
Preoperative Anxiety in Patients with Pancreatic Cancer: What Contributes to Anxiety Levels in Patients Waiting for Surgical Intervention

 ,
,  , and
, and
Abstract
1. Introduction
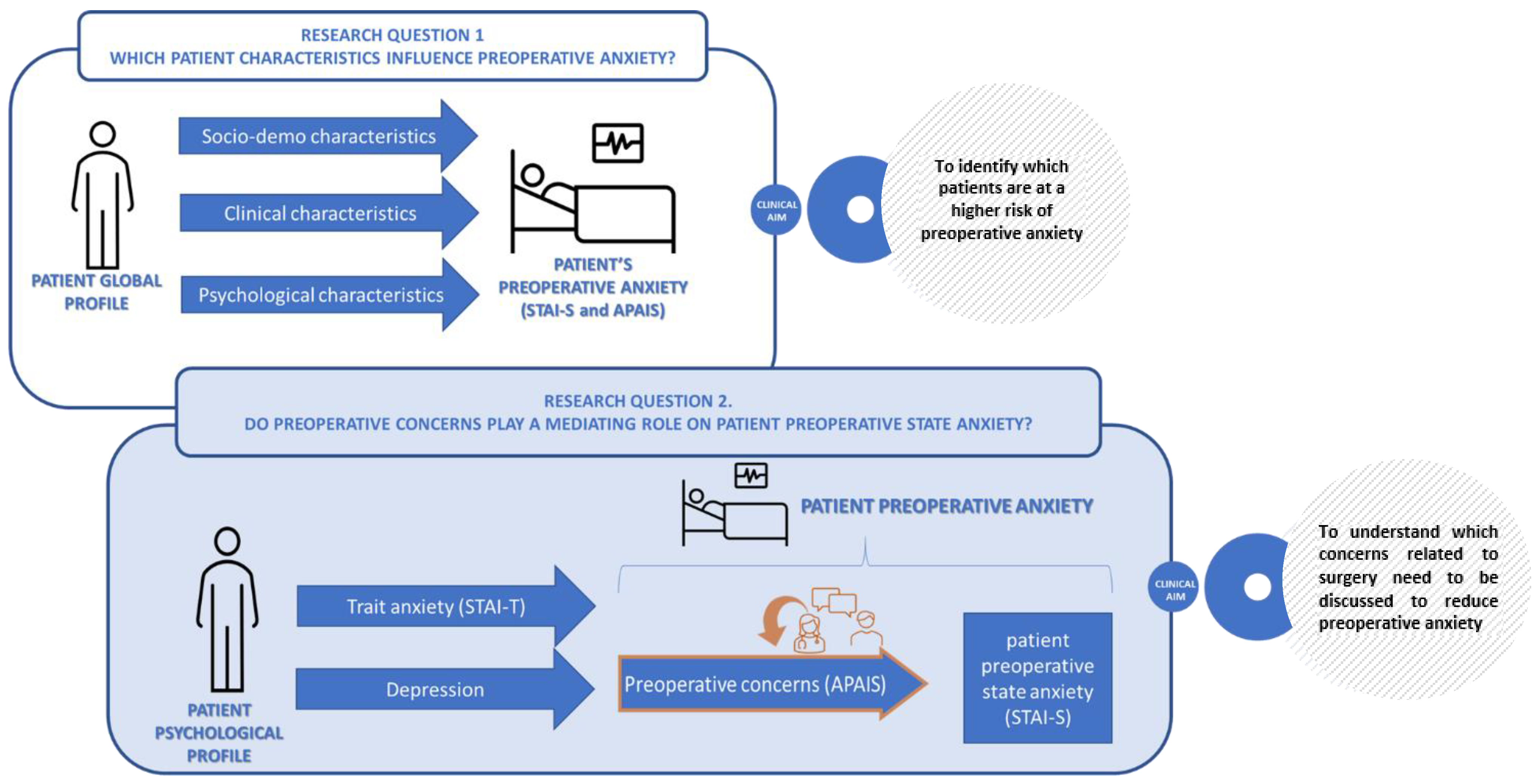
- To identify patients’ socio-demographic, clinical and psychological characteristics that most contribute to preoperative anxiety. According to Spielberg, anxiety can be distinguished into trait anxiety, as a stable feature of personality, and state anxiety, as the degree of anxiety at a particular time [21]. The latter is the type of anxiety considered in our study, and defined as preoperative anxiety preceding pancreatic surgery.
