
A Retrospective Study of Epidemiological Correlations of Food, Drug and Chemical Poisoning in Al-Baha, Western Saudi Arabia
 ,
,  , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Methodology and Data Collection Analysis
2.2. Statistical Analysis
2.3. Patient and Public Participation
3. Results
3.1. Aspects of Food Toxicity Instances in the Al-Baha Region
3.1.1. Demographic Variables
3.1.2. Correlation between Infection Severity, Type of Organism Involved, Signs and Symptoms, and Antibiotics Prescribed by Age Group
3.2. Aspects of Drug Toxicity Instances in the Al-Baha Region
3.3. Aspects of Chemical Toxicity Instances in the Al-Baha Region
Distribution of Toxic Agents with Respect to Age
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bakhaidar, M.; Jan, S.; Farahat, F.; Attar, A.; Alsaywid, B.; Abuznadah, W. Pattern of drug overdose and chemical poisoning among patients attending an emergency department, western Saudi Arabia. J. Community Health 2015, 40, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Rather, I.A.; Koh, W.Y.; Paek, W.K.; Lim, J. The Sources of Chemical Contaminants in Food and Their Health Implications. Front. Pharmacol. 2017, 8, 830. [Google Scholar] [CrossRef] [PubMed]
- Alghadeer, S.; Alrohaimi, M.; Althiban, A.; Kalagi, N.A.; Balkhi, B.; Khan, A.A. The patterns of children poisoning cases in community teaching hospital in Riyadh, Saudi Arabia. Saudi Pharm. J. 2018, 26, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Alzahrani, S.H.; Alqahtani, A.H.; Farahat, F.M.; Elnour, M.A.G.; Bashawri, J. Drug poisoning and associated factors in western Saudi Arabia: A five-year retrospective chart review (2011–2016). Pak. J. Med. Sci. 2017, 33, 1188–1193. [Google Scholar] [CrossRef]
- Al-Mazrou, Y.Y. Food poisoning in Saudi Arabia. Potential for prevention? Saudi Med. J. 2004, 25, 11–14. [Google Scholar]
- Aljoudi, A.S.; Al-Mazam, A.; Choudhry, A.J. Outbreak of food borne Salmonella among guests of a wedding ceremony: The role of cultural factors. J. Fam. Community Med. 2010, 17, 29–34. [Google Scholar] [CrossRef]
- Behera, A.; Singla, N.; Sharma, N.; Sharma, N. Paradigm shift in pattern and prevalence of poisoning during COVID-19 pandemic. J. Fam. Med. Prim. Care 2022, 1, 208–214. [Google Scholar]
- Boshehri, B.; Salimi, S.; Ranjbar, S. Mortality from acute poisoning in urmia: A three-year retrospective study. Iran. Red. Crescent Med. J. 2012, 14, 838–839. [Google Scholar] [CrossRef]
- Mathias, T.L.; Guidoni, C.M.; Girotto, E. Trends of drug-related poisoning cases attended to at a poison control center. Rev. Bras. Epidemiol. 2019, 22, e190018. [Google Scholar] [CrossRef]
