

Identifying the Drivers of Inter-Regional Patients’ Mobility: An Analysis on Hospital Beds Endowment



Abstract
1. Introduction
2. Materials and Methods
2.1. Admissions, Beds Endowment, Population Data and Catchment Area
2.2. Gandy’s Nomogram
- ₋
- The upper-left quadrant describes the catchment areas “marked oriented”, in which are admitted more patients attracted than residents and escapes are less than attractions and residents admission (E < R < A). At the point X = 0 and Y = 100 is shown the paradoxical condition in which are admitted only attracted patients and there are no escapes.
- ₋
- The upper-right quadrant describes the catchment areas which can meet the care needs of their residents on site. In the part above the bisector, named “hemi-quadrant of quality), attractions are more than escapes and the latter less than residents’ admissions (E < A < R). In the part under the bisector, escapes are more than attractions and the latter are less than residents’ admissions.
- ₋
- The lower-left quadrant describes the catchment areas in which the residents’ admissions are less than both escapes and attractions. In the part above the bisector, escapes are less than attractions (R < E < A), while in the part under the bisector is shown the opposite situation (A < R < E).
- ₋
- The lower-right quadrant describes the catchment areas in which the residents’ admissions are less than escapes but greater than attractions (A < R < E).
2.3. Attraction and Escape Indexes
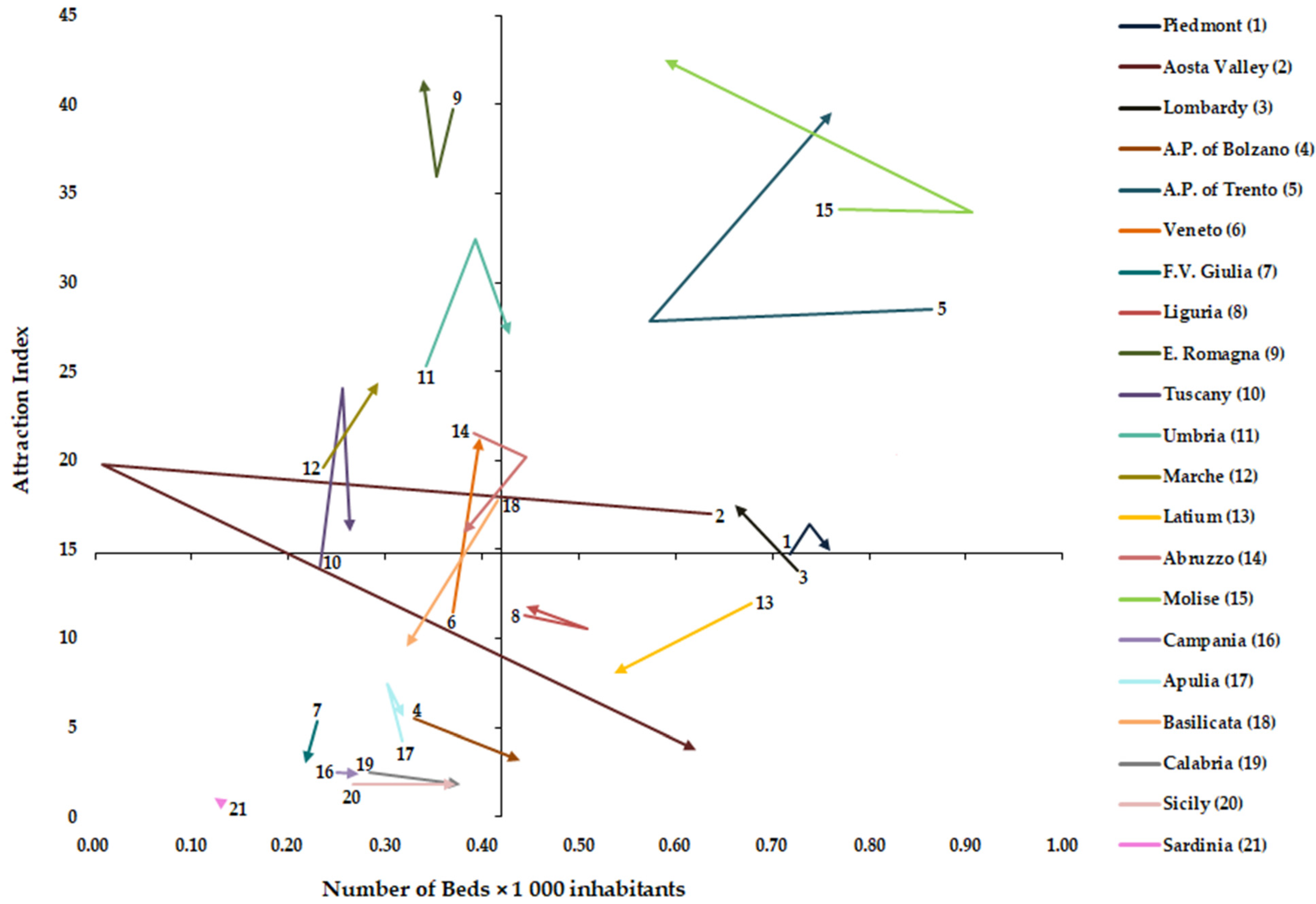
2.4. Graphical Representation of AI, EI and NB × 1000 Inhabitants
2.5. Vectorial and Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ricci, A.; Barzan, E.; Longo, F. How to identify the drivers of patient inter-regional mobility in beveridgean systems? Critical review and assessment matrix for policy design & managerial interventions. Health Serv. Manag. Res. 2021, 34, 258–268. [Google Scholar]
- Lunt, N.; Mannion, R. Patient mobility in the global marketplace. A multidisciplinary perspective. Int. J. Health Policy Manag. 2014, 2, 155–157. [Google Scholar] [CrossRef] [PubMed]
- Horsfall, D. Medical tourism from the UK to Poland: How the market masks migration. J. Ethn. Migr. Stud. 2019, 46, 4211–4229. [Google Scholar] [CrossRef]
- Perna, R.; Cruz-Martínez, G.; Moreno Fuentes, F.J. Patient mobility within national borders. Drivers and politics of cross-border healthcare agreements in the Spanish decentralized system. Health Policy 2022, 126, 1187–1193. [Google Scholar] [CrossRef]
- Yang, Y.; Wang, Y. Analysis of the charateristics of Cross-Regional Patient Group and Differences in Hospital Service Utilization in Beijin. Int. J. Environ. Res. Public Health 2022, 19, 3227. [Google Scholar] [CrossRef]
