_MD__MPH_PhD.png)
Association between Parity and Preterm Birth—Retrospective Analysis from a Single Center in Poland


 , and
, and 
Abstract
1. Introduction
2. Materials and Methods
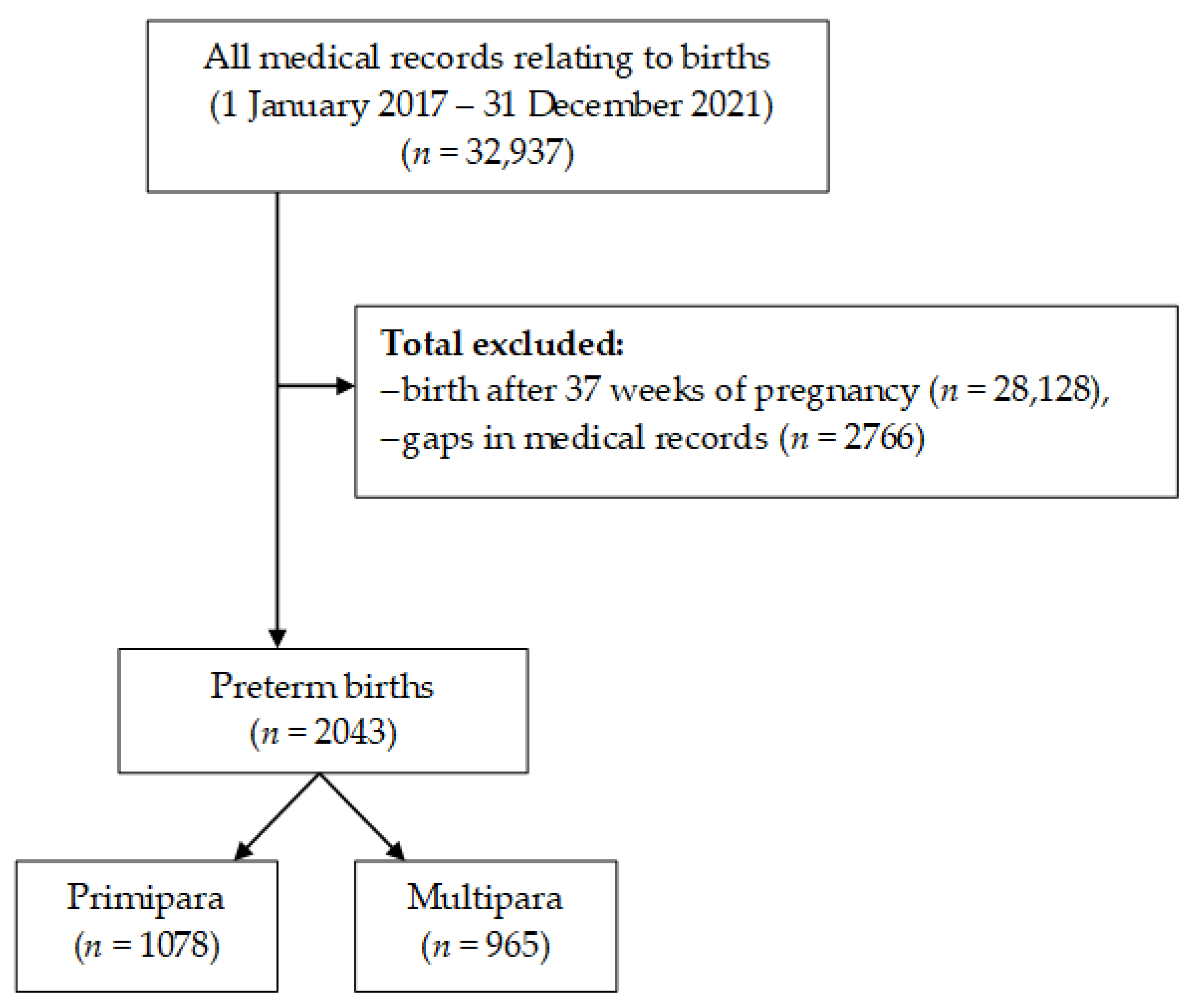
2.1. Study Design and Setting
2.2. Eligibility Criteria
2.3. Data Collection
2.4. Ethics
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Preterm Birth. Available online: https://www.who.int/news-room/fact-sheets/detail/preterm-birth (accessed on 11 January 2023).
