
Sociodemographic and Personal Predictors of Exclusive Breastfeeding in Pregnant Mexican Women Using Public Health Services

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Setting
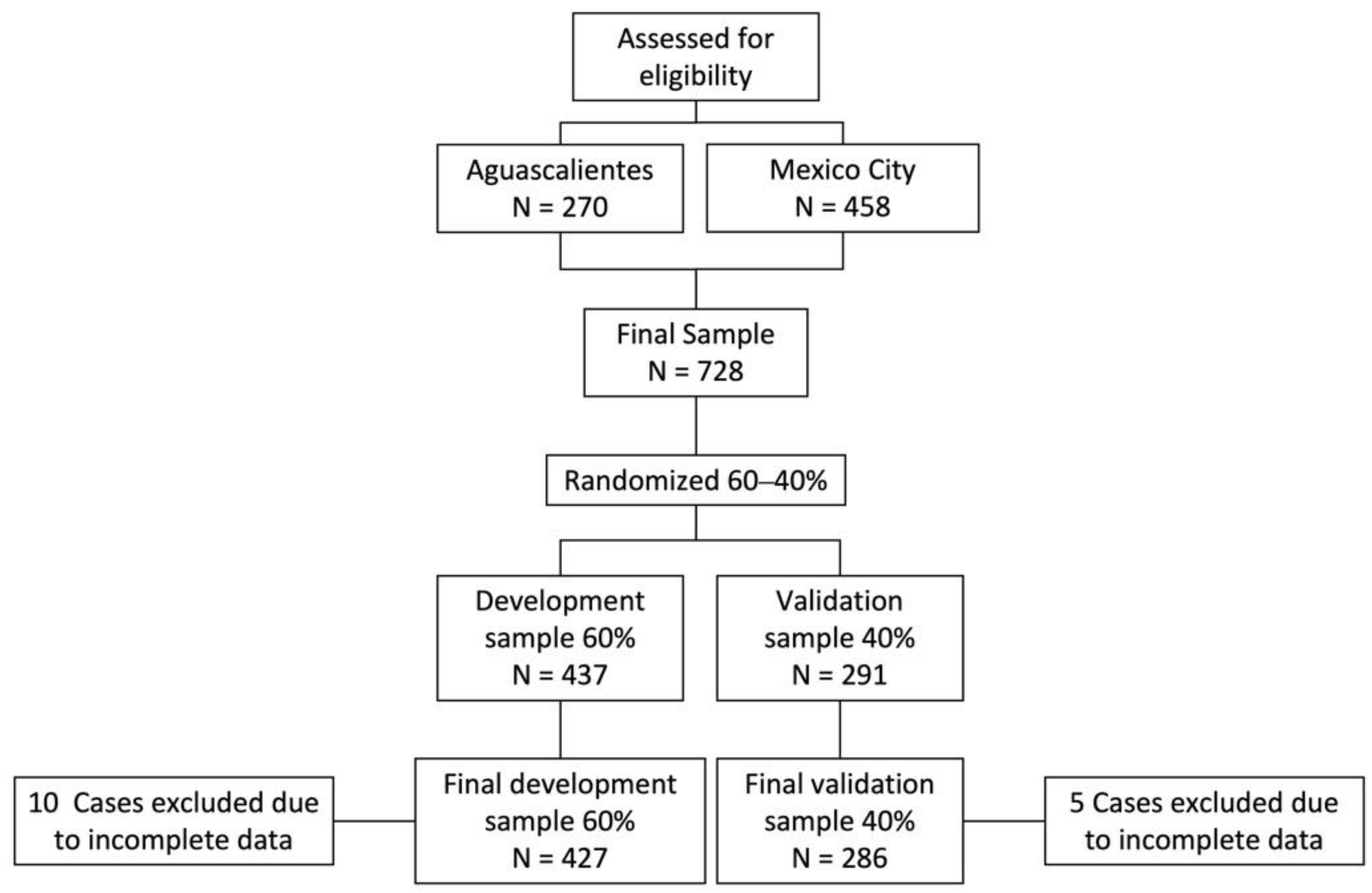
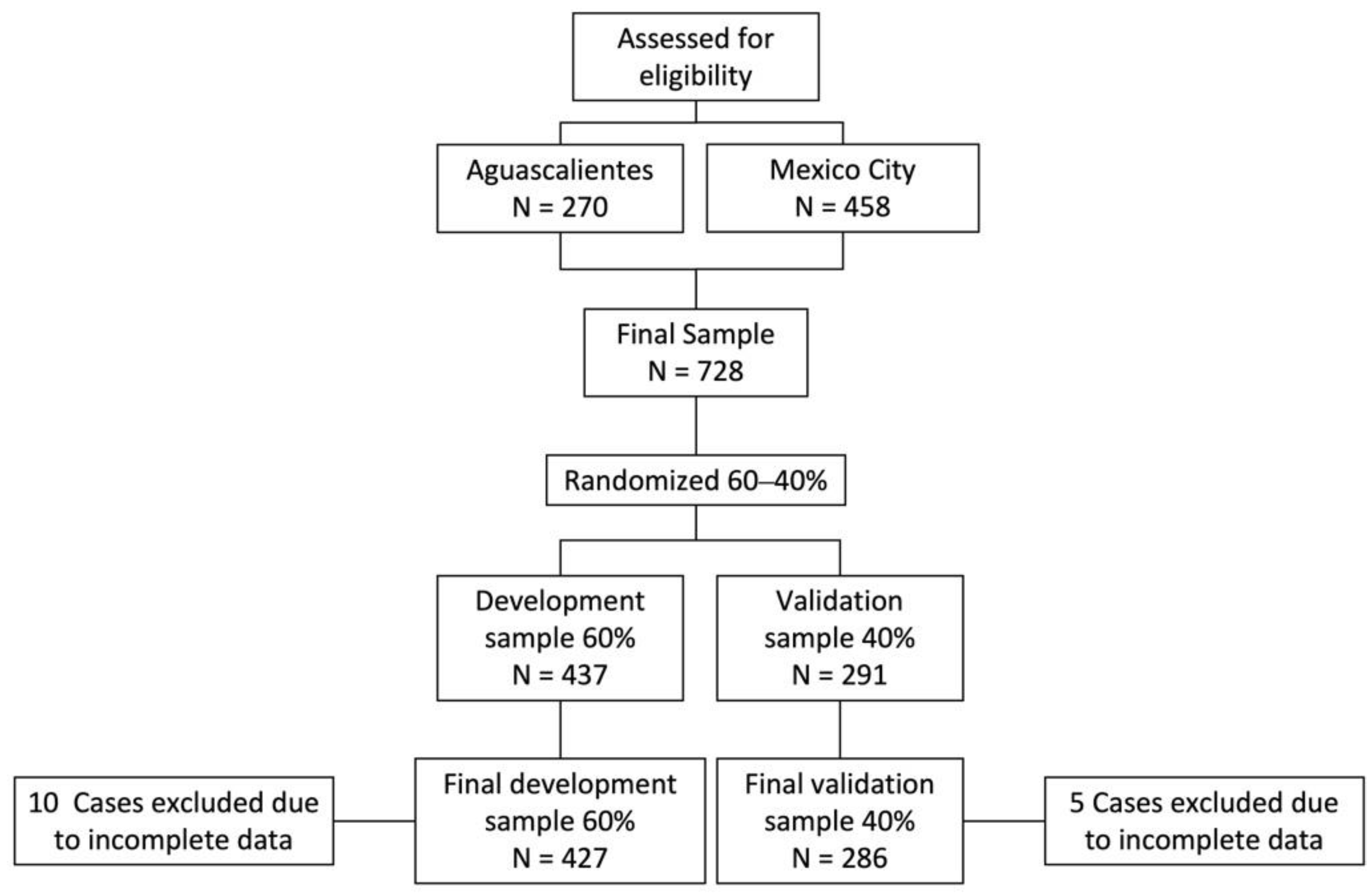
2.3. Sample
2.4. Measurement
2.5. Data Analysis
3. Results
3.1. Sociodemographic Data
3.2. Bivariate Results
3.3. Multivariate Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations Children’s Fund. UNICEF Lactancia Materna; 2022. Available online: https://www.unicef.org/mexico/lactancia-materna (accessed on 17 February 2022).
