
A Structural Equation Modeling Analysis to Explore Diabetes Self-Care Factors in a Rural Sample


Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample and Setting
2.2. Measures
2.2.1. Diabetes Self-Care Activities
2.2.2. Diabetes Fatalism
2.2.3. Perceived Diabetes Self-Management
2.2.4. Social Support
2.2.5. Diabetes Knowledge
2.3. Intervention
2.4. Data Analysis
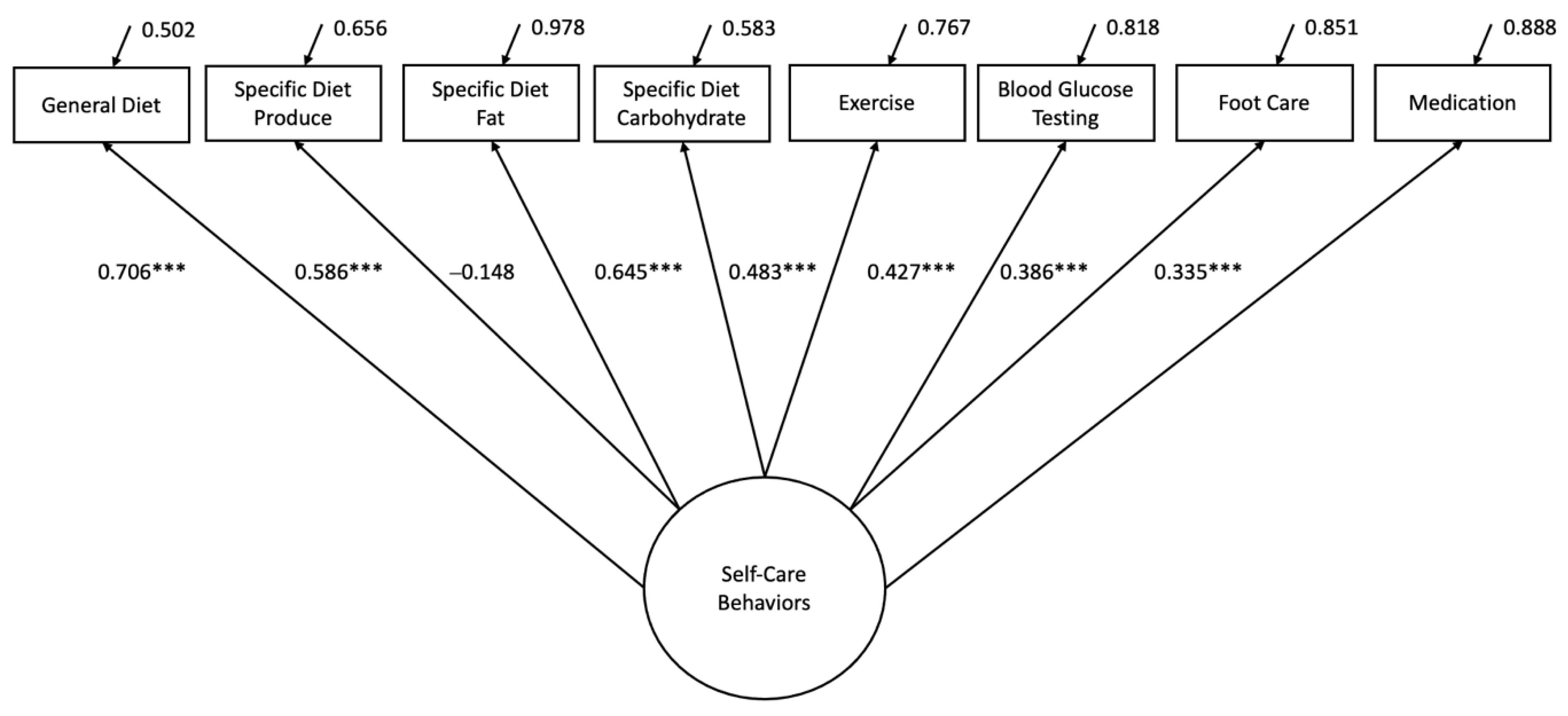
