
Effect of Resistance Training on Body Composition, Hemodynamic Parameters and Exercise Tolerance among Patients with Coronary Artery Disease: A Systematic Review
 , , ,
, , ,  , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocols and Registration
2.2. Criteria for Considering Studies
2.3. Search Strategies and Data Resources
2.4. Data Extraction
2.5. Methodological Quality Assessment
2.6. Collecting, Summarizing and Reporting Results
3. Results
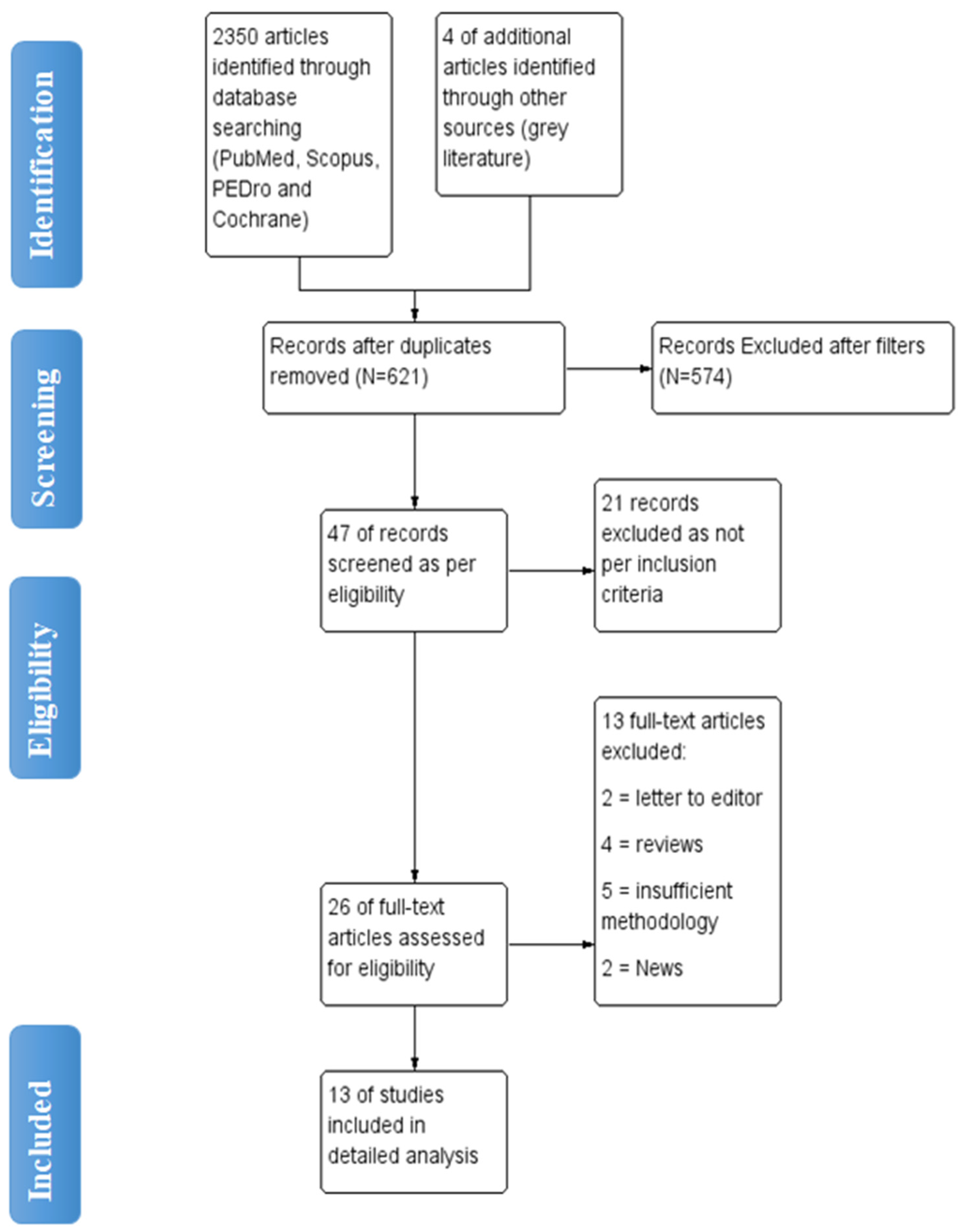
3.1. Selection of Studies
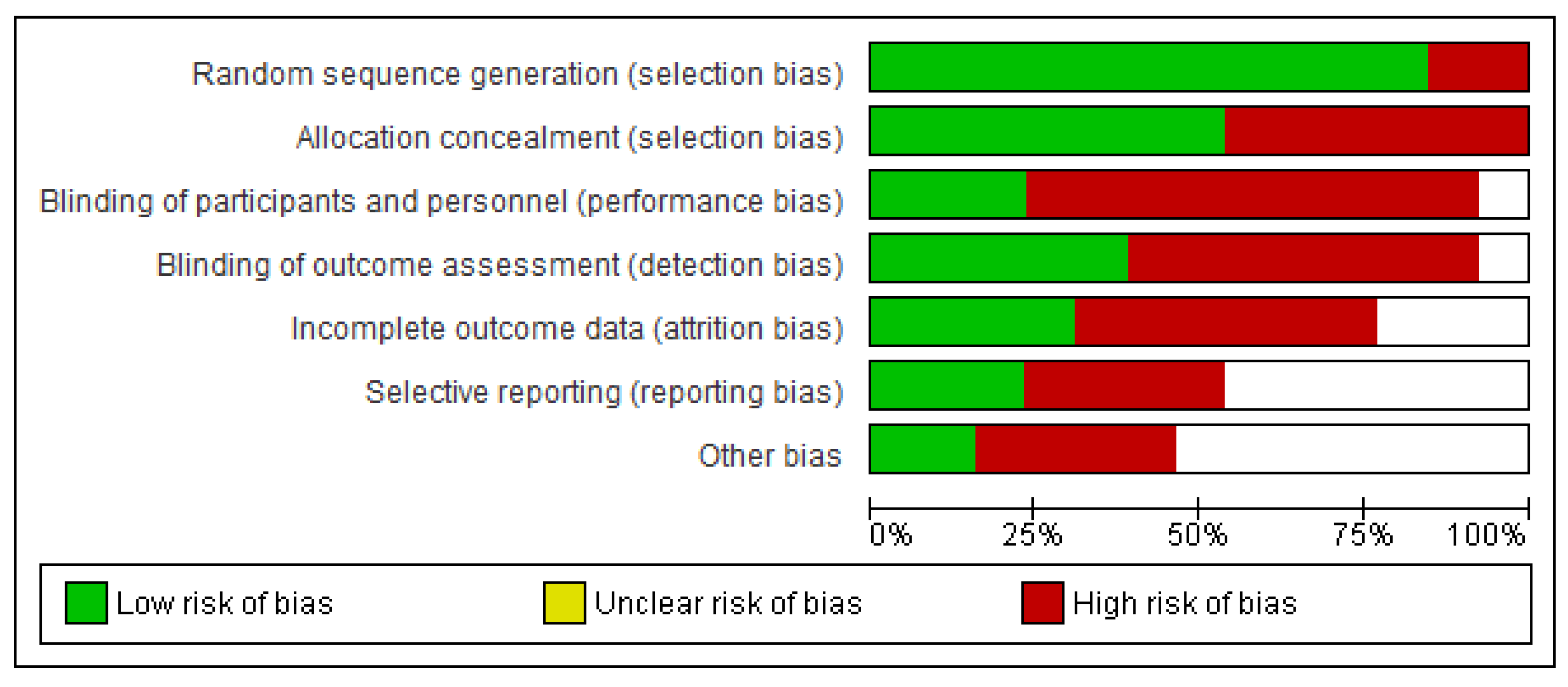
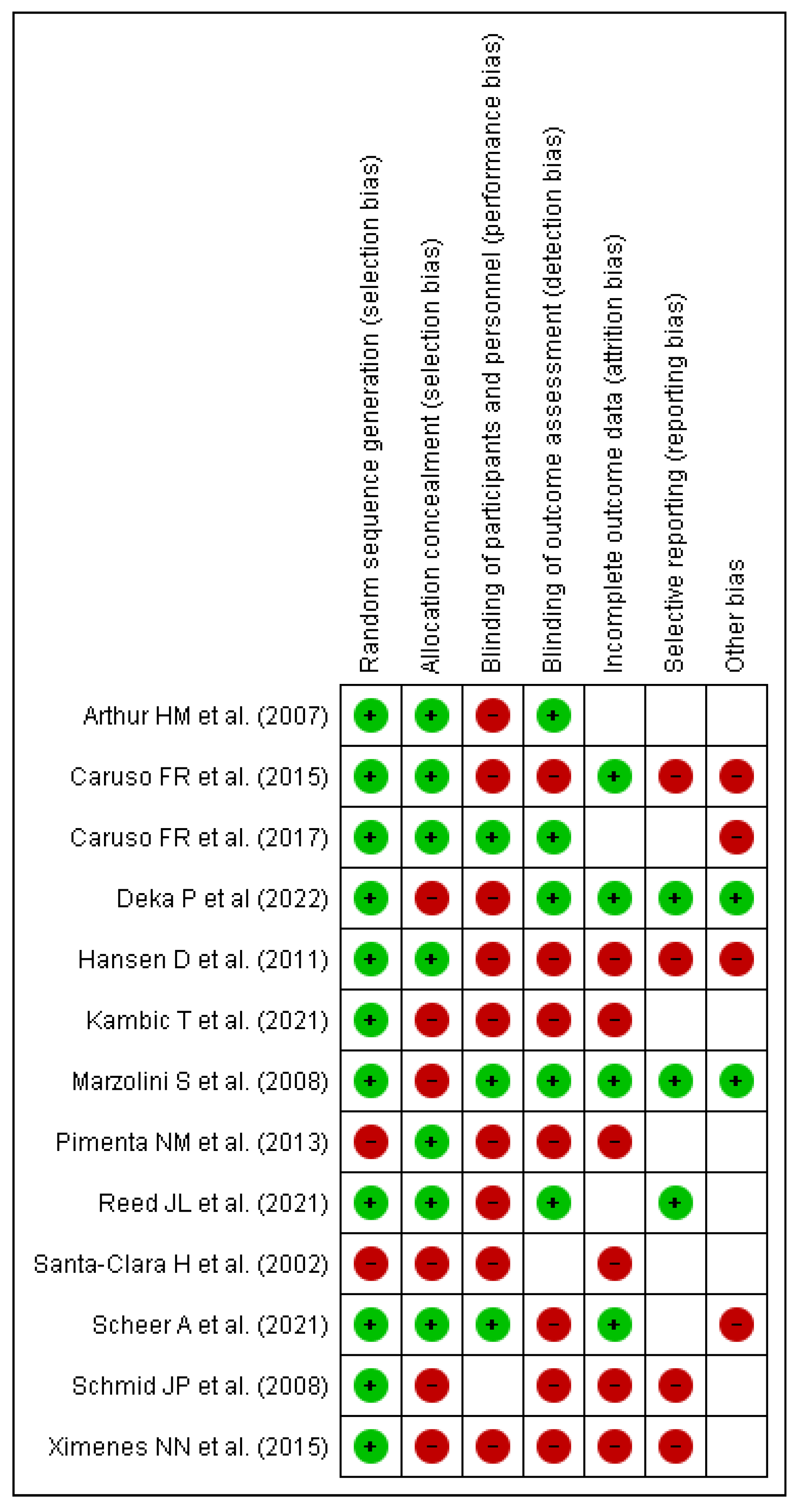
3.2. Risk of Bias Assessment
3.3. Main Findings
3.4. Impact on Hemodynamic and Metabolic Parameters
3.5. Impact on Exercise Tolerance and Peak Oxygen Consumption
3.6. Impact on Body Composition
3.7. Impact on Muscle Strength and Endurance
3.8. Impact on Sympathetic System Activity and Left Ventricular Remodeling
3.9. Psychological Benefits and Quality of Life
4. Discussion
5. Clinical Application
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Malakar, A.K.; Choudhury, D.; Halder, B.; Paul, P.; Uddin, A.; Chakraborty, S. A review on coronary artery disease, its risk factors, and therapeutics. J. Cell. Physiol. 2019, 234, 16812–16823. [Google Scholar] [CrossRef] [PubMed]
- McGill, H.C., Jr.; McMahan, C.A.; Herderick, E.E.; Tracy, R.E.; Malcom, G.T.; Zieske, A.W.; Strong, J.P. Effects of coronary heart disease risk factors on atherosclerosis of selected regions of the aorta and right coronary artery. PDAY Research Group. Pathobiological Determinants of Atherosclerosis in Youth. Arterioscler. Thromb. Vasc. Biol. 2000, 20, 836–845. [Google Scholar] [CrossRef] [PubMed]
- Bruning, R.S.; Sturek, M. Benefits of exercise training on coronary blood flow in coronary artery disease patients. Prog Cardiovasc Dis. 2015, 57, 543–553. [Google Scholar] [CrossRef]
- Solberg, L.A.; Strong, J.P. Risk factors and atherosclerotic lesions: A review of autopsy studies. Arteriosclerosis 1983, 3, 187–198. [Google Scholar] [CrossRef] [PubMed]
- Steg, P.G.; Ducrocq, G. Future of the Prevention and Treatment of Coronary Artery Disease. Circ. J. 2016, 80, 1067–1072. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.S.; Scirica, M.B.; Braunwald, E.; Murphy, S.A.; Ewa, K.-P.; Buros, J.L.; Chaitman, B.R.; Morrow, D.A. Efficacy of ranolazine in patients with chronic angina observations from the randomized, double-blind, placebo-controlled MERLIN-TIMI (Metabolic Efficiency with Ranolazine for Less Ischemia in Non-ST-Segment Elevation Acute Coronary Syndromes) 36 Trial. J. Am. Coll. Cardiol. 2009, 53, 1510–1516. [Google Scholar] [CrossRef] [PubMed]
- Serruys, P.W.; Morice, M.-C.; Kappetein, A.P.; Colombo, A.; Holmes, D.R.; Mack, M.J.; Ståhle, E.; Feldman, T.E.; Van Den Brand, M.; Bass, E.J.; et al. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N. Engl. J. Med. 2009, 360, 961–972. [Google Scholar] [CrossRef]
- Anderson, L.; Oldridge, N.; Thompson, D.R.; Zwisler, A.-D.; Rees, K.; Martin, N.; Taylor, R.S. Exercise-Based Cardiac Rehabilitation for Coronary Heart Disease: Cochrane Systematic Review and Meta-Analysis. J. Am. Coll. Cardiol. 2016, 67, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, P.A.; Boidin, M.; Juneau, M.; Nigam, A.; Gayda, M. High-intensity interval training in patients with coronary heart disease: Prescription models and perspectives. Ann. Phys. Rehabil. Med. 2017, 60, 50–57. [Google Scholar] [CrossRef]
- Hansen, D.; Eijnde, B.; Roelants, M.; Broekmans, T.; Rummens, J.; Hensen, K.; Daniels, A.; Van Erum, M.; Bonné, K.; Reyckers, I.; et al. Clinical benefits of the addition of lower extremity low- intensity resistance muscle training to early aerobic endurance training intervention in patients with coronary artery disease : A randomized controlled trial*. J. Rehabil. Med. 2011, 43, 800–807. [Google Scholar] [CrossRef]