- Diesenreiter, C.; Österle, A. Patients as EU citizens? The implementation and corporatist stakeholders’ perceptions of the EU cross-border health care directive in Austria. Health Policy 2021, 125, 1498–1505. [Google Scholar] [CrossRef]
- Pecoraro, F.; Luzi, D.; Clemente, F. The Impact of Hospital Accessibility on Interregional Patient Mobility in Italy. Stud. Health Technol. Inform. 2022, 294, 684–688. [Google Scholar]
- Rotulo, A.; Paraskevopoulou, C.; Kondilis, E. The Effects of Health Sector Fiscal Decentralisation on Availability, Accessibility, and Utilisation of Healthcare Services: A Panel Data Analysis. Int. J. Health Policy Manag. 2021, 11, 2440–2450. [Google Scholar] [CrossRef]
- Nante, N.; Guarducci, G.; Lorenzini, C.; Messina, G.; Carle, F.; Carbone, S.; Urbani, A. Inter-Regional Hospital Patients’ Mobility in Italy. Healthcare 2021, 9, 1182. [Google Scholar] [CrossRef]
- Fattore, G.; Petrarca, G.; Torbica, A. Traveling for care: Inter-regional mobility for aortic valve substitution in Italy. Health Policy 2014, 117, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, A.; Lewis, D.; Mason, M.; Sullivan, R.; Van Der Meulen, J. Patient Mobility for Elective Secondary Health Care Services in Response to Patient Choice Policies: A Systematic Review. Med. Care Res. Rev. 2016, 74, 379–403. [Google Scholar] [CrossRef] [PubMed]
- Lega, F.; Sargiacomo, M.; Ianni, L. The rise of governmentality in the Italian National Health System: Physiology or pathology of a decentralized and (ongoing) federalist system? Health Serv. Manag. Res. 2010, 23, 172–180. [Google Scholar] [CrossRef]
- Nante, N.; Messina, G.; Lispi, L.; Serafini, A.; Prisco, G.; Moirano, F. Mobility trends of Patients across Italian Regions: Implications for planning and evaluation of hospital services. Ann. Ig. 2016, 28, 328–338. [Google Scholar]
- Brenna, E.; Spandonaro, F. Regional incentives and patient cross-border mobility: Evidence from the Italian experience. Int. J. Health Policy Manag. 2015, 4, 363–372. [Google Scholar] [CrossRef] [PubMed]
- Balia, S.; Brau, R.; Moro, D. Choice of hospital and long-distances: Evidence from Italy. Reg. Sci. Urban Econ. 2020, 81, 103502. [Google Scholar] [CrossRef]
- Levaggi, R.; Zanola, R. Patients’ migration across regions: The case of Italy. Appl. Econ. 2004, 36, 1751–1757. [Google Scholar] [CrossRef]
- Ferré, F.; Seghieri, C.; Nuti, S. Women’s choices of hospital for breast cancer surgery in Italy: Quality and equity implications. Health Policy 2023, 131, 104781. [Google Scholar] [CrossRef]
