
A Systematic Review of Clinical Outcomes from Pharmacist Provided Medication Therapy Management (MTM) among Patients with Diabetes, Hypertension, or Dyslipidemia

 ,
, 
 ,
, 
Abstract
1. Introduction
2. Methods
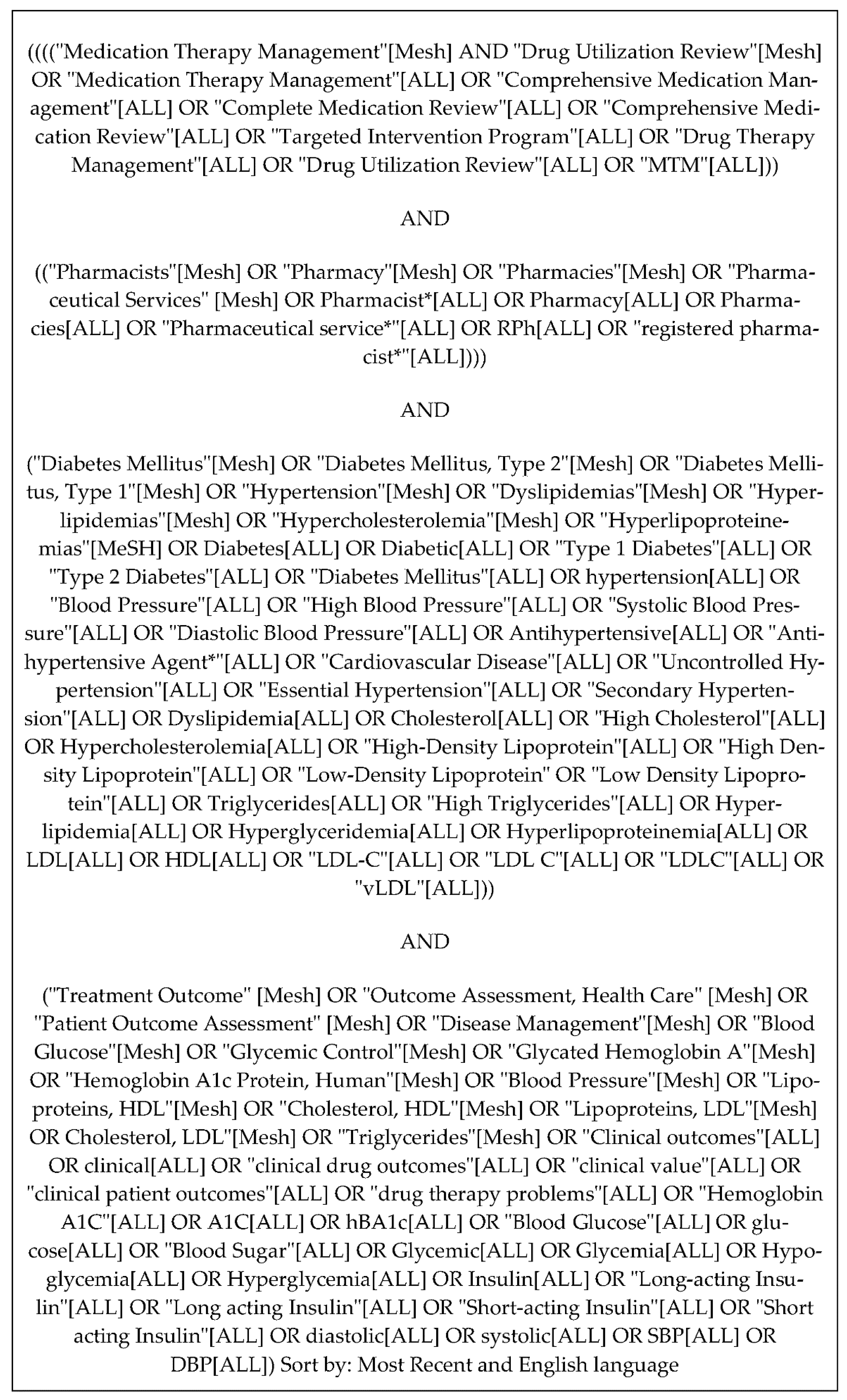
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Study Selection
2.4. Risk of Bias Assessment
3. Results
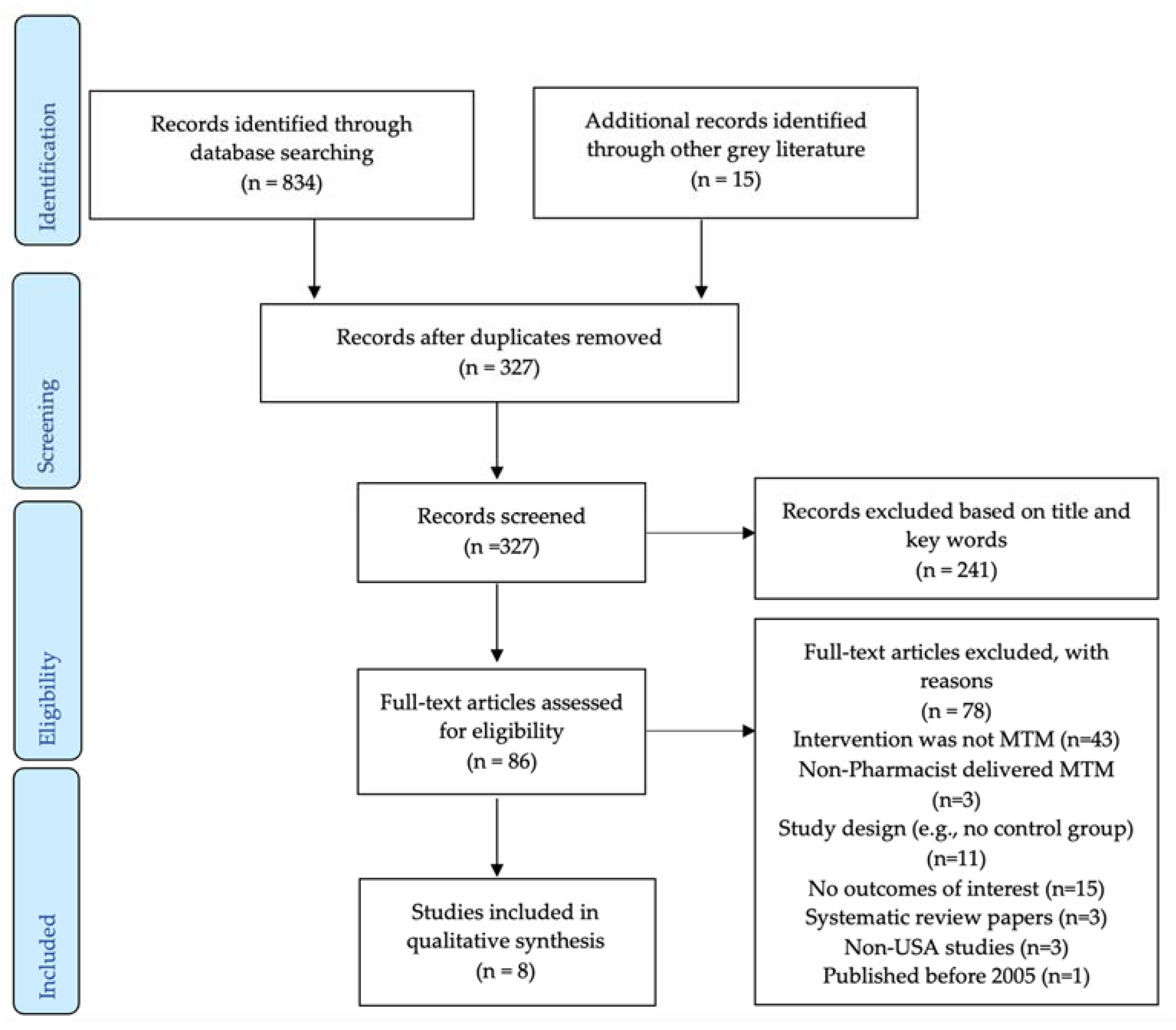
3.1. Study Selection
3.2. Characteristics of Included Studies
3.3. Results of Individual Studies
3.4. Risk of Bias in Included Studies
4. Discussion
4.1. Diabetes
4.2. Hypertension
4.3. Dyslipidemia
4.4. Clinical Implications
4.5. Limitations
4.6. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Joint Commission of Pharmacy Practitioners. The Pharmacists’ Patient Care Process. Available online: https://jcpp.net/wp-content/uploads/2016/03/PatientCareProcess-with-supporting-organizations.pdf (accessed on 24 January 2022).