- Purisch, S.E.; Gyamfi-Bannerman, C. Epidemiology of preterm birth. Semin. Perinatol. 2017, 41, 387–391. [Google Scholar] [CrossRef]
- Jiang, M.; Mishu, M.M.; Lu, D.; Yin, X. A case control study of risk factors and neonatal outcomes of preterm birth. Taiwan J. Obstet. Gynecol. 2018, 57, 814–818. [Google Scholar] [CrossRef]
- Romero, R.; Conde-Agudelo, A.; Da Fonseca, E.; O’Brien, J.M.; Cetingoz, E.; Creasy, G.W.; Hassan, S.S.; Nicolaides, K.H. Vaginal progesterone for preventing preterm birth and adverse perinatal outcomes in singleton gestations with a short cervix: A meta-analysis of individual patient data. Am. J. Obstet. Gynecol. 2018, 218, 161–180. [Google Scholar] [CrossRef] [PubMed]
- McGoldrick, E.; Stewart, F.; Parker, R.; Dalziel, S.R. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst. Rev. 2020, 12, CD004454. [Google Scholar] [CrossRef]
- Wolf, M.F.; Sgayer, I.; Miron, D.; Krencel, A.; Sheffer, V.F.; Idriss, S.S.; Sammour, R.N.; Peleg, D.; Shachar, I.B.; Rechnitzer, H.; et al. A novel extended prophylactic antibiotic regimen in preterm pre-labor rupture of membranes: A randomized trial. Int. J. Infect. Dis. 2020, 96, 254–259. [Google Scholar] [CrossRef] [PubMed]
- Härkin, P.; Marttila, R.; Pokka, T.; Saarela, T.; Hallman, M. Survival analysis of a cohort of extremely preterm infants born in Finland during 2005-2013. J. Matern. Fetal Neonatal Med. 2021, 34, 2506–2512. [Google Scholar] [CrossRef]
- Pravia, C.I.; Benny, M. Long-term consequences of prematurity. Cleve. Clin. J. Med. 2020, 87, 759–767. [Google Scholar] [CrossRef] [PubMed]
- Koo, H.Y.; Lee, B.R. Educational needs for practicing neonatal intensive care among Korean nursing students. Child Health Nurs. Res. 2021, 27, 339–353. [Google Scholar] [CrossRef]
- Stroustrup, A.; Bragg, J.B.; Busgang, S.A.; Andra, S.S.; Curtin, P.; Spear, E.A.; Just, A.C.; Arora, M.; Gennings, C. Sources of clinically significant neonatal intensive care unit phthalate exposure. J. Expo. Sci. Environ. Epidemiol. 2020, 30, 137–148. [Google Scholar] [CrossRef]
- Babaie, M.; Nourian, M.; Atashzadeh-Shoorideh, F.; Manoochehri, H.; Nasiri, M. Patient safety culture in neonatal intensive care units: A qualitative content analysis. Front. Public Health 2023, 11, 1065522. [Google Scholar] [CrossRef]
- Prullage, G.S.; Kenner, C.; Uwingabire, F.; Ndayambaje, A.; Boykova, M.; Walker, K. Survey of neonatal nursing: Staffing, education, and equipment availability in Rwanda. J. Neonatal Nurs. 2022, 28, 192–199. [Google Scholar] [CrossRef]
- Rutayisire, E.; Mochama, M.; Ntihabose, C.K.; Utumatwishima, J.N.; Habtu, M. Maternal, obstetric and gynecological factors associated with preterm birth in Rwanda: Findings from a national longitudinal study. BMC Pregnancy Childbirth 2023, 23, 365. [Google Scholar] [CrossRef] [PubMed]
- Di Renzo, G.C.; Tosto, V.; Giardina, I. The biological basis and prevention of preterm birth. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 52, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.D.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef]
- Ye, C.X.; Chen, S.B.; Wang, T.T.; Zhang, S.M.; Qin, J.B.; Chen, L.Z. Risk factors for preterm birth: A prospective cohort study. Chin. J. Contemp. Pediatr. 2021, 23, 1242–1249. [Google Scholar] [CrossRef]
- Phillips, C.; Velji, Z.; Hanly, C.; Metcalfe, A. Risk of recurrent spontaneous preterm birth: A systematic review and meta-analysis. BMJ Open 2017, 7, e015402. [Google Scholar] [CrossRef]
- Zhang, Y.J.; Zhu, Y.; Zhu, L.; Lu, C.Q.; Chen, C.; Yuan, L. Prevalence of preterm birth and risk factors associated with it at different gestational ages: A multicenter retrospective survey in China. Saudi Med. J. 2022, 43, 599–609. [Google Scholar] [CrossRef]
- Cao, G.; Liu, J.; Liu, M. Global, Regional, and National Incidence and Mortality of Neonatal Preterm Birth, 1990-2019. JAMA Pediatr. 2022, 176, 787–796. [Google Scholar] [CrossRef]
- Centers of Disease Control and Prevention. Preterm Birth. Available online: https://www.cdc.gov/reproductivehealth/maternalinfanthealth/pretermbirth.htm (accessed on 11 January 2023).
