
Acupuncture Decreases Risk of Hypertension in Patients with Chronic Spontaneous Urticaria in Taiwan: A Nationwide Study

 ,
,  , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Population
2.3. Primary Endpoint and Confounding Variables
2.4. Statistical Analysis
3. Results
3.1. Demographic Characteristics of Study Population
3.2. Risk of Hypertension According to Whether the CSU Patients Underwent Acupuncture and Other Covariates
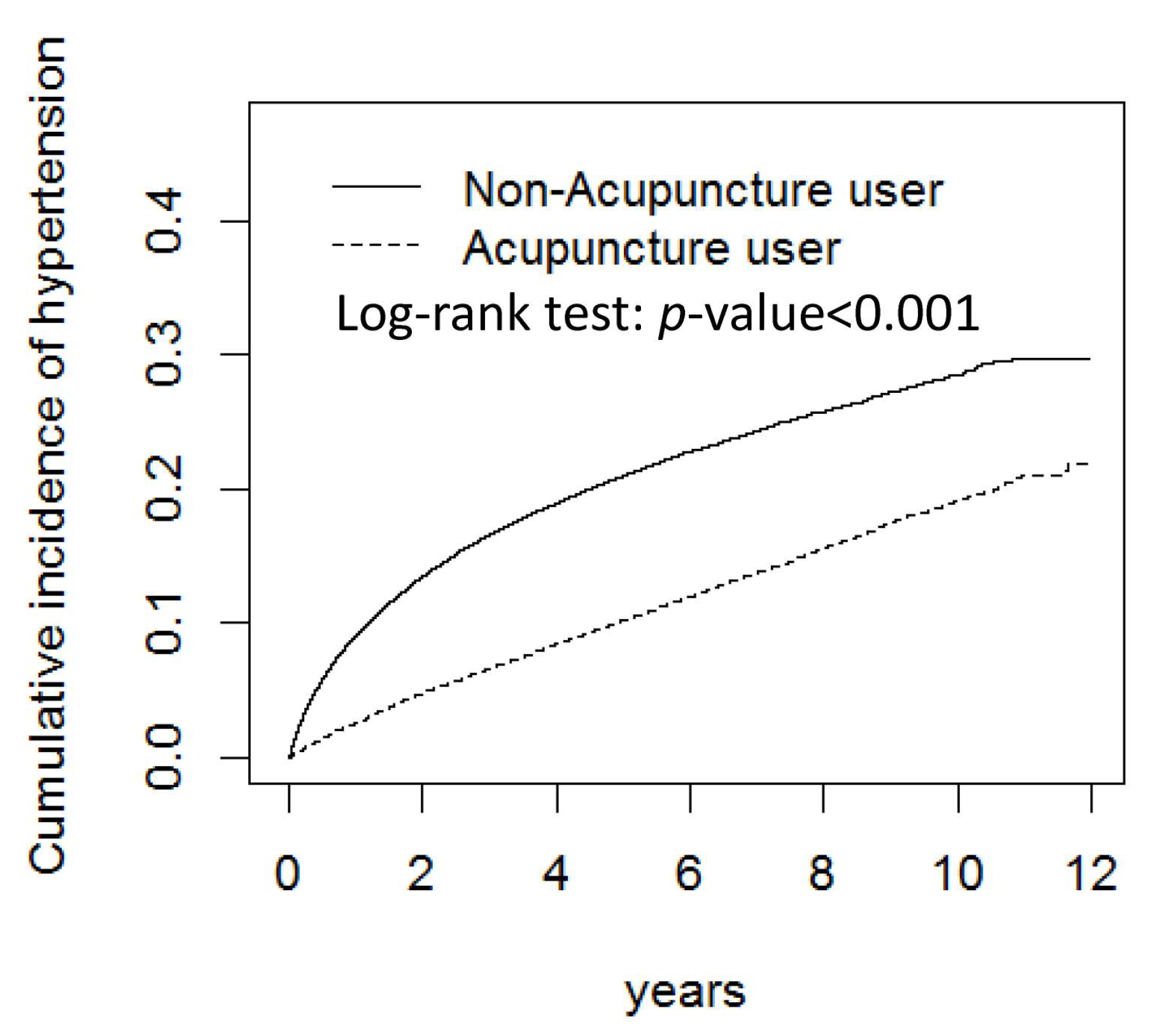
3.3. Risk of Hypertension among Patients with CSU Who Received and Did Not Receive Acupuncture
3.4. The Interaction EFFECT of Medication and Acupuncture on Hypertension
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kokubo, Y.; Kamide, K.; Okamura, T.; Watanabe, M.; Higashiyama, A.; Kawanishi, K.; Okayama, A.; Kawano, Y. Impact of high-normal blood pressure on the risk of cardiovascular disease in a Japanese urban cohort: The Suita study. Hypertension 2008, 52, 652–659. [Google Scholar] [CrossRef] [PubMed]
- Evangelista, A.; Isselbacher, E.M.; Bossone, E.; Gleason, T.G.; Eusanio, M.D.; Sechtem, U.; Ehrlich, M.P.; Trimarchi, S.; Braverman, A.C.; Myrmel, T.; et al. Insights From the International Registry of Acute Aortic Dissection: A 20-Year Experience of Collaborative Clinical Research. Circulation 2018, 137, 1846–1860. [Google Scholar] [CrossRef] [PubMed]
- Di Palo, K.E.; Barone, N.J. Hypertension and Heart Failure: Prevention, Targets, and Treatment. Heart Fail. Clin. 2020, 16, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Wilson, P.W. Established risk factors and coronary artery disease: The Framingham Study. Am. J. Hypertens. 1994, 7, 7S–12S. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018, 71, e13–e115. [Google Scholar] [CrossRef]
- Chang, H.W.; Cheng, H.M.; Yen, H.R.; Hsu, C.Y.; Lee, Y.C.; Chiang, J.H.; Sun, M.F. Association between chronic idiopathic urticaria and hypertension: A population-based retrospective cohort study. Ann. Allergy Asthma Immunol. 2016, 116, 554–558. [Google Scholar] [CrossRef]
- Zuberbier, T.; Aberer, W.; Asero, R.; Abdul Latiff, A.H.; Baker, D.; Ballmer-Weber, B.; Bernstein, J.A.; Bindslev-Jensen, C.; Brzoza, Z.; Buense Bedrikow, R.; et al. The EAACI/GA(2)LEN/EDF/WAO guideline for the definition, classification, diagnosis and management of urticaria. Allergy 2018, 73, 1393–1414. [Google Scholar] [CrossRef]
- Nebiolo, F.; Bergia, R.; Bommarito, L.; Bugiani, M.; Heffler, E.; Carosso, A.; Castiglioni, G.; Guida, G.; Badiu, I.; Pizzimenti, S.; et al. Effect of arterial hypertension on chronic urticaria duration. Ann. Allergy Asthma Immunol. 2009, 103, 407–410. [Google Scholar] [CrossRef]