- Caruso, F.R.; Arena, R.; A Phillips, S.A.; Bonjorno, J.C., Jr.; Mendes, R.G.; Arakelian, V.M.; Bassi, D.; Nogi, C.; Borghi-Silva, A. Resistance exercise training improves heart rate variability and muscle performance: A randomized controlled trial in coronary artery disease patients. Eur. J. Phys. Rehabil Med. 2015, 51, 281–289. [Google Scholar] [PubMed]
- Scheer, A.; Shah, A.; de Oliveira, B.I.R.; Moreno-Suarez, I.; Jacques, A.; Green, D.; Maiorana, A. Twelve weeks of water-based circuit training exercise improves fitness, body fat and leg strength in people with stable coronary heart disease: A randomised trial. J. Physiother. 2021, 67, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Reed, J.L.; Terada, T.; Cotie, L.M.; Tulloch, H.E.; Leenen, F.H.; Mistura, M.; Hans, H.; Wang, H.W.; Vidal-Almela, S.; Reid, R.D.; et al. Progress in Cardiovascular Diseases The effects of high-intensity interval training, Nordic walking and moderate-to-vigorous intensity continuous training on functional capacity, depression, and quality of life in patients with coronary artery disease enrolled in cardiac rehabilitation: A randomized controlled trial (CRX study). Prog. Cardiovasc. Dis. 2021. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Marzolini, S.; Oh, P.I.; Thomas, S.G.; Goodman, J.M. Aerobic and resistance training in coronary disease: Single versus multiple sets. Med. Sci. Sports Exerc. 2008, 40, 1557–1564. [Google Scholar] [CrossRef]
- Santa-Clara, H.; Fernhall, B.; Mendes, M.; Sardinha, L.B. Effect of a 1 year combined aerobic- and weight-training exercise programme on aerobic capacity and ventilatory threshold in patients suffering from coronary artery disease. Eur. J. Appl. Physiol. 2002, 87, 568–575. [Google Scholar] [CrossRef] [PubMed]
- Kambic, T.; Hadžić, V.; Lainscak, M. Hemodynamic Response to High- and Low-Load Resistance Exercise in Patients with Coronary Artery Disease: A Randomized, Crossover Clinical Trial. Int. J. Environ. Res. Public Health 2021, 18, 3905. [Google Scholar] [CrossRef]
- Caruso, F.R.; Bonjorno, J.C., Jr.; Arena, R.; Phillips, S.A.; Cabiddu, R.; Mendes, R.G.; Arakelian, V.M.; Bassi, D.; Borghi-Silva, A. Hemodynamic, Autonomic, Ventilatory, and Metabolic Alterations After Resistance Training in Patients with Coronary Artery Disease: A Randomized Controlled Trial. Am. J. Phys. Med. Rehabil. 2017, 96, 226–235. [Google Scholar] [CrossRef]
- Ximenes, N.N.; Borges, D.L.; Lima, R.O.; Barbosa e Silva, M.G.; Silva, L.N.; Costa Mde, A.; Baldez, T.E.; Nina, V.J. Effects of Resistance Exercise Applied Early After Coronary Artery Bypass Grafting: A Randomized Controlled Trial. Braz J. Cardiovasc. Surg. 2015, 30, 620–625. [Google Scholar] [CrossRef][Green Version]
- Deka, P.; Pathak, D.; Klompstra, L.; Sempere-Rubio, N.; Querol-Giner, F.; Marques-Sule, E. High-Intensity Interval and Resistance Training Improve Health Outcomes in Older Adults with Coronary Disease. J. Am. Med. Dir. Assoc. 2022, 23, 60–65. [Google Scholar] [CrossRef]
- Arthur, H.M.; Gunn, E.; Thorpe, K.E.; Ginis, K.M.; Mataseje, L.; McCartney, N.; McKelvie, R.S. Effect of aerobic vs combined aerobic-strength training on 1-year, post-cardiac rehabilitation outcomes in women after a cardiac event. J. Rehabil. Med. 2007, 39, 730–735. [Google Scholar] [CrossRef] [PubMed]
- Schmid, J.P.; Anderegg, M.; Romanens, M.; Morger, C.; Noveanu, M.; Hellige, G.; Saner, H. Combined endurance/resistance training early on, after a first myocardial infarction, does not induce negative left ventricular remodelling. Eur. J. Cardiovasc. Prev. Rehabil. 2008, 15, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Pimenta, N.M.; Santa-Clara, H.; Sardinha, L.B.; Fernhall, B. Body fat responses to a 1-year combined exercise training program in male coronary artery disease patients. Obesity (Silver Spring) 2013, 21, 723–730. [Google Scholar] [CrossRef] [PubMed]