- Ahmadi, A.; Pakravan, N.; Ghazizadeh, Z. Pattern of acute food, drug, and chemical poisoning in Sari City, Northern Iran. Hum. Exp. Toxicol. 2010, 29, 731–738. [Google Scholar] [CrossRef]
- Alnasser, S.M. Drug and Chemical Poisoning Patterns in Makkah Region, Saudi Arabia. Drug Res. 2022, 72, 148–155. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Yu, B.; Wang, N.; Li, T. Acute poisoning in Shenyang, China: A retrospective and descriptive study from 2012 to 2016. BMJ Open 2018, 8, e021881. [Google Scholar] [CrossRef] [PubMed]
- Galvez-Ruiz, A.; Elkhamary, S.M.; Asghar, N.; Bosley, T.M. Visual and neurologic sequelae of methanol poisoning in Saudi Arabia. Saudi Med. J. 2015, 36, 568–574. [Google Scholar] [CrossRef]
- Alnasser, S.; Hussain, S.M.; Kirdi, T.S.; Ahmed, A. Aluminum phosphide poisoning in Saudi Arabia over a nine-year period. Ann. Saudi Med. 2018, 38, 277–283. [Google Scholar] [CrossRef]
- Persson, H.; Sjöberg, G.; Haines, J.; Pronczuk de Garbino, J. Poisoning severity score: Grading of acute poisoning. J. Toxicol. Clin. Toxicol. 1998, 36, 205–213. [Google Scholar] [CrossRef]
- Bronstein, A.C.; Spyker, D.A.; Cantilena, L.R.; Rumack, B.H.; Dart, R.C. Annual report of the American Association of Poison Control Centers’ National Poison Data System (NPDS): 29th Annual Report. Clin. Toxicol. 2012, 50, 911–1164. [Google Scholar] [CrossRef] [PubMed]
- Ray, L.C.; Collins, J.P.; Griffin, P.M.; Shah, H.J.; Boyle, M.M.; Cieslak, P.R.; Dunn, J.; Lathrop, S.; McGuire, S.; Rissman, T.; et al. Decreased Incidence of Infections Caused by Pathogens Transmitted Commonly Through Food During the COVID-19 Pandemic—Foodborne Diseases Active Surveillance Network, 10 U.S. Sites, 2017–2020. Morb. Mortal. Wkly. Rep. 2021, 70, 1332–1336. [Google Scholar] [CrossRef] [PubMed]
- Alnasser, S.; Hussain, S.M.; Alnughaymishi, I.M.; Alnuqaydan, A.M. Pattern of food, drug and chemical poisoning in Qassim region, Saudi Arabia from January 2017 to December 2017. Toxicol. Rep. 2020, 15, 1438–1442. [Google Scholar] [CrossRef] [PubMed]
- Gautret, P.; Benkouiten, S.; Sridhar, S.; Al-Tawfiq, J.A.; Memish, Z.A. Diarrhea at the Hajj and Umrah. Travel Med. Infect. Dis. 2015, 13, 159–166. [Google Scholar] [CrossRef]
- Bintsis, T. Foodborne pathogens. AIMS Microbiol. 2017, 3, 529–563. [Google Scholar] [CrossRef]
- Yue, M.; Liu, D.; Li, X.; Jin, S.; Hu, X.; Zhao, X.; Wu, Y. Epidemiology, Serotype and Resistance of Salmonella Isolates from a Children’s Hospital in Hangzhou, Zhejiang, China, 2006–2021. Infect. Drug Resist. 2022, 15, 4735–4748. [Google Scholar] [CrossRef] [PubMed]
- Abdul-Mutalib, N.A.; Syafinaz, A.N.; Sakai, K.; Shirai, Y. An overview of foodborne illness and food safety in Malaysia. Int. Food Res. 2015, 6, 896–901. [Google Scholar]