- Walani, S.R. Global burden of preterm birth. Int. J. Gynaecol. Obstet. 2020, 150, 31–33. [Google Scholar] [CrossRef]
- Statistics Poland. Demographic Situation in Poland up to 2017. Births and Fertility. Available online: https://stat.gov.pl/files/gfx/portalinformacyjny/pl/defaultaktualnosci/5468/33/1/1/sytuacja_demograficzna_polski_do_2017_r.pdf (accessed on 11 January 2023).
- Mariańczyk, K.; Libera, A.; Rosińska, P. Psychologiczne i społeczne czynniki ryzyka porodu przedwczesnego. Kwart. Nauk. Fides Et Ratio 2020, 43, 260–273. [Google Scholar] [CrossRef]
- Shah, P.S. Knowledge Synthesis Group on Determinants of LBW/PT births. Parity and low birth weight and preterm birth: A systematic review and meta-analyses. Acta Obstet. Gynecol. Scand. 2010, 89, 862–875. [Google Scholar] [CrossRef] [PubMed]
- Iams, J.D.; Romero, R.; Culhane, J.F.; Goldenberg, R.L. Primary, secondary, and tertiary interventions to reduce the morbidity and mortality of preterm birth. Lancet 2008, 371, 164–175. [Google Scholar] [CrossRef]
- Beck, S.; Wojdyla, D.; Say, L.; Betran, A.P.; Merialdi, M.; Requejo, J.H.; Rubens, C.; Menon, R.; Van Look, P.F. The worldwide incidence of preterm birth: A systematic review of maternal mortality and morbidity. Bull. World Health Organ. 2010, 88, 31–38. [Google Scholar] [CrossRef]
- Koullali, B.; van Zijl, M.D.; Kazemier, B.M.; Oudijk, M.A.; Mol, B.W.J.; Pajkrt, E.; Ravelli, A.C.J. The association between parity and spontaneous preterm birth: A population based study. BMC Pregnancy Childbirth 2020, 20, 1–8. [Google Scholar] [CrossRef]
- Alhainiah, M.H.; Abdulljabbar, H.S.; Bukhari, Y.A. The prevalence, the fetal and maternal outcomes in grand multiparas women. Mater. Socio-Med. 2018, 30, 118. [Google Scholar] [CrossRef] [PubMed]
- Hangarga, U.S.; Yattinamani, B. Clinical study of primary cesarean section in multiparous women. Int. J. Clin. Obstet. Gynaecol. 2020, 4, 32–34. [Google Scholar] [CrossRef]
- Fuchs, F.; Monet, B.; Ducruet, T.; Chaillet, N.; Audibert, F. Effect of maternal age on the risk of preterm birth: A large cohort study. PLoS ONE 2018, 13, e0191002. [Google Scholar] [CrossRef] [PubMed]
- Lei, F.; Zhang, L.; Shen, Y.; Zhao, Y.; Kang, Y.; Qu, P.; Mi, B.; Dang, S.; Yan, H. Association between parity and macrosomia in Shaanxi Province of Northwest China. Ital. J. Pediatr. 2020, 46, 1–7. [Google Scholar] [CrossRef]
- Granés, L.; Torà-Rocamora, I.; Palacio, M.; De la Torre, L.; Llupià, A. Maternal educational level and preterm birth: Exploring inequalities in a hospital-based cohort study. PLoS ONE 2023, 18, e0283901. [Google Scholar] [CrossRef]
- Blitz, M.J.; Gerber, R.P.; Gulersen, M.; Shan, W.; Rausch, A.C.; Prasannan, L.; Meirowitz, N.; Rochelson, B. Preterm birth among women with and without severe acute respiratory syndrome coronavirus 2 infection. Acta Obstet. Gynecol. Scand. 2021, 100, 2253–2259. [Google Scholar] [CrossRef]