- Chen, F.P.; Kung, Y.Y.; Chen, T.J.; Hwang, S.J. Demographics and patterns of acupuncture use in the Chinese population: The Taiwan experience. J. Altern. Complement. Med. 2006, 12, 379–387. [Google Scholar] [CrossRef]
- Ishizaki, N.; Yano, T.; Kawakita, K. Public status and prevalence of acupuncture in Japan. Evid. Based Complement. Altern. Med. 2010, 7, 493–500. [Google Scholar] [CrossRef]
- Hwang, J.H.; Han, D.W.; Yoo, E.K.; Kim, W.Y. The utilisation of Complementary and Alternative Medicine (CAM) among ethnic minorities in South Korea. BMC Complement. Altern. Med. 2014, 14, 103. [Google Scholar] [CrossRef] [PubMed]
- Upchurch, D.M.; Rainisch, B.W. A sociobehavioral wellness model of acupuncture use in the United States, 2007. J. Altern. Complement. Med. 2014, 20, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Vincent, A.; Kruk, K.M.; Cha, S.S.; Bauer, B.A.; Martin, D.P. Utilisation of acupuncture at an academic medical centre. Acupunct. Med. 2010, 28, 189–190. [Google Scholar] [CrossRef]
- Cramer, H.; Chung, V.C.; Lauche, R.; Zhang, Y.; Zhang, A.; Langhorst, J.; Dobos, G. Characteristics of acupuncture users among internal medicine patients in Germany. Complement. Ther. Med. 2015, 23, 423–429. [Google Scholar] [CrossRef]
- Xue, C.C.; Zhang, A.L.; Lin, V.; Myers, R.; Polus, B.; Story, D.F. Acupuncture, chiropractic and osteopathy use in Australia: A national population survey. BMC Public Health 2008, 8, 105. [Google Scholar] [CrossRef]
- Huang, M.C.; Yen, H.R.; Lin, C.L.; Lee, Y.C.; Sun, M.F.; Wu, M.Y. Acupuncture decreased the risk of stroke among patients with fibromyalgia in Taiwan: A nationwide matched cohort study. PLoS ONE 2020, 15, e0239703. [Google Scholar] [CrossRef]
- Hsing, A.W.; Ioannidis, J.P. Nationwide Population Science: Lessons From the Taiwan National Health Insurance Research Database. JAMA Intern. Med. 2015, 175, 1527–1529. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.Y.; Lee, Y.C.; Lin, C.L.; Huang, M.C.; Sun, M.F.; Yen, H.R. Trends in use of acupuncture among adults in Taiwan from 2002 to 2011: A nationwide population-based study. PLoS ONE 2018, 13, e0195490. [Google Scholar] [CrossRef] [PubMed]
- Makris, T.K.; Stavroulakis, G.A.; Krespi, P.G.; Hatzizacharias, A.N.; Triposkiadis, F.K.; Tsoukala, C.G.; Votteas, V.V.; Kyriakidis, M.K. Fibrinolytic/hemostatic variables in arterial hypertension: Response to treatment with irbesartan or atenolol. Am. J. Hypertens. 2000, 13, 783–788. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Yanase, Y.; Takahagi, S.; Ozawa, K.; Hide, M. The Role of Coagulation and Complement Factors for Mast Cell Activation in the Pathogenesis of Chronic Spontaneous Urticaria. Cells 2021, 10, 1759. [Google Scholar] [CrossRef]