- Qi, X.; Li, P.; Xu, X.; Yuan, Y.; Bu, S.; Lin, D. Epidemiological and Molecular Investigations on Salmonella Responsible for Gastrointestinal Infections in the Southwest of Shanghai from 1998 to 2017. Front. Microbiol. 2019, 10, 2025. [Google Scholar] [CrossRef] [PubMed]
- Kunwar, R.; Singh, H.; Mangla, V.; Hiremath, R. Outbreak investigation: Salmonella food poisoning. Med. J. Armed Forces India 2013, 69, 388–391. [Google Scholar] [CrossRef]
- Okumus, B.; Sönmez, S.; Moore, S.; Auvil, D.P.; Parks, G.D. Exploring safety of food truck products in a developed country. Int. J. Hosp. Manag. 2019, 81, 150–158. [Google Scholar] [CrossRef]
- Guyer, B.; Mavor, A. Institute of Medicine Committee on Poison Prevention and Control. Forging a poison prevention and control system: Report of an Institute of Medicine committee. Ambul. Pediatr. 2005, 5, 197–200. [Google Scholar] [CrossRef]
- Al Madni, O.M.; Kharoshah, M.A.; Zaki, M.K.; Ghaleb, S.S. Hanging deaths in Dammam, Kingdom of Saudi Arabia. J. Forensic Leg. Med. 2010, 17, 265–268. [Google Scholar] [CrossRef]
- Kanchan, T.; Menezes, R.G. Suicidal poisoning in Southern India: Gender differences. J. Forensic Leg. Med. 2008, 15, 7–14. [Google Scholar] [CrossRef]
- Ibrahim, N.K.; Alamoudi, B.M.; Baamer, W.O.; Al-Raddadi, R.M. Self-medication with analgesics among medical students and interns in King Abdulaziz University, Jeddah, Saudi Arabia. Pak. J. Med. Sci. 2015, 31, 14–18. [Google Scholar] [CrossRef]
- Alnasser, S.M.; Kordi, T.S.; Asiri, A.A.; Gupta, D.K.; Alfadl, A.A.; Hussain, A.S.M. Epidemiology of Chemical Poisoning among Adults in Qassim Region: An Eight-Year Study. Toxics 2022, 10, 709. [Google Scholar] [CrossRef]
- Damalas, C.A.; Eleftherohorinos, I.G. Pesticide exposure, safety issues, and risk assessment indicators. Int. J. Environ. Res. Public Health 2011, 8, 1402–1419. [Google Scholar] [CrossRef] [PubMed]
- Brent, J.; McMartin, K.; Phillips, S.; Aaron, C.; Kulig, K. Fomepizole for the treatment of methanol poisoning. N. Engl. J. Med. 2001, 344, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Wahba, M.A.; Alshehri, B.M.; Hefny, M.M.; Al Dagrer, R.A.; Al-Malki, S.D. Incidence and profile of acute intoxication among adult population in Najran, Saudi Arabia: A retrospective study. Sci. Prog. 2021, 104, 368504211011339. [Google Scholar] [CrossRef]
- Mladenka, P.; Applova, L.; Patocka, J.; Costa, V.M.; Remiao, F.; Pourova, J.; Mladenka, A.; Karlíckova, J.; Jahodar, L.; Voprsalova, M.; et al. Comprehensive review of cardiovascular toxicity of drugs and related agents. Med. Res. Rev. 2018, 38, 1332–1403. [Google Scholar] [CrossRef]
- Goh, L.Y.; Vitry, A.I.; Semple, S.J.; Esterman, A.; Luszcz, M.A. Self-medication with over-the-counter drugs and complementary medications in South Australia’s elderly population. BMC Complement. Altern. Med. 2009, 11, 9–42. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Severity Grade Score | Symptoms |