- Gurung, A.; Wrammert, J.; Sunny, A.K.; Gurung, R.; Rana, N.; Basaula, Y.N.; Paudel, P.; Pokhrel, A.; Kc, A. Incidence, risk factors and consequences of preterm birth—findings from a multi-centric observational study for 14 months in Nepal. Arch. Public Health 2020, 78, 64. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Fan, C.; Luo, M.; Fang, J.; Zhou, S.; Zhang, F. Pregnancy complications among nulliparous and multiparous women with advanced maternal age: A community-based prospective cohort study in China. BMC Pregnancy Childbirth 2020, 20, 581. [Google Scholar] [CrossRef]
- Szylit, N.A.; Malburg, F.L.; Piccinato, C.A.; Ferreira, L.A.P.; Podgaec, S.; Zlotnik, E. Prevalence of rectovaginal colonization by group B Streptococcus in pregnant women seen at prenatal care program of a health organization. Einstein 2019, 18, eAO4920. [Google Scholar] [CrossRef]
- Chen, K.H.; Chen, I.C.; Yang, Y.C.; Chen, K.T. The trends and associated factors of preterm deliveries from 2001 to 2011 in Taiwan. Medicine 2019, 98, e15060. [Google Scholar] [CrossRef] [PubMed]
- Yong, H.Y.; Mohd Shariff, Z.; Mohd Yusof, B.N.; Rejali, Z.; Tee, Y.Y.S.; Bindels, J.; van der Beek, E.M. Higher Parity, Pre-Pregnancy BMI and Rate of Gestational Weight Gain Are Associated with Gestational Diabetes Mellitus in Food Insecure Women. Int. J. Environ. Res. Public Health 2021, 18, 2694. [Google Scholar] [CrossRef] [PubMed]
- Wagan, N.; Amanullah, A.T.; Makhijani, P.B.; Kumari, R. Factors Associated With Gestational Diabetes Mellitus: A Cross-Sectional Study. Cureus 2021, 13, e17113. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Binongo, J.N.; Kancherla, V. Effect of Parity on Pregnancy-Associated Hypertension Among Asian American Women in the United States. Matern. Child Health J. 2019, 23, 1098–1107. [Google Scholar] [CrossRef] [PubMed]
- Souter, V.; Painter, I.; Sitcov, K.; Caughey, A.B. Maternal and newborn outcomes with elective induction of labor at term. Am. J. Obstet. Gynecol. 2019, 220, 273.e1–273.e11. [Google Scholar] [CrossRef]
- Maeda, Y.; Kaneko, K.; Ogawa, K.; Sago, H.; Murashima, A. The effect of parity, history of preeclampsia, and pregnancy care on the incidence of subsequent preeclampsia in multiparous women with SLE. Mod. Rheumatol. 2021, 31, 843–848. [Google Scholar] [CrossRef]
- Gupta, P.; Jain, M.; Verma, V.; Gupta, N.K. The Study of Prevalence and Pattern of Thyroid Disorder in Pregnant Women: A Prospective Study. Cureus 2021, 13, e16457. [Google Scholar] [CrossRef]
- Toloza, F.J.K.; Derakhshan, A.; Männistö, T.; Bliddal, S.; Popova, P.V.; Carty, D.M.; Chen, L.; Taylor, P.; Mosso, L.; Oken, E.; et al. Association between maternal thyroid function and risk of gestational hypertension and pre-eclampsia: A systematic review and individual-participant data meta-analysis. Lancet Diabetes Endocrinol. 2022, 10, 243–252. [Google Scholar] [CrossRef]
- Oladapo, O.T.; Souza, J.P.; Fawole, B.; Mugerwa, K.; Perdoná, G.; Alves, D.; Souza, H.; Reis, R.; Oliveira-Ciabati, L.; Maiorano, A.; et al. Progression of the first stage of spontaneous labour: A prospective cohort study in two sub-Saharan African countries. PLoS Med. 2018, 15, e1002492. [Google Scholar] [CrossRef] [PubMed]