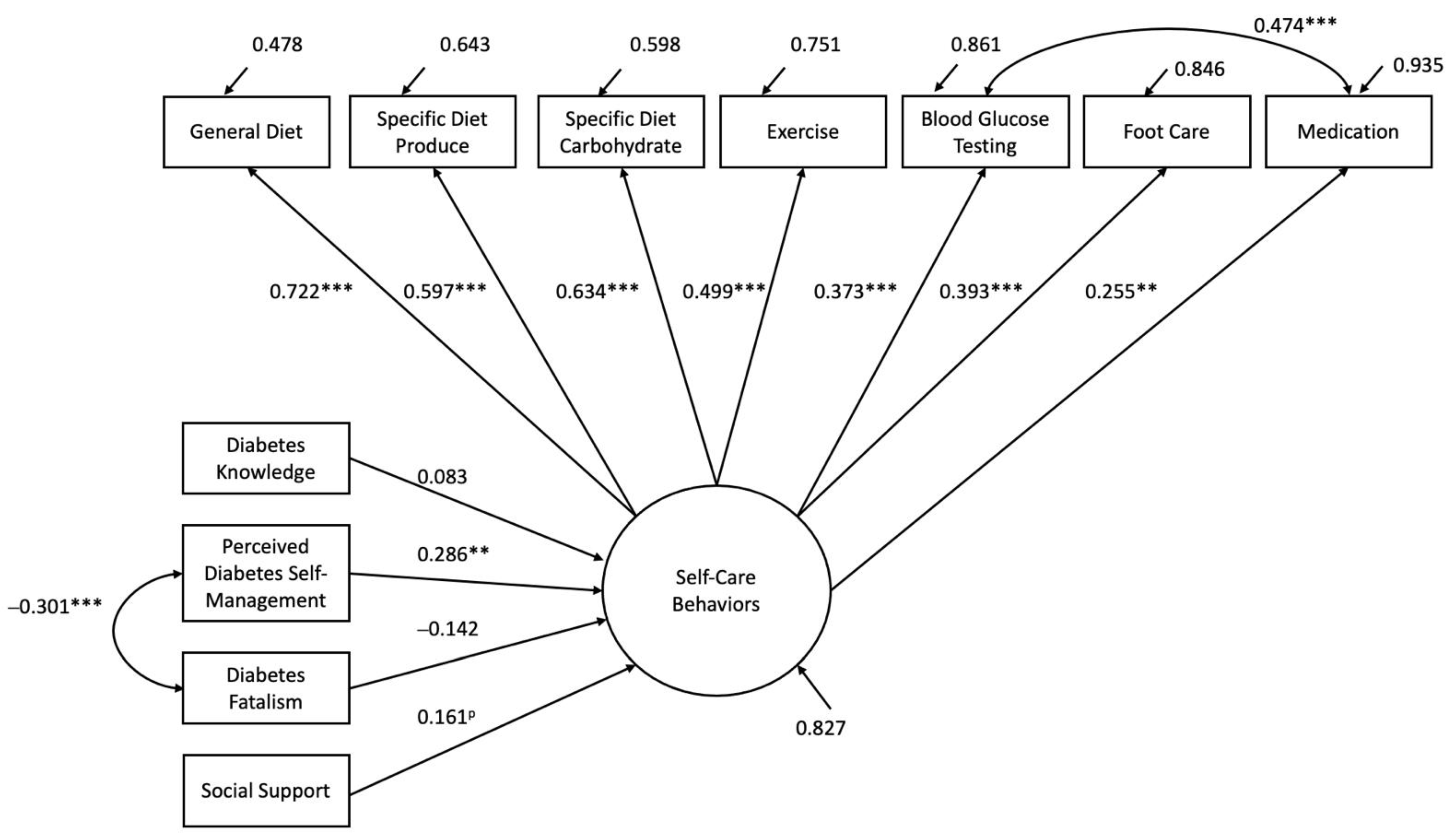
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Boersma, P.; Black, L.I.; Ward, B.W. Prevalence of Multiple Chronic Conditions Among US Adults, 2018. Prev. Chronic. Dis. 2020, 17, 200130. [Google Scholar] [CrossRef] [PubMed]
- CDC. National Center for Chronic Disease Prevention and Health Promotion. 2021. Available online: https://www.cdc.gov/chronicdisease/index.htm (accessed on 4 May 2022).