|---|---|
| None 0 | No symptoms or signs related to poisoning |
| Minor 1 | Diarrhea, fever, stomach cramps |
| Moderate 2 | Diarrhea, stomach cramps, occasional fever |
| Severe 3 | Fever with chills, severe headache, severe abdominal pain, micturition, nausea |
| Fatal 4 | Death |
| Age Group | n | % |
|---|---|---|
| 1–10 | 105 | 66% |
| 11–20 | 17 | 10.7% |
| 21–30 | 9 | 5.7% |
| 31–40 | 12 | 7.5% |
| ≥40 | 16 | 10.1% |
| Gender | ||
| Male | 85 | 53.5% |
| Female | 74 | 46.5% |
| Organism Type | ||
| Salmonella | 149 | 93.7% |
| Enterococcus species | 6 | 3.8% |
| E. coli | 4 | 2.5% |
| Region | ||
| Albaha | 109 | 68.5% |
| Qilwa | 4 | 2.5% |
| Alaqiq | 24 | 15.1% |
| Algara | 6 | 3.8% |
| Almandag | 10 | 6.3% |
| Bhaljureshi | 6 | 3.8% |
| Place of Poisoning | ||
| Home | 136 | 85.5% |
| Restaurants and weddings | 23 | 14.5% |
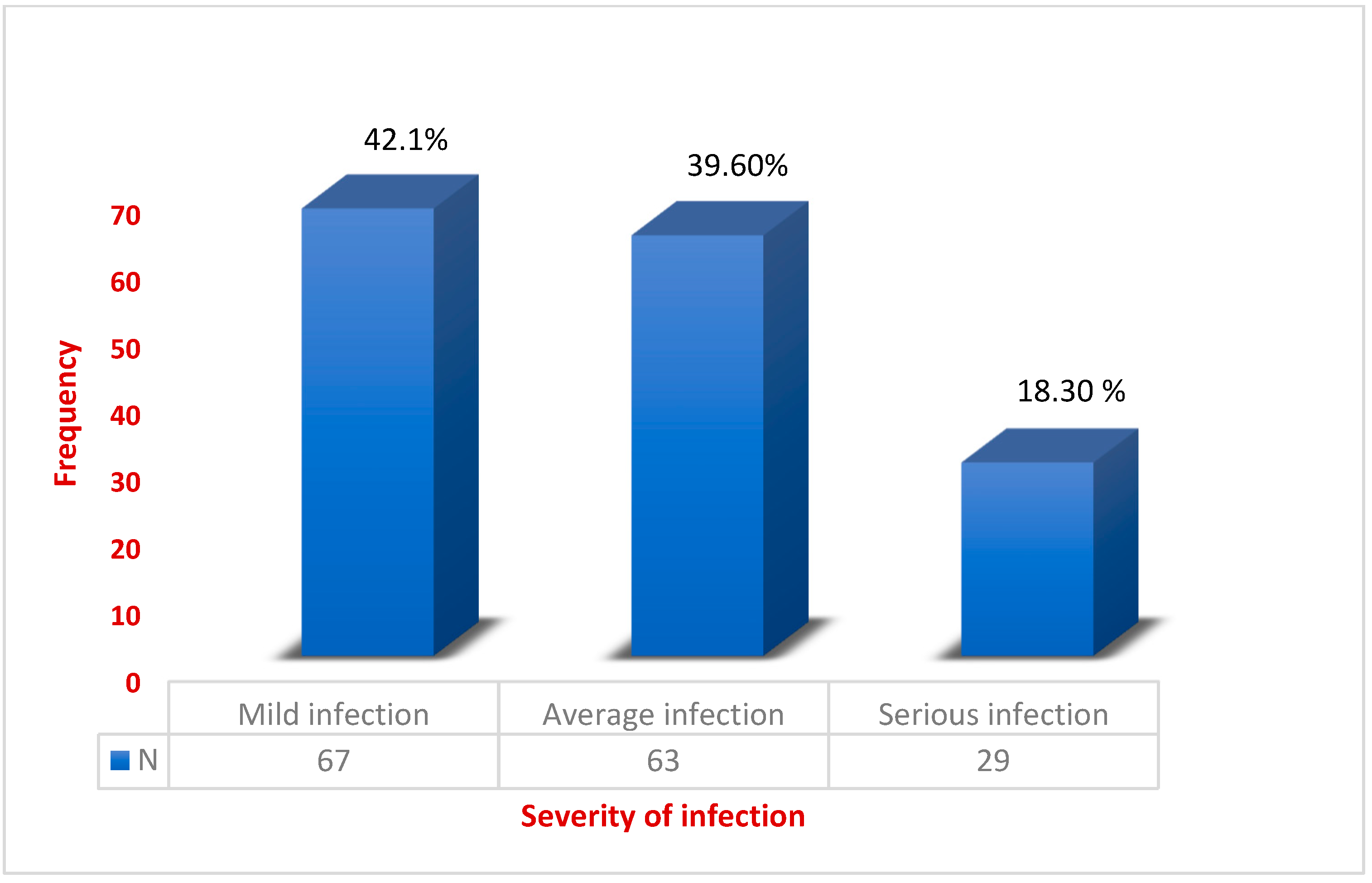
| Severity of Infection | ||
| Average infection | 63 | 39.6% |
| Mild infection | 67 | 42.1% |
| Serious infection | 29 | 18.3% |
| Type of Antibiotics | ||
| Augmentin | 78 | 49.1% |
| Cephalosporins | 29 | 18.2% |
| Quinolones | 35 | 22.0% |
| Penicillin | 17 | 10.7% |
| Year | ||
| 2019 | 34 | 21.4% |
| 2020 | 23 | 14.1% |
| 2021 | 68 | 42.8% |
| 2022 | 34 | 21.4% |
| Signs and Symptoms | ||
| Diarrhea, fever, stomach cramps | 150 | 94.3% |
| Fever with chills, severe headache, severe abdominal pain, micturition, nausea | 6 | 3.8% |
| Diarrhea, stomach cramps, occasional fever | 3 | 1.9% |
| Severity of Infection | 1–10 y | 11–20 y | 21–30 y | 31–40 y | ≥40 y | χ2 | p Value |
|---|---|---|---|---|---|---|---|
| Average infection | 43 | 9 | 4 | 2 | 5 | 21.123 | 0.001 s |
| Mild infection | 41 | 8 | 5 | 7 | 6 | ||
| Serious infection | 20 | 3 | 0 | 3 | 3 | ||
| Organism | |||||||
| Salmonella | 104 | 17 | 6 | 11 | 11 | 44.345 | 0.05 s |
| Enterococcus species | 0 | 0 | 1 | 1 | 4 | ||
| E. coli | 1 | 0 | 2 | 0 | 1 | ||
| Signs and Symptoms | |||||||
| Diarrhea, fever, stomach cramps | 104 | 17 | 6 | 11 | 12 | 48.392 | 0.001 s |
| Fever with chills, severe headache, severe abdominal pain, micturition, nausea | 0 | 0 | 1 | 1 | 4 | ||
| Diarrhea, stomach cramps, occasional fever | 1 | 0 | 2 | 0 | 0 | ||
| Antibiotics Prescribed | |||||||
| Augmentin | 73 | 5 | 0 | 0 | 0 | 103.678 | 0.001 s |
| cephalosporins | 21 | 5 | 0 | 0 | 3 | ||
| quinolones | 4 | 4 | 6 | 11 | 10 | ||
| Penicillin | 7 | 3 | 3 | 1 | 3 |
| Variables Categories | Frequency | % |
|---|---|---|
| Age Group | ||
| 1–10 | 120 | 31.8% |
| 11–20 | 101 | 26.8% |
| 21–30 | 74 | 19.6% |
| 31–40 | 47 | 12.5% |
