280–0.008 | −0.139 | 0.020 | −0.254–−0.023 | −0.136 | 0.019 | −0.250–−0.023 |
| Nationality | −0.058 | 0.477 | −0.220–0.103 | – 2 | - | - | - | ||
| Sex | −0.204 | 0.005 | −0.346–−0.062 | 0.142 | 0.017 | 0.011–0.273 | 0.140 | 0.015 | 0.017–0.263 |
| Living situation | 0.164 | 0.023 | 0.023–0.305 | – 2 | - | - | - | ||
| Parents’ employment status | 0.235 | 0.002 | 0.087–0.384 | 0.145 | 0.036 | 0.031–0.259 | 0.142 | 0.013 | 0.027–0.257 |
| Parents’ educational status | 0.032 | 0.658 | −0.111–0.176 | 0.135 | 0.039 | 0.023–0.248 | 0.133 | 0.017 | 0.022–0.244 |
| Parents’ citizenry (immigration status) | −0.043 | 0.616 | −0.212–0.126 | – 2 | - | - | - | - | |
| Cardio-Fitness and Physical Activity Measures | |||||||||
| PAQ-C (PA) | 0.418 | <0.001 | 0.257–0.579 | 0.429 | <0.001 | 0.304–0.554 | 0.421 | <0.001 | 0.300–0.542 |
| Cooper Test (speed) | 0.184 | 0.017 | 0.033–0.336 | 0.221 | 0.018 | 0.087–0.355 | 0.218 | 0.001 | 0.089–0.346 |
| Long jump | 0.011 | 0.919 | −0.199–0.221 | – 2 | - | – 2 | - | ||
| Shuttle run (agility) | −0.186 | 0.048 | −0.371–−0.001 | −0.207 | 0.044 | −0.337–−0.077 | −0.203 | 0.002 | −0.329–−0.077 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanmarchi, F.; Scheier, L.M.; Dallolio, L.; Ricci, M.; Longo, G.; Ceciliani, A.; Masini, A. Association of Socioeconomic Factors and Physical Activity with Health-Related Quality of Life in Italian Middle School Children: An Exploratory Cross-Sectional Study. Healthcare 2023, 11, 2092. https://doi.org/10.3390/healthcare11142092
Sanmarchi F, Scheier LM, Dallolio L, Ricci M, Longo G, Ceciliani A, Masini A. Association of Socioeconomic Factors and Physical Activity with Health-Related Quality of Life in Italian Middle School Children: An Exploratory Cross-Sectional Study. Healthcare. 2023; 11(14):2092. https://doi.org/10.3390/healthcare11142092
Chicago/Turabian StyleSanmarchi, Francesco, Lawrence M. Scheier, Laura Dallolio, Matteo Ricci, Giulia Longo, Andrea Ceciliani, and Alice Masini. 2023. "Association of Socioeconomic Factors and Physical Activity with Health-Related Quality of Life in Italian Middle School Children: An Exploratory Cross-Sectional Study" Healthcare 11, no. 14: 2092. https://doi.org/10.3390/healthcare11142092
APA StyleSanmarchi, F., Scheier, L. M., Dallolio, L., Ricci, M., Longo, G., Ceciliani, A., & Masini, A. (2023). Association of Socioeconomic Factors and Physical Activity with Health-Related Quality of Life in Italian Middle School Children: An Exploratory Cross-Sectional Study. Healthcare, 11(14), 2092. https://doi.org/10.3390/healthcare11142092