- H.R.1—108th Congress (2003–2004): Medicare Prescription Drug, Improvement, and Modernization Act of 2003. Available online: https://www.congress.gov/bill/108th-congress/house-bill/1 (accessed on 24 January 2022).
- Bluml, B.M. Definition of Medication Therapy Management: Development of Professionwide Consensus. J. Am. Pharm. Assoc. 2005, 45, 566–572. [Google Scholar] [CrossRef] [PubMed]
- Chavez-Valdez, A.L. Release of the CY 2020 MTM Program Submission Module in HPMS a CMS-Approved MTM Program Is One of Several Required Elements in the Development of a Medicare Part D Sponsor’s Bid. Annually, Sponsors Must Submit an MTM Program. 2019. Available online: https://www.cms.gov/Medicare/Prescription-Drug-Coverage/PrescriptionDrugCovContra/Downloads/Memo-Contract-Year-2020-Medication-Therapy-Management-MTM-Program-Submission-v-041019-.pdf (accessed on 24 January 2022).
- The Centers for Medicare & Medicaid Services. 2016 Final Advance Notice. Available online: https://www.cms.gov/Medicare/HealthPlans/MedicareAdvtgSpecRateStats/Downloads/Advance2016.pdf (accessed on 24 January 2022).
- Barnett, M.; Frank, J.; Wehring, H.; Newland, B.; VonMuenster, S.; Kumbera, P.; Halterman, T.; Perry, P.J. Analysis of Pharmacist-Provided Medication Therapy Management(MTM) Services in Community Pharmacies over 7 Years. J. Manag. Care Pharm. 2009, 15, 18–31. [Google Scholar] [CrossRef] [PubMed]
- Ferries, E.; Dye, J.T.; Hall, B.; Ndehi, L.; Schwab, P.; Vaccaro, J. Comparison of Medication Therapy Management Services and Their Effects on Health Care Utilization and Medication Adherence. J. Manag. Care Spec. Pharm. 2019, 25, 688–695. [Google Scholar] [CrossRef] [PubMed]
- Pal, A.; Babbott, S.; Wilkinson, S.T. Can the Targeted Use of a Discharge Pharmacist Significantly Decrease 30-Day Readmissions? Hosp. Pharm. 2013, 48, 380–388. [Google Scholar] [CrossRef] [PubMed]
- Viswanathan, M.; Kahwati, L.C.; Golin, C.E.; Blalock, S.J.; Coker-Schwimmer, E.; Posey, R.; Lohr, K.N. Medication Therapy Management Interventions in Outpatient Settings. JAMA Intern. Med. 2015, 175, 76. [Google Scholar] [CrossRef]
- National Institute of Diabetes and Digestive and Kidney Diseases. Diabetes. U.S. Department of Health and Human Services. Available online: https://www.niddk.nih.gov/health-information/diabetes (accessed on 24 January 2022).
- American Diabetes Association. Understanding A1c. Available online: https://www.diabetes.org/a1c/diagnosis (accessed on 24 January 2022).
- Cleveland Clinic. Diabetes: An Overview. Available online: https://my.clevelandclinic.org/health/diseases/7104-diabetes-mellitus-an-overview (accessed on 24 January 2022).
- Centers for Disease Control and Prevention. Estimating Hypertension Prevalence, Treatment, and Control among U.S. Adults. Million Hearts. Available online: https://millionhearts.hhs.gov/data-reports/hypertension-prevalence.html (accessed on 24 January 2022).
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J.; Himmelfarb, C.D.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults. J. Am. Coll. Cardiol. 2018, 71, e127–e248. [Google Scholar] [CrossRef]
- Pappan, N.; Rehman, A. Dyslipidemia. Available online: https://www.ncbi.nlm.nih.gov/books/NBK560891/ (accessed on 6 February 2022).
- Centers for Disease Control and Prevention. Total and high-density lipoprotein cholesterol in adults: United States, 2015–2018. Available online: https://www.cdc.gov/nchs/data/databriefs/db363-h.pdf (accessed on 27 June 2022).