- Leon, B.M.; Maddox, T.M. Diabetes and cardiovascular disease. Epidemiology, biological mechanisms, treatment recommendations and future research. World J. Diabetes 2015, 6, 1246–1258. [Google Scholar] [CrossRef] [PubMed]
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Alonso, A.; Beaton, A.Z.; Bittencourt, M.S.; Boehme, A.K.; Buxton, A.E.; Carson, A.P.; Commodore-Mensah, Y.; et al. Heart disease and stroke statistics-2022 update: A report from the American Heart Association. Circulation 2022, 145, e153–e639. [Google Scholar] [CrossRef]
- Carnethon, M.R.; Pu, J.; Howard, G.; Albert, M.A.; Anderson, C.A.; Bertoni, A.G.; Mujahid, M.S.; Palaniappan, L.; Taylor, H.A., Jr.; Willis, M.; et al. Cardiovascular Health in African Americans: A Scientific Statement from the American Heart Association. Circulation 2017, 136, e393–e423. [Google Scholar] [CrossRef] [PubMed]
- Havranek, E.P.; Mujahid, M.S.; Barr, D.A.; Blair, I.V.; Cohen, M.S.; Cruz-Flores, S.; Davey-Smith, G.; Dennison-Himmelfarb, C.R.; Lauer, M.S.; Lockwood, D.W.; et al. Social determinants of risk and outcomes for cardiovascular disease A scientific statement From the American Heart Association. Circulation 2015, 132, 873–898. [Google Scholar] [CrossRef]
- Howard, G.; Kleindorfer, D.O.; Cushman, M.; Long, D.L.; Jasne, A.; Judd, S.E.; Higginbotham, J.C.; Howard, V.J. Contributors to the excess stroke mortality in rural areas in the United States. Stroke 2017, 48, 1773–1778. [Google Scholar] [CrossRef]
- Kulshreshtha, A.; Goyal, A.; Dabhadkar, K.; Veledar, E.; Vaccarino, V. Urban-rural differences in coronary heart disease mortality in the United States: 1999–2009. Public Health Rep. 2014, 129, 19–29. [Google Scholar] [CrossRef]
- Limdi, N.A.; Howard, V.J.; Higginbotham, J.; Parton, J.; Safford, M.M.; Howard, G. US mortality: Influence of race, geography and cardiovascular risk among participants in the population-based REGARDS cohort. J. Racial Ethn. Health Disparities 2016, 3, 599. [Google Scholar] [CrossRef] [PubMed]
- Meit, M.; Knudson, A.; Gilbert, T.; Yu, A.T.; Tanenbaum, E.; Ormson, E.; Popat, S. Rural Health Reform Policy Research Center: The 2014 Update of the Rural-Urban Chartbook. 2014. Available online: https://ruralhealth.und.edu/projects/health-reform-policy-research-center/pdf/2014-rural-urban-chartbook-update.pdf (accessed on 6 May 2022).