- Vysoký, R.; Fiala, J.; Dosbaba, F.; Bat’alik, L.; Nehyba, S.; Ludka, O. Preventive training programme for patients after acute coronary event-correlation between selected parameters and age groups. Cent. Eur. J. Public Health 2015, 23, 208. [Google Scholar] [CrossRef]
- Khan, K.S.; Kunz, R.; Kleijnen, J.; Antes, G. Five steps to conducting a systematic review. J. R. Soc. Med. 2003, 96, 118–121. [Google Scholar] [CrossRef]
- Tibana, R.A.; Boullosa, D.A.; Leicht, A.S.; Prestes, J. Women with metabolic syndrome present different autonomic modulation and blood pressure response to an acute resistance exercise session compared with women without metabolic syndrome. Clin. Physiol. Funct. Imaging 2013, 33, 364–372. [Google Scholar] [CrossRef]
- Rognmo, Ø.; Moholdt, T.; Bakken, H.; Hole, T.; Mølstad, P.; Myhr, N.E.; Grimsmo, J.; Wisløff, U. Cardiovascular risk of high- versus moderate-intensity aerobic exercise in coronary heart disease patients. Circulation 2012, 126, 1436–1440. [Google Scholar] [CrossRef]
- Frankenstein, L.; Nelles, M.; Hallerbach, M.; Dukic, D.; Fluegel, A.; Schellberg, D.; Katus, H.; Remppis, A.; Zugck, C. Prognostic impact of peakVO2-changes in stable CHF on chronic beta-blocker treatment. Int. J. Cardiol. 2007, 122, 125–130. [Google Scholar] [CrossRef]
- Vromen, T.; Kraal, J.J.; Kuiper, J.; Spee, R.F.; Peek, N.; Kemps, H.M. The influence of training characteristics on the effect of aerobic exercise training in patients with chronic heart failure: A meta-regression analysis. Int. J. Cardiol. 2016, 208, 120–127. [Google Scholar] [CrossRef]
- Mandic, S.; Tymchak, W.; Kim, D.; Daub, B.; Quinney, H.A.; Taylor, D.; Al-Kurtass, S.; Haykowsky, M.J. Effects of aerobic or aerobic and resistance training on cardiorespiratory and skeletal muscle function in heart failure: A randomized controlled pilot trial. Clin. Rehabil. 2009, 23, 207–216. [Google Scholar] [CrossRef]
- Kavanagh, T.; Mertens, D.J.; Hamm, L.F.; Beyene, J.; Kennedy, J.; Corey, P.; Shephard, R.J. Prediction of long-term prognosis in 12 169 men referred for cardiac rehabilitation. Circulation 2002, 106, 666–671. [Google Scholar] [CrossRef] [PubMed]
- Michelini, L.C.; O’Leary, D.S.; Raven, P.B.; Nóbrega, A.C. Neural control of circulation and exercise: A translational approach disclosing interactions between central command, arterial baroreflex, and muscle metaboreflex. Am J Physiol Heart Circ Physiol. 2015, 309, H381–H392. [Google Scholar] [CrossRef] [PubMed]
- Fagard, R.H.; Cornelissen, V.A. Effect of exercise on blood pressure control in hypertensive patients. Eur. J. Cardiovasc. Prev. Rehabil. 2007, 14, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Lavie, C.J.; Milani, R.V. Cardiac rehabilitation and exercise training in secondary coronary heart disease prevention. Prog. Cardiovasc. Dis. 2011, 53, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Salvetti, X.M.; Oliveira, J.A.; Servantes, D.M.; Vincenzo de Paola, A.A. How much do the benefits cost? Effects of a home-based training programme on cardiovascular fitness, quality of life, programme cost and adherence for patients with coronary disease. Clin. Rehabil. 2008, 22, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Fisher, J.P.; Ogoh, S.; Dawson, E.A.; Fadel, P.J.; Secher, N.H.; Raven, P.B.; White, M.J. Cardiac and vasomotor components of the carotid baroreflex control of arterial blood pressure during isometric exercise in humans. J. Physiol. 2006, 572 Pt 3, 869–880. [Google Scholar] [CrossRef]
- Rezk, C.C.; Marrache, R.C.; Tinucci, T.; Mion DJr Forjaz, C.L. Post-resistance exercise hypotension, hemodynamics, and heart rate variability: Influence of exercise intensity. Eur. J. Appl. Physiol. 2006, 98, 105–112. [Google Scholar] [CrossRef]