- To explore the link between patient’s preoperative anxiety and the type of preoperative concerns related to surgery. Identifying which are the key concerns to address can help surgeons to improve doctor-patient communication.
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measures
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA A Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef]
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting Cancer Incidence and Deaths to 2030: The Unexpected Burden of Thyroid, Liver, and Pancreas Cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef]
- Strobel, O.; Neoptolemos, J.; Jäger, D.; Büchler, M.W. Optimizing the Outcomes of Pancreatic Cancer Surgery. Nat. Rev. Clin. Oncol. 2019, 16, 11–26. [Google Scholar] [CrossRef] [PubMed]
- de Albuquerque, V.C.; Silva Batista, I.A.; Oliveira, C.P. Evaluation of Anxiety Levels in Preoperative Patients: A Literature Review. Int. J. Innov. Sci. Res. Technol. 2019, 4, 478–480. [Google Scholar]
- Abate, S.M.; Chekol, Y.A.; Basu, B. Global Prevalence and Determinants of Preoperative Anxiety among Surgical Patients: A Systematic Review and Meta-Analysis. Int. J. Surg. Open 2020, 25, 6–16. [Google Scholar] [CrossRef]
- Aust, H.; Eberhart, L.; Sturm, T.; Schuster, M.; Nestoriuc, Y.; Brehm, F.; Rüsch, D. A Cross-Sectional Study on Preoperative Anxiety in Adults. J. Psychosom. Res. 2018, 111, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Kuzminskaitė, V.; Kaklauskaitė, J.; Petkevičiūtė, J. Incidence and Features of Preoperative Anxiety in Patients Undergoing Elective Non-Cardiac Surgery. Acta Med. Litu. 2019, 26, 93–100. [Google Scholar] [CrossRef]
- Ali, A.; Altun, D.; Oguz, B.H.; Ilhan, M.; Demircan, F.; Koltka, K. The Effect of Preoperative Anxiety on Postoperative Analgesia and Anesthesia Recovery in Patients Undergoing Laparascopic Cholecystectomy. J. Anesth. 2014, 28, 222–227. [Google Scholar] [CrossRef]
- Turksal, E.; Alper, I.; Sergin, D.; Yuksel, E.; Ulukaya, S. The Effects of Preoperative Anxiety on Anesthetic Recovery and Postoperative Pain in Patients Undergoing Donor Nephrectomy. Braz. J. Anesthesiol. 2020, 70, 271–277. [Google Scholar] [CrossRef]
- Wu, H.; Huang, Y.; Tian, X.; Zhang, Z.; Zhang, Y.; Mao, Y.; Wang, C.; Yang, S.; Liu, Y.; Zhang, W.; et al. Preoperative Anxiety-Induced Glucocorticoid Signaling Reduces GABAergic Markers in Spinal Cord and Promotes Postoperative Hyperalgesia by Affecting Neuronal PAS Domain Protein 4. Mol. Pain 2019, 15, 1744806919850383. [Google Scholar] [CrossRef]
- Bayrak, A.; Sagiroglu, G.; Copuroglu, E. Effects of Preoperative Anxiety on Intraoperative Hemodynamics and Postoperative Pain. J. Coll. Physicians Surg. Pak. 2019, 29, 868–873. [Google Scholar] [CrossRef] [PubMed]
- Wada, S.; Inoguchi, H.; Sadahiro, R.; Matsuoka, Y.J.; Uchitomi, Y.; Sato, T.; Shimada, K.; Yoshimoto, S.; Daiko, H.; Shimizu, K. Preoperative Anxiety as a Predictor of Delirium in Cancer Patients: A Prospective Observational Cohort Study. World J. Surg. 2019, 43, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Egan, K.J.; Ready, L.B.; Nessly, M.; Greer, B.E. Self-Administration of Midazolam for Postoperative Anxiety: A Double Blinded Study. Pain 1992, 49, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Jørgensen, P.; Aagaard, J.; Jespersen, J.H.; Mortensen, L. Nonspecific Psychological Distress, Psychosocial Stressors and Delusional Psychosis.: A Comparison with Psychiatrically Symptom Free Surgical Controls. Acta Psychiatr. Scand. 1987, 75, 190–194. [Google Scholar] [CrossRef]
