
e-Health Interventions Targeting Pain-Related Psychological Variables in Fibromyalgia: A Systematic Review

 ,
,  , ,
, ,  , , and
, , and 
Abstract
1. Introduction
- To provide a systematic and in-depth description of the available e-Health tools delivering multicomponent and psychosocial interventions targeting psychosocial outcomes and/or pain-related psychological variables for patients with FMS;
- To describe the main psychological approaches used in those e-Health interventions, their structure, and their main characteristics, along with the main psychosocial outcomes and pain-related psychological variables targeted in the included interventions;
- To describe the impact of the e-Health tools in terms of signals of efficacy, feasibility, and acceptability.
2. Materials and Methods
- What e-Heath tools are under investigation to deliver psychological and/or multicomponent interventions targeted psychosocial outcomes and/or pain-related psychological variables in patients with FMS?
- What are the main characteristics of those e-Health interventions in terms of underlying psychological approaches, structure, and addressed outcomes?
- What is the impact of such e-Health tools in terms of signals of efficacy, feasibility, and acceptability?
2.1. Searches
2.2. Inclusion and Exclusion Criteria
2.3. Risk of Bias Assessment
2.4. Data Extraction and Synthesis
3. Results
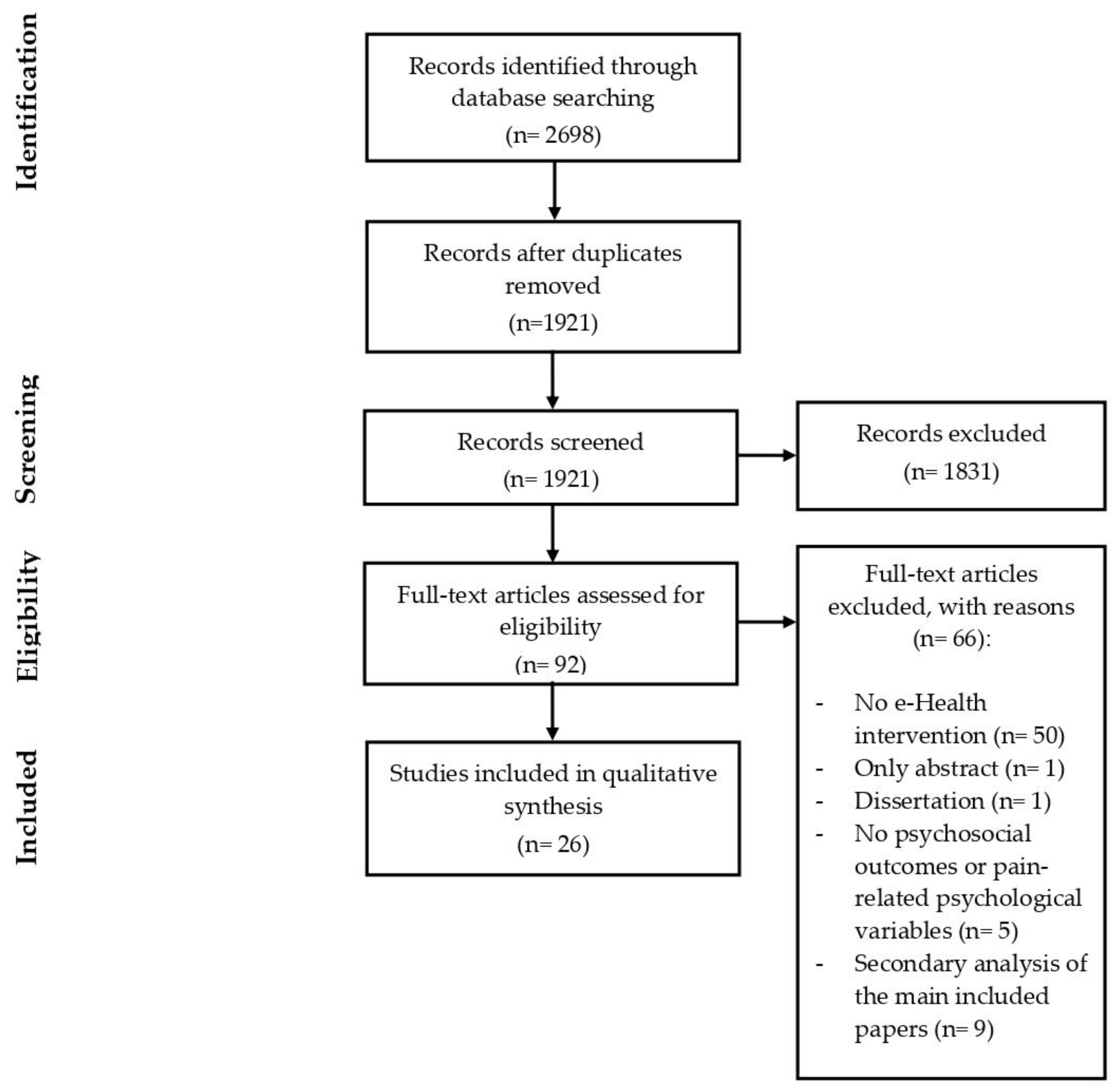
3.1. Study Selection
3.2. Characteristics of the Included Studies
3.3. Selected Populations in the Included Studies
3.4. Risk of Bias Assessment
3.5. e-Health Interventions for Patients with FMS
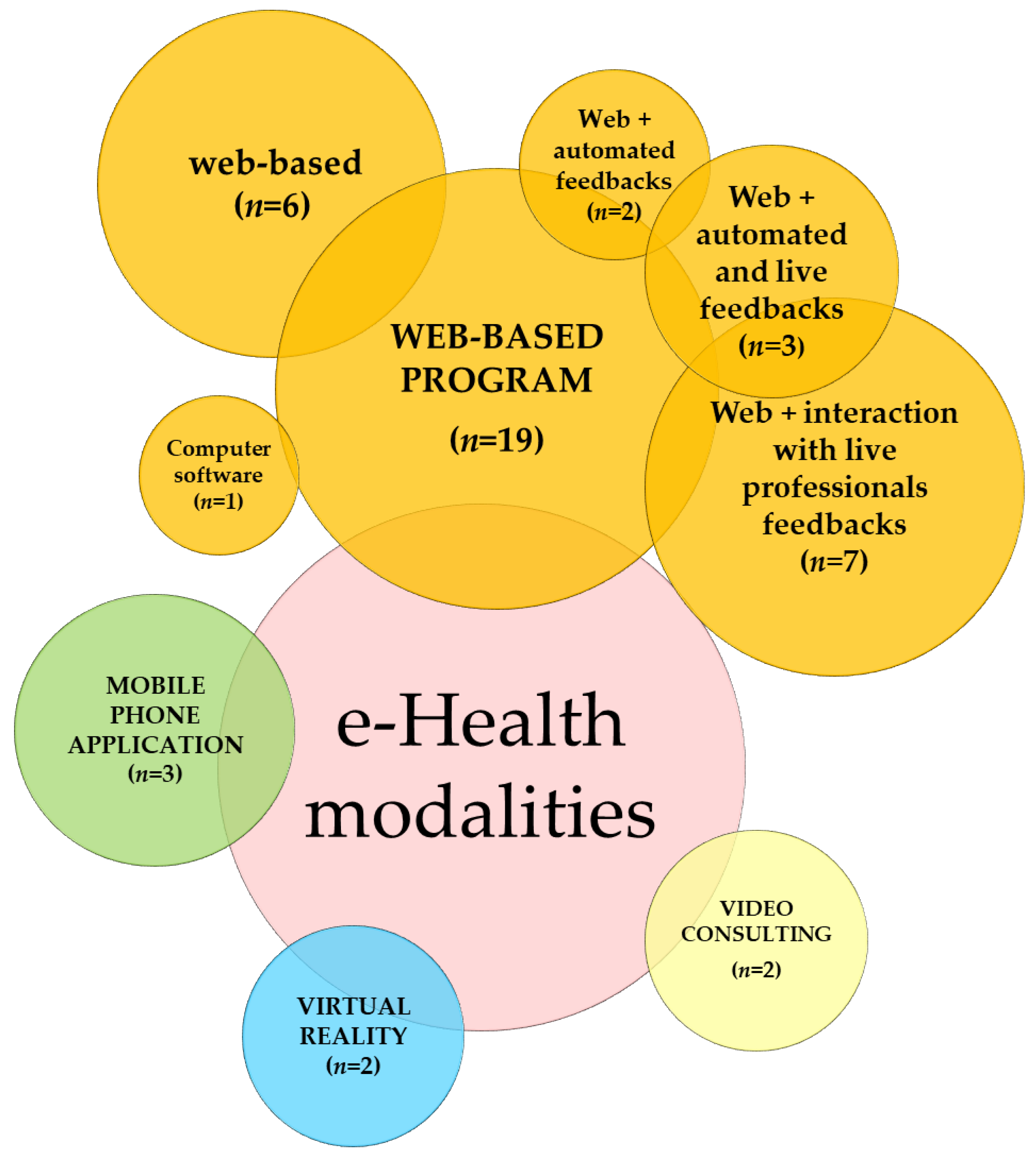
3.5.1. e-Health Modalities
3.5.2. Main Psychological Approaches and Strategies at the Basis of the Interventions
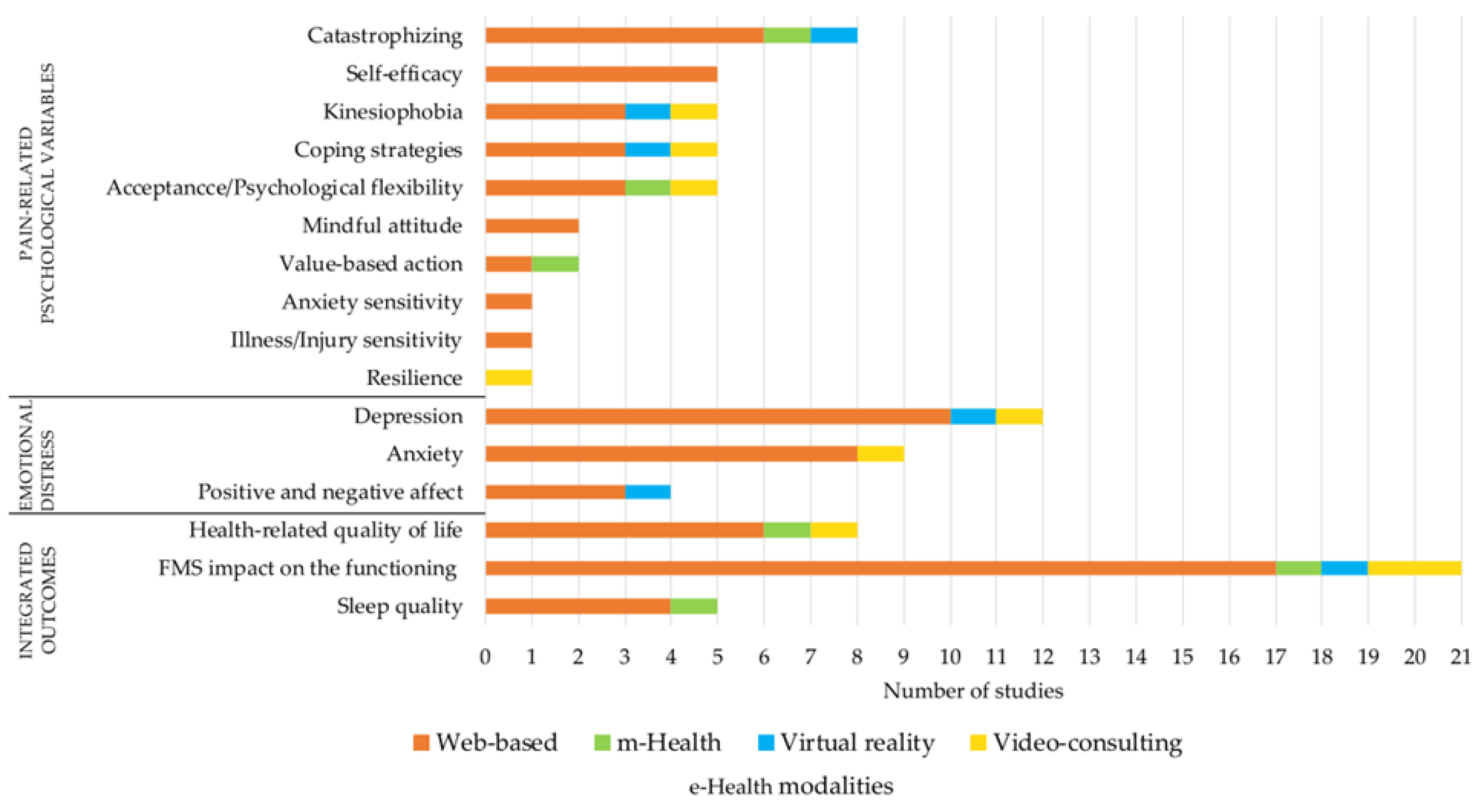
3.5.3. Psychosocial Outcomes and Pain-Related Psychological Variables Targeted by the e-Health Interventions
3.5.4. Signals of Efficacy of the e-Health Interventions
3.5.5. Feasibility and Acceptability of the e-Health Interventions
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- 1
- exp Telemedicine/ 11461
- 2
- telehealth.mp. 3071
- 3
- tele-medicine.mp. 23
- 4
- tele-health.mp. 83
- 5
- exp Mobile Health/or m-health.mp. 1929
- 6
- e-health.mp. or exp Electronic Health Services/ 15797
- 7
- ehealth.mp. 1550
- 8
- exp Internet/ 31104
- 9
- exp Websites/or web.mp. 45424
- 10
- online.mp. or exp Online Therapy/117795
- 11
- app.mp. 8414
- 12
- exp Computers/or computer.mp. 175508
- 13
- exp Technology/or exp Virtual Reality/ 257342
- 14
- exp Augmented Reality/ 80415 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 427776
- 16
- fibromyalgia.mp. 3798
- 17
- fibrositis.mp. 44
- 18
- FMS.mp. 1089
- 19
- 16 or 17 or 18 4373
- 20
- 15 and 19 314
Appendix B

{kind=link}
{kind=link}
{kind=link}
| First Author—Year of Publication | Type of Study | Participants (N; Type of Health Condition) | Age (M ± SD); Gender (% Female) | Psychiatric Diagnosis (I = Included/ E = Excluded; Type) | Summary of Intervention Characteristics | Outcomes (psy = Psychological/phy = Physical/int = Integrated/Other) | Outcome Measures | Follow-Up | Type of Control Group |
|---|---|---|---|---|---|---|---|---|---|
| Lorig et al. [28] | RCT | 885 patients with arthritis, 51.6% patients with FMS | Intervention group = 52.2 ± 10.9; 89.8% Control group = 52.2 ± 12.2; 90.5% | Not specified | Self-management program delivered via a website | Psy = health distress; self-efficacy Phy = pain and fatigue; disability; aerobic exercise; stretching and strengthening exercise; practice of stress management; and communication with physicians; physician visits; emergency room visits; chiropractic visits; physical therapist visits and nights in hospital Int = global health; activity limitation | Psy = HDS; ASES Int = SGHS; ALS | 1 year | Standard care |
| Williams et al. [29] | RCT | 118 patients with FMS | 50.5 ± 11.5; 95% | I (axis I and II psychiatric diagnoses) E (any present psychiatric disorder involving a history of psychosis, current suicide risk, or substance abuse) | Self-management program delivered via a website | Psy = mood; anxiety Phy = physical functional status; pain intensity; fatigue; sleep Other = patient global impression of change | Psy = CES-D; STPI | // | Standard care |
| Morris et al. [30] | Study protocol Secondary study [22]: exploratory, case-controlled study | 20 patients with FMS Secondary study: 13 patients with FMS | >18; male and female Secondary study: Intervention group: 46.0 ± 9.7; 100% Control group: 48.2 ± 14.8; 100% | E (previous hospitalization for a major psychiatric disorder; current or previous abuse of any illicit substances or alcohol) Secondary study: E (psychological/psychiatric disorders; previous hospitalization for a major psychiatric disorder; or current or previous abuse of any illicit substances or alcohol) | Exposure therapy program delivered through virtual reality (VR) | Psy = pain catastrophizing; fear-avoidance behaviors/kinesiophobia Phy = neurophysiological changes Secondary study: Psy = pain catastrophizing; kinesiophobia Phy = pain severity; physical activity levels; neurophysiological observations Int = impact of FMS | Psy = PCS; TSK | // | // Secondary study: matched control group (healthy subjects) |
| Kristjánsdóttir et al. [31] | RCT | 140 patients with chronic widespread pain Intervention group = 80.9% patients with FMS Control group = 84.4% patients with FMS | Intervention group = 44.6 ± 11.1; 100% Control group = 43.8 ± 11.2; 100% | E (severe psychiatric disorder) | ACT intervention delivered via a mobile software | Psy = pain catastrophizing; acceptance of pain; emotional distress Phy = current level of pain; fatigue and sleep Int = impact of FMS on functioning and symptom level | Psy = PCS; CPAQ; CPVI; GHQ Int = FIQ | 5 months 11 months (secondary study [19]) | 4-week inpatient rehabilitation program (as the intervention group) without smartphone intervention |
| Botella et al. [32] | Pilot study (pre/post-test) Secondary studies: (a) pilot pre/post-test study [20] (b) RCT [21] | 6 patients with FMS Secondary studies: (a) 40 patients with FMS (b) 61 patients with FMS | 55 ± 7.6; 100% Secondary studies: (a) 48.8 ± 9.3; 100% (b) 50.5 ± 9.8; 100% | I (mood disorder in remission) E (severe psychiatric disorders) Secondary studies: (a) I (diagnosis of anxiety disorder and depressive disorder) E (severe psychiatric disorders) (b) I (mood or anxiety disorders in remission) E (severe psychiatric disorders) | In-person CBT + virtual reality (VR) | Psy = depression; negative and positive affect; coping skills Int = functional status related to pain Secondary studies: (a) Psy = mood state; motivation and sense of self-efficacy regarding specific activities; intensity of different emotions Phy = pain and fatigue intensity Other = acceptability and satisfaction regarding the VR (b) Psy = coping; mood Phy = pain intensity and interference Int = disability; perceived quality of life Other = acceptability and satisfaction regarding the treatment program | Psy = CPCI; BDI-II; PANAS Int = FIQ Secondary studies: (a) Psy = ad hoc NRS (b) Psy = CPCI; BDI-II Int = FIQ; QLI-Sp | 6 months | // Secondary study: (b) standard care |
| Camerini et al. [33] | Cross-sectional study | 209 patients with FMS | 49 ± 10.0; 95% | Not specified | Self-management education intervention delivered via a website | Int = FMS impact Other = usage of website applications; knowledge about FMS; self-management | Int = FIQ | // | // |
| Davis & Zautra [34] | RCT | 79 patients with FMS | 46.1; 98% | E (history of more than five past episodes of depression) | Mindfulness-based socioemotional regulation intervention delivered via Adobe Presenter | Psy = pain-coping efficacy; positive and negative affect; perceived social relations Phy = pain. Int = pre-intervention functional health | Psy = PANAS; ad hoc online diaries Int = FIQ | // | Health tips attention control (12 modules of health behavior information) |
| Menga et al. [35] | RCT | 56 patients with FMS | 55; 88% | I (mild-to-moderate depression and anxiety) E (severe depression or other severe psychiatric disorders) | CBT and interpersonal-therapy-based program delivered via a website | Phy = change in tender point assessment Int = FIQ composite score | Int = FIQ | 12 weeks | Standard care |
| Ljótsson et al. [36] | Open trial—pilot study | 41 patients with FMS | 52 ± 0.9; 100% | E (severe psychiatric disorders) | Acceptance and values-based exposure treatment delivered via a website | Psy = depression; anxiety; psychological flexibility Int = FMS symptoms and impact; disability; health-related quality of life; impact and severity of fatigue Other = health-related costs | Psy = HADS; PIPS Int = FIQ; SF-12; FSS | 6 months | // |
