
Single-Center-Single-Blinded Clinical Trial to Evaluate the Efficacy of a Nutraceutical Containing Boswellia Serrata, Bromelain, Zinc, Magnesium, Honey, Tyndallized Lactobacillus Acidophilus and Casei to Fight Upper Respiratory Tract Infection and Otitis Media

 , ,
, , 

Abstract
1. Introduction
2. Materials and Methods
2.1. General Info and Randomization
2.2. Inclusion and Exclusion Criteria
2.3. Clinical Evaluation (Table 1)
2.4. Auditory Tests (Table 1)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1 | Microscopic evaluation and photo-recording of tympanic membrane (TM), using the following score:
|
| 2 | Rhynopharingeal fibroendoscopy (using the Cassano’s score to assess the adenoid tissue’s state) |
| 3 | Audiological assessment (tympanometry, pure tone audiometry,) |
| 4 | Powell’ health questionnaire (translated into Italian, to evaluate the general condition of the patients, at three follow-ups; T0, T1, and T2) |
2.5. Statistical Analysis
3. Results
3.1. Health Questionnaire
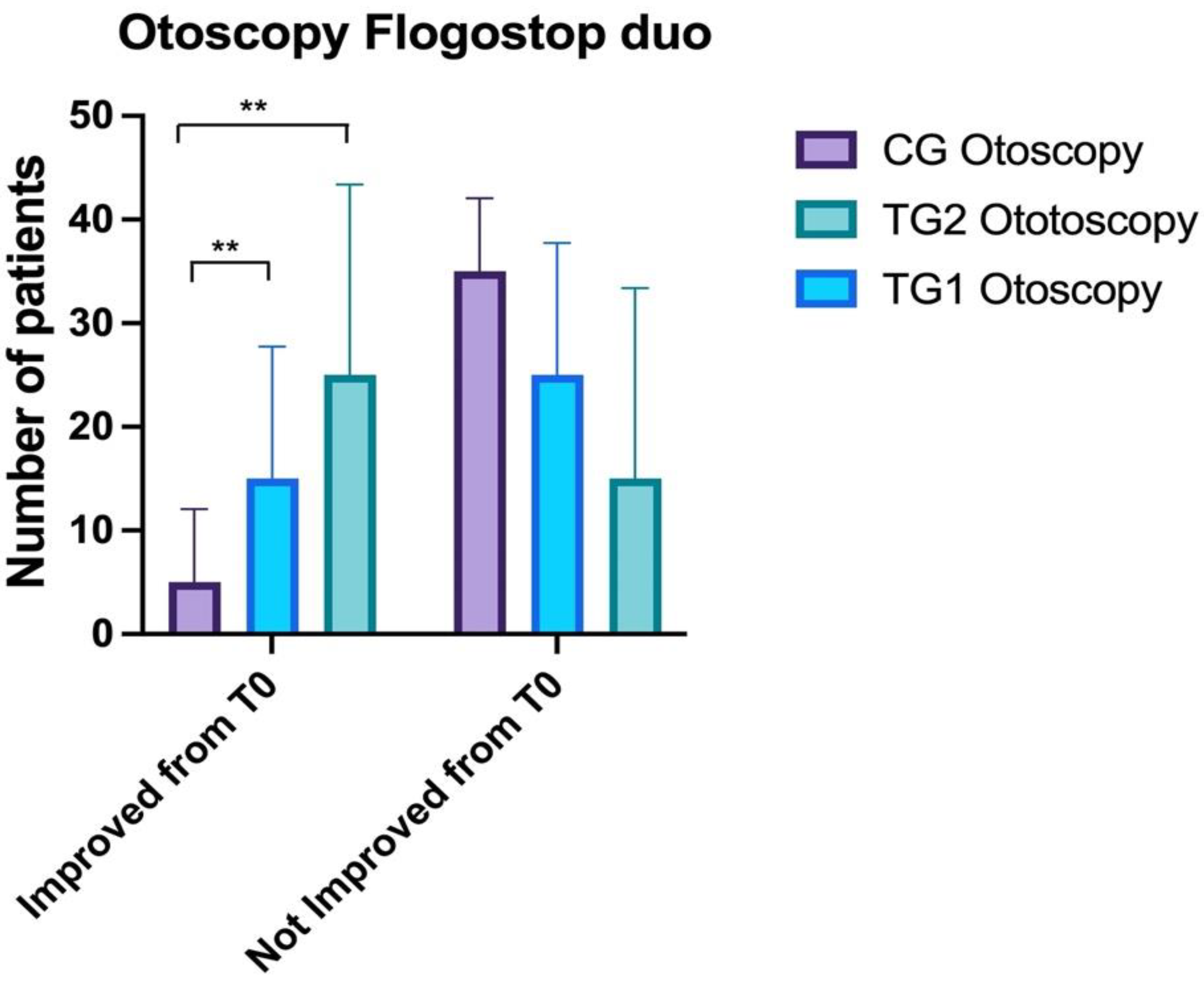
3.2. Otoscopy
3.3. Impedance
3.4. Fibroendoscopy
3.5. Audiometry
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Meherali, S.; Campbell, A.; Hartling, L.; Scott, S. Understanding Parents’ Experiences and Information Needs on Pediatric Acute Otitis Media: A Qualitative Study. J. Patient Exp. 2018, 6, 53–61. [Google Scholar] [CrossRef] [PubMed]
- De Luca, P.; Cassandro, C.; Cavaliere, M.; Gioacchini, F.M.; Albera, A.; Ralli, M.; De Vincentiis, M.; Cassandro, E.; Scarpa, A. Pediatric adenoidectomy: Where we are? A comparative review between cold curettage and emerging techniques. Otorhinolaryngology 2021, 71, 273–277. [Google Scholar] [CrossRef]
- Cavaliere, M.; De Luca, P.; De Bonis, E.; Maurizi, R.; Cassandro, C.; Ralli, M.; Cassandro, E.; Scarpa, A. Partial Intracapsular Tonsillectomy in the Treatment of Pediatric Obstructive Sleep Apnea/Hypopnea Syndrome: A prospective study with 5-years follow-up. Eur. Arch. Otorhinolaryngol. 2021, 279, 3089–3093. [Google Scholar] [CrossRef] [PubMed]
- Nelson, S.P.; Chen, E.H.; Syniar, G.M.; Christoffel, K.K. Prevalence of symptoms of gastroesophageal reflux during infancy: A pediatric practice based survey from the pediatric practice research group. Arch. Pediatr. Adolesc. 1997, 151, 569–572. [Google Scholar] [CrossRef] [PubMed]
- Chonmaitree, T.; Revai, K.; Grady, J.J.; Clos, A.; Patel, J.A.; Nair, S.; Fan, J.; Henrickson, K.J. Viral upper respiratory tract infection and otitis media complication in young children. Clin. Infect. Dis. 2008, 46, 815–823. [Google Scholar] [CrossRef] [PubMed]
- Della Volpe, A.; Ricci, G.; Ralli, M.; Gambacorta, V.; De Lucia, A.; Minni, A.; Pirozzi, C.; Paccone, M.; Pastore, V.; Di Stadio, A. The effects of oral supplements with Sambucus nigra, Zinc, Tyndallized Lactobacillus acidophilus (HA122), Arabinogalactans, vitamin D, vitamin E and vitamin C in otitis media with effusion in children: A randomized controlled trial. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 6360–6370. [Google Scholar] [CrossRef] [PubMed]