- Clark, D.A.; Cook, A.; Snow, D. Depressive Symptom Differences in Hospitalized, Medically Ill, Depressed Psychiatric Inpatients and Nonmedical Controls. J. Abnorm. Psychol. 1998, 107, 38–48. [Google Scholar] [CrossRef]
- Barnes, A.F.; Yeo, T.P.; Leiby, B.; Kay, A.; Winter, J.M. Pancreatic Cancer–Associated Depression: A Case Report and Review of the Literature. Pancreas 2018, 47, 1065–1077. [Google Scholar] [CrossRef]
- Del Piccolo, L.; Marinelli, V.; Mazzi, M.A.; Danzi, O.P.; Bonamini, D.; Secchettin, E.; Tuveri, M.; Bassi, C.; Rimondini, M.; Salvia, R. Prevalence of Depression in a Cohort of 400 Patients with Pancreatic Neoplasm Attending Day Hospital for Major Surgery: Role on Depression of Psychosocial Functioning and Clinical Factors. Psychooncology 2021, 30, 455–462. [Google Scholar] [CrossRef]
- Prado-Olivares, J.; Chover-Sierra, E. Preoperatory Anxiety in Patients Undergoing Cardiac Surgery. Diseases 2019, 7, 46. [Google Scholar] [CrossRef]
- Valenzuela Millán, J.; Barrera Serrano, J.R.; Ornelas Aguirre, J.M. Anxiety in Preoperative Anesthetic Procedures. Cir. Cir. 2010, 78, 147–151. [Google Scholar]
- Lemiński, A.; Kaczmarek, K.; Bańcarz, A.; Zakrzewska, A.; Małkiewicz, B.; Słojewski, M. Educational and Psychological Support Combined with Minimally Invasive Surgical Technique Reduces Perioperative Depression and Anxiety in Patients with Bladder Cancer Undergoing Radical Cystectomy. Int. J. Environ. Res. Public Health 2021, 18, 13071. [Google Scholar] [CrossRef]
- Spielberger, C.; Gorsuch, R.; Lushene, R.; Vagg, P.; Jacobs, G. Manual for the State-Trait Anxiety Inventory (Form Y1–Y2); Consulting Psychologists Press: Palo Alto, CA, USA, 1983; Volume IV. [Google Scholar]
- Marinelli, V.; Danzi, O.P.; Mazzi, M.A.; Secchettin, E.; Tuveri, M.; Bonamini, D.; Rimondini, M.; Salvia, R.; Bassi, C.; Del Piccolo, L. PREPARE: PreoPerative Anxiety REduction. One-Year Feasibility RCT on a Brief Psychological Intervention for Pancreatic Cancer Patients Prior to Major Surgery. Front. Psychol. 2020, 11, 362. [Google Scholar] [CrossRef]
- Spielberger, C.D.; Pedrabissi, L.; Santinello, M. Inventario Per L’ansia di Stato e di Tratto: Nuova Versione Italiana Dello S.T.A.I., Forma Y: Manuale; Organizzazioni Speciali: Florence, Italy, 1989; ISBN 978-88-09-40023-8. [Google Scholar]
- Bunevicius, A.; Staniute, M.; Brozaitiene, J.; Pop, V.J.; Neverauskas, J.; Bunevicius, R. Screening for Anxiety Disorders in Patients with Coronary Artery Disease. Health Qual. Life Outcomes 2013, 11, 37. [Google Scholar] [CrossRef]
- Ilardi, C.R.; Gamboz, N.; Iavarone, A.; Chieffi, S.; Brandimonte, M.A. Psychometric Properties of the STAI-Y Scales and Normative Data in an Italian Elderly Population. Aging Clin. Exp. Res. 2021, 33, 2759–2766. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B. Validation and Utility of a Self-Report Version of PRIME-MD: The PHQ Primary Care Study. Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire. JAMA 1999, 282, 1737–1744. [Google Scholar] [CrossRef]
- American Psychiatric Association Diagnostic and Statistical Manual of Mental Disorders; DSM-5-TR.; American Psychiatric Association Publishing: Washington, DC, USA, 2022; ISBN 978-0-89042-575-6.