| Vallejo et al. [37] | RCT | 60 patients with FMS | 51.6 ± 9.9; 100% | E (diagnosis of mental health disorders; suicidal ideation) | CBT delivered via a web application | Psy = general psychological distress; depression; catastrophizing; pain self-efficacy; coping Int = global impact of FMS | Psy = HADS; BDI; PCS; CPSS; CPCI Int = FIQ | 3, 6, and 12 months (iCBT and CBT groups) | Waiting list (standard care) CBT (face-to-face setting) |
| Sparks et al. [38] | Pilot study—descriptive design | 35 patients with FMS | 51.1 ± 11.4; 91.4% | E (suicidal and homicidal tendencies) | Psychoeducation intervention delivered via DVD format or USB flash drives | Int = overall impact of FMS Other = time spent and modules reviewed in the program; participants perceptions about the program | Int = FIQR | // | // |
| Friesen et al. [39] | RCT | 60 patients with FMS | 48 ± 11; (95%) | I (at least mild symptoms of depression or anxiety) | Self-management program delivered via a website | Psy = symptoms of generalized anxiety disorder; symptoms of major depressive disorder, anxiety and depression; pain self-efficacy; pain-related cognitions; fear of movement and re-injury Phy = pain severity and interference Int = FM severity and symptomology, severity and impact of fatigue; health-related quality of life Other = treatment acceptability and satisfaction | Psy = HADS; PSEQ; PRSS; TSK Int = FIQR; FSI; SF-12 | 4 weeks (intervention group only) | Waiting list (standard care) |
| de la Vega et al. [40] | Feasibility study Secondary study [25]: pilot study | Three patients with FMS (feasibility testing) Secondary study: 100 patients with FMS | FMS patients = 15, 21, and 24 years old; 100%. Secondary study: 49.8 ± 10; 94% | Not specified | CBT intervention delivered via a smartphone app | Other = app usability, feasibility and acceptability Secondary study: Psy = anxiety; depression Phy = pain severity; fatigue Int = sleep quality Other = use and satisfaction with the app | Secondary study: PROMIS Psy = Int = PSQI | // Secondary study: 3 months | // |
| Molinari et al. [41] | RCT | 71 patients with FMS | 51.1 ± 10.5; 100% | E (severe psychiatric disorders) | Positive future-thinking intervention through the use of an app and a web platform | Psy = depression and mood; negative and positive affect; optimism and future expectancies; self-efficacy; pain catastrophizing Int = quality of life; FMS interference with daily life | Psy = BDI-II; PANAS; LOT-R; GSES-12; PCS Int = QLI-Sp; FIQ-R | 1 and 3 months | Active control group (daily Activities) |
| Yuan & Marques [42] | Technical report Secondary study: randomized, parallel trial [24] | 15 patients with FMS Secondary study: 40 patients with FMS | Age range: 27–59; 32–72 Secondary study: 43.0 ± 10.1 Intervention group = 95% Control group = 100% | Not specified Secondary study: E (severe psychiatric disorders) | Multicomponent intervention (psychoeducation, CBT strategies, physical activity) delivered via a smartphone app | Other = app usability, communicability and applicability Secondary study: Int = health-related quality of life; self-care agency Phy = pain; severity of symptoms | Secondary study: Int = FIQ-R; ASAS-R | // | // Secondary study: paper book group |
| Simister et al. [43] | RCT | 67 patients with FMS | 39.7 ± 9.4; 95% | E (severe psychiatric disorders) | ACT intervention delivered via a web platform | Psy = pain-related acceptance; depression; mindfulness; cognitive fusion; valued living; kinesiophobia; pain catastrophizing Phy = pain intensity; functioning/physical ability Int = = FMS impact, sleep quality | Psy = CPAQ-R; CES-D; FFMQ; CFQ; VLQ; TSK-11; PCS Int = FIQ-R; PSQI | 3 months | Standard care |
| Hedman-Lagerlöf et al. [44] | RCT Secondary studies: mediation analysis using data from the RCT [23]; [26] | 140 patients with FMS | 50.3 ± 10.9 | I (previous or concurrent psychiatric disorder/s) E (psychosis, severe depression, suicidal ideation, or ongoing alcohol or substance abuse or dependency) | Exposure therapy delivered via a web platform | Psy = depressive symptoms; general anxiety symptoms; insomnia; pain-related distress; pain-related avoidance patterns Int = severity and impact of FM symptoms; fatigue; general disability; quality of life Other = global improvement | Psy = PHQ-9; GAD-7; ISI; PRS; FFMQ-NR; PIPS Int = FIQ; FSS; WHO-DAS II; BBQ | 6 months 12 months | Waiting list |
| Friedberg et al. [45] | Mixed-methods study | 29 patients with FMS | 45.4 ± 12.1; 96.6% | E (severe psychiatric disorders) | Bilateral stimulation and desensitization intervention involving the use of video and audio files and an online diary | Psy = pain catastrophizing Int = pain severity and impact on daily functioning; effect of fatigue on functioning Other = participant feedback | Psy = PCS Int = BPI-SF; FSS | 3 and 6 months | Waiting list |
| Collinge et al. [46] | Longitudinal observational Study | 76 patients with FMS | 47 ± 12; 99% | Not specified | Self-management program delivered via a website | Int = impact of FM Other = cumulative counts of the number of healthy diaries completed and of profiles produced for each subject | Int = FIQ | // | // |
| Carleton et al. [47] | RCT | 117 patients with FMS | Intervention group = 47.9 ± 10.8; 100% Control group = 48 ± 11.9; 100% | I (clinically significant symptoms of depression or anxiety, so long as fibromyalgia was the primary complaint) E (severe psychiatric disorders) | Attention bias modification (ABM) program administered through computer | Psy = anxiety sensitivity; symptoms of depression, anxiety and stress; fears of illness and injury Int = pain experience; FMS impact | Psy = ASI-3; DASS-21; PASS-20; ISI-R Int = SF-MPQ; FIQ-R | 1 months | Active control group (task similar to ABM group) |
| Climent-Sanz et al. [48] | Study protocol | Patients with FMS | Age range = 18-65; 100% | // | Therapeutic patient education intervention delivered via a website | Psy = pain catastrophizing; chronic pain self-efficacy Phy = pain intensity Int = sleep quality; dysfunctional beliefs and attitudes about sleep; health status and quality of life associated with FMS | Psy = PCS; CPSS Int = PSQI; DBAS; FIQ-R | // | Active control group (video + written materials about FMS) |
| Serrat et al. [49] | RCT Secondary study: study protocol of an RCT [27] | 151 patients with FMS Secondary study: 225 with FMS | 54.4 ± 8.7 Intervention group = 94.7% Control group = 92.1% Secondary study: age range: 18-65 | I (mild anxiety and depressive symptoms) Secondary study: E (severe psychiatric disorders) | Multicomponent intervention (therapeutic exercise, pain neuroscience education, CBT, and mindfulness training) delivered via online video | Psy = kinesiophobia, anxiety and depressive symptomatology Phy = physical functioning Int = functional impairment Secondary study: Psy = anxiety and depressive symptomatology; stress; pain catastrophizing; psychological inflexibility; kinesiophobia Phy = pain; fatigue; physical functioning; central sensitization symptoms; physiological markers Int = FMS impact; sleep quality; health-related quality of life Other: cognitive functioning; pain neurophysiology knowledge; cost–utility measures; treatment credibility/expectancy; global impression of change | Psy = TSK; HADS Int = FIQ-R Secondary study: Psy = HADS; PSS; PCS; PIPS; TSK Int = FIQ-R; B-PSQI; EuroQoL-5D-5L | // Secondary study: 6-months follow-up | Standard care Secondary study: (a) standard care; (b) in-person multicomponent intervention + standard care |
| García-Perea et al. [50] | RCT | 80 patients with FMS | 97,5% Intervention group = 55.5 ± 4.1 Control Group = 53.3 ± 7.5 | Not specified | Self-management education intervention delivered via a web platform | Int = perceived state of health; quality of life in relation to health | Int = FIQ; SF-36 | 6 months 12 months | Two face-to-face consultations |
| de la Coba et al. [51] | Feasibility and preliminary effectiveness study | Nine patients with FMS | 50.1 ± 5; 100% | E (severe psychiatric disorders) | ACT intervention delivered via online video-meeting sessions | Psy = emotional component of pain; anxiety and depression; experiential avoidance; cognitive fusion; pain acceptance; psychological inflexibility Phy = clinical pain Int = severity of FM impact | Psy = MPQ-E; HAS; HDS; AAQ-II; CFQ; CPAQ; PIPS Int = FIQ | 6 months | // |