- Horta, B.L. Breastfeeding: Investing in the Future. Breastfeed. Med. 2019, 14, S11–S12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Unar-Munguía, M.; Stern, D.; Colchero, M.A.; De Cosío, T.G. The burden of suboptimal breastfeeding in Mexico: Maternal health outcomes and costs. Matern. Child Nutr. 2018, 15, e12661. [Google Scholar] [CrossRef] [PubMed]
- Word Health Organization; UNICEF. The Extension of the 2025 Maternal, Infant and Young Child Nutrition Targets to 2030; Discussion paper; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Bhattacharjee, N.V.; Schaeffer, L.E.; Hay, S.I.; Lu, D.; Schipp, M.F.; Lazzar-Atwood, A.; Donkers, K.M.; Abady, G.G.; Abd-Allah, F.; Abdelalim, A.; et al. Mapping inequalities in exclusive breastfeeding in low- and middle-income countries, 2000–2018. Nat. Hum. Behav. 2021, 5, 1027–1045. [Google Scholar] [CrossRef]
- Shamah-Levy, T.; Cuevas-Nasu, L.; Gaona-Pineda, E.B.; Gómez-Acosta, L.M.; Morales-Rúan, M.D.C.; Hernandez-Avila, M.; Rivera-Dommarco, J. Sobrepeso y obesidad en niños y adolescentes en México, actualización de la Encuesta Nacional de Salud y Nutrición de Medio Camino 2016. Rev. Sal. Pub. Mex. 2018, 60, 244–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- González-Castell, L.D.; Unar-Munguía, M.; Quezada-Sánchez, A.D.; Bonvecchio-Arenas, A.; Rivera-Dommarco, J. Situación de las prácticas de lactancia materna y alimentación complementaria en México: Resultados de la Ensanut 2018-19. Salud Publica Mex. 2020, 62, 704–713. [Google Scholar] [CrossRef]
- Cosío-Martínez, T.G.; Hernández Cordero, S. Barreras de la lactancia materna en México. In Lactancia Matera en México; Bonvecchino Arenas, A., Théodore Rowlerson, F., Gonzalez, W., Lozada Tequeanes, A.L., Alvaro Casas, R., Blanco García, I., Eds.; CONACYT: Ciudad de México, Mexico, 2016; ISBN 978-607-443-625-9. [Google Scholar]
- Patil, D.S.; Pundir, P.; Dhyani, V.S.; Krishnan, J.B.; Parsekar, S.S.; D’Souza, S.M.; Ravishankar, N.; Renjith, V. A mixed-methods systematic review on barriers to exclusive breastfeeding. Nutr. Healths 2020, 26, 323–346. [Google Scholar] [CrossRef]
- Ejie, I.L.; Eleje, G.U.; Chibuzor, M.T.; Anetoh, M.U.; Nduka, I.J.; Umeh, I.B.; Ogbonna, B.O.; Ekwunife, O.I. A systematic review of qualitative research on barriers and facilitators to exclusive breastfeeding practice in sub-Saharan African countries. Int. Breastfeed. J. 2021, 16, 44. [Google Scholar] [CrossRef] [PubMed]
- Winegar, R.; Johnson, A. Do workplace policies influence a woman’s decision to breastfeed? Nurse Pract. 2017, 42, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Gebrekidan, K.; Fooladi, E.; Plummer, V.; Hall, H. Enablers and barriers of exclusive breastfeeding among employed women in low and lower middle-income countries. Sex. Reprod. Health. 2020, 25, 100514. [Google Scholar] [CrossRef] [PubMed]
- Conner, M.; Norman, P. Health behaviour: Current issues and challenges. Psychol. Health 2017, 32, 895–906. [Google Scholar] [CrossRef] [Green Version]
- Predicting and Changing Health Behaviour. Research and Practice with Social Cognition Models, 3rd ed.; Conner, M., Norman, P., Eds.; Open University Press: Berkshire, UK, 2015; ISBN 10: 0-335-26378-X. [Google Scholar]