- Moerman, N.; van Dam, F.S.; Muller, M.J.; Oosting, H. The Amsterdam Preoperative Anxiety and Information Scale (APAIS). Anesth. Analg. 1996, 82, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Buonanno, P.; Laiola, A.; Palumbo, C.; Spinelli, G.; Terminiello, V.; Servillo, G. Italian Validation of the Amsterdam Preoperative Anxiety and Information Scale. Minerva Anestesiol. 2017, 83, 705–711. [Google Scholar] [CrossRef] [PubMed]
- Moors, G. Exploring the Effect of a Middle Response Category on Response Style in Attitude Measurement. Qual. Quant. 2008, 42, 779–794. [Google Scholar] [CrossRef] [PubMed]
- Jonckheere, A.R. A Distribution-Free k-Sample Test Against Ordered Alternatives. Biometrika 1954, 41, 133. [Google Scholar] [CrossRef]
- Luchman, J.N. Determining Relative Importance in Stata Using Dominance Analysis: Domin and Domme. Stata J. 2021, 21, 510–538. [Google Scholar] [CrossRef]
- Streiner, D.L. Finding Our Way: An Introduction to Path Analysis. Can. J. Psychiatry 2005, 50, 115–122. [Google Scholar] [CrossRef]
- Mehmetoglu, M. Medsem: A Stata Package for Statistical Mediation Analysis. Int. J. Comput. Econ. Econom. 2018, 8, 63. [Google Scholar] [CrossRef]
- Lee, H.; Cashin, A.G.; Lamb, S.E.; Hopewell, S.; Vansteelandt, S.; VanderWeele, T.J.; MacKinnon, D.P.; Mansell, G.; Collins, G.S.; Golub, R.M.; et al. A Guideline for Reporting Mediation Analyses of Randomized Trials and Observational Studies: The AGReMA Statement. JAMA 2021, 326, 1045. [Google Scholar] [CrossRef] [PubMed]
- Jak, S.; Jorgensen, T.D.; Verdam, M.G.E.; Oort, F.J.; Elffers, L. Analytical Power Calculations for Structural Equation Modeling: A Tutorial and Shiny App. Behav. Res. 2021, 53, 1385–1406. [Google Scholar] [CrossRef]
- Jlala, H.A.; French, J.L.; Foxall, G.L.; Hardman, J.G.; Bedforth, N.M. Effect of Preoperative Multimedia Information on Perioperative Anxiety in Patients Undergoing Procedures under Regional Anaesthesia. Br. J. Anaesth. 2010, 104, 369–374. [Google Scholar] [CrossRef]
- Maranets, I.; Kain, Z.N. Preoperative Anxiety and Intraoperative Anesthetic Requirements. Anesth. Analg. 1999, 89, 1346–1351. [Google Scholar] [CrossRef]
- Hellstadius, Y.; Lagergren, J.; Zylstra, J.; Gossage, J.; Davies, A.; Hultman, C.M.; Lagergren, P.; Wikman, A. A Longitudinal Assessment of Psychological Distress after Oesophageal Cancer Surgery. Acta Oncol. 2017, 56, 746–752. [Google Scholar] [CrossRef]
- Arlı, Ş.K. Evaluation of the Preoperative Anxiety with APAIS and STAI-I Scales. J. Hacet. Univ. Fac. Nurs. 2017, 4, 38–47. [Google Scholar]
- Aykent, R.; Kocamanoǧlu, I.S.; Üstün, E.; Tür, A.; Şahinoǧlu, H. The Reasons and Evaluation of Preoperative Anxiety: A Comparison of APAIS and STAI Scores. Turk. Klin. J. Anest. Reanim. 2007, 5, 7–13. [Google Scholar]