- Lima, A.H.; Forjaz, C.L.; Silva, G.Q.; Menêses, A.L.; Silva, A.J.; Ritti-Dias, R.M. Acute effect of resistance exercise intensity in cardiac autonomic modulation after exercise. Arq Bras Cardiol. 2011, 96, 498–503. [Google Scholar] [CrossRef]
- Figueiredo, T.; Rhea, M.R.; Peterson, M.; Miranda, H.; Bentes, C.M.; Reis, V.; Simão, R. Influence of number of sets on blood pressure and heart rate variability after a strength training session. J. Strength Cond. Res. 2015, 29, 1556–1563. [Google Scholar] [CrossRef]
- Kingsley, J.D.; McMillan, V.; Figueroa, A. The effects of 12 weeks of resistance exercise training on disease severity and autonomic modulation at rest and after acute leg resistance exercise in women with fibromyalgia. Arch. Phys. Med. Rehabil. 2010, 91, 1551–1557. [Google Scholar] [CrossRef]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [PubMed]
- Shoemaker, J.K.; Mattar, L.; Kerbeci, P.; Trotter, S.; Arbeille, P.; Hughson, R.L. WISE 2005: Stroke volume changes contribute to the pressor response during ischemic handgrip exercise in women. J. Appl. Physiol. 2007, 103, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Ismail, H.; McFarlane, J.R.; Nojoumian, A.H.; Dieberg, G.; Smart, N.A. Clinical outcomes and cardiovascular responses to different exercise training intensities in patients with heart failure: A systematic review and meta-analysis. JACC Heart Fail. 2013, 1, 514–522. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Author | Country | Research Outline | Total Participants | Mean Age (Years) | Time of Assessment |
|---|---|---|---|---|---|
| Hansen, D. et al. [10] 2011 | Belgium | Prospective randomized controlled trial. | 60 Patients | AET = 58.9 ± 0.2 RMT = 60.4 ± 8.9 | Pre and post treatment |
| Caruso, F.R. et al. [11] 2015 | Brazil | Randomized controlled clinical trial | 28 Patients | Training group = 61.3 ± 5.2 Control group = 61 ± 4.4 | Pre and post treatment |
| Scheer, A. et al. [12] 2021 | Australia | Parallel group, randomized controlled trial | 52 Patients | WEX = 66 ± 8 GEX = 67 ± 8 Control = 71 ± 5 | Pre and post treatment |
| Reed, J.L. et al. [13] 2021 | Canada | Randomized Controlled Trial | 135 Patients | MICT = 60 ± 7 NW = 61 ± 8 HIIT = 61 ± 7 | Pre and post treatment |
| Marzolini, S. et al. [15] 2008 | Canada | Randomized controlled trial | 53 Patients | AT = 57.9 ± 2.6 AT/RT1 = 60.9 ± 2.3 AT/RT3 = 62.7 ± 2.7 | Pre and post treatment |
| Santa-Clara, H. et al. [16] 2002 | Portugal | Randomized controlled trial | 40 Patients | Combined training group = 55 ± 10 Aerobic training group = 57 ± 7 Control group = 57 ± 11 | Pre and post treatment |
| Kambic, T. et al. [17] 2021 | Slovenia | Randomized, crossover clinical trial | 43 Patients | 61 ± 10 | Baseline, in between and post treatment |
| Caruso, F.R. et al. [18] 2017 | Brazil | Randomized controlled trial | 20 Patients | 61.1 ± 4.7 | Pre and post treatment |
| Ximenes, N.N. et al. [19] 2015 | Brazil | Randomized controlled trial | 34 Patients | Intervention group = 59.9 ± 7 Control group = 61.8 ± 6.7 | Pre and post treatment |
| Deka, P. et al. [20] 2022 | Spain | Randomized controlled single-blinded trial | 90 Patients | HIIT + R = 69.2 ± 4.18 UC = 69.27 ± 5.68 | Pre and post treatment |
| Arthur, H.M. et al. [21] 2007 | Canada | Prospective two group, randomized controlled trial | 282 Patients | Not specified | Pre, in between and post treatment |
| Schmid, J.P. et al. [22] 2008 | Switzerland | Prospective randomized, controlled study | 38 Patients | ET/RT = 54.7 ± 9.4 ET = 57 ± 9.6 | Baseline, at 3rd month and 12th month |
| Pimenta, N.M. et al. [23] 2013 | Lisbon | Randomized controlled trial | 44 Patients | CET = 57 ± 12 Control group = 58 ± 11 | Pre and post treatment |