- Centers for Disease Control and Prevention. Community Pharmacists and Medication Therapy Management. Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/dhdsp/pubs/guides/best-practices/pharmacist-mtm.htm (accessed on 27 June 2022).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Br. Med. J. 2021, 372, n71. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A Tool for Assessing Risk of Bias in Non-Randomised Studies of Interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Hirsch, J.D.; Steers, N.; Adler, D.S.; Kuo, G.M.; Morello, C.M.; Lang, M.; Singh, R.F.; Wood, Y.; Kaplan, R.M.; Mangione, C.M. Primary Care–Based, Pharmacist–Physician Collaborative Medication-Therapy Management of Hypertension: A Randomized, Pragmatic Trial. Clin. Ther. 2014, 36, 1244–1254. [Google Scholar] [CrossRef]
- Planas, L.G.; Crosby, K.M.; Mitchell, K.D.; Farmer, K.C. Evaluation of a Hypertension Medication Therapy Management Program in Patients with Diabetes. J. Am. Pharm. Assoc. 2009, 49, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Brummel, A.R.; Soliman, A.M.; Carlson, A.M.; de Oliveira, D.R. Optimal Diabetes Care Outcomes Following Face-To-Face Medication Therapy Management Services. Popul. Health Manag. 2013, 16, 28–34. [Google Scholar] [CrossRef]
- Fox, D.; Ried, L.D.; Klein, G.E.; Myers, W.; Foli, K. A Medication Therapy Management Program’s Impact on Low-Density Lipoprotein Cholesterol Goal Attainment in Medicare Part D Patients with Diabetes. J. Am. Pharm. Assoc. 2009, 49, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Pindolia, V.K.; Stebelsky, L.; Romain, T.M.; Luoma, L.; Nowak, S.N.; Gillanders, F. Mitigation of Medication Mishaps via Medication Therapy Management. Ann. Pharmacother. 2009, 43, 611–620. [Google Scholar] [CrossRef] [PubMed]
- Prudencio, J.; Cutler, T.; Roberts, S.; Marin, S.; Wilson, M. The Effect of Clinical Pharmacist-Led Comprehensive Medication Management on Chronic Disease State Goal Attainment in a Patient-Centered Medical Home. J. Manag. Care Spec. Pharm. 2018, 24, 423–429. [Google Scholar] [CrossRef]
- Skinner, J.S.; Poe, B.; Hopper, R.; Boyer, A.; Wilkins, C.H. Assessing the Effectiveness of Pharmacist-Directed Medication Therapy Management in Improving Diabetes Outcomes in Patients with Poorly Controlled Diabetes. Diabetes Educ. 2015, 41, 459–465. [Google Scholar] [CrossRef]
- Tilton, J.J.; Edakkunnathu, M.G.; Moran, K.M.; Markel Vaysman, A.; DaPisa, J.L.; Goen, B.M.; Touchette, D.R. Impact of a Medication Therapy Management Clinic on Glycosylated Hemoglobin, Blood Pressure, and Resource Utilization. Ann. Pharmacother. 2018, 53, 13–20. [Google Scholar] [CrossRef]
- Measurement Resources. MN Community Measurement. Measurement Resources. Available online: https://mncm.org/measurement-resources/#:~:text=The%20D5%20is%20a%20set (accessed on 24 January 2022).