- King, A.; Bartley, J.; Johanson, D.L.; Broadbent, E. Components of Preoperative Anxiety: A Qualitative Study. J. Health Psychol. 2019, 24, 1897–1908. [Google Scholar] [CrossRef]
- Fogarty, L.A.; Curbow, B.A.; Wingard, J.R.; McDonnell, K.; Somerfield, M.R. Can 40 Seconds of Compassion Reduce Patient Anxiety? J. Clin. Oncol. 1999, 17, 371–379. [Google Scholar] [CrossRef]
- Liénard, A.; Merckaert, I.; Libert, Y.; Delvaux, N.; Marchal, S.; Boniver, J.; Etienne, A.-M.; Klastersky, J.; Reynaert, C.; Scalliet, P.; et al. Factors That Influence Cancer Patients’ Anxiety Following a Medical Consultation: Impact of a Communication Skills Training Programme for Physicians. Ann. Oncol. 2006, 17, 1450–1458. [Google Scholar] [CrossRef] [PubMed]
- Baile, W.F.; Buckman, R.; Lenzi, R.; Glober, G.; Beale, E.A.; Kudelka, A.P. SPIKES-A Six-Step Protocol for Delivering Bad News: Application to the Patient with Cancer. Oncologist 2000, 5, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Meitar, D.; Karnieli-Miller, O. Twelve Tips to Manage a Breaking Bad News Process: Using S-P-w-ICE-S—A Revised Version of the SPIKES Protocol. Med. Teach. 2022, 44, 1087–1091. [Google Scholar] [CrossRef] [PubMed]
- Oba, A.; Ho, F.; Bao, Q.R.; Al-Musawi, M.H.; Schulick, R.D.; Del Chiaro, V. Neoadjuvant treatment in pancreatic cancer. Front. Oncol. 2020, 10, 245. [Google Scholar] [CrossRef] [PubMed]
- Kang, W.; Steffens, F.; Pineda, S.; Widuch, K.; Malvaso, A. Personality traits and dimensions of mental health. Sci. Rep. 2023, 13, 7091. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| N | Mean | sd | Min | Max | t/F (p-Value) | |
|---|---|---|---|---|---|---|
| Total sample | 104 | 43.3 | 12.9 | 20 | 77 | |
| Gender | 1.58 | |||||
| Male | 47 | 41.1 | 13.7 | 20 | 74 | (0.12) |
| Female | 57 | 45.1 | 12.1 | 24 | 77 | |
| Age | 0.84 | |||||
| <50 | 11 | 46.0 | 12.0 | 30 | 68 | (0.43) |
| 51–69 | 64 | 42.0 | 12.7 | 20 | 74 | |
| >70 | 29 | 45.1 | 13.8 | 24 | 77 | |
| Education | 1.04 | |||||
| Primary/middle | 47 | 44.7 | 14.5 | 20 | 77 | (0.30) |
| high/degree | 57 | 42.1 | 11.5 | 22 | 70 | |
| Marital status | 0.28 | |||||
| Married/with partner | 18 | 44.1 | 13.6 | 24 | 77 | (0.78) |
| Single/Separated/widowed | 86 | 43.1 | 12.9 | 20 | 74 | |
| Working condition | 0.44 | |||||
| Employed/student | 37 | 42.5 | 11.6 | 22 | 70 | (0.66) |
| Other | 67 | 43.7 | 13.6 | 20 | 77 | |
| Region | 0.01 | |||||
| Veneto | 18 | 43.2 | 15.9 | 24 | 74 | (0.99) |
| Other regions | 86 | 43.3 | 12.4 | 20 | 77 | |
| Clinical pathway | 2.5 | |||||
| Malignant upfront | 51 | 42.5 | 13.5 | 22 | 74 | (0.09) |
| Malignant chemio | 27 | 40.4 | 10.6 | 20 | 62 | |
| Benign + uncertain behaviour | 26 | 47.8 | 12.3 | 28 | 77 | |
| Type of intervention | 1.06 | |||||
| DCP–whipple | 53 | 43.8 | 14.3 | 20 | 77 | (0.37) |
| exploratory laparotomy | 13 | 38.3 | 12.1 | 22 | 61 | |