- Parslew, R.; Pryce, D.; Ashworth, J.; Friedmann, P.S. Warfarin treatment of chronic idiopathic urticaria and angio-oedema. Clin. Exp. Allergy 2000, 30, 1161–1165. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.J.; Gona, P.; Larson, M.G.; Levy, D.; Benjamin, E.J.; Tofler, G.H.; Jacques, P.F.; Meigs, J.B.; Rifai, N.; Selhub, J.; et al. Multiple biomarkers and the risk of incident hypertension. Hypertension 2007, 49, 432–438. [Google Scholar] [CrossRef] [PubMed]
- Takahagi, S.; Mihara, S.; Iwamoto, K.; Morioke, S.; Okabe, T.; Kameyoshi, Y.; Hide, M. Coagulation/fibrinolysis and inflammation markers are associated with disease activity in patients with chronic urticaria. Allergy 2010, 65, 649–656. [Google Scholar] [CrossRef] [PubMed]
- Kasperska-Zajac, A.; Grzanka, A.; Misiolek, M.; Mazur, B.; Machura, E. Pentraxin-3 as a local inflammatory marker in chronic spontaneous urticaria. Cytokine 2015, 76, 566–568. [Google Scholar] [CrossRef] [PubMed]
- Mathis, K.W.; Broome, H.J.; Ryan, M.J. Autoimmunity: An underlying factor in the pathogenesis of hypertension. Curr. Hypertens. Rep. 2014, 16, 424. [Google Scholar] [CrossRef]
- Agache, I.; Rocha, C.; Pereira, A.; Song, Y.; Alonso-Coello, P.; Sola, I.; Beltran, J.; Posso, M.; Akdis, C.A.; Akdis, M.; et al. Efficacy and safety of treatment with omalizumab for chronic spontaneous urticaria: A systematic review for the EAACI Biologicals Guidelines. Allergy 2021, 76, 59–70. [Google Scholar] [CrossRef]
- Tharp, M.D.; Bernstein, J.A.; Kavati, A.; Ortiz, B.; MacDonald, K.; Denhaerynck, K.; Abraham, I.; Lee, C.S. Benefits and Harms of Omalizumab Treatment in Adolescent and Adult Patients With Chronic Idiopathic (Spontaneous) Urticaria: A Meta-analysis of “Real-world” Evidence. JAMA Dermatol. 2019, 155, 29–38. [Google Scholar] [CrossRef]
- Toubi, E.; Blant, A.; Kessel, A.; Golan, T.D. Low-dose cyclosporin A in the treatment of severe chronic idiopathic urticaria. Allergy 1997, 52, 312–316. [Google Scholar] [CrossRef]
- Stener-Victorin, E.; Baghaei, F.; Holm, G.; Janson, P.O.; Olivecrona, G.; Lonn, M.; Manneras-Holm, L. Effects of acupuncture and exercise on insulin sensitivity, adipose tissue characteristics, and markers of coagulation and fibrinolysis in women with polycystic ovary syndrome: Secondary analyses of a randomized controlled trial. Fertil. Steril. 2012, 97, 501–508. [Google Scholar] [CrossRef]