| Ong et al. [52] | Study protocol | 90 patients with FMS | ≥50 years | E (moderate or severe cognitive impairment) | Positive affect skills-building intervention program delivered via a website | Psy = positive and negative affect; depressive symptoms; stressor appraisals; daily positive and negative affect; daily stressors Phy = physical functioning Int = pain intensity and pain interference Other = feasibility and acceptability of the program | Psy = PANAS; CESD-R-10; PSS; m-DES; DISE Int = PROMIS-SI; PROMIS-PI | 1 month | Active control group (completing daily emotion reports) |
| Paolucci et al. [53] | Longitudinal observational Study | 28 patients with FMS | 56.6 ± 8.6; 100% | E (severe psychiatric disorders; major neurological problems) | Mind–body intervention delivered via online video-meeting sessions | Psy = fear of movement; resilience; coping ability Phy = pain Int = effect of fatigue on functioning; FMS impact; health-related quality of life | Psy = FABQ; RSA; CSQR Int = FAS; FIQ; SF-12 | 1 month | // |
References
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Häuser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. 2016 Revisions to the 2010/2011 Fibromyalgia Diagnostic Criteria. Semin. Arthritis Rheum. 2016, 46, 319–329. [Google Scholar] [CrossRef]
- Fernandez-Feijoo, F.; Samartin Veiga, N.; Carrillo de la Peña, M.T. Quality of life in patients with fibromyalgia: Contributions of disease symptoms, lifestyle and multi-medication. Front. Psychol. 2022, 13, 924405. [Google Scholar] [CrossRef] [PubMed]
- Drozd, M.; Marzęda, M.; Blicharz, A.; Czarnota, J.; Piecewicz-Szczęsna, H. Unclear etiology and current hypotheses of the pathogenesis of fibromyalgia. J. Educ. Health Sport. 2020, 10, 338–344. [Google Scholar] [CrossRef]
- Albajes, K.; Moix, J. Psychological interventions in fibromyalgia: An updated systematic review. Mediterr. J. Clin. Psychol. 2021, 9, 338–344. [Google Scholar]
- Pasini, I.; Perlini, C.; Donisi, V.; Mason, A.; Schweiger, V.; Secchettin, E.; Lugoboni, F.; Valenza, G.; Del Piccolo, L. “INTEGRO INTEGRated Psychotherapeutic InterventiOn” on the Management of Chronic Pain in Patients with Fibromyalgia: The Role of the Therapeutic Relationship. Int. J. Environ. Res. Public Health 2023, 20, 3973. [Google Scholar] [CrossRef] [PubMed]
- Bernardy, K.; Klose, P.; Welsch, P.; Häuser, W. Efficacy, acceptability and safety of cognitive behavioural therapies in fibromyalgia syndrome—A systematic review and meta-analysis of randomized controlled trials. Eur. J. Pain 2018, 22, 242–260. [Google Scholar] [CrossRef]
- Perlini, C.; Donisi, V.; Del Piccolo, L. From research to clinical practice: A systematic review of the implementation of psychological interventions for chronic headache in adults. BMC Health Serv. Res. 2020, 20, 459. [Google Scholar] [CrossRef]
- WHO. WHO Guideline: Recommendations on Digital Interventions for Health System Strengthening: Web Supplement 2: Summary of Findings and GRADE Tables; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Williams, G.A.; Fahy, N.; Aissat, D.; Lenormand, M.-C.; Stüwe, L.; Zablit-Schmidt, I.; Delafuys, S.; Le Douarin, Y.-M.; Muscat, N.A. COVID-19 and the use of digital health tools: Opportunity amid crisis that could transform health care delivery. Eurohealth 2022, 28, 1. [Google Scholar]
- Eysenbach, G. What is e-health? J. Med. Internet Res. 2001, 3, e833. [Google Scholar] [CrossRef]
- Slattery, B.W.; Haugh, S.; O’Connor, L.; Francis, K.; Dwyer, C.P.; O’Higgins, S.; Egan, J.; McGuire, B.E. An evaluation of the effectiveness of the modalities used to deliver electronic health interventions for chronic pain: Systematic review with network meta-analysis. J. Med. Internet Res. 2019, 21, e11086. [Google Scholar] [CrossRef]
- Goudman, L.; Jansen, J.; Billot, M.; Vets, N.; De Smedt, A.; Roulaud, M.; Rigoard, P.; Moens, M. Virtual reality applications in chronic pain management: Systematic review and meta-analysis. JMIR Ser. Games 2022, 10, e34402. [Google Scholar] [CrossRef] [PubMed]
- Eccleston, C.; Fisher, E.; Craig, L.; Duggan, G.B.; Rosser, B.A.; Keogh, E. Psychological therapies (Internet-delivered) for the management of chronic pain in adults. Cochrane Database Syst. Rev. 2014, 2. [Google Scholar] [CrossRef]
- Buhrman, M.; Gordh, T.; Andersson, G. Internet interventions for chronic pain including headache: A systematic review. Internet Interv. 2016, 4, 17–34. [Google Scholar] [CrossRef]
- Bernardy, K.; Klose, P.; Welsch, P.; Häuser, W. Efficacy, acceptability and safety of internet-delivered psychological therapies for fibromyalgia syndrome: A systematic review and meta-analysis of randomized controlled trials. Eur. J. Pain 2019, 23, 3–14. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Sirriyeh, R.; Lawton, R.; Gardner, P.; Armitage, G. Reviewing studies with diverse designs: The development and evaluation of a new tool. J. Eval. Clin. Pract. 2012, 18, 746–752. [Google Scholar] [CrossRef] [PubMed]
- Kristjánsdóttir, Ó.B.; Fors, E.A.; Eide, E.; Finset, A.; Stensrud, T.L.; van Dulmen, S.; Wigers, S.H.; Eide, H. A smartphone-based intervention with diaries and therapist feedback to reduce catastrophizing and increase functioning in women with chronic widespread pain. part 2: 11-month follow-up results of a randomized trial. J. Med. Internet Res. 2013, 15, e2442. [Google Scholar] [CrossRef] [PubMed]
- Herrero, R.; García-Palacios, A.; Castilla, D.; Molinari, G.; Botella, C. Virtual reality for the induction of positive emotions in the treatment of fibromyalgia: A pilot study over acceptability, satisfaction, and the effect of virtual reality on mood. Cyberpsychol. Behav. Soc. Netw. 2014, 17, 379–384. [Google Scholar] [CrossRef]
- Díaz-García, A.; Herrero Camarano, R.; Vizcaíno, Y.; Belmonte, M.Á.; Castilla, D.; Molinari, G.; Baños, R.; Botella, C. Integrating Virtual Reality with Activity Management for the Treatment of Fibromyalgia Acceptability and Preliminary Efficacy. Clin. J. Pain 2015, 31, 564–572. [Google Scholar] [CrossRef]
- Morris, L.D.; Louw, Q.A.; Grimmer, K.A.; Meintjes, E. Targeting pain catastrophization in patients with fibromyalgia using virtual reality exposure therapy: A proof-of-concept study. J. Phys. Ther. Sci. 2015, 27, 3461–3467. [Google Scholar] [CrossRef]
- Hedman-Lagerlöf, M.; Andersson, E.; Hedman-Lagerlöf, E.; Wicksell, R.K.; Flink, I.; Ljótsson, B. Approach as a key for success: Reduced avoidance behaviour mediates the effect of exposure therapy for fibromyalgia. Behav. Res. Ther. 2019, 122, 103478. [Google Scholar] [CrossRef]
- Yuan, S.L.K.; Couto, L.A.; Marques, A.P. Effects of a six-week mobile app versus paper book intervention on quality of life, symptoms, and self-care in patients with fibromyalgia: A randomized parallel trial. Braz. J. Phys. Ther. 2021, 25, 428–436. [Google Scholar] [CrossRef]
- Miró, J.; Lleixà-Daga, M.; de la Vega, R.; Llorens-Vernet, P.; Jensen, M.P. A Mobile Application to Help Self-Manage Pain Severity, Anxiety, and Depressive Symptoms in Patients with Fibromyalgia Syndrome: A Pilot Study. Int. J. Environ. Res. Public Health 2022, 19, 12026. [Google Scholar] [CrossRef]
- Hedman-Lagerlöf, M.; Andersson, E.; Ljótsson, B.; Engelbrektsson, J.; Lundbäck, K.; Björkander, D.; Hedman-Lagerlöf, E.; Flink, I.; Axelsson, E. Effect moderators in Internet-based exposure therapy for fibromyalgia: The role of pain intensity. Eur. J. Pain 2023, 27, 507–517. [Google Scholar] [CrossRef]
- Serrat, M.; Ferrés, S.; Auer, W.; Almirall, M.; Lluch, E.; D’Amico, F.; Maes, M.; Lorente, S.; Navarrete, J.; Montero-Marín, J. Effectiveness, cost-utility and physiological underpinnings of the FIBROWALK multicomponent therapy in online and outdoor format in individuals with fibromyalgia: Study protocol of a randomized, controlled trial (On&Out study). Front. Physiol. 2022, 13, 2335. [Google Scholar]
- Lorig, K.R.; Ritter, P.L.; Laurent, D.D.; Plant, K. The internet-based arthritis self-management program: A one-year randomized trial for patients with arthritis or fibromyalgia. Arthritis Care Res. Off. J. Am. Coll. Rheumatol. 2008, 59, 1009–1017. [Google Scholar] [CrossRef]
- Williams, D.A.; Kuper, D.; Segar, M.; Mohan, N.; Sheth, M.; Clauw, D.J. Internet-enhanced management of fibromyalgia: A randomized controlled trial. PAIN 2010, 151, 694–702. [Google Scholar] [CrossRef]
- Morris, L.D.; Grimmer-Somers, K.A.; Spottiswoode, B.; Louw, Q.A. Virtual reality exposure therapy as treatment for pain catastrophizing in fibromyalgia patients: Proof-of-concept study (Study Protocol). BMC Musculoskelet. Disord. 2011, 12, 85. [Google Scholar] [CrossRef]
- Kristjánsdóttir, Ó.B.; Fors, E.A.; Eide, E.; Finset, A.; Stensrud, T.L.; van Dulmen, S.; Wigers, S.H.; Eide, H. A smartphone-based intervention with diaries and therapist-feedback to reduce catastrophizing and increase functioning in women with chronic widespread pain: Randomized controlled trial. J. Med. Internet Res. 2013, 15, e5. [Google Scholar] [CrossRef]