- Pecoraro, F.; Accordino, F.; Cecconi, F.; Paolucci, M. Agent Based Modelling for Simulating the Interregional Patient Mobility in Italy. Stud. Health Technol. Inform. 2023, 302, 297–301. [Google Scholar]
- Rubino, C.; Di Maria, C.; Abbruzzo, A.; Ferrante, M. Socio-economic inequality, interregional mobility and mortality among cancer patients: A mediation analysis approach. Socio-Econ. Plan. Sci. 2022, 82, 101247. [Google Scholar] [CrossRef]
- Beukers, P.D.C.; Kemp, R.G.M.; Varkevisser, M. Patient hospital choice for hip replacement: Empirical evidence from the Netherlands. Eur. J. Health Econ. 2013, 15, 927–936. [Google Scholar] [CrossRef]
- Ruwaard, S.; Douven, R.C.M.H. Hospital Choice for Cataract Treatments: The Winner Takes Most. Int. J. Health Policy Manag. 2018, 7, 1120–1129. [Google Scholar] [CrossRef] [PubMed]
- Nante, N.; Ricchiardi, G.; Al Farraj, O.; Morgagni, S.; Siliquini, R.; Moirana, F.; Messina, G.G.; Sassi, F. Hospital patient migration: Analysis using a utility index. In Public Health in Europe; Kirch, W., Ed.; Springer: Berlin/Heidelberg, Germany, 2004; pp. 293–316. [Google Scholar]
- Sivey, P. The effect of waiting time and distance on hospital choice for English cataract patients. Health Econ. 2012, 21, 444–456. [Google Scholar] [CrossRef]
- Moscelli, G.; Siciliani, L.; Gutacker, N.; Gravelle, H. Location, quality and choice of hospital: Evidence from England 2002–2013. Reg. Sci. Urban Econ. 2016, 60, 112–124. [Google Scholar] [CrossRef]
- Pinto, C. Percived quality and formation of inter-regional networks of health care migration. Adv. Manag. Appl. Econ. 2017, 7, 93–111. Available online: https://www.scienpress.com/journal_focus.asp?main_id=55&Sub_id=IV&Issue=259775 (accessed on 27 May 2023).
- Schnatz, P.F.; Murphy, J.L.; O’Sullivan, D.M.; Sorosky, J.I. Patient choice: Comparing criteria for selecting an obstetrician-gynecologist based on image, gender, and professional attributes. Am. J. Obstet. Gynecol. 2007, 197, 548.e1–548.e7. [Google Scholar] [CrossRef] [PubMed]
- Howell, E.A.; Gardiner, B.; Concato, J. Do women prefer female obstetricians? Obstet. Gynecol. 2002, 99, 1031–1035. [Google Scholar]
- Martini, G.; Levaggi, R.; Spinelli, D. Is there a bias in patient choices for hospital care? Evidence from three Italian regional health systems. Health Policy 2022, 126, 668–679. [Google Scholar] [CrossRef]
- Italian Ministry of Health. Beds per Hospital Facility. Available online: https://www.dati.salute.gov.it/dati/dettaglioDataset.jsp?menu=dati&idPag=114 (accessed on 3 April 2023).
- ISTAT. Health for All—Italia. Update December 2022. Available online: http://www.istat.it/it/archivio/14562 (accessed on 3 January 2023).