- Marchisio, P.G.; Consonni, D.; Baggi, E.; Zampiero, A.; Bianchini, S.; Terranova, L.; Tirelli, S.; Esposito, S.; Principi, N. Vitamin D supplementation reduces the risk of acute otitis media in otitis-prone children. Pediatr. Infect. Dis. J. 2013, 32, 1055–1060. [Google Scholar] [CrossRef] [PubMed]
- Cassano, M.; De Corso, E.; Fiore, V.; Giancaspro, R.; Moffa, A.; Casale, M.; Trecca, E.M.C.; Mele, D.A.; Cassano, P.; Gelardi, M. Update of endoscopic classification system of adenoid hypertrophy based on clinical experience on 7621 children. Acta Otorhinolaryngol. Ital. 2022, 42, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Powell, C.V.; McNamara, P.; Solis, A.; Shaw, N.J. A parent completed questionnaire to describe the patterns of wheezing and other respiratory symptoms in infants and preschool children. Arch. Dis. Child. 2002, 87, 376–379. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Di Stadio, A.; Della Volpe, A.; Korsch, F.M.; De Lucia, A.; Ralli, M.; Martines, F.; Ricci, G. Difensil Immuno Reduces Recurrence and Severity of Tonsillitis in Children: A Randomized Controlled Trial. Nutrients 2020, 12, 1637. [Google Scholar] [CrossRef] [PubMed]
- Cárdenas, N.; Martín, V.; Arroyo, R.; López, M.; Carrera, M.; Badiola, C.; Jiménez, E.; Rodríguez, J.M. Prevention of Recurrent Acute Otitis Media in Children through the Use of Lactobacillus salivarius PS7, a Target-Specific Probiotic Strain. Nutrients 2019, 11, 376. [Google Scholar] [CrossRef] [PubMed]
- Cohen, R.; Martin, E.; de La Rocque, F.; Thollot, F.; Pecquet, S.; Werner, A.; Boucherat, M.; Varon, E.; Bingen, E.; Levy, C. Probiotics and prebiotics in preventing episodes of acute otitis media in high-risk children: A randomized, double-blind, placebo-controlled study. Pediatr. Infect. Dis. J. 2013, 32, 810–814. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, M.Z. Boswellia serrata, a potential antiinflammatory agent: An overview. Indian J. Pharm. Sci. 2011, 73, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Yu, G.; Xiang, W.; Zhang, T.; Zeng, L.; Yang, K.; Li, J. Effectiveness of Boswellia and Boswellia extract for osteoarthritis patients: A systematic review and meta-analysis. MC Complement. Med. Ther. 2020, 20, 225. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Tawab, M.; Werz, O.; Schubert-Zsilavecz, M. Boswellia serrata: An overall assessment of in vitro, preclinical, pharmacokinetic and clinical data. Clin. Pharmacokinet. 2011, 50, 349–369. [Google Scholar] [CrossRef] [PubMed]
- Hikisz, P.; Bernasinska-Slomczewska, J. Beneficial Properties of Bromelain. Nutrients 2021, 13, 4313. [Google Scholar] [CrossRef] [PubMed]