- Clifford, R.M.; Batty, K.T.; Davis, T.M.E.; Davis, W.; Stein, G.; Stewart, G.; Plumridge, R.J. A Randomised Controlled Trial of a Pharmaceutical Care Programme in High-Risk Diabetic Patients in an Outpatient Clinic. Int. J. Pharm. Pract. 2002, 10, 85–89. [Google Scholar] [CrossRef]
- Ndefo, U.A.; Moultry, A.M.; Davis, P.N.; Askew, R. Provision of Medication Therapy Management by Pharmacists to Patients with Type-2 Diabetes Mellitus in a Federally Qualified Health Center. Pharm. Ther. 2017, 42, 632–637. [Google Scholar]
- Smith, M. Pharmacists’ Role in Improving Diabetes Medication Management. J. Diabetes Sci. Technol. 2009, 3, 175–179. [Google Scholar] [CrossRef]
- Reeves, L.; Robinson, K.; McClelland, T.; Adedoyin, C.A.; Broeseker, A.; Adunlin, G. Pharmacist Interventions in the Management of Blood Pressure Control and Adherence to Antihypertensive Medications: A Systematic Review of Randomized Controlled Trials. J. Pharm. Pract. 2020, 34, 480–492. [Google Scholar] [CrossRef] [PubMed]
- Iyer, R.; Coderre, P.; McKelvey, T.; Cooper, J.; Berger, J.; Moore, E.; Kushner, M. An Employer-Based, Pharmacist Intervention Model for Patients with Type 2 Diabetes. Am. J. Health-Syst. Pharm. 2010, 67, 312–316. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Strand, M.A.; Mager, N.A.D.; Hall, L.; Martin, S.L.; Sarpong, D.F. Pharmacy Contributions to Improved Population Health: Expanding the Public Health Roundtable. Prev. Chronic Dis. 2020, 17, 200350. [Google Scholar] [CrossRef] [PubMed]
- Manolakis, P.G.; Skelton, J.B. Pharmacists’ Contributions to Primary Care in the United States Collaborating to Address Unmet Patient Care Needs: The Emerging Role for Pharmacists to Address the Shortage of Primary Care Providers. Am. J. Pharm. Educ. 2010, 74, S7. [Google Scholar] [CrossRef]
- Bayliss, E.A.; Bosworth, H.B.; Noel, P.H.; Wolff, J.L.; Damush, T.M.; Mciver, L. Supporting Self-Management for Patients with Complex Medical Needs: Recommendations of a Working Group. Chronic Illn. 2007, 3, 167–175. [Google Scholar] [CrossRef]
- Petrie, J.R.; Guzik, T.J.; Touyz, R.M. Diabetes, Hypertension, and Cardiovascular Disease: Clinical Insights and Vascular Mechanisms. Can. J. Cardiol. 2018, 34, 575–584. [Google Scholar] [CrossRef]
- O’Connor, P.J.; Bodkin, N.L.; Fradkin, J.; Glasgow, R.E.; Greenfield, S.; Gregg, E.; Kerr, E.A.; Pawlson, L.G.; Selby, J.V.; Sutherland, J.E.; et al. Diabetes Performance Measures: Current Status and Future Directions. Diabetes Care 2011, 34, 1651–1659. [Google Scholar] [CrossRef]
- Rydén, L.; Ferrannini, G.; Mellbin, L. Risk Factor Reduction in Type 2 Diabetes Demands a Multifactorial Approach. Eur. J. Prev. Cardiol. 2019, 26, 81–91. [Google Scholar] [CrossRef]
- Lee, J.K.; McCutcheon, L.R.M.; Fazel, M.T.; Cooley, J.H.; Slack, M.K. Assessment of Interprofessional Collaborative Practices and Outcomes in Adults with Diabetes and Hypertension in Primary Care: A Systematic Review and Meta-Analysis. JAMA Netw. Open 2021, 4, e2036725. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author, Year | Study Design | Settings | Insurance Status | Eligible Conditions | Mode of Delivery | Team | Frequency of Follow Up/Year | Total N | Mean Age Patients | % Male Patients |
|---|---|---|---|---|---|---|---|---|---|---|