- Bartle, N.C.; Harvey, K. Explaining infant feeding: The role of previous personal and vicarious experience on attitudes, subjective norms, self-efficacy, and breastfeeding outcomes. Br. J. Health Psychol. 2017, 22, 763–785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, J.; Wang, T.; Liao, J.; Huang, C. Efficacy of the theory of planned behavior in predicting breastfeeding: Meta-analysis and structural equation modeling. Appl. Nurs. Res. 2015, 29, 37–42. [Google Scholar] [CrossRef]
- Hmone, M.P.; Li, M.; Agho, K.; Alam, A.; Dibley, M.J. Factors associated with intention to exclusive breastfeed in central women’s hospital, Yangon, Myanmar. Int. Breastfeed. J. 2017, 12, 29. [Google Scholar] [CrossRef] [Green Version]
- Lau, C.Y.K.; Lok, K.Y.W.; Tarrant, M. Breastfeeding Duration and the Theory of Planned Behavior and Breastfeeding Self-Efficacy Framework: A Systematic Review of Observational Studies. Matern. Child Health J. 2018, 22, 327–342. [Google Scholar] [CrossRef] [PubMed]
- Balogun, O.O.; Dagvadorj, A.; Anigo, K.M.; Ota, E.; Sasaki, S. Factors influencing breastfeeding exclusivity during the first 6 months of life in developing countries: A quantitative and qualitative systematic review. Matern. Child Nutr. 2015, 11, 433–451. [Google Scholar] [CrossRef] [PubMed]
- Khasawneh, W.; Kheirallah, K.; Mazin, M.; Abdulnabi, S. Knowledge, attitude, motivation and planning of breastfeeding: A cross-sectional study among Jordanian women. Int. Breastfeed. J. 2020, 15, 60. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez-De-Terán-Moreno, G.; Ruiz-Litago, F.; Ariz, U.; Fernández-Atutxa, A.; Mulas-Martín, M.-J.; Benito-Fernández, E.; Sanz, B. Successful breastfeeding among women with intention to breastfeed: From physiology to socio-cultural factors. Early Hum. Dev. 2021, 164, 105518. [Google Scholar] [CrossRef]
- Naja, F.; Chatila, A.; Ayoub, J.J.; Abbas, N.; Mahmoud, A.; Abdulmalik, M.A.; Nasreddine, L.; Collaborators, M. Prenatal breastfeeding knowledge, attitude and intention, and their associations with feeding practices during the first six months of life: A cohort study in Lebanon and Qatar. Int. Breastfeed. J. 2022, 17, 15. [Google Scholar] [CrossRef] [PubMed]
- Chantry, C.J.; Dewey, K.G.; Peerson, J.M.; Wagner, E.A.; Nommsen-Rivers, L.A. In-Hospital Formula Use Increases Early Breastfeeding Cessation Among First-Time Mothers Intending to Exclusively Breastfeed. J. Pediatr. 2014, 164, 1339–1345.e5. [Google Scholar] [CrossRef] [Green Version]
- Keddem, S.; Frasso, R.; Dichter, M.; Hanlon, A. The Association Between Pregnancy Intention and Breastfeeding. J. Hum. Lact. 2017, 34, 97–105. [Google Scholar] [CrossRef] [Green Version]
- Bandura, A. Health Promotion by Social Cognitive Means. Health Educ. Behav. 2004, 31, 143–164. [Google Scholar] [CrossRef] [PubMed]
- Brockway, M.; Benzies, K.; Hayden, K.A. Interventions to Improve Breastfeeding Self-Efficacy and Resultant Breastfeeding Rates: A Systematic Review and Meta-Analysis. J. Hum. Lact. 2017, 33, 486–499. [Google Scholar] [CrossRef]
- Ranganathan, P.; Pramesh, C.S.; Aggarwal, R. Common pitfalls in statistical analysis: Logistic regression. Perspect. Clin. Res. 2017, 8, 148–151. [Google Scholar] [PubMed]