- Singh, G.K.; Daus, G.P.; Allender, M.; Ramey, C.T.; Martin, E.K.; Perry, C.; Reyes, A.A.D.L.; Vedamuthu, I.P. Social determinants of health in the United States: Addressing major health inequality trends for the nation, 1935–2016. Int. J. MCH AIDS 2017, 6, 139–164. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.K.; Siahpush, M. Widening rural-urban disparities in all-cause mortality and mortality from major causes of death in the USA, 1969–2009. J. Urban Health 2014, 91, 272–292. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, T.; Liu, J.; Probst, J.C.; Merchant, A.; Jones, S.; Martin, A.B. Obesity and obesity-related behaviors among rural and urban adults in the USA. Rural. Remote Health 2015, 15, 3267. [Google Scholar] [CrossRef] [PubMed]
- Coughlin, S.S.; Clary, C.; Johnson, J.A.; Berman, A.; Heboyan, V.; Benevides, T.; Moore, J.; George, V. Continuing Challenges in Rural Health in the United States. J. Environ. Health Sci. 2019, 5, 90–92. [Google Scholar]
- Garcia, M.C.; Faul, M.; Massetti, G.; Thomas, C.C.; Hong, Y.; Bauer, U.E.; Iademarco, M.F. Reducing Potentially Excess Deaths from the Five Leading Causes of Death in the Rural United States. MMWR Surveill. Summ. 2017, 66, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Garcia, M.C.; Faul, M.; Dowling, N.F.; Thomas, C.C.; Iademarco, M.F. Bridging the Gap in Potentially Excess Deaths Between Rural and Urban Counties in the United States. Public Health Rep. 2020, 135, 177–180. [Google Scholar] [CrossRef] [PubMed]
- Moy, E.; Garcia, M.C.; Bastian, B.; Rossen, L.M.; Ingram, D.D.; Faul, M.; Massetti, G.M.; Thomas, C.C.; Hong, Y.; Yoon, P.W.; et al. Leading Causes of Death in Nonmetropolitan and Metropolitan Areas—United States, 1999–2014. MMWR Surveill. Summ. 2017, 66, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Matthews, K.A.; Croft, J.B.; Liu, Y.; Lu, H.; Kanny, D.; Wheaton, A.G.; Cunningham, T.J.; Khan, L.K.; Caraballo, R.S.; Holt, J.B.; et al. Health-Related Behaviors by Urban-Rural County Classification—United States, 2013. MMWR Surveill. Summ. 2017, 66, 1–8. [Google Scholar] [CrossRef]
- Logan, H.; Guo, Y.; Dodd, V.J.; Muller, K.; Riley, J. The burden of chronic diseases in a rural North Florida sample. BMC Public Health 2013, 13, 906. [Google Scholar] [CrossRef]
- Swanoski, M.T.; Lutfiyya, M.N.; Amaro, M.L.; Akers, M.F.; Huot, K.L. Knowledge of heart attack and stroke symptomology: A cross-sectional comparison of rural and non-rural US adults. BMC Public Health 2012, 12, 283. [Google Scholar] [CrossRef]
- Chatterjee, R.; Maruthur, N.M.; Edelman, D. Novel risk factors for type 2 diabetes in African Americans. Curr. Diab. Rep. 2015, 15, 103. [Google Scholar] [CrossRef]
- Cummings, D.M.; Lutes, L.D.; Littlewood, K.; Solar, C.; Hambidge, B.; Gatlin, P. Impact on distress reduction on behavioral correlates and A1C in African American women with uncontrolled type 2 diabetes: Results from EMPOWER. Ethn. Dis. 2017, 27, 155–160. [Google Scholar] [CrossRef]
- Richards Adams, I.K.; Figueroa, W.; Hatsu, I.; Odei, J.B.; Sotos-Prieto, M.; Leson, S.; Huling, J.; Joseph, J.J. An examination of demographic and psychosocial factors, barriers to health eating, and diet quality among African American adults. Nutrients 2019, 11, 519. [Google Scholar] [CrossRef] [PubMed]