| ≥40 | 35 | 9.3% |
| Gender | ||
| Male | 204 | 54.1% |
| Female | 173 | 45.9% |
| Type of Exposure | ||
| Accidental | 363 | 96.3% |
| Suicidal | 14 | 3.7% |
| Route of administration | ||
| Ingestion (Oral) | 350 | 92.83% |
| Inhalation (Nasal) | 20 | 5.30% |
| Other | 7 | 1.87% |
| Place of Residence | ||
| Al-Aqiq | 4 | 1.1% |
| Al-Baha | 216 | 57.3% |
| Al-Gara | 17 | 4.5% |
| Al-Hajra | 2 | 0.5% |
| Al-Mandaq | 2 | 0.5% |
| Al-Miha | 1 | 0.3% |
| Al-Mikhwah | 12 | 3.2% |
| Biljurashi | 103 | 27.3% |
| Namerah | 1 | 0.3% |
| Qilwa | 19 | 5.0% |
| Severity of infection | ||
| Mild infection | 97 | 25.7% |
| Average infection | 217 | 57.6% |
| Serious infection | 63 | 16.7% |
| Outcome | ||
| Recovered | 376 | 99.7% |
| Death | 1 | 0.3% |
| Nationality | ||
| Saudi | 360 | 95.5% |
| Non-Saudi | 17 | 4.5% |
| Year of Drug Poisoning | ||
| 2019 | 146 | 38.7% |
| 2020 | 76 | 20.2% |
| 2021 | 122 | 32.4% |
| 2022 | 33 | 8.8% |
| Type of Drugs | n | % | Females | Males |
|---|---|---|---|---|
| Analgesic | 66 | 17 | 39 | 27 |
| Antiarrhythmics | 1 | 0.3 | 1 | 0 |
| Antibiotics | 9 | 2.4 | 1 | 8 |
| Anticoagulants | 8 | 1.1 | 5 | 3 |
| Anticonvulsants | 20 | 5.6 | 6 | 14 |
| Antidepressants | 25 | 5.9 | 13 | 12 |
| Antidiabetic | 2 | 0.6 | 1 | 1 |
| Antiemetic | 2 | 0.5 | 2 | 0 |
| Antihistamine | 5 | 1.5 | 3 | 2 |
| Antilipemic | 1 | 0.3 | 1 | 0 |
| Antipsychotics | 8 | 1.1 | 2 | 6 |
| Antispasmodic drug | 1 | 0.3 | 1 | 0 |
| Antitussives | 5 | 4.1 | 0 | 5 |
| Aspirin | 10 | 2.7 | 2 | 1 |
| Atypical Antipsychotic | 15 | 2.8 | 8 | 7 |
| Beta agonists | 1 | 0.3 | 1 | 0 |
| Biguanides | 4 | 1 | 4 | 0 |
| Caffeine | 3 | 0.9 | 3 | 0 |
| Beta agonists | 1 | 0.3 | 1 | 0 |
| DPP-4 inhibitors | 1 | 0.3 | 1 | 0 |
| Drug of abuse | 3 | 0.9 | 0 | 3 |
| Fenethylline | 1 | 0.3 | 0 | 1 |
| Hormones | 3 | 0.9 | 1 | 2 |
| Hypertensive drugs | 4 | 1 | 1 | 3 |
| Laxatives | 4 | 1 | 3 | 1 |
| Leukotriene receptor antagonists | 1 | 0.3 | 1 | 0 |
| Multiple drug ingestion | 17 | 4.5 | 13 | 4 |
| Mycophenolic acid | 2 | 0.3 | 2 | 0 |
| NSAIDs | 12 | 3.1 | 7 | 5 |
| Opioid analgesics | 6 | 0.7 | 2 | 4 |
| Contraceptives | 2 | 1 | 0 | 1 |
| PDE5 inhibitors | 1 | 0.3 | 0 | 1 |
| Pentagon | 1 | 0.3 | 1 | 0 |
| Phenethylamine | 13 | 3.4 | 12 | 1 |
| Poisonous herbs | 1 | 0.3 | 0 | 1 |
| Proton pump inhibitors | 1 | 0.3 | 1 | 0 |
| Rythmodan | 1 | 0.3 | 0 | 1 |
| Skeletal muscle relaxants | 4 | 2 | 2 | 2 |
| Sulfonylurea | 2 | 0.6 | 2 | 0 |
| Teriflunomide | 1 | 0.6 | 1 | 0 |
| Tetrahydrocannabinol | 1 | 0.3 | 0 | 1 |
| Unknown | 113 | 30.5 | 34 | 79 |
| Vitamins | 5 | 0.8 | 3 | 2 |
| Xanthines | 1 | 0.3 | 1 | 0 |
| Type of Drug Toxicity | 1–10 | 11–20 | 21–30 | 31–40 | ≥40 |
|---|---|---|---|---|---|