- Jarosz, M.; Olbert, M.; Wyszogrodzka, G.; Mlyniec, K.; Librowski, T. Antioxidant and anti-inflammatory effects of zinc. Zinc-dependent NF-κB signaling. Inflammopharmacology 2017, 25, 11–24. [Google Scholar] [CrossRef] [PubMed]
- Mittal, M.; Siddiqui, M.R.; Tran, K.; Reddy, S.P.; Malik, A.B. Reactive oxygen species in inflammation and tissue injury. Antioxid. Redox Signal. 2014, 20, 1126–1167. [Google Scholar] [CrossRef] [PubMed]
- Mehranfard, N.; Yazdi, A.; Sardooi, A.R.; Shakerin, Z.; Ghasemi, M. Honey protects against chronic unpredictable mild stress induced-intestinal barrier disintegration and hepatic inflammation. Mol. Biol. Rep. 2020, 47, 8475–8484. [Google Scholar] [CrossRef] [PubMed]





| Number | Gender | Age (Months) | Health Questionnaire T0 * | Comorbidities | |
|---|---|---|---|---|---|
| Control Group | 40 | 22 male, 18 female | 52.1 ± 15.3 | 14 | none |
| Treatment Group 1 | 40 | 22 female, 18 male | 47.2 ± 15.7 | 15.25 | none |
| Treatment Group 2 | 40 | 26 female, 14 male | 51.1 ± 17.5 | 16.3 | none |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Della Volpe, A.; De Luca, P.; De Lucia, A.; Martines, F.; Piroli, P.; D’Ascanio, L.; Camaioni, A.; La Mantia, I.; Di Stadio, A. Single-Center-Single-Blinded Clinical Trial to Evaluate the Efficacy of a Nutraceutical Containing Boswellia Serrata, Bromelain, Zinc, Magnesium, Honey, Tyndallized Lactobacillus Acidophilus and Casei to Fight Upper Respiratory Tract Infection and Otitis Media. Healthcare 2022, 10, 1526. https://doi.org/10.3390/healthcare10081526
Della Volpe A, De Luca P, De Lucia A, Martines F, Piroli P, D’Ascanio L, Camaioni A, La Mantia I, Di Stadio A. Single-Center-Single-Blinded Clinical Trial to Evaluate the Efficacy of a Nutraceutical Containing Boswellia Serrata, Bromelain, Zinc, Magnesium, Honey, Tyndallized Lactobacillus Acidophilus and Casei to Fight Upper Respiratory Tract Infection and Otitis Media. Healthcare. 2022; 10(8):1526. https://doi.org/10.3390/healthcare10081526
Chicago/Turabian StyleDella Volpe, Antonio, Pietro De Luca, Antonietta De Lucia, Francesco Martines, Piera Piroli, Luca D’Ascanio, Angelo Camaioni, Ignazio La Mantia, and Arianna Di Stadio. 2022. "Single-Center-Single-Blinded Clinical Trial to Evaluate the Efficacy of a Nutraceutical Containing Boswellia Serrata, Bromelain, Zinc, Magnesium, Honey, Tyndallized Lactobacillus Acidophilus and Casei to Fight Upper Respiratory Tract Infection and Otitis Media" Healthcare 10, no. 8: 1526. https://doi.org/10.3390/healthcare10081526
APA StyleDella Volpe, A., De Luca, P., De Lucia, A., Martines, F., Piroli, P., D’Ascanio, L., Camaioni, A., La Mantia, I., & Di Stadio, A. (2022). Single-Center-Single-Blinded Clinical Trial to Evaluate the Efficacy of a Nutraceutical Containing Boswellia Serrata, Bromelain, Zinc, Magnesium, Honey, Tyndallized Lactobacillus Acidophilus and Casei to Fight Upper Respiratory Tract Infection and Otitis Media. Healthcare, 10(8), 1526. https://doi.org/10.3390/healthcare10081526