| Author/Year | Objective of the Study | Intervention | Outcome Measures | Results | Conclusion |
|---|---|---|---|---|---|
| Hansen, D. et al. [10] 2011 | Evaluate the efficacy of aerobic training in combination of lower limb low intensity resistance training in patients with coronary artery disease. | Aerobic training group = Aerobic training for 3 times in a week for 8 weeks. Combined group = Limbs along with aerobic exercises 3 times a week for 8 weeks. |
| In comparison to AET, RT tends to increase the total body lean tissue mass with a higher magnitude (p = 0.07), and blood high-density lipoprotein cholesterol content with a considerably greater magnitude (p < 0.05). | Low-intensity RT during early aerobic endurance training in individuals with coronary artery disease accounts for a substantial increase in blood high-density lipid cholesterol content, along with tends to alter lean tissue mass. |
| Caruso, F.R. et al. [11] 2015 | The effect of resistance training on improving heart variability in patients with coronary heart disease. | Resistance training group = Session of resistance training along with aerobic training for a total duration of 1 h, 2 times a week for 8 weeks. Usual care group = In this group patients were provided with a session composed of warm-up, aerobic exercises, stretching and cool-down of 1 h, 2 times a week for 8 weeks. |
| Significantly increase in RMSSD and SD1 indices in the resistance training group after 8 weeks of training session. | Significant improvement in heart rate volume, muscle strength and endurance in coronary artery disease patients. |
| Scheer, A. et al. [12] 2021 | Effect of water-based circuit training on body fat, fitness and leg strength in patients with stable coronary artery disease. | Water based exercise group = Circuit of light aerobic and stretching exercises, with an alternative session of aerobic exercises with resistance exercises 60 min, 3 times a week 12 weeks. Gym based exercise group = Aerobic exercises and resistance exercises were given to the patients 60 min, 3 times a week for 12 weeks. Control group = Usual activities of daily living |
| VO2 peak significantly increased in both training groups as compared to controls: WEX by 2.5 mL/kg/min (95 % CI 0.6 to 4.4) and GEX by 2.3 mL/kg/min (95 % CI 0.6 to 4.0). When compared to the control, both WEX and GEX increased hamstring strength: WEX by 6.3 kg (95 % CI 1.2 to 11.3) and GEX by 7.6 kg (95 % CI 2.9 to 12.2). GEX enhanced leg press strength by 15.5 kg (95% CI 5.7 to 25.3) in comparison to control. Latissimus dorsi pulldown strength was only increased with GEX. | WEX was well tolerated. It enhanced body composition, leg strength, and aerobic ability. Data suggest WEX as a useful exercise training substitute for GEX for individuals with coronary heart disease. |
| Reed, J.L. et al. [13] 2021 | Effect of high intensity interval training, walking on cardiovascular system in patients with coronary artery disease. | High intensity interval training = Session of 45 min was given to the patients that consist of warm-up high intensity training and cool-down. Moderate to vigorous intensity continuous training = A session of 60 min was given that consist of 10–15 min of warm-up, 10–15 min aerobic exercises and 15 min cool-down. Nordic walking = Session of 60 min was given to the patients that included 15 min warm-up, 10–15 min walking and 15 min cool-down. |
| There was a higher increase in 6 MWT distance (m) for NW (77.2–60.9) than HIIT (51.4–47.8) and MICT (48.3–47.3), according to a significant time–group interaction (p = 0.042). BDI-II considerably improved (HIIT: 1.4 3.7, NW: 1.6 4.0, MICT: 2.3 6.0 points, main effect of time p < 0.001). Values for the SF-36 and Heart QoL significantly improved (main effects of time: p < 0.05). | All exercise programs (HIIT, NW, and MICT) were well-attended, secure, and helpful for enhancing physical and emotional health in patients with CAD. |