- Hill-Briggs, F.; Adler, N.E.; Berkowitz, S.A.; Chin, M.H.; Gary-Webb, T.L.; Navas-Acien, A.; Thornton, P.L.; Haire-Joshu, D. Social Determinants of Health and Diabetes: A Scientific Review. Diabetes Care 2020, 44, 258–279. [Google Scholar] [CrossRef] [PubMed]
- Davis, A.M.; Vinci, L.M.; Okwuosa, T.M.; Chase, A.R.; Huang, E.S. Cardiovascular health disparities: A systematic review of health care interventions. Med. Care Res. Rev. 2007, 64, 29S–100S. [Google Scholar] [CrossRef]
- Berardi, V.; Bellettiere, J.; Nativ, O.; Ladislav, S.; Hovell, M.F.; Baron-Epel, O. Fatalism, diabetes management, and the role of religiosity. J. Relig. Health 2016, 55, 602–617. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, R.; Ruggiero, L.; Riley, B.B.; Wang, Y.; Chavez, N.; Quinn, L.T.; Gerber, B.S.; Choi, Y.K. Correlates of self-care in low-income African American and Latino patients with diabetes. Health Psychol. 2014, 33, 597–607. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.A.; Ansa, B. A systematic review of lifestyle interventions for chronic diseases in rural communities. J. Ga. Public Health Assoc. 2016, 5, 304–313. [Google Scholar] [CrossRef]
- Osborne, C.Y.; Egede, L.E. Validation of an Information-Motivation-Behavioral skills model of diabetes self-care (IMB-DSC). Patient Educ. Couns. 2010, 79, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Egede, L.E.; Ellis, C. Development and psychometric properties of the 12-item diabetes fatalism scale. J. Gen. Intern. Med. 2010, 25, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Al-Dwaikat, T.N.; Chlebowy, D.O.; Hall, L.A.; Crawford, T.N.; Yankeelov, P.A. Self-management as a mediator of the relationship between social support dimensions and health outcomes of African American adults with type 2 diabetes. West J. Nurs. Res. 2020, 42, 485–494. [Google Scholar] [CrossRef]
- Fitzpatrick, S.L.; Hill-Briggs, F. Strategies for sustained weight management: Perspectives from African American patients with type 2 diabetes. Diabetes Educ. 2017, 43, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, J.M.; Mitchell, J. Can social integration and social support help to explain racial disparities in health care utilization among men with diabetes? Int. J. Men’s Health 2017, 16, 66–83. [Google Scholar]
- Rutledge, P.M.; Montgomery, A.J.; Lott, S.M.; McGee, Z.M.; Burns, D.M. The relationship between family support, self-care, and health in selected African American females with type 2 diabetes. J. Natl. Black Nurses Assoc. 2019, 30, 1–9. [Google Scholar]
- Abbott, L.S.; Slate, E.H.; Graven, L.J. Cardiovascular disease risk among rural residents living with diabetes and prediabetes: A cluster randomized trial. Public Health Nurs. 2020, 37, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Donner, A.; Klar, N. Pitfalls and controversies in cluster randomization trials. Am. J. Public Health 2004, 94, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Murray, D.M.; Blitstein, J.L. Methods to reduce the impact of intraclass correlation in group-randomized trials. Eval. Rev. 2003, 27, 79–103. [Google Scholar] [CrossRef] [PubMed]
- Dsn, P.S.F.; Pribulick, M.; Williams, I.C.; James, G.D.; Rovynak, V.; Seibold-Simpson, S.M. Promoting heart health in rural women. J. Rural Health 2013, 29, 248–257. [Google Scholar]