- Li, N.; Guo, Y.; Gong, Y.; Zhang, Y.; Fan, W.; Yao, K.; Chen, Z.; Dou, B.; Lin, X.; Chen, B.; et al. The Anti-Inflammatory Actions and Mechanisms of Acupuncture from Acupoint to Target Organs via Neuro-Immune Regulation. J. Inflamm. Res. 2021, 14, 7191–7224. [Google Scholar] [CrossRef]
- Inci, H.; Inci, F. Acupuncture Effects on Blood Parameters in Patients with Fibromyalgia. Med. Acupunct. 2021, 33, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Shi, G.X.; Tu, J.F.; Wang, T.Q.; Yang, J.W.; Wang, L.Q.; Lin, L.L.; Wang, Y.; Li, Y.T.; Liu, C.Z. Effect of Electro-Acupuncture (EA) and Manual Acupuncture (MA) on Markers of Inflammation in Knee Osteoarthritis. J. Pain. Res. 2020, 13, 2171–2179. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhu, F.; Huang, W.; Chen, Z.; Zhao, P.; Lei, Y.; Liu, Y.; Liu, X.; Sun, B.; Li, H. Therapeutic Effect and Mechanism of Acupuncture in Autoimmune Diseases. Am. J. Chin. Med. 2022, 50, 639–652. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.K.; Bae, H. Acupuncture and immune modulation. Auton. Neurosci. 2010, 157, 38–41. [Google Scholar] [CrossRef]
- Ginty, A.T.; Carroll, D.; Roseboom, T.J.; Phillips, A.C.; de Rooij, S.R. Depression and anxiety are associated with a diagnosis of hypertension 5 years later in a cohort of late middle-aged men and women. J. Hum. Hypertens. 2013, 27, 187–190. [Google Scholar] [CrossRef]
- Sensoy, B.; Gunes, A.; Ari, S. Anxiety and depression levels in Covid-19 disease and their relation to hypertension. Clin. Exp. Hypertens. 2021, 43, 237–241. [Google Scholar] [CrossRef]
- Scalco, A.Z.; Scalco, M.Z.; Azul, J.B.; Lotufo Neto, F. Hypertension and depression. Clinics 2005, 60, 241–250. [Google Scholar] [CrossRef]
- Bergantin, L.B. Depression Rises the Risk of Hypertension Incidence: Discussing the Link through the Ca2+/cAMP Signalling. Curr. Hypertens. Rev. 2020, 16, 73–78. [Google Scholar] [CrossRef]
- Hamam, M.S.; Kunjummen, E.; Hussain, M.S.; Nasereldin, M.; Bennett, S.; Miller, J. Anxiety, Depression, and Pain: Considerations in the Treatment of Patients with Uncontrolled Hypertension. Curr. Hypertens. Rep. 2020, 22, 106. [Google Scholar] [CrossRef]
- Choi, G.S.; Nam, Y.H.; Park, C.S.; Kim, M.Y.; Jo, E.J.; Park, H.K.; Kim, H.K. Anxiety, depression, and stress in Korean patients with chronic urticaria. Korean J. Intern. Med. 2020, 35, 1507–1516. [Google Scholar] [CrossRef]
- Huang, Y.; Xiao, Y.; Jing, D.; Li, J.; Zhang, J.; Chen, X.; Shen, M. Association of Chronic Spontaneous Urticaria with Anxiety and Depression in Adolescents: A Mediation Analysis. Front. Psychiatry 2021, 12, 655802. [Google Scholar] [CrossRef]