- Botella, C.; Garcia-Palacios, A.; Vizcaíno, Y.; Herrero, R.; Baños, R.M.; Belmonte, M.A. Virtual reality in the treatment of fibromyalgia: A pilot study. Cyberpsychol. Behav. Soc. Netw. 2013, 16, 215–223. [Google Scholar] [CrossRef]
- Camerini, L.; Camerini, A.-L.; Schulz, P.J. Do participation and personalization matter? A model-driven evaluation of an Internet-based patient education intervention for fibromyalgia patients. Patient Educ. Couns. 2013, 92, 229–234. [Google Scholar] [CrossRef]
- Davis, M.C.; Zautra, A.J. An online mindfulness intervention targeting socioemotional regulation in fibromyalgia: Results of a randomized controlled trial. Ann. Behav. Med. 2013, 46, 273–284. [Google Scholar] [CrossRef]
- Menga, G.; Ing, S.; Khan, O.; Dupre, B.; Dornelles, A.C.; Alarakhia, A.; Davis, W.; Zakem, J.; Webb-Detiege, T.; Scopelitis, E. Fibromyalgia: Can online cognitive behavioral therapy help? Ochsner J. 2014, 14, 343–349. [Google Scholar]
- Ljótsson, B.; Atterlöf, E.; Lagerlöf, M.; Andersson, E.; Jernelöv, S.; Hedman, E.; Kemani, M.; Wicksell, R.K. Internet-delivered acceptance and values-based exposure treatment for fibromyalgia: A pilot study. Cogn. Behav. Ther. 2014, 43, 93–104. [Google Scholar] [CrossRef]
- Vallejo, M.A.; Ortega, J.; Rivera, J.; Comeche, M.I.; Vallejo-Slocker, L. Internet versus face-to-face group cognitive-behavioral therapy for fibromyalgia: A randomized control trial. J. Psychiatr. Res. 2015, 68, 106–113. [Google Scholar] [CrossRef]
- Sparks, T.; Kawi, J.; Menzel, N.N.; Hartley, K. Implementation of health information technology in routine care for fibromyalgia: Pilot study. Pain Manag. Nurs. 2016, 17, 54–62. [Google Scholar] [CrossRef]
- Friesen, L.N.; Hadjistavropoulos, H.D.; Schneider, L.H.; Alberts, N.M.; Titov, N.; Dear, B.F. Examination of an internet-delivered cognitive behavioural pain management course for adults with fibromyalgia: A randomized controlled trial. Pain 2017, 158, 593–604. [Google Scholar] [CrossRef]
- de la Vega, R.; Roset, R.; Galan, S.; Miro, J. Fibroline: A mobile app for improving the quality of life of young people with fibromyalgia. J. Health Psychol. 2018, 23, 67–78. [Google Scholar] [CrossRef]
- Molinari, G.; Garcia-Palacios, A.; Enrique, A.; Roca, P.; Fernandez-Llanio Comella, N.; Botella, C. The power of visualization: Back to the future for pain management in fibromyalgia syndrome. Pain Med. 2018, 19, 1451–1468. [Google Scholar] [CrossRef]
- Yuan, S.L.K.; Marques, A.P. Development of ProFibro—A mobile application to promote self-care in patients with fibromyalgia. Physiotherapy 2018, 104, 311–317. [Google Scholar] [CrossRef]
- Simister, H.D.; Tkachuk, G.A.; Shay, B.L.; Vincent, N.; Pear, J.J.; Skrabek, R.Q. Randomized controlled trial of online acceptance and commitment therapy for fibromyalgia. J. Pain 2018, 19, 741–753. [Google Scholar] [CrossRef]
- Hedman-Lagerlöf, M.; Hedman-Lagerlöf, E.; Axelsson, E.; Ljótsson, B.; Engelbrektsson, J.; Hultkrantz, S.; Lundbäck, K.; Björkander, D.; Wicksell, R.K.; Flink, I. Internet-delivered exposure therapy for fibromyalgia. Clin. J. Pain 2018, 34, 532–542. [Google Scholar] [CrossRef]
- Friedberg, F.; Adamowicz, J.L.; Caikauskaite, I. Home-based pain and fatigue management in fibromyalgia: Feasibility of a new intervention. Fatigue Biomed. Health Behav. 2019, 7, 153–165. [Google Scholar] [CrossRef]
- Collinge, W.; Soltysik, R.; Yarnold, P. Fibromyalgia impact reduction using online personal health informatics: Longitudinal observational study. J. Med. Internet Res. 2020, 22, e15819. [Google Scholar] [CrossRef]
- Carleton, R.N.; Asmundson, G.J.; Korol, S.L.; LeBouthillier, D.M.; Hozempa, K.; Katz, J.D.; Vlaeyen, J.W.; Crombez, G. Evaluating the efficacy of an attention modification program for patients with fibromyalgia: A randomized controlled trial. Pain 2020, 161, 584–594. [Google Scholar] [CrossRef]
- Climent-Sanz, C.; Gea-Sánchez, M.; Moreno-Casbas, M.T.; Blanco-Blanco, J.; García-Martínez, E.; Valenzuela-Pascual, F. A web-based therapeutic patient education intervention for pain and sleep for women with fibromyalgia: A sequential exploratory mixed-methods research protocol. J. Adv. Nurs. 2020, 76, 1425–1435. [Google Scholar] [CrossRef]
- Serrat, M.; Coll-Omaña, M.; Albajes, K.; Solé, S.; Almirall, M.; Luciano, J.V.; Feliu-Soler, A. Efficacy of the FIBROWALK multicomponent program moved to a virtual setting for patients with fibromyalgia during the COVID-19 pandemic: A proof-of-concept RCT performed alongside the state of alarm in Spain. Int. J. Environ. Res. Public Health 2021, 18, 10300. [Google Scholar] [CrossRef]
- García-Perea, E.; Pedraz-Marcos, A.; Martínez-Rodríguez, S.H.; Otones-Reyes, P.; Palmar-Santos, A.M. Effectiveness of a Fibromyalgia Online Nursing Consultation in the Quality of Life: A Randomized Controlled Trial. Pain Manag. Nurs. 2022, 23, 478–485. [Google Scholar] [CrossRef]
- De la Coba, P.; Rodríguez-Valverde, M.; Hernández-López, M. Online ACT intervention for fibromyalgia: An exploratory study of feasibility and preliminary effectiveness with smartphone-delivered experiential sampling assessment. Internet Interv. 2022, 29, 100561. [Google Scholar] [CrossRef]
- Ong, A.D.; Moskowitz, J.T.; Wethington, E.; Addington, E.L.; Sanni, M.; Goktas, S.; Sluys, E.; Swong, S.; Kim, P.; Reid, M.C. Lessons in Affect Regulation to Keep Stress and Pain UndeR control (LARKSPUR): Design of a randomized controlled trial to increase positive affect in middle-aged and older adults with fibromyalgia. Contemp. Clin. Trials 2022, 120, 106880. [Google Scholar] [CrossRef] [PubMed]
- Paolucci, T.; de Sire, A.; Ferrillo, M.; di Fabio, D.; Molluso, A.; Patruno, A.; Pesce, M.; Lai, C.; Ciacchella, C.; Saggino, A. Telerehabilitation proposal of mind-body technique for physical and psychological outcomes in patients with fibromyalgia. Front. Physiol. 2022, 13, 1664. [Google Scholar] [CrossRef]
- Wolfe, F.; Smythe, H.A.; Yunus, M.B.; Bennett, R.M.; Bombardier, C.; Goldenberg, D.L.; Tugwell, P.; Campbell, S.M.; Abeles, M.; Clark, P. The American College of Rheumatology 1990 criteria for the classification of fibromyalgia. Arthritis Rheum. Off. J. Am. Coll. Rheumatol. 1990, 33, 160–172. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.-A.; Goldenberg, D.L.; Häuser, W.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B. Fibromyalgia criteria and severity scales for clinical and epidemiological studies: A modification of the ACR Preliminary Diagnostic Criteria for Fibromyalgia. J. Rheumatol. 2011, 38, 1113–1122. [Google Scholar] [CrossRef] [PubMed]
- Barello, S.; Triberti, S.; Graffigna, G.; Libreri, C.; Serino, S.; Hibbard, J.; Riva, G. eHealth for patient engagement: A systematic review. Front. Psychol. 2016, 6, 2013. [Google Scholar] [CrossRef]
- Donisi, V.; Gajofatto, A.; Mazzi, M.A.; Gobbin, F.; Busch, I.M.; Ghellere, A.; Klonova, A.; Rudi, D.; Vitali, F.; Schena, F. A bio-psycho-social co-created intervention for young adults with multiple sclerosis (ESPRIMO): Rationale and study protocol for a feasibility study. Front. Psychol. 2021, 12, 215. [Google Scholar] [CrossRef]
- Eyles, H.; Jull, A.; Dobson, R.; Firestone, R.; Whittaker, R.; Te Morenga, L.; Goodwin, D.; Mhurchu, C.N. Co-design of mHealth delivered interventions: A systematic review to assess key methods and processes. Curr. Nutr. Rep. 2016, 5, 160–167. [Google Scholar] [CrossRef]
- Botti, A.; Monda, A. Sustainable value co-creation and digital health: The case of trentino eHealth ecosystem. Sustainability 2020, 12, 5263. [Google Scholar] [CrossRef]
- Jones, G.T.; Atzeni, F.; Beasley, M.; Flüß, E.; Sarzi-Puttini, P.; Macfarlane, G.J. The prevalence of fibromyalgia in the general population: A comparison of the American College of Rheumatology 1990, 2010, and modified 2010 classification criteria. Arthritis Rheumatol. 2015, 67, 568–575. [Google Scholar] [CrossRef]
- Conversano, C.; Ciacchini, R.; Orru, G.; Bazzichi, M.L.; Gemignani, A.; Miniati, M. Gender differences on psychological factors in fibromyalgia: A systematic review on male’s experience. Clin. Exp. Rheumatol. 2020, 2, 174–185. [Google Scholar] [CrossRef]
- Martini, A.; Schweiger, V.; Del Balzo, G.; Sartori, G.; Parolini, M.; Chinellato, E.; Sarzi-Puttini, P.; Polati, E. Epidemiological, pharmacological and sociodemographic characterisation of a population of 386 fibromyalgic patients referred to a tertiary pain centre in Italy. Clin. Exp. Rheumatol. 2019, 37 (Suppl. S116), 27–38. [Google Scholar]
- Galvez-Sánchez, C.M.; Duschek, S.; Reyes Del Paso, G.A. Psychological impact of fibromyalgia: Current perspectives. Psychol. Res. Behav. Manag. 2019, 12, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Galvez-Sánchez, C.M.; Montoro, C.I.; Duschek, S.; Del Paso, G.A.R. Depression and trait-anxiety mediate the influence of clinical pain on health-related quality of life in fibromyalgia. J. Affect. Disord. 2020, 265, 486–495. [Google Scholar] [CrossRef]