- Toobert, D.J.; Hampson, S.E.; Glasgow, R.E. The summary of diabetes self-care activities measure. Diabetes Care 2000, 23, 943–950. [Google Scholar] [CrossRef] [PubMed]
- Wallston, K.A.; Rothman, R.L.; Cherrington, A. Psychometric properties of the perceived diabetes self-Management scale (PDSMS). J. Behav. Med. 2007, 30, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Sherbourne, C.D.; Stewart, A.L. The MOS social support survey. Soc. Sci. Med. 1991, 32, 705–714. [Google Scholar] [CrossRef]
- Fitzgerald, J.T.; Funnell, M.M.; Anderson, R.M.; Nwankwo, R.; Stansfield, R.B.; Piatt, G.A. Validation of the revised brief Diabetes Knowledge Test (DKT2). Diabetes Educ. 2016, 42, 178–187. [Google Scholar] [CrossRef] [PubMed]
- Muthén, L.K.; Muthén, B.O. (1998–2011). Mplus User’s Guide, 6th ed.; Muthén & Muthén: Los Angeles, CA, USA, 1998. [Google Scholar]
- Browne, M.W.; Cudeck, R.I. Alternative ways of assessing model fit. In Testing Structural Equation Models; Bollen, K., Long, K., Eds.; Sage: Newbury Park, CA, USA, 1993; pp. 136–162. [Google Scholar]
- Steiger, J.H. Structural model evaluation and modification: An interval estimation approach. Multivar. Behav. Res. 1990, 25, 173–180. [Google Scholar] [CrossRef] [PubMed]
- MacCallum, R.C.; Browne, M.W.; Sugawara, H.M. Power analysis and determination of sample size for covariance structure modeling. Psychol. Methods 1996, 1, 130–149. [Google Scholar] [CrossRef]
- Abbott, L.; Slate, E.; Graven, L.; Lemacks, J.; Grant, J. Fatalism, social support and self-management perceptions among rural African Americans living with diabetes and pre-diabetes. Nurs. Rep. 2021, 11, 242–252. [Google Scholar] [CrossRef]
- Gao, J.; Wang, J.; Zhu, Y.; Yu, J. Validation of an information-motivation-behavioral skills model of self-care among Chinese adults with type 2 diabetes. BMC Public Health 2013, 13, 100. [Google Scholar] [CrossRef]
- Alshutwi, S.; Miligi, E.; Alhumidan, L.; Almutairi, A.F. The influence of the disclosure of diabetes on the cognitive, physical ability and diabetes self-management in diabetic employed adults in Saudi Arabia. Nurs. Open 2022, 9, 978–985. [Google Scholar] [CrossRef] [PubMed]
- Sayin Kasar, K.; Duru Asiret, G.; Kutmec Yilmaz, C.; Canlar, Ş. The effect of model-based telephone counseling on HbA1c and self-management for individuals with type 2 diabetes: A randomized controlled trial. Prim. Care Diabetes 2022, 16, 41–48. [Google Scholar] [CrossRef]
- Dogru, A.; Ovayolu, N.; Ovayolu, O. The effect of motivational interview persons with diabetes on self-management and metabolic variables. J. Pak. Med. Assoc. 2019, 69, 294–300. [Google Scholar]
- Pai, L.W.; Chiu, S.C.; Liu, H.L.; Chen, L.L.; Peng, T. Effects of a health education technology program on long-term glycemic control and self-management ability of adults with type 2 diabetes: A randomized controlled trial. Diabetes Res. Clin. Pract. 2021, 175, 108785. [Google Scholar] [CrossRef]
- Asuzu, C.C.; Walker, R.J.; Williams, J.S.; Egede, L.E. Pathways for the relationship between diabetes distress, depression, fatalism and glycemic control in adults with type 2 diabetes. J. Diabetes Complicat. 2017, 31, 169–174. [Google Scholar] [CrossRef]