- Luo, S.; Chen, Z.; Wang, X.; Zhu, C.; Su, S. Labor epidural analgesia versus without labor epidural analgesia for multiparous women: A retrospective case control study. BMC Anesthesiol. 2021, 21, 133. [Google Scholar] [CrossRef] [PubMed]
- Orbach-Zinger, S.; Landau, R.; Davis, A.; Oved, O.; Caspi, L.; Fireman, S.; Fein, S.; Ioscovich, A.; Bracco, D.; Hoshen, M.; et al. The Effect of Labor Epidural Analgesia on Breastfeeding Outcomes: A Prospective Observational Cohort Study in a Mixed-Parity Cohort. Anesth. Analg. 2019, 129, 784–791. [Google Scholar] [CrossRef]
- Kartal, B.; Kızılırmak, A.; Calpbinici, P.; Demir, G. Retrospective analysis of episiotomy prevalence. J. Turk. Ger. Gynecol. Assoc. 2017, 18, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Beyene, F.; Nigussie, A.A.; Limenih, S.K.; Tesfu, A.A.; Wudineh, K.G. Factors Associated with Episiotomy Practices in Bahirdar City, Ethiopia: A Cross-Sectional Study. Risk Manag. Healthc. Policy 2020, 13, 2281–2289. [Google Scholar] [CrossRef]
- Myrick, T.G.; Sandri, K.J. Epidural Analgesia and Any Vaginal Laceration. J. Am. Board Fam. Med. 2018, 31, 768–773. [Google Scholar] [CrossRef]
- Wilson, A.N.; Homer, C.S.E. Third- and fourth-degree tears: A review of the current evidence for prevention and management. Aust. N. Z. J. Obstet. Gynaecol. 2020, 60, 175–182. [Google Scholar] [CrossRef]
- Ashwal, E.; Livne, M.Y.; Benichou, J.I.; Unger, R.; Hiersch, L.; Aviram, A.; Mani, A.; Yogev, Y. Contemporary patterns of labor in nulliparous and multiparous women. Am. J. Obstet. Gynecol. 2020, 222, 267.e1–267.e9, Erratum in Am. J. Obstet. Gynecol. 2020, 223, 918. [Google Scholar] [CrossRef]
- Rosenbloom, J.I.; Rottenstreich, A.; Yagel, S.; Sompolinksy, Y.; Levin, G. The length of the second stage of labor in nulliparous, multiparous, grand-multiparous, and grand-grand multiparous women in a large modern cohort. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 253, 273–277. [Google Scholar] [CrossRef]
- Chen, H.; Cao, L.; Cao, W.; Wang, H.; Zhu, C.; Zhou, R. Factors affecting labor duration in Chinese pregnant women. Medicine 2018, 97, e13901. [Google Scholar] [CrossRef] [PubMed]
- Gu, C.; Wang, X.; Zhang, Z.; Schwank, S.; Zhu, C.; Zhang, Z.; Qian, X. Pregnant women’s clinical characteristics, intrapartum interventions, and duration of labour in urban China: A multi-center cross-sectional study. BMC Pregnancy Childbirth. 2020, 20, 386. [Google Scholar] [CrossRef]
- Barakat, R.; Franco, E.; Perales, M.; López, C.; Mottola, M.F. Exercise during pregnancy is associated with a shorter duration of labor. A randomized clinical trial. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 224, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Tadese, M.; Tessema, S.D.; Taye, B.T. Adverse Perinatal Outcomes Among Grand Multiparous and Low Multiparous Women and Its Associated Factors in North Shewa Zone Public Hospitals: The Role of Parity. Int. J. Gen. Med. 2021, 14, 6539–6548. [Google Scholar] [CrossRef]