- Tat, T.S. Higher Levels of Depression and Anxiety in Patients with Chronic Urticaria. Med. Sci. Monit. 2019, 25, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Tzur Bitan, D.; Berzin, D.; Cohen, A. The association of chronic spontaneous urticaria (CSU) with anxiety and depression: A nationwide cohort study. Arch. Dermatol. Res. 2021, 313, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Amorim, D.; Amado, J.; Brito, I.; Fiuza, S.M.; Amorim, N.; Costeira, C.; Machado, J. Acupuncture and electroacupuncture for anxiety disorders: A systematic review of the clinical research. Complement. Ther. Clin. Pract. 2018, 31, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.A.; de Lacey, S.; Chapman, M.; Ratcliffe, J.; Norman, R.J.; Johnson, N.P.; Fahey, P. The effects of acupuncture on the secondary outcomes of anxiety and quality of life for women undergoing IVF: A randomized controlled trial. Acta Obstet. Gynecol. Scand. 2019, 98, 460–469. [Google Scholar] [CrossRef]
- Armour, M.; Smith, C.A.; Wang, L.Q.; Naidoo, D.; Yang, G.Y.; MacPherson, H.; Lee, M.S.; Hay, P. Acupuncture for Depression: A Systematic Review and Meta-Analysis. J. Clin. Med. 2019, 8, 1140. [Google Scholar] [CrossRef]
- Liu, C.; Zhao, Y.; Qin, S.; Wang, X.; Jiang, Y.; Wu, W. Randomized controlled trial of acupuncture for anxiety and depression in patients with chronic insomnia. Ann. Transl. Med. 2021, 9, 1426. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Acupuncture | p-Value | SMD | |||
|---|---|---|---|---|---|---|
| No (N = 43,547) | Yes (N = 43,547) | |||||
| n | % | n | % | |||
| Sex | 0.44 | |||||
| Female | 29,762 | 68.3 | 29,868 | 68.6 | 0.005 | |
| Male | 13,785 | 31.7 | 13,679 | 31.4 | 0.005 | |
| Age mean ± SD (years) | 40.2 ± 13.2 | 40.1 ± 13.0 | 0.43 a | 0.005 | ||
| Age group | 0.21 | |||||
| 20–39 | 33,192 | 76.2 | 33,268 | 76.4 | 0.004 | |
| 40–65 | 8282 | 19.0 | 8315 | 19.1 | 0.002 | |
| ≥65 | 2073 | 4.76 | 1964 | 4.51 | 0.012 | |
| Urbanization level ‡ | 0.74 | |||||
| 1 | 24,502 | 56.3 | 24,399 | 56.0 | 0.005 | |
| 2 | 16,604 | 38.1 | 16,638 | 38.2 | 0.002 | |
| 3 | 1902 | 4.37 | 1950 | 4.48 | 0.005 | |
| 4+ | 539 | 1.24 | 560 | 1.29 | 0.004 | |
| Monthly income (NTD) † | 0.84 | |||||
| <20,000 | 6311 | 14.5 | 6360 | 14.6 | 0.003 | |
| 20,001–39,999 | 24,435 | 56.1 | 24,356 | 55.9 | 0.004 | |
| ≥40,000 | 12,801 | 29.4 | 12,831 | 29.5 | 0.002 | |
| Occupation | 0.99 | |||||
| White-collar | 26,290 | 60.4 | 26,297 | 60.4 | 0.001 | |
| Blue-collar | 11,073 | 25.4 | 11,059 | 25.4 | 0.001 | |
| Others & | 6184 | 14.2 | 6191 | 14.2 | 0.001 | |
| Comorbidity | ||||||
| Diabetes mellitus | 5427 | 12.5 | 5493 | 12.6 | 0.50 | 0.005 |
| Hyperlipidemia | 9148 | 21.0 | 9309 | 21.4 | 0.18 | 0.009 |