- Sullivan, M.J.; Thorn, B.; Haythornthwaite, J.A.; Keefe, F.; Martin, M.; Bradley, L.A.; Lefebvre, J.C. Theoretical perspectives on the relation between catastrophizing and pain. Clin. J. Pain 2001, 17, 52–64. [Google Scholar] [CrossRef] [PubMed]
- Baastrup, S.; Schultz, R.; Brødsgaard, I.; Moore, R.; Jensen, T.S.; Vase Toft, L.; Bach, F.W.; Rosenberg, R.; Gormsen, L. A comparison of coping strategies in patients with fibromyalgia, chronic neuropathic pain, and pain-free controls. Scand. J. Psychol. 2016, 57, 516–522. [Google Scholar] [CrossRef] [PubMed]
- Conversano, C.; Marchi, L.; Rebecca, C.; Mirabelli, V.; Gemignani, A. Catastrophizing and fibromyalgia: A mini-review. J. Transl. Neurosci. 2018, 3, 7. [Google Scholar] [CrossRef]
- Jackson, T.; Wang, Y.; Wang, Y.; Fan, H. Self-efficacy and chronic pain outcomes: A meta-analytic review. J. Pain 2014, 15, 800–814. [Google Scholar] [CrossRef] [PubMed]
- Khan, K.; Hall, C.L.; Davies, E.B.; Hollis, C.; Glazebrook, C. The effectiveness of web-based interventions delivered to children and young people with neurodevelopmental disorders: Systematic review and meta-analysis. J. Med. Internet Res. 2019, 21, e13478. [Google Scholar] [CrossRef] [PubMed]
- Heapy, A.A.; Higgins, D.M.; Cervone, D.; Wandner, L.; Fenton, B.T.; Kerns, R.D. A systematic review of technology-assisted self-management interventions for chronic pain. Clin. J. Pain 2015, 31, 470–492. [Google Scholar] [CrossRef]
- White, V.; Linardon, J.; Stone, J.; Holmes-Truscott, E.; Olive, L.; Mikocka-Walus, A.; Hendrieckx, C.; Evans, S.; Speight, J. Online psychological interventions to reduce symptoms of depression, anxiety, and general distress in those with chronic health conditions: A systematic review and meta-analysis of randomized controlled trials. Psychol. Med. 2022, 52, 548–573. [Google Scholar] [CrossRef]
- Moman, R.N.; Dvorkin, J.; Pollard, E.M.; Wanderman, R.; Murad, M.H.; Warner, D.O.; Hooten, W.M. A systematic review and meta-analysis of unguided electronic and mobile health technologies for chronic pain—Is it time to start prescribing electronic health applications? Pain Med. 2019, 20, 2238–2255. [Google Scholar] [CrossRef] [PubMed]
- Ftouni, R.; AlJardali, B.; Hamdanieh, M.; Ftouni, L.; Salem, N. Challenges of Telemedicine during the COVID-19 pandemic: A systematic review. BMC Med. Inform. Decis. Mak. 2022, 22, 207. [Google Scholar] [CrossRef] [PubMed]
- Rhon, D.I.; Fritz, J.M.; Kerns, R.D.; McGeary, D.D.; Coleman, B.C.; Farrokhi, S.; Burgess, D.J.; Goertz, C.M.; Taylor, S.L.; Hoffmann, T. TIDieR-telehealth: Precision in reporting of telehealth interventions used in clinical trials-unique considerations for the Template for the Intervention Description and Replication (TIDieR) checklist. BMC Med. Res. Methodol. 2022, 22, 161. [Google Scholar] [CrossRef] [PubMed]
- Bond, F.W.; Hayes, S.C.; Baer, R.A.; Carpenter, K.M.; Guenole, N.; Orcutt, H.K.; Waltz, T.; Zettle, R.D. Preliminary psychometric properties of the Acceptance and Action Questionnaire–II: A revised measure of psychological inflexibility and experiential avoidance. Behav. Ther. 2011, 42, 676–688. [Google Scholar] [CrossRef] [PubMed]
- Lorig, K.; Stewart, A.; Ritter, P.; Gonzalez, V.; Lynch, J.; Laurent, D. Outcome Measures for Health Education and Other Health Care Interventions, 1st ed.; Sage: Thousand Oaks, CA, USA, 1996. [Google Scholar]
- Lorig, K.; Chastain, R.L.; Ung, E.; Shoor, S.; Holman, H.R. Development and evaluation of a scale to measure perceived self-efficacy in people with arthritis. Arthritis Rheum. Off. J. Am. Coll. Rheumatol. 1989, 32, 37–44. [Google Scholar] [CrossRef]
- Taylor, S.; Zvolensky, M.J.; Cox, B.J.; Deacon, B.; Heimberg, R.G.; Ledley, D.R.; Abramowitz, J.S.; Holaway, R.M.; Sandin, B.; Stewart, S.H. Robust dimensions of anxiety sensitivity: Development and initial validation of the Anxiety Sensitivity Index-3. Psychol. Assess. 2007, 19, 176. [Google Scholar] [CrossRef] [PubMed]
- Lindner, P.; Frykheden, O.; Forsström, D.; Andersson, E.; Ljótsson, B.; Hedman, E.; Andersson, G.; Carlbring, P. The Brunnsviken Brief Quality of life scale (BBQ): Development and psychometric evaluation. Cogn. Behav. Ther. 2016, 45, 182–195. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Bdi-ii Manual; The Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Cleeland, C. Measurement of pain by subjective report. Adv. Pain Res. Ther. 1989, 12, 391–403. [Google Scholar]
- Sancho-Domingo, C.; Carballo, J.L.; Coloma-Carmona, A.; Buysse, D.J. Brief version of the Pittsburgh Sleep Quality Index (B-PSQI) and measurement invariance across gender and age in a population-based sample. Psychol. Assess. 2021, 33, 111. [Google Scholar] [CrossRef]
- Hertzog, C.; Van Alstine, J.; Usala, P.D.; Hultsch, D.F.; Dixon, R. Measurement properties of the Center for Epidemiological Studies Depression Scale (CES-D) in older populations. Psychol. Assess. A J. Consult. Clin. Psychol. 1990, 2, 64. [Google Scholar] [CrossRef]
- Björgvinsson, T.; Kertz, S.J.; Bigda-Peyton, J.S.; McCoy, K.L.; Aderka, I.M. Psychometric properties of the CES-D-10 in a psychiatric sample. Assessment 2013, 20, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Gillanders, D.T.; Bolderston, H.; Bond, F.W.; Dempster, M.; Flaxman, P.E.; Campbell, L.; Kerr, S.; Tansey, L.; Noel, P.; Ferenbach, C. The development and initial validation of the cognitive fusion questionnaire. Behav. Ther. 2014, 45, 83–101. [Google Scholar] [CrossRef]
- McCracken, L.M.; Vowles, K.E.; Eccleston, C. Acceptance of chronic pain: Component analysis and a revised assessment method. Pain 2004, 107, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.P.; Turner, J.A.; Romano, J.M.; Strom, S.E. The chronic pain coping inventory: Development and preliminary validation. Pain 1995, 60, 203–216. [Google Scholar] [CrossRef] [PubMed]
- Anderson, K.O.; Dowds, B.N.; Pelletz, R.E.; Edwards, W.T.; Peeters-Asdourian, C. Development and initial validation of a scale to measure self-efficacy beliefs in patients with chronic pain. Pain 1995, 63, 77–83. [Google Scholar] [CrossRef] [PubMed]
- McCracken, L.M.; Yang, S.-Y. The role of values in a contextual cognitive-behavioral approach to chronic pain. Pain 2006, 123, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Monticone, M.; Ferrante, S.; Giorgi, I.; Galandra, C.; Rocca, B.; Foti, C. The 27-item coping strategies questionnaire—Revised: Confirmatory factor analysis, reliability and validity in italian-speaking subjects with chronic pain. Pain Res. Manag. 2014, 19, 153–158. [Google Scholar] [CrossRef]
- Antony, M.M.; Bieling, P.J.; Cox, B.J.; Enns, M.W.; Swinson, R.P. Psychometric properties of the 42-item and 21-item versions of the Depression Anxiety Stress Scales in clinical groups and a community sample. Psychol. Assess. 1998, 10, 176. [Google Scholar] [CrossRef]
- Morin, C. Dysfunctional beliefs and attitudes about sleep: Preliminary scale development and description. Behav. Ther. 1994, 17, 163. [Google Scholar]
- Almeida, D.M.; Wethington, E.; Kessler, R.C. The daily inventory of stressful events: An interview-based approach for measuring daily stressors. Assessment 2002, 9, 41–55. [Google Scholar] [CrossRef]
- Badia, X.; Roset, M.; Montserrat, S.; Herdman, M.; Segura, A. The Spanish version of EuroQol: A description and its applications. European Quality of Life scale. Med. Clin. 1999, 112, 79–85. [Google Scholar]
- Monticone, M.; Baiardi, P.; Bonetti, F.; Ferrari, S.; Foti, C.; Pillastrini, P.; Rocca, B.; Vanti, C.; Zanoli, G. The Italian version of the Fear-Avoidance Beliefs Questionnaire (FABQ-I): Cross-cultural adaptation, factor analysis, reliability, validity, and sensitivity to change. Spine 2012, 37, E374–E380. [Google Scholar] [CrossRef]
- De Vries, J.; Michielsen, H.; Van Heck, G.L.; Drent, M. Measuring fatigue in sarcoidosis: The Fatigue Assessment Scale (FAS). Br. J. Health Psychol. 2004, 9, 279–291. [Google Scholar] [CrossRef]
- Baer, R.A.; Smith, G.T.; Hopkins, J.; Krietemeyer, J.; Toney, L. Using self-report assessment methods to explore facets of mindfulness. Assessment 2006, 13, 27–45. [Google Scholar] [CrossRef]
- Burckhardt, C.S.; Clark, S.R.; Bennett, R.M. The fibromyalgia impact questionnaire: Development and validation. J. Rheumatol. 1991, 18, 728–733. [Google Scholar]
- Bennett, R.M.; Friend, R.; Jones, K.D.; Ward, R.; Han, B.K.; Ross, R.L. The revised fibromyalgia impact questionnaire (FIQR): Validation and psychometric properties. Arthritis Res. Ther. 2009, 11, R120. [Google Scholar] [CrossRef]