- Guarducci, G.; Messina, G.; Carbone, S.; Urbani, A.; Nante, N. Inter-Regional Patients’ Migration for Hospital Orthopedic Intensive Rehabilitation: The Italian Experience. Int. J. Environ. Res. Public Health 2022, 19, 13726. [Google Scholar] [CrossRef]
- Gandy, R.J. A graphical representation of the inter-relationship between districts. Hosp. Health Serv. Rev. 1979, 75, 50–51. [Google Scholar]
- Gandy, R.; Franci, A.; Gurrieri, C.; McClelland, R. Demonstrating Access to Public Services Diagrammatically. Int. J. Public Adm. 2011, 34, 516–527. [Google Scholar] [CrossRef]
- De Curtis, M.; Bortolan, F.; Diliberto, D.; Villani, L. Pediatric interregional healthcare mobility in Italy. Ital. J. Pediatr. 2021, 47, 139. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, I.W. Principles of Biomechanics & Motion Analysis; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2006. [Google Scholar]
- Blàsquez-Fernàndez, C.; Cantarero-Prieto, D.; Pascual-Sàez, M. Patient cross-border mobility: New findings and implications in Spanish regions. Econ. Sociol. 2017, 10, 11–21. [Google Scholar] [CrossRef]
- Berta, P.; Guerriero, C.; Levaggi, R. Hospitals’ strategic behaviours and patient mobility: Evidence from Italy. Socio-Econ. Plan. Sci. 2021, 77, 101030. [Google Scholar] [CrossRef]
- Conference of the Regions and Autonomous Provinces. Health Pact 2019–2021. Available online: http://www.regioni.it/newsletter/n-3750/del-07-01-2020/patto-per-la-salute-2019-2021-il-testo-20616/ (accessed on 10 June 2023).
- Berta, P.; Martini, G.; Spinelli, D.; Vittadini, G. The beaten paths effect on patient inter-regional mobility: An application to the Italian NHS. Pap. Reg. Sci. 2022, 101, 945–977. [Google Scholar] [CrossRef]
- Calovi, M.; Seghieri, C. Using a GIS to support the spatial reorganization of outpatient care services delivery in Italy. BMC Health Serv Res. 2018, 18, 883. [Google Scholar] [CrossRef] [PubMed]
- Seghieri, C.; Calovi, M.; Ferrè, F. Proximity and waiting times in choice models for outpatient cardiological visits in Italy. PLoS ONE 2018, 13, e0203018. [Google Scholar] [CrossRef] [PubMed]
- Roh, C.Y.; Lee, K.H.; Fottler, M.D. Determinants of hospital choice of rural hospital patients: The impact of networks, service scopes, and market competition. J. Med. Syst. 2008, 32, 343–353. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Year | Residents | Mobility | Total | Total (ORD + DH) * | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ORD | DH * | ORD/DH * | ORD * | DH * | ORD/DH * | ORD | DH * | ORD/DH * | ||
| 2011 | 263,884 | 47,550 | 5.55 | 44,067 | 5733 | 7.69 | 307,951 | 53,283 | 5.78 | 361,234 |
| 2012 | 266,029 | 39,783 | 6.69 | 46,069 | 5328 | 8.65 | 312,098 | 45,111 | 6.92 | 357,209 |
| 2013 | 269,373 | 36,419 | 7.40 | 48,132 | 4452 | 10.81 | 317,505 | 40,871 | 7.77 | 358,376 |
| 2014 | 265,473 | 31,692 | 8.38 | 48,462 | 3173 | 15.27 | 313,935 | 34,865 | 9.00 | 348,800 |
| 2015 | 267,010 | 30,812 | 8.67 | 50,466 | 3236 | 15.60 | 317,476 | 34,048 | 9.32 | 351,524 |
| 2016 | 265,753 | 28,905 | 9.19 | 51,796 | 2949 | 17.56 | 317,549 | 31,854 | 9.97 | 349,403 |
| 2017 | 263,474 | 27,716 | 9.51 | 51,579 | 3001 | 17.19 | 315,053 | 30,717 | 10.26 | 345,770 |