| Medication | ||||||
| Cetirizine | 34,502 | 79.2 | 37,481 | 86.1 | <0.001 | 0.181 |
| Desloratadine | 15,688 | 36.0 | 18,393 | 42.2 | <0.001 | 0.138 |
| Fexofenadine | 38,815 | 89.1 | 40,811 | 93.7 | <0.001 | 0.164 |
| Levocetirizine | 27,441 | 63.0 | 31,142 | 71.5 | <0.001 | 0.182 |
| Loratadine | 28,415 | 65.3 | 31,355 | 72.0 | <0.001 | 0.146 |
| Follow time, years (mean, median) | (5.26, 2.85) | (3.50, 4.99) | 0.615 | |||
| Variable | Event | 1000 Person-Years | IR | Crude | Adjusted $ | ||
|---|---|---|---|---|---|---|---|
| N = 12,559 | HR (95% CI) | p-Value | HR (95% CI) | p-Value | |||
| Acupuncture | |||||||
| No | 7593 | 152,567 | 49.8 | 1 (Reference) | 1 (Reference) | ||
| Yes | 4966 | 228,993 | 21.7 | 0.47 (0.46, 0.49) | <0.001 | 0.58 (0.55, 0.60) | <0.001 |
| Sex | |||||||
| Female | 7517 | 265,328 | 28.3 | 1 (Reference) | 1 (Reference) | ||
| Male | 5.042 | 116,232 | 43.4 | 1.52 (1.46, 1.57) | <0.001 | 1.22 (1.18, 1.27) | <0.001 |
| Age (years) | |||||||
| 20–39 | 6278 | 306,833 | 20.5 | 1 (Reference) | 1 (Reference) | ||
| 40–65 | 4466 | 63,047 | 70.8 | 3.32 (3.20, 3.45) | <0.001 | 2.32 (2.23, 2.42) | <0.001 |
| ≥65 | 1815 | 11,680 | 155.4 | 6.86 (6.51, 7.23) | <0.001 | 3.78 (3.57, 4.00) | <0.001 |
| Urbanization level ‡ | |||||||
| 1 | 6659 | 215,987 | 30.8 | 1.16 (0.97, 1.38) | 0.10 | 1.16 (0.97, 1.38) | 0.10 |
| 2 | 5047 | 144,753 | 34.9 | 1.31 (1.10, 1.56) | 0.003 | 1.23 (1.03, 1.46) | 0.02 |
| 3 | 723 | 15,944 | 45.4 | 1.68 (1.39, 2.02) | <0.001 | 1.31 (1.09, 1.58) | 0.004 |
| 4+ | 130 | 4877 | 26.7 | 1 (Reference) | 1 (Reference) | ||
| Monthly income (NTD) † | |||||||
| <20,000 | 2342 | 53,213 | 44.0 | 1.57 (1.49, 1.66) | <0.001 | 1.42 (1.13, 1.79) | 0.001 |
| 20,001–39,999 | 7034 | 212,911 | 33.0 | 1.19 (1.14, 1.24) | <0.001 | 1.02 (0.97, 1.07) | 0.40 |
| ≥40,000 | 3183 | 115,436 | 27.6 | 1 (Reference) | 1 (Reference) | ||
| Occupation | |||||||
| White-collar | 6127 | 234,346 | 26.2 | 1 (Reference) | 1 (Reference) | ||
| Blue-collar | 4165 | 95,051 | 43.8 | 1.67 (1.60, 1.73) | <0.001 | 1.22 (1.17, 1.28) | <0.001 |
| Others & | 2267 | 52,163 | 43.5 | 1.65 (1.57, 1.73) | <0.001 | 0.79 (0.62, 0.99) | 0.04 |
| Comorbidities | |||||||
| Diabetes mellitus | |||||||
| No | 9810 | 335,730 | 29.2 | 1 (Reference) | 1 (Reference) | ||
| Yes | 2749 | 45,830 | 60.0 | 2.04 (1.95, 2.12) | <0.001 | 1.15 (1.10, 1.21) | <0.001 |
| Hyperlipidemia | |||||||
| No | 8077 | 303,649 | 26.6 | 1 (Reference) | 1 (Reference) | ||
| Yes | 4482 | 77,911 | 57.5 | 2.14 (2.07, 2.22) | <0.001 | 1.51 (1.45, 1.58) | <0.001 |
| Medications | |||||||
| Cetirizine | |||||||