- Krupp, L.B.; LaRocca, N.G.; Muir-Nash, J.; Steinberg, A.D. The fatigue severity scale: Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch. Neurol. 1989, 46, 1121–1123. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef]
- Goldberg, D.P.; Gater, R.; Sartorius, N.; Ustun, T.B.; Piccinelli, M.; Gureje, O.; Rutter, C. The validity of two versions of the GHQ in the WHO study of mental illness in general health care. Psychol. Med. 1997, 27, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Bosscher, R.J.; Smit, J.H. Confirmatory factor analysis of the general self-efficacy scale. Behav. Res. Ther. 1998, 36, 339–343. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Stewart, A.L.; Ware, J.E.; Ware, J.E., Jr. (Eds.) Measuring Functioning and Well-Being: The Medical Outcomes Study Approach; Duke University Press: Durham, NC, USA, 1992. [Google Scholar]
- Bastien, C.H.; Vallières, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef] [PubMed]
- Carleton, R.N.; Asmundson, G.J.; Taylor, S. Fear of physical harm: Factor structure and psychometric properties of the injury/illness sensitivity index. J. Psychopathol. Behav. Assess. 2005, 27, 235–241. [Google Scholar] [CrossRef]
- Scheier, M.F.; Carver, C.S.; Bridges, M.W. Distinguishing optimism from neuroticism (and trait anxiety, self-mastery, and self-esteem): A reevaluation of the Life Orientation Test. J. Personal. Soc. Psychol. 1994, 67, 1063. [Google Scholar] [CrossRef]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Personal. Soc. Psychol. 1988, 54, 1063. [Google Scholar] [CrossRef]
- Sullivan, M.J.; Bishop, S.R.; Pivik, J. The pain catastrophizing scale: Development and validation. Psychol. Assess. 1995, 7, 524. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Wicksell, R.K.; Renöfält, J.; Olsson, G.L.; Bond, F.W.; Melin, L. Avoidance and cognitive fusion–central components in pain related disability? Development and preliminary validation of the Psychological Inflexibility in Pain Scale (PIPS). Eur. J. Pain 2008, 12, 491–500. [Google Scholar] [CrossRef]
- Amtmann, D.; Cook, K.F.; Jensen, M.P.; Chen, W.-H.; Choi, S.; Revicki, D.; Cella, D.; Rothrock, N.; Keefe, F.; Callahan, L. Development of a PROMIS item bank to measure pain interference. Pain 2010, 150, 173–182. [Google Scholar] [CrossRef]
- Deyo, R.A.; Ramsey, K.; Buckley, D.I.; Michaels, L.; Kobus, A.; Eckstrom, E.; Forro, V.; Morris, C. Performance of a patient reported outcomes measurement information system (PROMIS) short form in older adults with chronic musculoskeletal pain. Pain Med. 2016, 17, 314–324. [Google Scholar] [CrossRef]
- Wicksell, R.K.; Olsson, G.L.; Hayes, S.C. Mediators of change in acceptance and commitment therapy for pediatric chronic pain. Pain 2011, 152, 2792–2801. [Google Scholar] [CrossRef]
- Nicholas, M.K. The pain self-efficacy questionnaire: Taking pain into account. Eur. J. Pain 2007, 11, 153–163. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Mezzich, J.E.; Ruipérez, M.A.; Pérez, C.; Yoon, G.; Liu, J.; Mahmud, S. The Spanish version of the quality of life index: Presentation and validation. J. Nerv. Ment. Dis. 2000, 188, 301–305. [Google Scholar] [CrossRef]
- Bonfiglio, N.S.; Renati, R.; Hjemdal, O.; Friborg, O. The resilience scale for adults in italy: A validation study comparing clinical substance abusers with a nonclinical sample. Psychol. Addict. Behav. 2016, 30, 509. [Google Scholar] [CrossRef] [PubMed]
- Idler, E.L.; Angel, R.J. Self-rated health and mortality in the NHANES-I Epidemiologic Follow-up Study. Am. J. Public Health 1990, 80, 446–452. [Google Scholar] [CrossRef]
- Ware, J.E., Jr.; Kosinski, M.; Keller, S.D. A 12-Item Short-Form Health Survey: Construction of scales and preliminary tests of reliability and validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef]
- Melzack, R. The short-form McGill pain questionnaire. Pain 1987, 30, 191–197. [Google Scholar] [CrossRef]
- Spielberger, C.D.; Reheiser, E.C. Assessment of emotions: Anxiety, anger, depression, and curiosity. Appl. Psychol. Health Well-Being 2009, 1, 271–302. [Google Scholar] [CrossRef]
- Roelofs, J.; Goubert, L.; Peters, M.L.; Vlaeyen, J.W.; Crombez, G. The Tampa Scale for Kinesiophobia: Further examination of psychometric properties in patients with chronic low back pain and fibromyalgia. Eur. J. Pain 2004, 8, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Wilson, K.G.; Sandoz, E.K.; Kitchens, J.; Roberts, M. The Valued Living Questionnaire: Defining and measuring valued action within a behavioral framework. Psychol. Rec. 2010, 60, 249–272. [Google Scholar] [CrossRef]
- Üstün, T.B.; Chatterji, S.; Kostanjsek, N.; Rehm, J.; Kennedy, C.; Epping-Jordan, J.; Saxena, S.; Korff, M.V.; Pull, C. Developing the World Health Organization disability assessment schedule 2.0. Bull. World Health Organ. 2010, 88, 815–823. [Google Scholar] [CrossRef] [PubMed]



| PICOs | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population (P) |
|
|
| Intervention (I) |
|
|
| Comparison (C) |
|
|
| Outcomes (O) |
|
|
| Study design (S) |
|
|
| Study | Explicit Theoretical Framework | Statement of Aims/Objectives in Main Body of Report | Clear Description of Research Setting | Evidence of Sample Size Considered in Terms of Analysis | Representative Sample of Target Group of a Reasonable Size | Description of Procedure for Data Collection | Rationale for Choice of Data-Collection Tool(s) | Detailed Recruitment Data | Statistical Assessment of Reliability and Validity of Measurement Tool(s) * | Fit Between Stated Research Question and Content of Data-Collection Tool ° | Fit Between Stated Research Question and Method of Data Collection * | Fit Between Stated Research Question and Method of Analysis | Assessment of Reliability of Analytical Process ° | Good Justification for Analytical Method Selected | Evidence of User Involvement in Design | Strengths and Limitations Critically Discussed | QATSDD Total Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lorig et al. [28] | 3 | 3 | 2 | 0 | 2 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 0 | 3 | 34 | ||
| Williams et al. [29] | 3 | 3 | 3 | 3 | 2 | 3 | 3 | 1 | 0 | 3 | 3 | 3 | 0 | 3 | 33 | ||
| Morris et al. [30] | 3 | 3 | 3 | 0 | 2 | 3 | 2 | 3 | 3 | 3 | 3 | 3 | 0 | 0 | 31 | ||
| Kristjánsdóttir et al. [31] | 3 | 3 | 3 | 3 | 2 | 3 | 1 | 3 | 3 | 3 | 3 | 3 | 1 | 3 | 37 | ||
| Botella et al. [32] | 3 | 3 | 3 | 0 | 1 | 1 | 1 | 3 | 2 | 2 | 2 | 2 | 0 | 2 | 25 | ||
| Camerini et al. [33] | 1 | 3 | 2 | 0 | 3 | 2 | 2 | 2 | 1 | 2 | 3 | 3 | 3 | 3 | 30 | ||
| Davis & Zautra [34] | 3 | 3 | 2 | 3 | 2 | 3 | 1 | 2 | 3 | 2 | 3 | 3 | 0 | 3 | 33 | ||
| Menga et al. [35] | 3 | 3 | 3 | 0 | 2 | 3 | 1 | 3 | 0 | 1 | 3 | 3 | 0 | 2 | 27 | ||
| Ljótsson et al. [36] | 3 | 3 | 2 | 3 | 2 | 3 | 1 | 3 | 1 | 3 | 3 | 3 | 0 | 3 | 33 | ||
| Vallejo et al. [37] | 3 | 3 | 3 | 3 | 2 | 2 | 2 | 3 | 3 | 3 | 3 | 3 | 0 | 2 | 35 | ||
| Sparks et al. [38] | 3 | 3 | 3 | 1 | 3 | 3 | 2 | 3 | 3 | 2 | 3 | 3 | 0 | 2 | 34 | ||
| Friesen et al. [39] | 3 | 3 | 3 | 3 | 2 | 3 | 1 | 3 | 3 | 3 | 3 | 3 | 0 | 3 | 36 | ||
| de la Vega et al. [40] | 3 | 3 | 2 | 3 | 2 | 3 | 1 | 2 | 3 | 2 | 3 | 2 | 3 | 2 | 34 | ||
| Molinari et al. [41] | 3 | 3 | 3 | 3 | 2 | 3 | 1 | 3 | 3 | 3 | 3 | 3 | 0 | 3 | 36 | ||
| Yuan & Marques [42] | 1 | 3 | 2 | 0 | 1 | 2 | 1 | 1 | 2 | 2 | 0 | 2 | 3 | 0 | 20 | ||
| Simister et al. [43] | 3 | 3 | 2 | 3 | 2 | 3 | 1 | 3 | 3 | 3 | 3 | 3 | 1 | 3 | 36 | ||
| Hedman-Lagerlöf et al. [44] | 3 | 3 | 3 | 3 | 2 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 1 | 3 | 39 | ||
| Friedberg et al. [45] | 2 | 3 | 2 | 3 | 2 | 2 | 2 | 3 | 3 | 3 | 3 | 2 | 0 | 2 | 32 | ||
| Collinge et al. [46] | 0 | 3 | 2 | 2 | 2 | 3 | 2 | 3 | 3 | 2 | 3 | 3 | 0 | 2 | 30 | ||
| Carleton et al. [47] | 1 | 2 | 2 | 3 | 2 | 3 | 1 | 2 | 3 | 3 | 3 | 2 | 0 | 3 | 30 | ||
| Climent-Sanz et al. [48] | 3 | 3 | 3 | 3 | 3 | 2 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 0 | 3 | 35 1 | |
| Serrat et al. [49] | 3 | 3 | 3 | 1 | 2 | 2 | 3 | 3 | 3 | 3 | 3 | 3 | 0 | 3 | 35 | ||
| García-Perea et al. [50] | 1 | 3 | 3 | 3 | 2 | 3 | 1 | 2 | 1 | 3 | 3 | 3 | 0 | 2 | 30 | ||
| de la Coba et al. [51] | 3 | 3 | 3 | 1 | 1 | 3 | 3 | 2 | 3 | 3 | 3 | 3 | 0 | 3 | 34 | ||
| Ong et al. [52] | 3 | 3 | 3 | 3 | 2 | 3 | 2 | 3 | 1 | 3 | 3 | 3 | 0 | 2 | 34 | ||
| Paolucci et al. [53] | 3 | 3 | 3 | 0 | 1 | 3 | 1 | 2 | 2 | 3 | 3 | 3 | 0 | 3 | 30 | ||
| Mean value | 2.5 | 3.0 | 2.6 | 1.9 | 2.0 | 2.7 | 1.7 | 2.6 | 2.3 | 2.7 | 2.7 | 2.9 | 2.0 | 2.8 | 0.5 | 2.4 | 32.4 |
| e-Health Modality | Reference | Type of Intervention | Intervention Details |
|---|---|---|---|
| WEB-BASED PROGRAM | |||