- Gómez-García, J.A.; Rojas-Russell, M.E.; Serrano-Alvarado, K.; Juárez-Castelán, M.A.; Huerta-Ibáñez, A.; Ramírez-Aguilar, M. Intención de Lactar exclusivamente con Leche Materna: Un Estudio Basado en la Teoría de la Conducta Planeada. Clínica Salud 2020, 31, 13–20. [Google Scholar] [CrossRef]
- Ajzen, I. Explaining Intentions and Behavior. In Attitudes, Personality and Behavior; Ajzen, I., Ed.; Open University Press: Berkshire, UK, 2005; pp. 117–140. ISBN 978-0-335-21703-8. [Google Scholar]
- Fishbein, M.; Ajzen, I. Belief, Attitude, Intention and Behavior. An Introduction to Theory and Research; Addison-Wesley: Reading, MA, USA, 1975; ISBN 0201020890. [Google Scholar]
- Duckett, L.; Henly, S.; Avery, M.; Potter, S.; Hills-Bonczyk, S.; Hulden, R.; Savik, K. A Theory of Planned Behavior-Based Structural Model for Breast-Feeding. Nurs. Res. 1998, 47, 325–336. [Google Scholar] [CrossRef] [PubMed]
- Ajzen, I.; Sheikh, S. Action versus inaction: Anticipated affect in the theory of planned behavior. J. Appl. Soc. Psychol. 2013, 43, 155–162. [Google Scholar] [CrossRef]
- Castelán, M.A.J.; Russell, M.E.R.; Alvarado, K.S.; García, J.A.G.; Ibáñez, A.H.; Aguilar, M.R. Diseño y validación de un instrumento para medir la autoeficacia para lactar de mujeres embarazadas mexicanas. Psychologia 2018, 12, 25–34. [Google Scholar] [CrossRef]
- Evans, N.T.; Hsu, Y.-L.; Sheu, J.-J. Path Model Validation of Breastfeeding Intention Among Pregnant Women. J. Obstet. Gynecol. Neonatal Nurs. 2021, 50, 167–180. [Google Scholar] [CrossRef] [PubMed]
- Grano, C.; Fernandes, M.; Conner, M. Predicting intention and maintenance of breastfeeding up to 2-years after birth in primiparous and multiparous women. Psychol. Health 2022, 1–17. [Google Scholar] [CrossRef]
- Fernandes, R.C.; Höfelmann, D.A. Intention to Breastfeed among Pregnant Women: Association with Work, Smoking, and Previous Breastfeeding Experience. Cienc. Saude Coletiva 2020, 25, 1061–1072. [Google Scholar] [CrossRef] [PubMed]
- Mattiello, R.; Kotoski, A.; Ayala, C.O.; Recha, C.L.; Quiroga, C.V.; Machado, C.R.; Roxo, C.D.O.; Varela, F.H.; Couto, G.T.; Cassão, G.; et al. Prevalence and factors associated with no intention to exclusively breastfeed for the first 6 months of life. J. de Pediatr. 2021, 98, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Claesson, I.-M.; Myrgård, M.; Wallberg, M.; Blomberg, M. Pregnant women’s intention to breastfeed; their estimated extent and duration of the forthcoming breastfeeding in relation to the actual breastfeeding in the first year postpartum—A Swedish cohort study. Midwifery 2019, 76, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Marshall, S.; Jones, J.M.; Phongsavan, P.; Wen, L.M. Modifiable predictors of breastfeeding status and duration at 6 and 12 months postpartum. Birth 2021, 49, 97–106. [Google Scholar] [CrossRef]
- Ayers, B.L.; Purvis, R.S.; White, A.; CarlLee, S.; Andersen, J.A.; Bogulski, C.A.; McElfish, P.A. Best of Intentions: Influential Factors in Infant Feeding Intent among Marshallese Pregnant Women. Int. J. Environ. Res. Public Health 2022, 19, 1740. [Google Scholar] [CrossRef] [PubMed]