| No | 4307 | 56,319 | 76.5 | 1 (Reference) | 1 (Reference) | ||
| Yes | 8252 | 325,241 | 25.4 | 0.34 (0.33, 0.36) | <0.001 | 0.62 (0.60, 0.65) | <0.001 |
| Desloratadine | |||||||
| No | 9027 | 225,286 | 40.1 | 1 (Reference) | 1 (Reference) | ||
| Yes | 3532 | 156,274 | 22.6 | 0.57 (0.55, 0.60) | <0.001 | 0.93 (0.89, 0.97) | <0.001 |
| Fexofenadine | |||||||
| No | 3773 | 23,511 | 160.5 | 1 (Reference) | 1 (Reference) | ||
| Yes | 8786 | 358,049 | 24.5 | 0.16 (0.16, 0.17) | <0.001 | 0.32 (0.31, 0.33) | <0.0001 |
| Levocetirizine | |||||||
| No | 7370 | 115,600 | 63.8 | 1 (Reference) | 1 (Reference) | ||
| Yes | 5189 | 265,961 | 19.5 | 0.31 (0.30, 0.32) | <0.001 | 0.50 (0.48, 0.52) | <0.001 |
| Loratadine | |||||||
| No | 5942 | 109,516 | 54.3 | 1 (Reference) | 1 (Reference) | ||
| Yes | 6617 | 272,044 | 24.3 | 0.46 (0.44, 0.48) | <0.001 | 0.77 (0.74, 0.80) | <0.001 |
| Non-Acupuncture | Acupuncture | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variable | Event | 1000 Person-Years | IR | Event | 1000 Person-Years | IR | Crude | Adjusted $ | ||
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |||||||
| Sex | ||||||||||
| Female | 4575 | 106,632 | 42.9 | 2942 | 158,697 | 18.5 | 0.47 (0.45, 0.49) | <0.001 | 0.52 (0.50, 0.55) | <0.001 |
| Male | 3018 | 45,935 | 65.7 | 2024 | 70,297 | 28.8 | 0.48 (0.45, 0.51) | <0.001 | 0.56 (0.53, 0.60) | <0.001 |
| Age (years) | ||||||||||
| 20–39 | 3792 | 124,381 | 30.5 | 2486 | 182,451 | 13.6 | 0.47 (0.45, 0.50) | <0.001 | 0.57 (0.54, 0.60) | <0.001 |
| 40–65 | 2745 | 23,799 | 115.3 | 1721 | 39,248 | 43.9 | 0.42 (0.40, 0.45) | <0.001 | 0.51 (0.48, 0.54) | <0.001 |
| ≥65 | 1056 | 4386 | 240.8 | 759 | 7294 | 104.1 | 0.48 (0.44, 0.53) | <0.001 | 0.57 (0.52, 0.62) | <0.001 |
| Comorbidity † | ||||||||||
| No | 4434 | 115,548 | 38.4 | 2793 | 170,320 | 16.4 | 0.47 (0.45, 0.49) | <0.001 | 0.54 (0.52, 0.57) | <0.001 |
| Yes | 3159 | 37,019 | 85.3 | 2173 | 58,674 | 37.0 | 0.47 (0.44, 0.49) | <0.001 | 0.53 (0.50, 0.56) | <0.001 |
| Medications | ||||||||||
| Cetirizine | ||||||||||
| No | 2944 | 27,582 | 106.7 | 1363 | 28,737 | 47.4 | 0.51 (0.48, 0.54) | <0.001 | 0.54 (0.51, 0.58) | <0.001 |
| Yes | 4649 | 124,985 | 37.2 | 3603 | 200,256 | 18.0 | 0.51 (0.49, 0.53) | <0.001 | 0.54 (0.52, 0.56) | <0.001 |
| Desloratadine | ||||||||||
| No | 5705 | 95,098 | 60.0 | 3322 | 130,188 | 25.5 | 0.47 (0.45, 0.49) | <0.001 | 0.54 (0.51, 0.56) | <0.001 |
| Yes | 1888 | 57,469 | 32.9 | 1644 | 98,806 | 16.6 | 0.53 (0.49, 0.56) | <0.001 | 0.54 (0.51, 0.58) | <0.001 |
| Fexofenadine | ||||||||||
| No | 2542 | 11,938 | 212.9 | 1231 | 11,574 | 106.4 | 0.58 (0.54, 0.62) | <0.001 | 0.58 (0.54, 0.62) | <0.001 |