| Marzolini, S. et al. [15] 2008 | Determine the effect of aerobic and resistance training in patients with coronary artery disease. | Aerobic training group = 30 to 60 min of walking and jogging AT/RT1 and AT/RT3 = Within a 24-week period, attended 6 RT exercise training sessions during their regularly scheduled weekly classes, including follow-up sessions at weeks 12, 16, and 22 |
| The average increase in VO2 peak from baseline was 11% for AT (p < 0.05), 14% for AT/RT1, and 18% for AT/RT3, although there was no statistically significant difference between the groups. VAT dramatically increased in the AT/RT3 group (p < 0.05). Only the AT + RT groups showed a decrease in body fat (p < 0.05). In comparison to AT alone, endurance improved greater in the AT + RT groups (p < 0.05). Compliance with the number of sets completed was less in than AT/RT1 is AT/RT3 (p < 0.02). | Despite of 28% reduction in the actual AT training stimulus, combination of RT and AT result in larger improvements in cardiovascular endpoints of exercise performance, skeletal muscle function, and body composition than AT alone. Findings strongly suggest use of multiple-set RT for patients requiring a higher RT stimulus and a combined training intervention in CAD patients. |
| Santa-Clara, H. et al. [16] 2002 | The effect of a combined effect of aerobic and weight training program of 1 year in patients with coronary artery disease. | Aerobic training group = Session of aerobic exercises for 50 min along with warm-up and cool-down phase. Combined exercise group = Aerobic activities along with weight training program. Control group = No intervention |
| One-repetition maximum approach was used for each of the eight weight exercises to measure muscle strength exclusively in the combined exercise group. Strength in the arms and legs rose from pre- to post-tests by 21.9 and 27.8 percent, respectively (p < 0.0001). | VT was raised more by weight training in addition to aerobic exercise than by aerobic exercise alone. When compared to the no-exercise group, aerobic exercise, whether it included weight training or not, significantly increased VO2, peak, functional capacity, and VT. |
| Kambic, T. et al. [17] 2021 | The efficacy of high and low load resistance exercises on hemodynamic in patient with coronary artery disease. | Group 1 = Low load resistance exercises after 48–72 h rest then given high load resistance exercises. Group2 = High load resistance exercises after 48–72 h rest then given low load resistance exercises. |
| During HL-RE or LL-RE, no clinically significant changes in HR, BP, or patient-reported symptoms were noted. When compared to baseline, HR and SBP increased during LL-RE (from 66 to 86 bpm; from 129 to 146 mmHg; time effect: p < 0.001; and HL-RE (from 68 to 86 bpm; from 130 to 146 mmHg; time effect: p < 0.001). The increase in HR was larger after the final set of LL-RE (32 percent vs. 28 percent, p = 0.015) than it was after HL-RE. | Both HL-RE and LL-RE were effective and well-tolerated in patients with CAD. |
| Caruso, F.R. et al. [18] 2017 | Evaluate the after effect of resistance exercises in patients with coronary artery disease on hemodynamic, autonomic, ventilatory, and metabolic alterations. | Aerobic group = Cardiovascular rehabilitation program that consist of aerobic exercises, stretching, treadmill training for 50 min 2 times a week for 8 weeks. Combined group = Cardiovascular rehabilitation program along with resistance training program. Each session was of 40 min 2 times a week for 8 weeks. |