| 2018 | 260,856 | 25,477 | 10.24 | 50,596 | 2974 | 17.01 | 311,452 | 28,451 | 10.95 | 339,903 |
| 2019 | 261,481 | 25,524 | 10.24 | 49,386 | 3092 | 15.97 | 310,867 | 28,616 | 10.86 | 339,483 |
| Region | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | Mean 2011–2019 |
|---|---|---|---|---|---|---|---|---|---|---|
| Piedmont | 0.72 | 0.75 | 0.75 | 0.74 | 0.74 | 0.74 | 0.74 | 0.75 | 0.76 | 0.74 |
| Aosta Valley | 0.64 | 0.01 | 0.51 | 0.61 | 0.59 | 0.59 | 0.59 | 0.62 | 0.62 | 0.53 |
| Lombardy | 0.73 | 0.67 | 0.65 | 0.65 | 0.66 | 0.67 | 0.66 | 0.66 | 0.66 | 0.67 |
| A.P. of Bolzano * | 0.33 | 0.33 | 0.34 | 0.37 | 0.37 | 0.43 | 0.42 | 0.44 | 0.35 | 0.37 |
| A.P. of Trento | 0.86 | 0.57 | 0.80 | 0.75 | 0.69 | 0.69 | 0.71 | 0.70 | 0.76 | 0.73 |
| Veneto | 0.37 | 0.37 | 0.37 | 0.37 | 0.38 | 0.40 | 0.40 | 0.40 | 0.40 | 0.38 |
| F.V. Giulia | 0.23 | 0.22 | 0.24 | 0.24 | 0.23 | 0.24 | 0.23 | 0.23 | 0.22 | 0.23 |
| Liguria | 0.44 | 0.41 | 0.48 | 0.51 | 0.43 | 0.46 | 0.45 | 0.45 | 0.44 | 0.45 |
| E. Romagna * | 0.37 | 0.37 | 0.36 | 0.35 | 0.35 | 0.35 | 0.34 | 0.34 | 0.34 | 0.35 |
| Tuscany * | 0.23 | 0.24 | 0.24 | 0.25 | 0.26 | 0.25 | 0.24 | 0.26 | 0.26 | 0.25 |
| Umbria * | 0.34 | 0.35 | 0.39 | 0.39 | 0.39 | 0.40 | 0.42 | 0.43 | 0.43 | 0.39 |
| Marche * | 0.24 | 0.24 | 0.25 | 0.25 | 0.26 | 0.29 | 0.29 | 0.29 | 0.29 | 0.27 |
| Latium * | 0.68 | 0.59 | 0.56 | 0.56 | 0.55 | 0.54 | 0.54 | 0.53 | 0.54 | 0.56 |
| Abruzzo | 0.39 | 0.39 | 0.39 | 0.38 | 0.38 | 0.45 | 0.38 | 0.39 | 0.38 | 0.39 |
| Molise | 0.77 | 0.75 | 0.91 | 0.78 | 0.77 | 0.77 | 0.65 | 0.65 | 0.59 | 0.74 |
| Campania | 0.25 | 0.24 | 0.25 | 0.25 | 0.24 | 0.25 | 0.25 | 0.25 | 0.27 | 0.25 |
| Apulia | 0.32 | 0.30 | 0.31 | 0.31 | 0.30 | 0.30 | 0.30 | 0.30 | 0.32 | 0.31 |
| Basilicata | 0.42 | 0.33 | 0.34 | 0.34 | 0.34 | 0.32 | 0.32 | 0.32 | 0.32 | 0.34 |
| Calabria | 0.28 | 0.26 | 0.32 | 0.41 | 0.37 | 0.36 | 0.40 | 0.41 | 0.38 | 0.36 |
| Sicily * | 0.27 | 0.29 | 0.31 | 0.32 | 0.32 | 0.32 | 0.32 | 0.35 | 0.37 | 0.32 |
| Sardinia | 0.13 | 0.13 | 0.10 | 0.13 | 0.13 | 0.13 | 0.13 | 0.13 | 0.12 | 0.13 |
| Italy | 0.49 | 0.48 | 0.48 | 0.49 | 0.46 | 0.49 | 0.49 | 0.49 | 0.50 | 0.49 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guarducci, G.; Messina, G.; Carbone, S.; Nante, N. Identifying the Drivers of Inter-Regional Patients’ Mobility: An Analysis on Hospital Beds Endowment. Healthcare 2023, 11, 2045. https://doi.org/10.3390/healthcare11142045
Guarducci G, Messina G, Carbone S, Nante N. Identifying the Drivers of Inter-Regional Patients’ Mobility: An Analysis on Hospital Beds Endowment. Healthcare. 2023; 11(14):2045. https://doi.org/10.3390/healthcare11142045
Chicago/Turabian StyleGuarducci, Giovanni, Gabriele Messina, Simona Carbone, and Nicola Nante. 2023. "Identifying the Drivers of Inter-Regional Patients’ Mobility: An Analysis on Hospital Beds Endowment" Healthcare 11, no. 14: 2045. https://doi.org/10.3390/healthcare11142045
APA StyleGuarducci, G., Messina, G., Carbone, S., & Nante, N. (2023). Identifying the Drivers of Inter-Regional Patients’ Mobility: An Analysis on Hospital Beds Endowment. Healthcare, 11(14), 2045. https://doi.org/10.3390/healthcare11142045