- Wallenborn, J.T.; Perera, R.A.; Wheeler, D.C.; Lu, J.; Masho, S.W. Workplace support and breastfeeding duration: The mediating effect of breastfeeding intention and self-efficacy. Birth 2018, 46, 121–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baumgartner, T.; Bhamidipalli, S.S.; Guise, D.; Daggy, J.; Parker, C.B.; Westermann, M.; Parry, S.; Grobman, W.A.; Mercer, B.M.; Simhan, H.N.; et al. Psychosocial and Sociodemographic Contributors to Breastfeeding Intention in First-Time Mothers. Matern. Child Health J. 2020, 24, 1047–1056. [Google Scholar] [CrossRef]
- Brown, A. Breastfeeding as a public health responsibility: A review of the evidence. J. Hum. Nutr. Diet. 2017, 30, 759–770. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristics | Development Sample | Validation Sample | ||
|---|---|---|---|---|
| % | [95% CI] | % | [95% CI] | |
| N | 427 | 286 | ||
| Age (years) | ||||
| ≤1 | 34.4 | [30.0, 39.0] | 29.0 | [24.0, 34.5] |
| 22–27 | 31.3 | [27.1, 35.9] | 34.6 | [29.3, 40.3] |
| ≥8 | 34.1 | [29.8, 38.8] | 36.4 | [30.9, 42.1] |
| Socioeconomic level | ||||
| Low | 57.1 | [52.4, 61.8] | 54.5 | [48.7, 60.3] |
| High | 42.8 | [38.2, 47.6] | 45.4 | [39.7, 51.3] |
| Marital status | ||||
| Single | 23 | [19.2, 27.2] | 19.6 | [15.4, 24.6] |
| Married/Consensual union | 76.7 | [72.7, 80.8] | 80.4 | [75.4, 84.6] |
| Working status | ||||
| Not Working | 66.5 | [61.9, 70.8] | 64.6 | [58.9, 70.0] |
| Working | 33.5 | [29.1, 38.1] | 35.3 | [29.9, 41.1] |
| Education level | ||||
| Middle school or less | 49.9 | [45.1, 54.6] | 51.7 | [45.9, 57.5] |
| High school or more | 50.1 | [45.4, 54.8] | 48.2 | [42.4, 54.1] |
| Planned pregnancy | ||||
| No | 46.6 | [41.8, 51.4] | 46.8 | [41.1, 52.7] |
| Yes | 53.4 | [48.6, 58.1] | 53.1 | [47.3, 58.9] |
| Weeks of pregnancy # | 27 | [20, 33] | 26.0 | [20, 32] |
| Parity | ||||
| Primiparous | 43.7 | [39.0, 48.4] | 41.9 | [36.3, 47.8] |
| Multiparous | 56.3 | [51.6, 60.9] | 58.0 | [52.2, 63.7] |
| Characteristics | Total | Low Intention | High Intention | ||||
|---|---|---|---|---|---|---|---|
| % | [95% CI] | % | [95% CI] | % | [95% CI] | ||
| Sample size n (%) | 427 | 156 [0.36] | 271 [0.63] | ||||
| Age | * | ||||||
| <21 years | 34.4 | [30.0, 39.0] | 42.3 | [34.7, 50.3] | 29.8 | [24.7, 35.6] | |
| 22–27 | 31.3 | [27.1, 35.9] | 21 | [15.4, 28.3] | 37.3 | [31.7, 43.2] | |
| ≥28 | 34.1 | [29.8, 38.8] | 37 | [29.3, 44.4] | 32.8 | [27.5, 38.7] | |
| Socioeconomic level | |||||||
| Low | 57.1 | [52.4, 61.8] | 55 | [47.2, 62.8] | 48.3 | [39.3, 57.4] | |
| High | 42.8 | [38.2, 47.6] | 45 | [37.2, 52.8] | 51.7 | [42.6, 60.7] | |
| Marital status | |||||||
| Single | 23 | [19.2, 27.2] | 25 | [18.8, 32.5] | 21.8 | [17.3, 27.2] | |
| Married/Consensual union | 76.7 | [72.7, 80.8] | 75 | [67.5, 81.2] | 78.1 | [72.8, 82.7] | |
| Working status | * | ||||||
| Not Working | 66.5 | [61.9, 70.8] | 60 | [52.3, 67.7] | 70.1 | [64.3, 75.3] | |
| Working | 33.5 | [29.1, 38.1] | 40 | [32.3, 47.7] | 29.9 | [24.7, 35.6] | |
| Education level | |||||||
| Middle school or less | 49.9 | [45.1, 54.6] | 52 | [44.0, 59.7] | 48.7 | [42.8, 54.7] | |
| High school or more | 50.1 | [45.4, 54.8] | 48 | [40.3, 55.9] | 51.3 | [45.3, 57.2] | |
| Planned pregnancy | |||||||
| No | 46.6 | [41.8, 51.4] | 49 | [41.5, 57.2] | 45 | [39.1, 51.0] | |
| Yes | 53.4 | [48.6, 58.1] | 51 | [42.7, 58.5] | 54.9 | [48.9, 60.8] | |
| Weeks of pregnancy # | 27 | [20, 33] | 26 | [18, 32] | 27 | [20, 33] | |
| Parity | |||||||