| partial S-P resection | 26 | 45.7 | 10.6 | 32 | 70 | |
| total S-P resection | 12 | 41.3 | 11.6 | 29 | 65 | |
| STAI-T | 12.59 | |||||
| Absent (20–39) | 87 | 41.1 | 11.6 | 20 | 74 | (<0.01) |
| Mild (40–49) | 10 | 51.1 | 12.9 | 35 | 70 | |
| Moderate + Serious (≥50) | 6 | 63.3 | 11.8 | 45 | 77 | |
| PHQ9 | 8.00 | |||||
| Absent (<4) | 59 | 39.7 | 11.3 | 20 | 70 | (<0.01) |
| Mild (5–9) | 34 | 46.5 | 13.1 | 24 | 74 | |
| Major depression (>10) | 10 | 54.4 | 14.1 | 37 | 77 |
| APAIS-Anaesthesia | APAIS-Surgery | APAIS-Information | |||||||
|---|---|---|---|---|---|---|---|---|---|
| M | sd | t/F (p) | M | sd | t/F (p) | M | sd | t/F (p) | |
| Total sample | 4.4 | 3.1 | 7.1 | 3.3 | 3.5 | 2.1 | |||
| Gender | 1.83 | 1.73 | 1.38 | ||||||
| Male | 3.7 | 3.2 | (0.07) | 6.5 | 3.5 | (0.09) | 3.2 | 1.6 | (0.17) |
| Female | 4.9 | 3.0 | 7.6 | 3.1 | 3.8 | 2.4 | |||
| Age | 0.05 | 0.35 | 0.27 | ||||||
| <50 | 4.5 | 3.2 | (0.95) | 7.9 | 3.4 | (0.70) | 3.5 | 1.7 | (0.77) |
| 51–69 | 4.3 | 3.1 | 7.1 | 3.2 | 3.4 | 2.2 | |||
| >70 | 4.4 | 3.2 | 6.9 | 3.6 | 3.8 | 2.0 | |||
| Education | 0.67 | 0.73 | 0.91 | ||||||
| Primary/middle | 4.1 | 2.9 | (0.50) | 7.4 | 3.4 | (0.48) | 3.7 | 2.1 | (0.36) |
| high/degree | 4.5 | 3.3 | 6.9 | 3.3 | 3.4 | 2.0 | |||
| Marital status | 0.13 | 0.66 | 0.08 | ||||||
| Married/with partner | 4.4 | 2.7 | (0.90) | 7.6 | 3.0 | (0.51) | 3.6 | 2.4 | (0.93) |
| Single/Separated/widowed | 4.3 | 3.2 | 7.0 | 3.4 | 3.5 | 2.0 | |||
| Working condition | 0.12 | 0.91 | 1.92 | ||||||
| Employed/student | 4.4 | 3.1 | (0.98) | 7.5 | 3.2 | (0.37) | 3.0 | 1.5 | (0.06) |
| Other | 4.3 | 3.2 | 6.9 | 3.3 | 3.8 | 2.3 | |||
| Region | 0.53 | 0.03 | 0.21 | ||||||
| Veneto | 4.0 | 2.7 | (0.60) | 7.2 | 0.9 | (0.98) | 3.6 | 2.1 | (0.84) |
| Other regions | 4.4 | 3.2 | 7.1 | 3.3 | 3.5 | 2.1 | |||
| Clinical pathway | 2.21 | 1.21 | 2.31 | ||||||
| Malignant upfront | 4.4 | 3.3 | (0.11) | 6.9 | 3.3 | (0.30) | 3.4 | 2.0 | (0.10) |
| Malignant chemio | 3.4 | 1.9 | 6.7 | 3.3 | 3.1 | 1.3 | |||
| Benign + uncertain behaviour | 5.2 | 3.6 | 8.0 | 3.4 | 4.2 | 2.7 | |||
| Type of intervention | 1.95 | 1.08 | 1.56 | ||||||
| DCP–whipple | 4.1 | 3.0 | (0.13) | 7.5 | 3.2 | (0.36) | 3.3 | 1.9 | (0.20) |
| exploratory laparotomy | 3.0 | 1.6 | 5.7 | 3.8 | 3.2 | 1.8 | |||
| partial S-P resection | 5.4 | 3.7 | 7.3 | 3.3 | 4.3 | 2.6 | |||
| total S-P resection | 4.7 | 3.0 | 6.8 | 3.1 | 3.3 | 1.6 | |||
| STAI-T | 4.28 | 4.43 | 7.31 | ||||||
| Absent (20–39) | 4.0 | 2.8 | (0.02) | 6.7 | 3.2 | (0.01) | 3.3 | 1.7 | (<0.01) |
| Mild (40–49) | 5.7 | 4.5 | 9.0 | 3.9 | 3.4 | 2.1 | |||
| Moderate + Serious (≥50) | 7.2 | 3.4 | 9.8 | 2.1 | 6.3 | 3.9 | |||
| PHQ9 | 3.23 | 2.61 | 1.9 | ||||||
| Absent (<4) | 3.7 | 2.8 | (0.04) | 6.5 | 3.2 | (0.08) | 3.2 | 1.7 | (0.15) |