| Yes | 5051 | 140,629 | 35.9 | 3735 | 217,420 | 17.2 | 0.50 (0.48, 0.53) | <0.001 | 0.53 (0.51, 0.56) | <0.001 |
| Levocetirizine | ||||||||||
| No | 4850 | 52,620 | 92.2 | 2520 | 62,980 | 40.0 | 0.49 (0.47, 0.52) | <0.001 | 0.53 (0.50, 0.55) | <0.001 |
| Yes | 2743 | 99,947 | 27.4 | 2446 | 166,013 | 14.7 | 0.55 (0.52, 0.58) | <0.001 | 0.56 (0.53, 0.59) | <0.001 |
| Loratadine | ||||||||||
| No | 3925 | 47,882 | 80.5 | 2017 | 60,744 | 33.2 | 0.46 (0.44, 0.49) | <0.001 | 0.53 (0.50, 0.56) | <0.001 |
| Yes | 3668 | 103,795 | 35.3 | 2949 | 168,249 | 17.5 | 0.52 (0.50, 0.55) | <0.001 | 0.55 (0.52, 0.58) | <0.001 |
| Variable | Crude | Adjusted $ | ||
|---|---|---|---|---|
| SHR (95% CI) | p-Value | SHR (95% CI) | p-Value | |
| Acupuncture | ||||
| No | 1 (Reference) | 1 (Reference) | ||
| Yes | 0.48 (0.46, 0.50) | <0.001 | 0.56 (0.54, 0.58) | <0.001 |
| Acupuncture | Medication | N | Event | 1000 Person-Years | IR | Crude HR (95% CI) | Adjusted HR $ (95% CI) |
|---|---|---|---|---|---|---|---|
| No | No | 995 | 712 | 1719 | 414.2 | 1.00 | 1.00 |
| No | Yes | 42,552 | 6881 | 150,848 | 45.6 | 0.13 (0.12, 0.14) *** | 0.21 (0.19, 0.24) *** |
| Yes | No | 339 | 195 | 1053 | 185.1 | 0.52 (0.44, 0.62) *** | 0.51 (0.42, 0.62) *** |
| Yes | Yes | 43,208 | 4771 | 227,940 | 20.9 | 0.06 (0.06, 0.07) *** | 0.10 (0.09, 0.12) *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, H.-W.; Lin, W.-D.; Shih, P.-J.; Peng, S.-L.; Hsu, C.-Y.; Lin, C.-L.; Liao, W.-L.; Sun, M.-F. Acupuncture Decreases Risk of Hypertension in Patients with Chronic Spontaneous Urticaria in Taiwan: A Nationwide Study. Healthcare 2023, 11, 1510. https://doi.org/10.3390/healthcare11101510
Chang H-W, Lin W-D, Shih P-J, Peng S-L, Hsu C-Y, Lin C-L, Liao W-L, Sun M-F. Acupuncture Decreases Risk of Hypertension in Patients with Chronic Spontaneous Urticaria in Taiwan: A Nationwide Study. Healthcare. 2023; 11(10):1510. https://doi.org/10.3390/healthcare11101510
Chicago/Turabian StyleChang, Heng-Wei, Wei-De Lin, Pai-Jun Shih, Shin-Lei Peng, Chung-Y. Hsu, Cheng-Li Lin, Wen-Ling Liao, and Mao-Feng Sun. 2023. "Acupuncture Decreases Risk of Hypertension in Patients with Chronic Spontaneous Urticaria in Taiwan: A Nationwide Study" Healthcare 11, no. 10: 1510. https://doi.org/10.3390/healthcare11101510
APA StyleChang, H.-W., Lin, W.-D., Shih, P.-J., Peng, S.-L., Hsu, C.-Y., Lin, C.-L., Liao, W.-L., & Sun, M.-F. (2023). Acupuncture Decreases Risk of Hypertension in Patients with Chronic Spontaneous Urticaria in Taiwan: A Nationwide Study. Healthcare, 11(10), 1510. https://doi.org/10.3390/healthcare11101510