| (a) Only web-based | Williams et al. [29] | CBT-based self-management program for symptom adaptive lifestyle management (web-enhanced behavioral self-management—WEB SM) | Contents and structure: Thirteen modules contained in a website and segregated into three broad segments: educational lectures providing background knowledge about FMS; education, behavioral, and cognitive skills designed to help with symptom management; and behavioral and cognitive skills designed to facilitate adaptive lifestyle changes for managing FMS. Duration: 6 months |
| Davis & Zautra [34] | Mindfulness-based socioemotional regulation intervention for coping with pain and stress, positive and negative affect, and positive engagement in social relations | Contents and structure: Twelve modules delivered via Adobe Presenter and centered on the following topics: welcome and introduction to mindfulness; positive and negative emotions; mindfulness of emotions; awareness of emotions and pain; acceptance of emotions; mindful living with pain; pacing yourself mindfully; emotions and thoughts; thoughts and beliefs; savoring the positive; building mindful relationships; and bringing it all together. Duration: 6 weeks | |
| Menga et al. [35] | CBT and interpersonal-therapy-based program to prevent and manage depression and anxiety symptoms (MoodGYM) | Contents and structure: Five modules delivered via a website based on cognitive reconstructing, relaxation, pleasant events, assertiveness training, and problem-solving. Duration: 6 weeks | |
| Sparks et al. [38] | Psychoeducation intervention to improve knowledge about FMS, skills for symptom management, and adopt healthier lifestyles (FibroGuide) | Contents and structure: Ten modules delivered via DVD format or USB flash drives (since the program was not available via the internet during study implementation) and including the following components: understanding FMS; communicating with family and healthcare providers; being active; improving sleep; relaxing; coping with “fibro fog” (cognitive difficulties); setting goals; pacing self; thinking differentially; and making time for self. Duration: 12 weeks | |
| Friedberg et al. [45] | Self-management intervention based on bilateral stimulation and desensitization (BSD) targeting pain and fatigue reduction | Contents and structure: BSD technique involving gentle bilateral stimulation using soft audio sounds (via earphones) or gentle finger tapping on the upper legs while the patient focuses on their most salient pain. After an initial training session, BSD was delivered for pain and stress reduction through a BSD demonstration video, duplicate written instructions, and an mp3 file of the audio BSD technique. Online diary tracked pain, fatigue, and intervention use. Duration: 90 days | |
| Climent-Sanz et al. [48] | Therapeutic patient education intervention for pain and sleep | Contents and structure: The intervention was delivered via a website according to the following plan: completing a socio-demographic data sheet and questionnaires; watching a video about the objective, characteristics, and functions of the web platform; watching a video where FMS and its associated symptoms were validated; focus on cognitive factors (week 1 and 2); behavioral factors (week 3 and 4); different activities to challenge participants to implement daily management strategies for pain and poor sleep quality based on what they learned during the previous 4 weeks; and access to a personal diary (week 5 and 6). Duration: 6 weeks | |
| (b) Web + automated feedbacks | Molinari et al. [41] | Positive future-thinking intervention for promoting positive affect and functioning (best possible self intervention—BPS) | Contents and structure: In a face-to-face session, patients were asked to imagine and write down their future best possible self through a computer application and then to visualize what they had just written. Patients were instructed to continue visualizing their BPS at home, accessing a dedicated web platform. During the intervention, participants received two automatic weekly SMS reminders to practice their exercises and reinforcements. Duration: 4 weeks |
| Collinge et al. [46] | A self-management program targeting the functional impact of FMS | Contents and structure: Participants accessed a website using an online health diary program (“SMARTLog”) to report symptom ratings, behaviors, and management strategies. The automated feedback program provided individualized recommendations based on a single-subject analysis of the accumulated data over time (“SMARTProfile”). Duration: 11-month | |
| (c) Web + interaction with live professionals’ feedbacks | Camerini et al. [33] | Self-management education intervention to increase knowledge and empowerment (ONESELF) | Contents and structure: The intervention was delivered via a website, which included the following functionalities: a virtual library providing users with relevant information on the disease; a first aid and a frequently asked questions section (FAQ), providing brief and practical information on the syndrome management; and a virtual gymnasium providing patients with tailored multimedia contents on several physical exercises. The website also enabled asynchronous and synchronous interactions with health professionals and laypeople to provide social support. Duration: 167 days |
| Ljótsson et al. [36] | Acceptance and values-based exposure treatment to improve quality of life, psychological flexibility, and health-related costs | Contents and structure: The intervention material was presented on printer-friendly web pages and divided into five successive steps: introduction with information about pain and FMS; explanation of the learning of symptom-related fear of how FM-related avoidance behaviors maintain fear and ultimately lead to disability; promotion of a mindful and accepting stance towards negative thoughts and experiences; continued values-based behavioral change through exposure; and relapse management. Participants were encouraged to send at least a weekly message about their work with the intervention to their therapist, who could, in turn, contact them through text messages. Duration: 10 weeks | |
| Hedman-Lagerlöf et al. [44] | Exposure therapy to break the vicious cycle of preoccupation with symptoms, avoidance, and increased pain | Contents and structure: The intervention was delivered by a web platform and divided into eight modules, to which the participant gained gradual access by completing homework assignments: role of avoidance behaviors; psychoeducation about exposure; identification of personal avoidance behaviors; planning phase; and personalized exposure exercises. Treatment progress was closely monitored by a therapist, with whom participants had regular (about one-to-three times/week) contact through asynchronous text messages on the platform. Duration: 10 weeks | |
| Serrat et al. [49] | Multicomponent intervention (therapeutic exercise, pain neuroscience education, CBT, and mindfulness training) for reducing functional impairment and improving several psychological and physical variables (FIBROWALK) | Contents and structure: Participants were emailed a link to a 60 min video on a private YouTube channel once a week. Each video provided detailed guidelines explaining how to perform different home-based aerobic exercises, education in the neuroscience of pain, CBT to decrease anxiety and depressive symptoms, pain catastrophizing, and changing inadequate emotional regulation strategies. Participants could contact the therapist (via email) at any time. The therapist could also contact them in case of any issue related to the program or the study. Duration: 12 weeks | |
| Simister et al. [43] | ACT-based intervention for reducing the FMS impact on daily functioning and improving pain, mood, and physical function | Contents and structure: The intervention was delivered via a website on seven units: introduction; acceptance; values; medications, sleep, “fibro fog”, exercise, and effective communication; cognitive defusion (or you are not your thoughts!); mindfulness and self-as-context; and are you willing? Written unit materials were provided in PDF format and enhanced through mp3 audio recordings, videos, and experiential homework exercises. The treatment team provided participants with weekly email reminders to complete the program and a reminder to contact a team member if they had any concerns. Duration: 8 weeks | |
| García-Perea et al. [50] | Self-management education intervention to improve quality of life (Red Sinapsis) | Contents and structure: A web platform provided patients with information on their illnesses, access to their clinical history, and a messaging system for communicating with the medical or nursing staff at any time. Duration: 12 months | |