| RT increased maximal and submaximal load tolerance (p < 0.01), reduced hemodynamic response (p < 0.01), and decreased blood lactate levels during the 45° leg press. During exercise on a cycle ergometer and a 45° leg press, during the 8-week RT program increased parasympathetic tone and increased the SDNN index (p < 0.05). | An 8-week program of resistance exercise combined with aerobic exercise may reduce hemodynamic stress and alters metabolic and autonomic responses and reflect significant benefits on heart and autonomic nervous system. |
| Ximenes, N.N. et al. [19] 2015 | Effect of early resistance exercises in patients with coronary artery disease. | Intervention group = Patients were provided with diaphragmatic breathing, resistance exercises and ambulation exercises 30 min twice a day. Control group = Patients were given diaphragmatic breathing exercises for 30 min twice a week. |
| When compared to the control group, resistance exercise had no impact on the pulmonary function of the intervention group. | Early implementation of RT in CAD disease patient’s artery surgery is more beneficial and does not alter pulmonary function. |
| Deka, P. et al. [20] 2022 | The effect of high intensity interval and resistance exercise training in patients with coronary artery disease. | Intervention group = In this group high intensity interval training along with resistance training of 50–60 min, 1 session per week for 8 weeks were given. Usual care group = Conventional medical treatment was given in this group to the patients. |
| In comparison to the usual care group, there was a significant group and time interaction for the participants in the HIIT + R Group for BMI (p < 0.001), body fat percentage (p < 0.001), waist circumference (p = 0.001), physical activity (p < 0.001), functional capacity (p< 0.001), and QoL (p < 0.001). The HIIT + R group experienced a significant decrease in systolic blood pressure (p < 0.001). | To achieve desired health goals, elderly with CAD may benefit from a combined HIIT + R exercise strategy. |
| Arthur, H.M. [21] 2007 | Effect of aerobic and combined aerobic strength training in women after an event of coronary artery by-pass grafting as post-surgery cardiac rehabilitation. | Intervention group = Aerobic exercises and aerobic plus strength training for a period of 6 months, 2 times in a week. Usual care group = Aerobic exercises for a duration of 6 months for 2 times in a week. |
| Both groups demonstrated statistically significant improvements in physical quality of life (p = 0.0002), peak VO2 (19% in aerobic/strength training vs. 22% in aerobic training alone), strength (p = 0.0001), and self-efficacy for stair climbing (p = 0.0024), lifting (p = 0.0001), and walking (p = 0.0012) after 6 months of supervised exercise training. Aerobic/strength training group had a statistically significant change in physical quality of life at the 1-year follow-up (p = 0.05). | Aerobic training alone and both aerobic/strength training are both beneficial in women with coronary artery disease. Combining strength and aerobic exercise maintains physical quality of life. |
| Schmid, J.P. et al. [22] 2007 | The effect of endurance and resistance exercises after myocardial infarction in patients with coronary artery disease. | Combined group = endurance training and resistance training was given to patients for 4 times and 2 times respectively in a week. Endurance training group = In these group 6 sessions per week of endurance training of lower limb and abdominal muscles were given to the patients. |
| Over the course of a year, the end-diastolic volume increased from 206 ± 41 to 210 ± 48 mL (p = 0.379) compared to 183 ± 44 to 186 ± 52 mL (p = 0.586), the Left Ventricular mass increased from 149 ± 28 to 155 ± 31 g (p = 0.408) compared to 144 ± 36 to 149 ± 42 g (p = 0.227), and peak oxygen consumption and muscle strength both increased dramatically in both groups. | For three months, either an ET/RT combination or an ET alone can dramatically raise peak VO2 and muscle strength. |