| Analgesic Antiarrhythmics | 18 1 | 25 0 | 16 0 | 5 0 | 2 0 |
| Antibiotics | 2 | 3 | 1 | 1 | 2 |
| Anticoagulants | 5 | 1 | 0 | 2 | 0 |
| Anticonvulsants | 5 | 4 | 5 | 3 | 3 |
| Antidepressants | 0 | 6 | 2 | 14 | 3 |
| Antidiabetic | 0 | 1 | 0 | 1 | 0 |
| Antiemetic | 1 | 0 | 0 | 1 | 0 |
| Antihistamine | 5 | 0 | 0 | 0 | 0 |
| Antilipemic | 1 | 0 | 0 | 0 | 0 |
| Antipsychotics | 3 | 1 | 2 | 1 | 1 |
| Antispasmodic drug | 0 | 0 | 1 | 0 | 0 |
| Antitussives | 3 | 1 | 1 | 0 | 0 |
| Atypical Antipsychotic | 6 | 5 | 3 | 1 | 0 |
| Beta agonists | 0 | 0 | 1 | 0 | 0 |
| Biguanides | 1 | 2 | 1 | 0 | 0 |
| Caffeine | 1 | 2 | 0 | 0 | 0 |
| Contraceptives | 0 | 0 | 2 | 0 | 0 |
| DPP-4 inhibitors | 0 | 1 | 0 | 0 | 0 |
| Drug of abuse | 0 | 0 | 2 | 1 | 0 |
| fenethylline | 0 | 0 | 1 | 0 | 0 |
| Hormones | 2 | 0 | 0 | 1 | 0 |
| Hypertensive drugs | 0 | 1 | 3 | 0 | 0 |
| Laxatives | 3 | 1 | 0 | 0 | 0 |
| Leukotriene receptor antagonists | 1 | 0 | 0 | 0 | 0 |
| Multiple drug ingestion | 4 | 8 | 4 | 0 | 1 |
| Mycophenolic acid | 1 | 0 | 0 | 0 | 1 |
| NSAIDs | 3 | 4 | 3 | 2 | 0 |
| Opioid analgesics | 0 | 0 | 2 | 3 | 1 |
| PDE5 inhibitors | 0 | 0 | 0 | 1 | 0 |
| Pentagon | 0 | 0 | 1 | 0 | 0 |
| Phenethylamine | 0 | 3 | 4 | 5 | 1 |
| Poisonous herbs | 1 | 0 | 0 | 0 | 0 |
| Proton-pump inhibitors | 0 | 0 | 0 | 1 | 0 |
| Rythmodan | 1 | 0 | 0 | 0 | 0 |
| Skeletal muscle relaxants | 0 | 0 | 3 | 1 | 0 |
| Sulfonylurea | 1 | 0 | 0 | 1 | 0 |
| Teriflunomide | 0 | 1 | 0 | 0 | 0 |
| Tetrahydrocannabinol | 0 | 0 | 0 | 0 | 1 |
| Unknown | 25 | 29 | 24 | 15 | 21 |
| Vitamins | 5 | 0 | 0 | 0 | 0 |
| Xanthines | 0 | 1 | 0 | 0 | 0 |
| Variables Categories | Frequency | % |
|---|---|---|
| Age Group | ||
| 1–10 | 36 | 41.9% |
| 11–20 | 41 | 47.7% |
| 21–30 | 8 | 9.3% |
| ≥40 | 1 | 1.2% |
| Gender | ||
| Male | 64 | 74.4% |
| Female | 22 | 25.6% |
| Toxic agent | ||
| Clorox | 16 | 18.7% |
| Clorox + unknown drug | 6 | 6.9% |
| Dettol + unknown drug | 3 | 3.8% |
| Alcohol | 8 | 9.3% |
| Alcohol + unknown drug | 1 | 1.2% |
| Carbon monoxide | 2 | 2.3% |
| Chemical material | 1 | 1.2% |
| Hair dye | 5 | 3.5% |
| Insecticides + pesticides | 15 | 17.2% |
| Methanol + kerosine | 2 | 2.4% |
| Methanol + drug | 21 | 24.4% |
| Perfume spray | 2 | 2.4% |
| Mercury | 1 | 1.2% |
| Paint thinner | 1 | 1.2% |
| Printer ink | 1 | 1.2% |
| Unknown | 1 | 1.22% |
| Type for exposure | ||
| Accidental | 81 | 94.2% |
| Suicidal | 5 | 5.8% |
| Region | ||
| Al-Aqiq | 4 | 4.7% |
| Al-Baha | 47 | 54.7% |
| Al-Gara | 1 | 1.2% |
| Al-Hougra | 3 | 3.5% |
| Al-Mandaq | 1 | 1.2% |
| Al-Miha | 1 | 1.2% |
| AL-Mikhwah | 4 | 4.7% |
| Algara | 1 | 1.2% |
| Biljurashi | 13 | 15.1% |
| Namerah | 1 | 1.2% |
| Qilwa | 10 | 11.6% |
| Nationality | ||
| Saudi | 75 | 87.21% |