| Hirsch, 2014 [21] | RCT | University-based primary care clinic | All plans | DM, HTN | Face to face and telephone | Collaborative pharmacist–primary care provider | ≥4 | 667 | 67.5 | 42.6 |
| Planas, 2009 [22] | RCT | Community pharmacy | Insured | DM, HTN | Face to face | Pharmacist | 12 | 52 | 64.7 | 37.2 |
| Brummel, 2006 [23] | Cohort | Comprehensive provider of pharmacy service | Medicare, Medicaid | DM | Face to face | Pharmacist | Any | 224 | 58.3 | 48.2 |
| Fox, 2009 [24] | Cohort | Managed care organization (Florida Health Care Plans) | Medicare D | DM | Telephone | Collaborative pharmacist–primary care provider | ≥3 | 2114 | 69.2 | 50.1 |
| Pindolia, 2009 [25] | Cohort | Health Alliance Plan | Health alliance plan | 26 possible chronic conditions * | Telephone | Collaborative pharmacist–primary care provider | N/A | 2681 | 73.7 | 39.8 |
| Prudencio, 2018 [26] | Cohort | Patient-Centered Medical Home | N/A | DM | Face to face | Pharmacist | ≥1 | 811 | 63.0 | 49.0 |
| Skinner, 2015 [27] | Cohort | Community health center | N/A | DM | Face to face | Pharmacist | ≥4 | 58 | 53.7 | 42.0 |
| Tilton, 2019 [28] | Cohort | Academic health center | Low income | DM, HTN | Face to face | Pharmacist | ≥3 | 316 | 69.6 | 40.5 |
| Author, Year | N Analyzed in Each Group | Follow-Up Period | Outcomes Reported | Intervention | Control | p Value |
|---|---|---|---|---|---|---|
| Hirsch, 2014 [21] | I-75 C-91 | Baseline, 3, 6, and 9 months | Mean ± SD change in LDL (mg/dL) | 6 months: 0.1 ± 19.9 | 6 months: 4.6 ± 24.1 | 0.21 |
| 9 months: −3.5 ± 26.3 | 9 months: −3.1 ± 41.9 | 0.95 | ||||
| Mean ± SD change in HDL (mg/dL) | 6 months: 2.4 ± 28.3 | 6 months: 0.3 ± 11.5 | 0.54 | |||
| 9 months: −1.0 ± 20.4 | 9 months: 0.4 ± 20.9 | 0.67 | ||||
| Mean ± SD change in SBP (mmHg) | 6 months: −7.1 ± 19.4 | 6 months: 1.6 ± 21.0 | 0.008 | |||
| 9 months: −5.2 ± 16.9 | 9 months: −1.7 ± 17.7 | 0.22 | ||||
| Mean ± SD change in DBP (mmHg) | 6 months: −3.8 ± 10.5 | 6 months: 1.7 ± 13.9 | 0.006 | |||
| 9 months: −2.5 ± 10.2 | 9 months: −0.3 ± 13.8 | 0.27 | ||||
| Planas, 2009 [22] | I-32 C-20 | Monthly within study period of 9 months | % With BP <130/80 mmHg at 9 months | 48.00 | 6.67 | 0.021 |
| Mean SBP (mmHg) at 9 months | 124.44 | 148.13 | 0.003 | |||
| Brummel, 2013 [23] | I-121 C-103 | 2006, 2007, 2008 | % With HbA1c <7% | 2006: 43.80 | 2006: 63.11 | 0.003 |
| 2007: 73.55 | 2007: 72.82 | 0.90 | ||||
| 2008: 42.15 | 2008: 59.22 | 0.01 | ||||
| % With LDL <100 mg/dL | 2006: 63.64 | 2006: 65.05 | 0.82 | |||
| 2007: 83.47 | 2007: 73.79 | 0.07 | ||||
| 2008: 79.34 | 2008: 73.79 | 0.32 | ||||
| % With BP <130/80 mmHg | 2006: 66.12 | 2006: 61.17 | 0.44 | |||
| 2007: 71.07 | 2007: 72.82 | 0.77 | ||||
| 2008: 76.03 | 2008: 69.90 | 0.30 | ||||
| Fox, 2009 [24] | I-255 C-56 | 1 January 2006– 30 September 2007 | % With LDL <100 mg/dL | 69.00 | 50.00 | <0.001 |
| Mean ± SD LDL (mg/dL) | 83.4 ± 31.2 | 90.8 ± 31.0 | <0.001 | |||
| Pindolia, 2009 [25] | I-520 C-2161 | 2006, 2007 | % Change in people with HbA1c <7% | 3 | 7 | N/A |
| % Change in people with LDL <100 mg/dL | −5 | 7 | N/A | |||
| Prudencio, 2018 [26] | I-95 C-132 | 1 October 2014– 31 October 2015 | % With HbA1c <8% | 54 | 36 | 0.010 |
| % With BP <140/90 mmHg | 93 | 77 | 0.001 | |||
| % With statin prescription | 79 | 63 | 0.010 | |||