- Kaur, S.; Ng, C.M.; Badon, S.E.; Jalil, R.A.; Maykanathan, D.; Yim, H.S.; Mohamed, H.J. Risk factors for low birth weight among rural and urban Malaysian women. BMC Public Health 2019, 19 (Suppl. 4), 539. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Total n = 2043 | Primipara n = 1078 (52.77%) | Multipara n = 965 (47.23%) | OR (95% CI) | p-Value |
|---|---|---|---|---|---|
| Age—Me (IQR) | 33 (29–36) | 31 (28–34) | 34 (31–37) | - | <0.01 |
| Place of residence—n (%) | |||||
| Village | 444 (21.83) | 196 (18.18) | 248 (25.70) | 1 | <0.01 |
| City/town | 1599 (78.17) | 882 (81.82) | 717 (74.30) | 1.56 (1.26–1.92) | |
| Education—n (%) | |||||
| Primary education | 91 (4.45) | 36 (3.34) | 55 (5.70) | 1 | |
| Secondary education | 366 (17.91) | 179 (16.60) | 187 (19.38) | 1.46 (0.92–2.33) | 0.111 |
| Higher education | 1586 (77.63) | 863 (80.06) | 723 (74.92) | 1.82 (1.18–2.81) | 0.006 |
| Marital status—n (%) | |||||
| Single | 450 (22.03) | 280 (25.97) | 170 (17.62) | 1 | <0.01 |
| In a relationship | 1593 (77.97) | 798 (74.03) | 795 (82.38) | 0.61 (0.49–0.76) | |
| COVID-19 Era—n (%) | |||||
| No | 1432 (70.09) | 763 (70.78) | 669 (69.33) | 1 | 0.474 |
| Yes | 611 (29.91) | 315 (29.22) | 296 (30.87) | 0.93 (0.77–1.13) | |
| Variables | Total | Primipara n = 1078 | Multipara n = 965 | OR (95% CI) | p-Value |
|---|---|---|---|---|---|
| No. of pregnancies—Me (IQR) | 2 (1–3) | 1 (1–1) | 3 (2–3) | - | <0.01 |
| HBD—Me (IQR) | 35 (32–36) | 35 (33–36) | 35 (32–36) | - | 0.341 |
| Pregnancy type—n (%) | |||||
| Single | 1527 (74.74) | 777 (72.08) | 750 (77.72) | 1 | |
| Twin | 474 (23.20) | 280 (25.97) | 194 (20.10) | 1.39 (1.13–1.72) | 0.002 |
| Triplet | 42 (2.06) | 21 (1.95) | 21 (2.18) | 0.97 (0.52–1.78) | 0.910 |
| History of miscarriage—n (%) | |||||
| No | 1492 (73.03) | 869 (80.61) | 623 (64.56) | 1 | <0.01 |
| Yes | 551 (26.97) | 209 (19.39) | 342 (35.44) | 0.44 (0.36–0.64) | |
| Pessary—n (%) | |||||
| No | 1848 (90.46) | 963 (89.33) | 885 (91.71) | 1 | 0.068 |
| Yes | 195 (9.54) | 115 (10.67) | 80 (8.29) | 1.32 (0.98–1.78) | |
| GBS—n (%) | |||||
| No | 1477 (72.30) | 781 (72.45) | 696 (72.12) | 1 | 0.369 |
| Yes | 169 (8.27) | 85 (7.88) | 84 (8.70) | 0.90 (0.66–1.24) | |
| No | 397 (19.43) | 212 (19.67) | 185 (19.17) | 1.02 (0.82–1.28) | |
| Thromboprophylaxis—n (%) | |||||
| No | 809 (39.60) | 432 (40.07) | 377 (39.07) | 1 | 0.642 |
| Yes | 1234 (60.40) | 646 (59.93) | 588 (60.93) | 0.96 (0.80–1.15) | |
| Antibiotic prophylaxis—n (%) | |||||
| No | 266 (13.02) | 123 (11.41) | 143 (14.82) | 1 | 0.022 |
| Yes | 1777 (86.98) | 955 (88.59) | 822 (85.18) | 1.35 (1.04–1.57) | |
| Variables | Total | Primipara n = 1078 | Multipara n = 965 | OR (95% CI) | p-Value |
|---|---|---|---|---|---|
| Gestational diabetes—n (%) | |||||
| No | 1680 (82.23) | 905 (83.95) | 775 (80.31) | 1 | 0.032 |
| Yes | 363 (17.77) | 173 (16.05) | 190 (19.69) | 0.78 (0.62–0.98) | |
| Gestational hypertension—n (%) | |||||