| Non-Saudi | 11 | 12.8% |
| Route of Administration | ||
| Dermal | 4 | 4.7% |
| Inhalation | 21 | 24.4% |
| Injection | 2 | 2.3% |
| Swallowing | 59 | 68.6% |
| Severity of Infection | ||
| Average infection | 42 | 48.8% |
| Mild infection | 16 | 18.6% |
| Serious infection | 28 | 32.5% |
| Recovery rate | ||
| Recovered | 85 | 98.8% |
| Death | 1 | 1.2% |
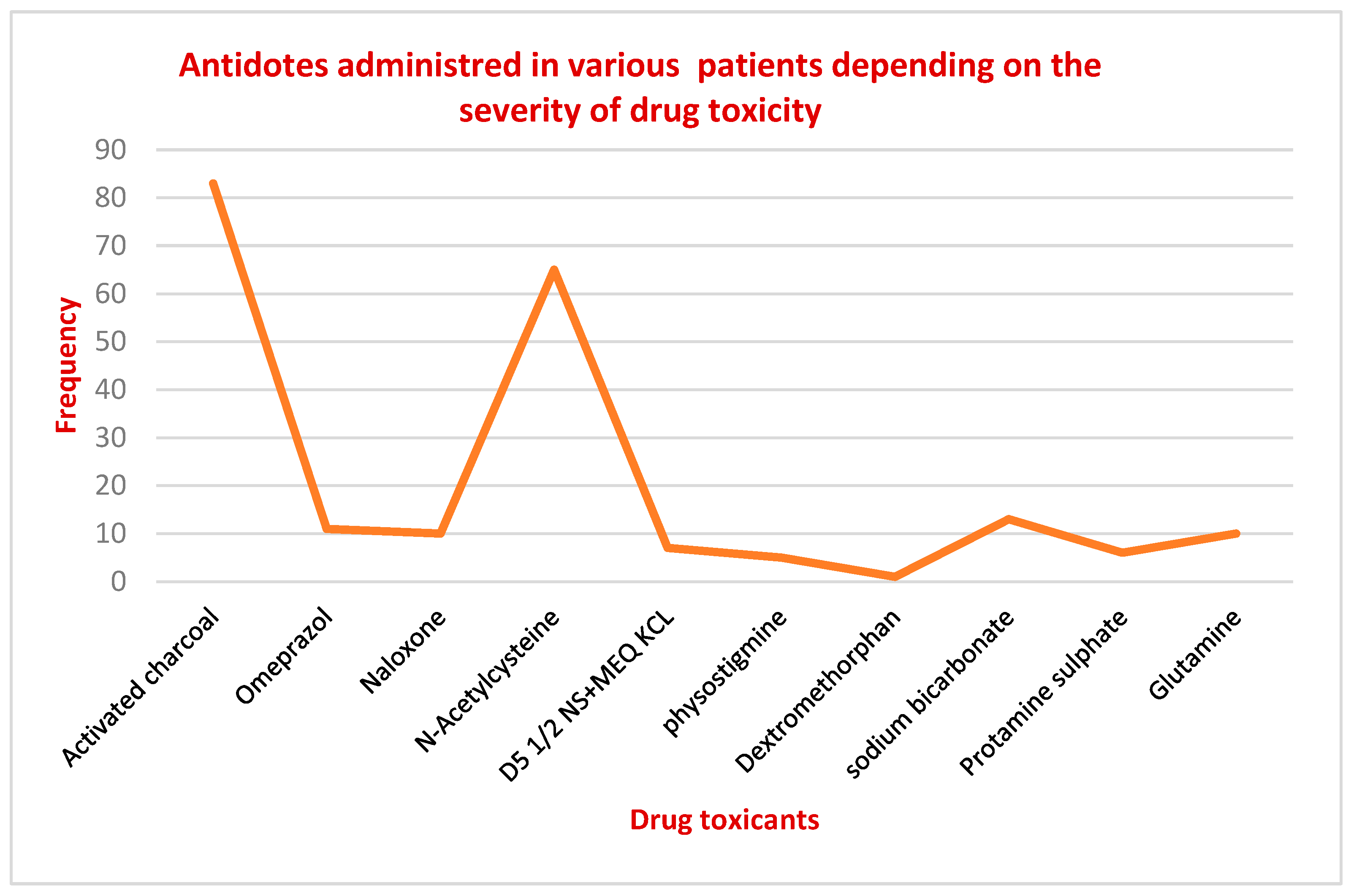
| Antidotes | ||
| Activated charcoal | 18 | 21% |
| Antiseptic cream | 3 | 3.5% |
| Atropine | 2 | 2.4% |
| Hydrocortisone + D5w | 4 | 5.9% |
| Clexane | 10 | 11.7% |
| D50w + sodium bicarbonate | 8 | 10.8% |
| Levoleucovorin calcium | 2 | 15.1% |
| Methylprednisolone | 12 | 13.2% |
| N-Acetylcysteine | 5 | 5.7% |
| No antidote | 1 | 1.2% |
| O2 mask | 4 | 4.7% |
| Omeprazole | 8 | 9.3% |
| Potassium chloride in NS | 2 | 2.4% |
| Pyridoxine hydrochloride B6 | 2 | 2.3% |
| Vitamin K1 | 5 | 5.8% |
| Year of Poisoning | ||
| 2019 | 15 | 17.4% |
| 2020 | 37 | 43.0% |
| 2021 | 15 | 17.4% |
| 2022 | 19 | 22.1% |
| Chemical Toxicant | M | F | χ2 | p Value |
|---|---|---|---|---|
| Clorox | 7 | 9 | ||
| Clorox + unknown drug | 5 | 1 | 46.190 | 0.05 s |
| Dettol + unknown drug | 2 | 1 | ||
| Alcohol | 8 | 0 | ||
| Alcohol + unknown drug | 0 | 1 | ||
| Carbon monoxide | 2 | 0 | ||
| Chemical material | 1 | 0 | ||
| Hair dye | 3 | 2 | ||
| Insecticides + pesticides | 5 | 10 | ||
| Methanol + kerosine | 0 | 2 | ||
| Methanol + drug | 14 | 7 | ||
| Perfume spray | 1 | 1 | ||
| Mercury | 1 | 0 | ||
| Paint thinner | 1 | 0 | ||
| Printer ink | 1 | 0 | ||
| Unknown | 1 | 0 | ||
| Toxicant source | ||||
| Accidental | 63 | 18 | ||
| Suicidal | 1 | 4 | ||
| Route of Administration | 8.258 | 0.01 s | ||
| Dermal | 3 | 1 | ||
| Inhalation | 11 | 10 | ||
| Injection | 1 | 1 | 0.05 s | |
| Swallowing | 49 | 10 | ||
| Types of Antidotes | 8.294 | |||
| Activated charcoal | 9 | 9 | ||
| Antiseptic cream | 3 | 0 | ||
| Atropine | 2 | 1 | ||
| Hydrocortisone + D5w | 3 | 1 | ||
| Clexane | 4 | 3 | ||
| D50w + sodium bicarbonate | 7 | 3 | ||
| Levoleucovorin calcium | 1 | 1 | ||
| Methylprednisolone | 11 | 1 | ||
| N-Acetylcysteine | 4 | 1 | 0.001 s | |
| No antidote | 0 | 1 | ||
| O2 mask | 5 | 0 | ||
| Omeprazole | 7 | 1 | 45.947 | |
| Potassium chloride in NS | 2 | 0 | ||
| Potassium hydrochloride B6 | 3 | 0 | ||
| Vitamin K1 | 4 | 1 |
| Recovery Rate | 1–10 y | 11–20 y | 21–30 y | ≥40 y | χ2 |
|---|---|---|---|---|---|
| Average infection | 26 | 6 | 9 | 1 | 28.038 0.001 s (p value) |
| Mild infection | 11 | 4 | 1 | 0 | |
| Serious infection | 5 | 12 | 10 | 1 | |
| Toxic agent | |||||
| Chlorox | 8 | 8 | 0 | 0 | 82.171 0.01 s (p value) |
| Chlorox + unknown drug | 1 | 2 | 2 | 1 | |
| Dettol + unknown drug | 2 | 1 | 0 | 0 | |