| Mild (5–9) | 4.9 | 3.2 | 7.9 | 3.2 | 3.7 | 2.4 | |||
| Major depression (>10) | 6.1 | 4.2 | 8.3 | 3.9 | 3.5 | 2.0 | |||
| Dependent Variable | Independent Variable | Unstd Coef (Std Err) | z Test | p-Value | 95% CI | Std Coeff |
|---|---|---|---|---|---|---|
| STAI-S | APAIS-S | 1.75 (0.27) | 6.38 | <0.01 | 1.21–2.29 | 0.45 |
| STAI-T | 0.45 (0.09) | 4.84 | <0.01 | 0.27–0.64 | 0.31 | |
| PHQ9 | 0.54 (0.19) | 2.82 | <0.01 | 0.16–0.91 | 0.17 | |
| const | 14.32 (2.99) | 4.78 | <0.01 | 8.44–20.17 | 1.11 | |
| APAIS-S | STAI-T | 0.14 (0.03) | 4.52 | <0.01 | 0.08–0.20 | 0.37 |
| const | 2.72 (1.03) | 2.63 | <0.01 | 0.70–4.74 | 0.82 | |
| APAIS-I | STAI-T | 0.07 (0.03) | 2.83 | <0.01 | 0.02–0.13 | 0.33 |
| const | 1.09 (0.80) | 1.37 | 0.17 | −0.47–2.65 | 0.54 | |
| APAIS-A | PHQ9 | 0.23 (0.08) | 2.96 | <0.01 | 0.08–0.40 | 0.31 |
| const | 3.27 (0.40) | 8.08 | <0.01 | 2.48–4.07 | 0.05 | |
| mean | STAI-T | 31.39 (0.87) | 35.86 | <0.01 | 29.68–33.11 | 3.57 |
| mean | PHQ9 | 4.47 (0.40) | 11.07 | <0.01 | 3.68–5.26 | 1.10 |
| cov | STAI-T; PHQ9 | 14.15 (3.69) | 3.83 | <0.01 | 6.92–21.38 | 0.40 |
| var | STAI-S | 81.34 (11.69) | 61.37–107.81 | 0.41 | ||
| var | APAIS-S | 9.47 (1.04) | 7.62–11.76 | 0.86 | ||
| var | APAIS-I | 3.59 (0.63) | 2.55–5.06 | 0.90 | ||
| var | APAIS-A | 8.77 (1.21) | 6.69–11.49 | 0.90 | ||
| var | STAI-T | 77.40 (14.40) | 53.75–11.45 | 1 | ||
| var | PHQ9 | 16.46 (2.62) | 12.06–22.48 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marinelli, V.; Mazzi, M.A.; Rimondini, M.; Danzi, O.P.; Bonamini, D.; Bassi, C.; Salvia, R.; Del Piccolo, L. Preoperative Anxiety in Patients with Pancreatic Cancer: What Contributes to Anxiety Levels in Patients Waiting for Surgical Intervention. Healthcare 2023, 11, 2039. https://doi.org/10.3390/healthcare11142039
Marinelli V, Mazzi MA, Rimondini M, Danzi OP, Bonamini D, Bassi C, Salvia R, Del Piccolo L. Preoperative Anxiety in Patients with Pancreatic Cancer: What Contributes to Anxiety Levels in Patients Waiting for Surgical Intervention. Healthcare. 2023; 11(14):2039. https://doi.org/10.3390/healthcare11142039
Chicago/Turabian StyleMarinelli, Veronica, Maria Angela Mazzi, Michela Rimondini, Olivia Purnima Danzi, Deborah Bonamini, Claudio Bassi, Roberto Salvia, and Lidia Del Piccolo. 2023. "Preoperative Anxiety in Patients with Pancreatic Cancer: What Contributes to Anxiety Levels in Patients Waiting for Surgical Intervention" Healthcare 11, no. 14: 2039. https://doi.org/10.3390/healthcare11142039
APA StyleMarinelli, V., Mazzi, M. A., Rimondini, M., Danzi, O. P., Bonamini, D., Bassi, C., Salvia, R., & Del Piccolo, L. (2023). Preoperative Anxiety in Patients with Pancreatic Cancer: What Contributes to Anxiety Levels in Patients Waiting for Surgical Intervention. Healthcare, 11(14), 2039. https://doi.org/10.3390/healthcare11142039