| Ong et al. [52] | Positive affect (PA) skills-building intervention program to keep stress and pain under control (LARKSPUR) | Contents and structure: The intervention was delivered via a website and included eight PA skills over five learning modules: noticing positive events; savoring positive events; identifying personal strengths; behavioral activation; mindfulness and positive reappraisal; gratitude; and acts of kindness. The intervention was supplemented by support from research staff via telephone and email. Duration: 5 weeks | |
| (d) Web + automated and live feedbacks | Lorig et al. [28] | The self-management program focused on reducing pain and improving functioning | Contents and structure: The program was delivered via a website targeting the following components: self-management principles; goal setting/action plans; pain management; problem-solving steps; fitness/exercise; feedback/problem-solving; difficult emotions; healthy eating; osteoporosis; fatigue and energy conservation; medication; depression; work with your health care professional; evaluating treatment plans; and sleep. Participants were asked to log on at least three times for 1-2 h and participate in the weekly activities. Any problem they wished to discuss could be posted on the bulletin board and responded to by other group members and the moderators. The program also used email reminders to encourage nonparticipants to participate. Duration: 6 weeks |
| Vallejo et al. [37] | CBT intervention for reducing the FMS impact on daily functioning and improving different pain-related psychological variables | Contents and structure: The intervention was delivered via a web application and included ten modules: psychoeducation; progressive relaxation training; emotional training; increasing and adjusting daily activities; techniques for insomnia and sexual dysfunctions; problem-solving; cognitive restructuring; attentional control and illness behaviors; intellectual problems; and revision and relapse intervention. Participants could send individual messages to the therapist. The program had several points to facilitate interaction with the professional (e.g., feedback message to the participant to reinforce the weekly schedule). Duration: 10 weeks | |
| Friesen et al. [39] | CBT based self-management program addressing pain, disability, and emotional wellbeing (The Pain Course) | Contents and structure: The intervention was delivered via a website and included five weekly lessons, homework, and additional resources. The following components were included: prevalence of chronic pain and symptoms of depression and anxiety; information about pain perception; cognitive behavioral model; principles of cognitive therapy; strategies for monitoring and challenging thoughts; physical symptoms of anxiety and depression, chronic pain; controlled breathing; pleasant activity scheduling; pacing; graded exposure; relapse prevention; and goal setting. Clinical contact with participants occurred weekly via secure messaging and telephone to provide general support and encouragement. They also received standardized automated emails each week. Duration: 8 weeks | |
| (e) Dedicated computer software | Carleton et al. [47] | Attention bias modification (ABM) computer program for reducing patients’ hypervigilance for pain-related cues | Contents and structure: Participants were given attention tasks using word stimuli established as relevant to pain-specific attentional biases and matched to neutral words of comparable length. At each treatment session, participants were required to rate their emotional intensity associated with each of the 48 pain-specific threat words from “not at all bothersome” to “very bothersome”. The computer then used the 20 words rated as most negative by each participant as the threat words for that session, which should have facilitated personal relevance. Duration: 4 weeks |
| MOBILE PHONE APPLICATION (m-Health) | Kristjánsdóttir et al. [31] | ACT intervention to reduce catastrophizing and improve function | Contents and structure: The intervention was delivered via mobile software after participants completed an inpatient multidimensional rehabilitation program for chronic pain and included the following components face-to-face sessions; web-based diaries; written situational feedback from a therapist; and audio files with guided mindfulness exercises. Duration: 4 weeks |
| Yuan & Marques [42] | Multicomponent intervention (psychoeducation, CBT strategies, and physical activity) to improve HrQoL, symptoms, and self-care agency (ProFibro) | Contents and structure: The intervention was delivered via a mobile phone application. It included the following components: patient education through animation, self-monitoring, sleep strategies, scheduling, graded exercise program, gratitude practice, family adjustments, and hints. Duration: 1 week | |
| de la Vega et al. [40] | CBT intervention to improve the quality of life (Fibroline) | Contents and structure: The intervention was delivered via a mobile phone application. It included different modules targeting the following components: life values and goal setting, sleep quality, anxiety management, pain education and coping, medication use, physical conditions, mood regulation, thoughts management, and relapse prevention. Four types of tasks were activated when treatment modules were accessed: resources; assessments; notes; and reminders. Duration: 9 weeks | |
| VIRTUAL REALITY (VR) | Morris et al. [30] | Exposure therapy program as a treatment for exercise-related pain catastrophizing | Contents and structure: Visual exposure to exercise activities delivered via a VR head-mount display (HMD) as part of an in-person intervention. Duration: 16 weeks |
| Botella et al. [32] | CBT intervention to improve pain- and mood-related variables | Contents and structure: A VR system was used as an adjunct to face-to-face CBT for delivering relaxation and mindfulness. In more detail, while participants were immersed in the VR, the system provided instructions on observing the different elements offered by the scenarios, remaining focused on the present moment and participating in the experience without making any judgments. Duration: 6 weeks | |
| VIDEO CONSULTING | de la Coba et al. [51] | ACT intervention to enhance the patient’s openness to experiencing pain and associated emotional discomfort | Contents and structure: Online groups of Google Meet video-meeting sessions (105 min. duration each), where each consisted of an initial presentation (or participatory summary of the previous session), a review of experiences after practicing the proposed activities at home, a presentation of metaphors and practice of experiential exercises, scheduling of practice activities at home, reflections, and resolution of doubts and queries. Duration: 5 weeks |
| Paolucci et al. [53] | Mind–body intervention to improve pain, function, and different pain-related psychological variables | Contents and structure: Video-meeting sessions (60 min. duration each) using an online communication platform (i.e., Zoom) based on the following principles: anchoring to a positive emotion through the choice of a color, “here and now”: listen and perceive your “own” body in motion, conscious breathing, “close your eyes”: improve interoceptive awareness during physical exercises, and relaxation: breathe, moving slowly and without pain. Duration: 8 weeks |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Donisi, V.; De Lucia, A.; Pasini, I.; Gandolfi, M.; Schweiger, V.; Del Piccolo, L.; Perlini, C. e-Health Interventions Targeting Pain-Related Psychological Variables in Fibromyalgia: A Systematic Review. Healthcare 2023, 11, 1845. https://doi.org/10.3390/healthcare11131845
Donisi V, De Lucia A, Pasini I, Gandolfi M, Schweiger V, Del Piccolo L, Perlini C. e-Health Interventions Targeting Pain-Related Psychological Variables in Fibromyalgia: A Systematic Review. Healthcare. 2023; 11(13):1845. https://doi.org/10.3390/healthcare11131845
Chicago/Turabian StyleDonisi, Valeria, Annalisa De Lucia, Ilenia Pasini, Marialuisa Gandolfi, Vittorio Schweiger, Lidia Del Piccolo, and Cinzia Perlini. 2023. "e-Health Interventions Targeting Pain-Related Psychological Variables in Fibromyalgia: A Systematic Review" Healthcare 11, no. 13: 1845. https://doi.org/10.3390/healthcare11131845
APA StyleDonisi, V., De Lucia, A., Pasini, I., Gandolfi, M., Schweiger, V., Del Piccolo, L., & Perlini, C. (2023). e-Health Interventions Targeting Pain-Related Psychological Variables in Fibromyalgia: A Systematic Review. Healthcare, 11(13), 1845. https://doi.org/10.3390/healthcare11131845