| Alcohol | 0 | 6 | 2 | 0 | |
| Alcohol + unknown drug | 0 | 1 | 0 | 0 | |
| Carbon monoxide | 0 | 2 | 0 | 0 | |
| Chemical material | 1 | 0 | 0 | 0 | |
| Hair dye | 0 | 0 | 0 | 5 | |
| Insecticides + pesticides | 5 | 5 | 1 | 4 | |
| Methanol + kerosine | 1 | 0 | 1 | 0 | |
| Methanol + drug | 11 | 4 | 3 | 3 | |
| Perfume spray | 1 | 0 | 1 | 0 | |
| Mercury | 0 | 0 | 0 | 1 | |
| Paint thinner | 0 | 1 | 1 | 0 | |
| Printer ink | 0 | 1 | 0 | 0 | |
| Unknown | 1 | 0 | 0 | 0 | |
| Type for exposure | 2.32 0.06 ns (p value) | ||||
| Accidental | 35 | 37 | 8 | 1 | |
| Suicidal | 1 | 4 | 0 | 0 | |
| Route of Administration | |||||
| Dermal | 3 | 0 | 1 | 0 | 3.632 0.06 ns (p value) |
| Inhalation | 3 | 11 | 3 | 2 | |
| Injection | 0 | 1 | 0 | 1 | |
| Swallowing | 26 | 16 | 16 | 1 | |
| Type of antidotes | |||||
| Activated charcoal | 9 | 7 | 1 | 1 | 41.24 0.942 ns (p value) |
| Antiseptic cream | 2 | 1 | 0 | 0 | |
| Atropine | 1 | 0 | 1 | 0 | |
| Hydrocortisone + D5w | 2 | 1 | 1 | 0 | |
| Clexane | 3 | 4 | 0 | 3 | |
| D50w + sodium bicarbonate | 6 | 1 | 0 | 1 | |
| Levoleucovorin calcium | 1 | 0 | 1 | 0 | |
| Methylprednisolone | 12 | 0 | 0 | 0 | |
| N-Acetylcysteine | 0 | 1 | 2 | 2 | |
| No antidote | 1 | 0 | 0 | 0 | |
| O2 mask | 2 | 1 | 1 | 0 | |
| Omeprazole | 1 | 1 | 4 | 2 | |
| Potassium chloride in NS | 2 | 0 | 0 | 0 | |
| Pyridoxine hydrochloride B6 | 1 | 0 | 1 | 0 | |
| Vitamin K1 | 0 | 1 | 4 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beigh, S.; Mahzari, A.; Alharbi, R.A.; Al-Ghamdi, R.A.; Alyahyawi, H.E.; Al-Zahrani, H.A.; Al-Jadani, S. A Retrospective Study of Epidemiological Correlations of Food, Drug and Chemical Poisoning in Al-Baha, Western Saudi Arabia. Healthcare 2023, 11, 1398. https://doi.org/10.3390/healthcare11101398
Beigh S, Mahzari A, Alharbi RA, Al-Ghamdi RA, Alyahyawi HE, Al-Zahrani HA, Al-Jadani S. A Retrospective Study of Epidemiological Correlations of Food, Drug and Chemical Poisoning in Al-Baha, Western Saudi Arabia. Healthcare. 2023; 11(10):1398. https://doi.org/10.3390/healthcare11101398
Chicago/Turabian StyleBeigh, Saba, Ali Mahzari, Read A. Alharbi, Rahaf A. Al-Ghamdi, Hanan E. Alyahyawi, Hind A. Al-Zahrani, and Saeedah Al-Jadani. 2023. "A Retrospective Study of Epidemiological Correlations of Food, Drug and Chemical Poisoning in Al-Baha, Western Saudi Arabia" Healthcare 11, no. 10: 1398. https://doi.org/10.3390/healthcare11101398
APA StyleBeigh, S., Mahzari, A., Alharbi, R. A., Al-Ghamdi, R. A., Alyahyawi, H. E., Al-Zahrani, H. A., & Al-Jadani, S. (2023). A Retrospective Study of Epidemiological Correlations of Food, Drug and Chemical Poisoning in Al-Baha, Western Saudi Arabia. Healthcare, 11(10), 1398. https://doi.org/10.3390/healthcare11101398