| Primiparous | 43.7 | [39.0, 48.4] | 47 | [39.0, 54.7] | 41.8 | [36.1, 47.8] | |
| Multiparous | 56.3 | [51.6, 60.9] | 53 | [45.3, 60.9] | 58.1 | [52.1, 63.9] | |
| Personal Characteristics | Total | Low Intention | High Intention | ||||
|---|---|---|---|---|---|---|---|
| Median | [Q1, Q3] | Median | [Q1, Q3] | Median | [Q1, Q3] | ||
| Sample size n (%) | 427 | 156 [36.5] | 271 [63.5] | ||||
| Attitudes | |||||||
| Positive attitudes to physical symptoms | 21 | [15, 27] | 20 | [15, 24] | 23 | [16, 28] | * |
| Positive attitudes to emotions | 64 | [57, 70] | 61 | [48, 66] | 66 | [60, 70] | * |
| Positive attitudes to naturalness breastfeeding | 39 | [34, 40] | 37 | [32, 40] | 40 | [35, 40] | * |
| Perceived Behavioral Control | |||||||
| Perceived difficulty to breastfeed in public | 7 | [5, 9] | 7 | [5, 10] | 6 | [4, 9] | * |
| Perceived of tension and lack of time | 10 | [8, 13] | 11 | [9, 14] | 10 | [7, 13] | * |
| Perceived of comfort and calm | 27 | [22, 31] | 26 | [22, 30] | 28 | [23, 31] | * |
| Subjective Norm | |||||||
| Family opinion | 3 | [1, 9] | 3 | [1, 9] | 3 | [0, 9] | |
| Partner opinion | 6 | [3, 9] | 6 | [3, 9] | 9 | [3, 9] | |
| Mother opinion | 4 | [1, 9] | 4 | [0, 9] | 6 | [2, 9] | * |
| Sister(s)-in-law opinion | 1 | [0, 4] | 1 | [0, 4] | 1 | [0, 6] | |
| Mother-in-law opinion | 2 | [0, 9] | 2 | [0, 6] | 3 | [0, 9] | |
| Doctor opinion | 9 | [4, 9] | 6 | [4, 9] | 9 | [6, 9] | * |
| Anticipated feelings | |||||||
| Positive feelings | 1 | [0, 4] | 2 | [0, 4] | 0 | [0, 4] | * |
| Negative feelings | 4 | [0, 9] | 6 | [0, 9] | 3 | [0, 9] | * |
| Breastfeeding self-efficacy | 37 | [28, 45] | 33 | [24, 42] | 38 | [29, 46] | * |
| Variable | n | OR | [95% CI] | |
|---|---|---|---|---|
| Sociodemographic variables | ||||
| Age. Reference: ≤21 years | 427 | |||
| 22–27 | 2.49 | [1.49, 4.15] | * | |
| ≥28 | 1.27 | [0.79, 2.02] | ||
| Socioeconomic level. Reference: Low | 427 | |||
| High | 0.87 | [0.59, 1.31] | ||
| Marital Status. Reference: Single | 426 | |||
| Married/consensual union | 1.19 | [0.75, 1.89] | ||
| Working status. Reference: Not working | 427 | |||
| Working | 0.64 | [0.43, 0.98] | * | |
| Education level. Reference: Middle school or less | 427 | |||
| High school or more | 1.14 | [0.77, 1.69] | ||
| Pregnancy variables | ||||
| Planned pregnancy. Reference: No | 427 | |||
| Yes | 1.19 | [0.80, 1.77] | ||
| Parity. Reference: Primiparous | 426 | |||
| Multiparous | 1.22 | [0.82, 1.81] | ||
| Weeks of pregnancy | 426 | 1.02 | [0.99, 1.04] | + |
| Personal variables by tertiles | ||||
| Attitudes | ||||
| Positive attitudes to physical symptoms. Reference: tertile 1 | 427 | |||
| tertile 2 | 0.95 | [0.59, 1.53] | ||
| tertile 3 | 2.32 | [1.39, 3.89] | * | |
| Positive attitudes to emotions. Reference: 1 tertile 1 | 427 | |||
| tertile 2 | 2.46 | [1.51, 4.00] | * | |
| tertile 3 | 5.11 | [3.02, 8.65] | * | |
| Positive attitudes to naturalness breastfeeding. Reference: tertile 1 | 427 | |||
| tertile 2 | 1.23 | [0.72, 2.09] | ||
| tertile 3 | 2.43 | [1.53, 3.85] | * | |
| Perceived Behavioral Control | ||||
| Perceived difficulty to breastfeed in public. Reference: tertile 1 | 426 | |||
| tertile 2 | 0.79 | [0.46, 1.37] | ||
| tertile 3 | 0.57 | [0.34, 0.97] | * | |