| Skinner, 2015 [27] | I-50 C-50 | 12-month | Mean ± SD HbA1c (%) | 7.5 ± 0.38 | 10.8 ± 2.0 | <0.01 |
| Mean ± SD LDL (mg/dL) | 92.7 ± 36.4 | 110.8 ± 65.7 | 0.17 | |||
| Mean ± SD HDL (mg/dL) | 48.2 ± 10.3 | 45.2 ± 12.9 | 0.16 | |||
| Mean ± SD SBP (mmHg) | 136.5 ± 19.8 | 145.4 ± 17.8 | 0.12 | |||
| Mean ± SD DBP (mmHg) | 72.7 ± 10.3 | 73.8 ± 14.7 | 0.63 | |||
| Tilton, 2019 [28] | I-158 C-158 | 2001–2011 | Mean ± SD HbA1c (%) | 6 months: 7.39 | 6 months: 7.56 | 0.007 |
| 12 months: 7.49 | 12 months: 7.75 | 0.016 | ||||
| Mean ± SD SBP (mmHg) | 6 months: 135.3 | 6 months: 135.2 | 0.011 | |||
| 12 months: 133.0 | 12 months: 134.6 | 0.002 | ||||
| Mean ± SD DBP (mmHg) | 6 months: 72.8 | 6 months: 76.3 | 0.014 | |||
| 12 months: 72.2 | 12 months: 73.6 | 0.269 |
| Randomized Controlled Trials | ||||||||
|---|---|---|---|---|---|---|---|---|
| Author, Year | Randomization | Deviations from Intended Intervention | Missing Outcome Data | Measurement of Outcome | Selection of Reported Results | Overall | ||
| Hirsch, 2014 [21] | Low | Low | Some Concerns | Low | Low | Moderate | ||
| Planas, 2009 [22] | Low | Low | Low | Low | Low | Low | ||
| Cohort Studies | ||||||||
| Author, Year | Confounding | Selection of Participants | Classifications of Interventions | Deviations of Interventions | Missing Data | Measurement of Outcomes | Selection of Reported Results | Overall |
| Brummel, 2013 [23] | Moderate | Low | Low | Moderate | Moderate | Moderate | Low | Moderate |
| Fox, 2009 [24] | Moderate | Low | Low | Low | Moderate | Low | Low | Moderate |
| Pindolia, 2009 [25] | Moderate | Moderate | Moderate | Low | Low | Low | Low | Moderate |
| Prudencio, 2018 [26] | Moderate | Low | Low | Low | Low | Low | Low | Moderate |
| Skinner, 2015 [27] | Moderate | Moderate | Low | Moderate | Low | Low | Low | Moderate |
| Tilton, 2019 [28] | Moderate | Low | Low | Low | Low | Low | Low | Moderate |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marupuru, S.; Roether, A.; Guimond, A.J.; Stanley, C.; Pesqueira, T.; Axon, D.R. A Systematic Review of Clinical Outcomes from Pharmacist Provided Medication Therapy Management (MTM) among Patients with Diabetes, Hypertension, or Dyslipidemia. Healthcare 2022, 10, 1207. https://doi.org/10.3390/healthcare10071207
Marupuru S, Roether A, Guimond AJ, Stanley C, Pesqueira T, Axon DR. A Systematic Review of Clinical Outcomes from Pharmacist Provided Medication Therapy Management (MTM) among Patients with Diabetes, Hypertension, or Dyslipidemia. Healthcare. 2022; 10(7):1207. https://doi.org/10.3390/healthcare10071207
Chicago/Turabian StyleMarupuru, Srujitha, Alexis Roether, A. J. Guimond, Chris Stanley, Tyler Pesqueira, and David R. Axon. 2022. "A Systematic Review of Clinical Outcomes from Pharmacist Provided Medication Therapy Management (MTM) among Patients with Diabetes, Hypertension, or Dyslipidemia" Healthcare 10, no. 7: 1207. https://doi.org/10.3390/healthcare10071207
APA StyleMarupuru, S., Roether, A., Guimond, A. J., Stanley, C., Pesqueira, T., & Axon, D. R. (2022). A Systematic Review of Clinical Outcomes from Pharmacist Provided Medication Therapy Management (MTM) among Patients with Diabetes, Hypertension, or Dyslipidemia. Healthcare, 10(7), 1207. https://doi.org/10.3390/healthcare10071207