| Pimenta, N.M. et al. [23] 2013 | Effect of combined exercise training on body fat response in male coronary artery disease patients. | Combined exercise training group = Aerobic training and resistance training on 3 non-consecutive days in a week for 12 months. Control group = Aerobic training was given to the patients. |
| Both groups’ body mass and BMI did not differ between the start of the study and the end of the follow-up, but in the CET group, a significant decrease in all the outcome measures were observed. | Despite no changes in body mass or BMI, CET has positive impact on the body composition in CAD patients. No changes in BF distribution, which indicates that the rate of fat loss was identical across all BF depots that were evaluated. |
| Criteria * | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study Authors/Year | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Score |
| Hansen, D. et al. [10] 2011 | 1 | 1 | 1 | 1 | - | - | - | 1 | - | 1 | 1 | 6/10 |
| Caruso, F.R. et al. [11] 2015 | 1 | 1 | 1 | 1 | - | - | - | 1 | 1 | 1 | 1 | 7/10 |
| Scheer, A. et al. [12] 2021 | 1 | 1 | 1 | 1 | - | - | - | 1 | 1 | 1 | 1 | 8/10 |
| Reed, J.L. et al. [13] 2021 | 1 | 1 | 1 | 1 | - | - | - | 1 | 1 | 1 | 1 | 8/10 |
| Marzolini, S. et al. [15] 2008 | 1 | 1 | - | 1 | - | - | - | 1 | - | 1 | 1 | 5/10 |
| Santa-Clara H. et al. [16] 2002 | 1 | - | - | 1 | - | - | - | 1 | - | 1 | 1 | 5/10 |
| Kambic, T. et al. [17] 2021 | 1 | 1 | 1 | 1 | - | - | - | 1 | - | 1 | 1 | 7/10 |
| Caruso, F.R. et al. [18] 2017 | 1 | 1 | 1 | 1 | - | - | - | 1 | - | 1 | 1 | 7/10 |
| Vysoký, R. et al. [24] 2015 | 1 | 1 | 1 | 1 | - | 1 | - | 1 | - | 1 | 1 | 7/10 |
| Ximenes, N.N. et al. [19] 2015 | 1 | 1 | - | 1 | - | - | - | 1 | - | 1 | 1 | 6/10 |
| Deka, P. et al. [20] 2021 | 1 | 1 | 1 | 1 | - | - | 1 | 1 | - | 1 | 1 | 8/10 |
| Arthur, H.M. et al. [21] 2007 | 1 | 1 | 1 | 1 | - | 1 | - | 1 | 1 | 1 | 1 | 9/10 |
| Schmid, J.P. et al. [22] 2008 | 1 | 1 | - | 1 | - | - | - | 1 | - | 1 | 1 | 6/10 |
| Pimenta, N.M. et al. [23] 2013 | 1 | 1 | - | 1 | - | - | - | 1 | - | 1 | 1 | 6/10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sharma, A.; Sharma, N.; Vats, S.; Jain, M.; Chahal, A.; Kashoo, F.Z.; Hakamy, A.; Alajam, R.A.; Alshehri, M.M.; Bharath Kumar, M.; et al. Effect of Resistance Training on Body Composition, Hemodynamic Parameters and Exercise Tolerance among Patients with Coronary Artery Disease: A Systematic Review. Healthcare 2023, 11, 131. https://doi.org/10.3390/healthcare11010131
Sharma A, Sharma N, Vats S, Jain M, Chahal A, Kashoo FZ, Hakamy A, Alajam RA, Alshehri MM, Bharath Kumar M, et al. Effect of Resistance Training on Body Composition, Hemodynamic Parameters and Exercise Tolerance among Patients with Coronary Artery Disease: A Systematic Review. Healthcare. 2023; 11(1):131. https://doi.org/10.3390/healthcare11010131
Chicago/Turabian StyleSharma, Abhishek, Nidhi Sharma, Sakshi Vats, Mansi Jain, Aksh Chahal, Faizan Z. Kashoo, Ali Hakamy, Ramzi Abdu Alajam, Mohammed M. Alshehri, Mallela Bharath Kumar, and et al. 2023. "Effect of Resistance Training on Body Composition, Hemodynamic Parameters and Exercise Tolerance among Patients with Coronary Artery Disease: A Systematic Review" Healthcare 11, no. 1: 131. https://doi.org/10.3390/healthcare11010131
APA StyleSharma, A., Sharma, N., Vats, S., Jain, M., Chahal, A., Kashoo, F. Z., Hakamy, A., Alajam, R. A., Alshehri, M. M., Bharath Kumar, M., Sanjeevi, R. R., Alwadaani, F., & Shaphe, M. A. (2023). Effect of Resistance Training on Body Composition, Hemodynamic Parameters and Exercise Tolerance among Patients with Coronary Artery Disease: A Systematic Review. Healthcare, 11(1), 131. https://doi.org/10.3390/healthcare11010131