| No | 1866 (91.34) | 968 (89.90) | 898 (93.06) | 1 | 0.009 |
| Yes | 177 (8.66) | 110 (10.20) | 67 (6.94) | 1.52 (1.11–2.09) | |
| Pre-eclampsia—n (%) | |||||
| No | 1877 (91.87) | 968 (89.80) | 909 (94.20) | 1 | <0.01 |
| Yes | 166 (8.13) | 110 (10.20) | 56 (5.80) | 1.85 (1.32–2.58) | |
| Cholestasis of pregnancy—n (%) | |||||
| No | 1936 (94.76) | 1007 (93.41) | 929 (96.27) | 1 | 0.004 |
| Yes | 107 (5.24) | 71 (6.59) | 36 (3.73) | 1.82 (1.21–2.74) | |
| Hypothyroidism—n (%) | |||||
| No | 1531 (74.94) | 782 (72.54) | 749 (77.62) | 1 | 0.008 |
| Yes | 512 (25.06) | 296 (27.46) | 216 (22.38) | 1.31 (1.07–1.61) | |
| Hashimoto’s—n (%) | |||||
| No | 1893 (82.66) | 1001 (92.86) | 892 (92.44) | 1 | 0.715 |
| Yes | 150 (7.34) | 77 (7.14) | 73 (7.56) | 0.94 (0.67–1.31) | |
| Anemia—n (%) | |||||
| No | 1014 (49.63) | 516 (47.87) | 498 (51.61) | 1 | 0.091 |
| Yes | 1029 (50.37) | 562 (52.13) | 467 (48.39) | 0.86 (0.72–1.02) | |
| Thrombocytopenia—n (%) | |||||
| No | 1787 (87.47) | 934 (86.64) | 853 (88.39) | 1 | 0.233 |
| Yes | 256 (15.53) | 144 (13.36) | 112 (11.61) | 1.17 (0.90–1.53) | |
| Cervical incompetence—n (%) | |||||
| No | 1982 (97.01) | 1039 (96.38) | 943 (97.72) | 1 | 0.076 |
| Yes | 61 (2.99) | 39 (3.62) | 22 (2.28) | 1.61 (0.85–2.73) | |
| Health Problems—n (%) | |||||
| No | 384 (18.80) | 174 (16.14) | 210 (21.76) | 1 | 0.001 |
| Yes | 1659 (81.20) | 904 (83.86) | 755 (78.24) | 1.45 (1.16–1.81) | |
| Variables | Total | Primipara n = 1078 | Multipara n = 965 | OR (95% CI) | p-Value |
|---|---|---|---|---|---|
| Labor type—n (%) | |||||
| Physiologic | 748 (36.61) | 388 (35.99) | 360 (37.31) | 1 | |
| C-section | 1281 (62.70) | 680 (63.08) | 601 (62.28) | 1.05 (0.88–1.26) | 0.598 |
| Intervention | 14 (0.69) | 10 (0.93) | 4 (0.41) | 2.32 (0.72–7.46) | 0.158 |
| Family member present—n (%) | |||||
| No | 1625 (79.54) | 851 (78.94) | 774 (80.21) | 1 | 0.479 |
| Yes | 191 (20.46) | 227 (21.06) | 191 (19.79) | 1.08 (0.87–1.34) | |
| Pre-induction—n (%) | |||||
| No | 2008 (98.29) | 1058 (98.14) | 950 (98.45) | 1 | 0.601 |
| Yes | 35 (1.71) | 20 (1.86) | 15 (1.55) | 1.20 (0.61–2.35) | |
| Induction—n (%) | |||||
| No | 1867 (91.39) | 976 (90.54) | 891 (92.33) | 1 | 0.149 |
| Yes | 176 (8.61) | 102 (9.46) | 74 (7.67) | 1.26 (0.92–1.72) | |
| Stimulation—n (%) | |||||
| No | 1917 (93.83) | 987 (91.56) | 930 (96.37) | 1 | <0.01 |
| Yes | 126 (6.17) | 91 (8.44) | 35 (3.63) | 2.45 (1.64–3.66) | |
| Oxytocin—stage 1 *—n (%) | |||||
| No | 1888 (92.41) | 977 (90.63) | 911 (94.40) | 1 | 0.001 |
| Yes | 155 (7.59) | 101 (9.37) | 54 (5.60) | 1.74 (1.24–2.46) | |
| Oxytocin—stage 2 **—n (%) | |||||
| No | 1859 (90.99) | 989 (88.96) | 900 (93.26) | 1 | 0.001 |
| Yes | 184 (9.01) | 119 (11.04) | 65 (6.74) | 1.72 (1.25–2.36) | |
| Oxytocin—stage 3 ***—n (%) | |||||
| No | 1529 (74.84) | 797 (73.93) | 732 (75.85) | 1 | 0.318 |
| Yes | 514 (25.16) | 281 (26.07) | 233 (24.15) | 1.11 (0.91–1.35) | |
| Amniotomy—n (%) | |||||
| No | 2024 (99.07) | 1068 (99.07) | 956 (99.07) | 1 | 0.991 |