| Perceived of tension and lack of time. Reference: tertile 1 | 426 | |||
| tertile 2 | 0.63 | [0.36, 1.09] | + | |
| tertile 3 | 0.45 | [0.27, 0.78] | * | |
| Perceived of comfort and calm. Reference: tertile 1 | 424 | |||
| tertile 2 | 1.12 | [0.69, 1.82] | ||
| tertile 3 | 1.75 | [1.06, 2.88] | * | |
| Subjective Norm | ||||
| Family opinion. Reference: tertile 1 | 413 | |||
| tertile 2 | 0.74 | [0.44, 1.25] | ||
| tertile 3 | 0.88 | [0.55, 1.42] | ||
| Partner opinion. Reference: tertile 1 | 403 | |||
| tertile 2 | 0.9 | [0.50, 1.62] | ||
| tertile 3 | 1.15 | [0.73, 1.82] | ||
| Mother opinion. Reference: tertile 1 | 415 | |||
| tertile 2 | 1.72 | [1.04, 2.84] | * | |
| tertile 3 | 1.88 | [1.16, 3.05] | * | |
| Sister(s)-in-law opinion. Reference: low # | 358 | |||
| High | 1.00 | [0.65, 1.54] | ||
| Mother-in-law opinion. Reference: low # | 377 | |||
| High | 1.24 | [0.81, 1.88] | ||
| Doctor opinion. Reference: tertile 1 | 419 | |||
| tertile 2 | 1.22 | [0.65, 2.29] | ||
| tertile 3 | 2.41 | [1.54, 3.79] | * | |
| Anticipated feelings | ||||
| Positive feelings. Reference: Low # | 427 | |||
| High | 0.51 | [0.26, 1.03] | + | |
| Negative feelings. Reference: Low # | 425 | |||
| High | 0.78 | [0.52, 1.16] | ||
| Self-efficacy | ||||
| Breastfeeding self-efficacy. Reference: tertile 1 | 427 | |||
| tertile 2 | 1.16 | [0.72, 1.87] | ||
| tertile 3 | 2.85 | [1.71, 4.73] | * |
| Variable | OR | [95% CI] | |
|---|---|---|---|
| Positive attitudes to emotions: Reference tertile 1 | |||
| Tertile 2 | 2.43 | [1.44, 4.07] | * |
| Tertile 3 | 4.19 | [2.39, 7.37] | * |
| Breastfeeding self-efficacy: Reference tertile 1 | |||
| Tertile 2 | 0.89 | [0.53, 1.51] | |
| Tertile 3 | 2.12 | [1.20, 3.72] | * |
| Doctor opinion: Reference tertile 1 | |||
| Tertile 2 | 1.16 | [0.58, 2.29] | |
| Tertile 3 | 2.04 | [1.25, 3.32] | * |
| Age: Reference < 21 years | |||
| 22–27 | 2.42 | [1.37, 4.26] | * |
| ≥ 28 | 1.38 | [0.79, 2.39] | |
| Working status: Reference Not working | |||
| Working | 0.61 | [0.37, 0.98] | * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serrano-Alvarado, K.; Castro-Porras, L.V.; Astudillo-García, C.I.; Rojas-Russell, M.E. Sociodemographic and Personal Predictors of Exclusive Breastfeeding in Pregnant Mexican Women Using Public Health Services. Healthcare 2022, 10, 1432. https://doi.org/10.3390/healthcare10081432
Serrano-Alvarado K, Castro-Porras LV, Astudillo-García CI, Rojas-Russell ME. Sociodemographic and Personal Predictors of Exclusive Breastfeeding in Pregnant Mexican Women Using Public Health Services. Healthcare. 2022; 10(8):1432. https://doi.org/10.3390/healthcare10081432
Chicago/Turabian StyleSerrano-Alvarado, Karina, Lilia V. Castro-Porras, Claudia I. Astudillo-García, and Mario E. Rojas-Russell. 2022. "Sociodemographic and Personal Predictors of Exclusive Breastfeeding in Pregnant Mexican Women Using Public Health Services" Healthcare 10, no. 8: 1432. https://doi.org/10.3390/healthcare10081432
APA StyleSerrano-Alvarado, K., Castro-Porras, L. V., Astudillo-García, C. I., & Rojas-Russell, M. E. (2022). Sociodemographic and Personal Predictors of Exclusive Breastfeeding in Pregnant Mexican Women Using Public Health Services. Healthcare, 10(8), 1432. https://doi.org/10.3390/healthcare10081432