- Sukkarieh-Haraty, O.; Egede, L.E.; Abi Kharma, J.; Bassil, M. Diabetes fatalism and its emotional distress subscale are independent predictors of glycemic control among Lebanese patients with type 2 diabetes. Ethn. Health 2019, 24, 767–778. [Google Scholar] [CrossRef] [PubMed]
- Walker, R.J.; Smalls, B.L.; Hernandez-Tejada, M.A.; Campbell, J.A.; Davis, K.S.; Egede, L.E. Effect of diabetes fatalism on medication adherence and self-care behaviors in adults with diabetes. Gen. Hosp. Psychiatry 2012, 34, 598–603. [Google Scholar] [CrossRef]
- Awad, N.; Saade, R.; Bassil, M.; Sukkarieh-Haraty, O.; Egede, L.E. Relationship between social determinants of health and clinical outcomes in adults with type 2 diabetes in Lebanon. J. Natl. Med. Assoc. 2022, 114, 392–405. [Google Scholar] [CrossRef] [PubMed]
- Sukkarieh-Haraty, O.; Egede, L.E.; Abi Kharma, J.; Bassil, M. Predictors of Diabetes Fatalism Among Arabs: A Cross-Sectional Study of Lebanese Adults with Type 2 Diabetes. J. Relig. Health 2018, 57, 858–868. [Google Scholar] [CrossRef]
- Power, T.; Kelly, R.; Usher, K.; East, L.; Travaglia, J.; Robertson, H.; Wong, A.; Jackson, D.; Balintongog, A. Living with diabetes and disadvantage: A qualitative, geographical case study. J. Clin. Nurs. 2020, 29, 2710–2722. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Schoufour, J.; Wang, D.D.; Dhana, K.; Pan, A.; Liu, X.; Song, M.; Liu, G.; Shin, H.J.; Sun, Q.; et al. Healthy lifestyle and life expectancy free of cancer, cardiovascular disease, and type 2 diabetes: Prospective cohort study. BMJ 2020, 368, l6669. [Google Scholar] [CrossRef]
- Yang, R.; Xu, H.; Pedersen, N.L.; Li, X.; Yu, J.; Bao, C.; Qi, X.; Xu, W. A healthy lifestyle mitigates the risk of heart disease related to type 2 diabetes: A prospective nested case-control study in a nationwide Swedish twin cohort. Diabetologia 2021, 64, 530–539. [Google Scholar] [CrossRef] [PubMed]
- Zhu, M.; Wang, T.; Huang, Y.; Zhao, X.; Ding, Y.; Zhu, M.; Ji, M.; Wang, C.; Dai, J.; Yin, R.; et al. Genetic Risk for Overall Cancer and the Benefit of Adherence to a Healthy Lifestyle. Cancer Res. 2021, 81, 4618–4627. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Diabetes Knowledge | Perceived Diabetes Self-Management | Diabetes Fatalism | Social Support | |
|---|---|---|---|---|
| Diabetes Knowledge | 1 | −0.098 | −0.066 | 0.155 |
| Perceived Diabetes Self-Management | 1 | −0.301 *** | 0.101 | |
| Diabetes Fatalism | 1 | −0.074 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abbott, L.; Graven, L.; Schluck, G.; Lemacks, J. A Structural Equation Modeling Analysis to Explore Diabetes Self-Care Factors in a Rural Sample. Healthcare 2022, 10, 1536. https://doi.org/10.3390/healthcare10081536
Abbott L, Graven L, Schluck G, Lemacks J. A Structural Equation Modeling Analysis to Explore Diabetes Self-Care Factors in a Rural Sample. Healthcare. 2022; 10(8):1536. https://doi.org/10.3390/healthcare10081536
Chicago/Turabian StyleAbbott, Laurie, Lucinda Graven, Glenna Schluck, and Jennifer Lemacks. 2022. "A Structural Equation Modeling Analysis to Explore Diabetes Self-Care Factors in a Rural Sample" Healthcare 10, no. 8: 1536. https://doi.org/10.3390/healthcare10081536
APA StyleAbbott, L., Graven, L., Schluck, G., & Lemacks, J. (2022). A Structural Equation Modeling Analysis to Explore Diabetes Self-Care Factors in a Rural Sample. Healthcare, 10(8), 1536. https://doi.org/10.3390/healthcare10081536