| Yes | 19 (0.93) | 10 (0.93) | 9 (0.97) | 0.99 (0.40–2.46) | |
| Epidural anesthesia—n (%) | |||||
| No | 1761 (86.20) | 891 (82.65) | 870 (90.16) | 1 | <0.01 |
| Yes | 282 (13.80) | 187 (17.35) | 95 (9.84) | 1.92 (1.48–2.50) | |
| Perineal trauma—n (%) | |||||
| No | 1559 (76.31) | 783 (72.63) | 776 (80.41) | 1 | |
| Perineal tear | 117 (5.73) | 40 (3.71) | 77 (7.98) | 0.52 (0,35–0,76) | 0.001 |
| Episiotomy | 367 (17.96) | 255 (23.65) | 112 (11.61) | 2.26 (1.77–2.88) | <0.01 |
| Uterine curettage—n (%) | |||||
| No | 1724 (84.39) | 899 (83.40) | 825 (85.49) | 1 | 0.192 |
| Yes | 319 (15.61) | 179 (16.60) | 140 (14.51) | 1.17 (0.92–1.49) | |
| Labor duration—stage 1 (min)—Me (IQR) | 240 (170–360) | 293 (200–405) | 205 (150–290) | - | <0.01 |
| Labor duration—stage 2 (min)—Me (IQR) | 16 (10–30) | 25 (15–40) | 10 (8–20) | - | <0.01 |
| Labor duration—stage 3 (min)—Me (IQR) | 10 (10–10) | 10 (10–10) | 10 (10–10) | - | 0.432 |
| Labor duration (min)—Me (IQR) | 280 (195–400) | 331 (240–445) | 225 (170–313) | - | <0.01 |
| Blood loss (ml)—Me (IQR) | 500 (400–500) | 500 (400–500) | 500 (350–500) | - | 0.590 |
| Hospital stay (days)—Me (IQR) | 8 (6–13) | 8 (6–13) | 8 (5–13) | - | <0.01 |
| Variables | Total | Primipara n = 1078 | Multipara n = 965 | OR (95% CI) | p-Value |
|---|---|---|---|---|---|
| 1-min APGAR score—n (%) | |||||
| ≤7 | 479 (23.45) | 230 (21.34) | 249 (25.80) | 1 | 0.017 |
| >7 | 1564 (76.55) | 848 (78.66) | 716 (74.20) | 1.28 (1.05–1.57) | |
| 5-min APGAR score—n (%) | |||||
| ≤7 | 280 (13.71) | 132 (12.24) | 148 (15.34) | 1 | 0.043 |
| >7 | 1763 (86.29) | 946 (87.76) | 817 (84.66) | 1.30 (1.01–1.67) | |
| Birth weight (grams)—Me (IQR) | 2340 (1750–2750) | 2300 (1750–2690) | 2400 (1730–2800) | - | 0.018 |
| NICU transfer—n (%) | |||||
| No | 676 (33.09) | 334 (30.98) | 342 (35.44) | 1 | 0.033 |
| Yes | 1367 (66.91) | 744 (69.02) | 623 (64.56) | 1.22 (1.02–1.47) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szyszka, M.; Rzońca, E.; Rychlewicz, S.; Bączek, G.; Ślęzak, D.; Rzońca, P. Association between Parity and Preterm Birth—Retrospective Analysis from a Single Center in Poland. Healthcare 2023, 11, 1763. https://doi.org/10.3390/healthcare11121763
Szyszka M, Rzońca E, Rychlewicz S, Bączek G, Ślęzak D, Rzońca P. Association between Parity and Preterm Birth—Retrospective Analysis from a Single Center in Poland. Healthcare. 2023; 11(12):1763. https://doi.org/10.3390/healthcare11121763
Chicago/Turabian StyleSzyszka, Monika, Ewa Rzońca, Sylwia Rychlewicz, Grażyna Bączek, Daniel Ślęzak, and Patryk Rzońca. 2023. "Association between Parity and Preterm Birth—Retrospective Analysis from a Single Center in Poland" Healthcare 11, no. 12: 1763. https://doi.org/10.3390/healthcare11121763
APA StyleSzyszka, M., Rzońca, E., Rychlewicz, S., Bączek, G., Ślęzak, D., & Rzońca, P. (2023). Association between Parity and Preterm Birth—Retrospective Analysis from a Single Center in Poland. Healthcare, 11(12), 1763. https://doi.org/10.3390/healthcare11121763