
Symptoms of Burnout Syndrome among Physicians during the Outbreak of COVID-19 Pandemic—A Systematic Literature Review





{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
- The inclusion criteria followed the PICOS approach [22]:
- The exclusion criteria used were (1) review articles and systematic review studies and (2) studies carried out before the COVID-19 pandemic.
- Population (P): studies that included physicians.
- Intervention (I): studies that analyzed the effects of MBIs and other scales on burnout in physicians.
- Comparison (C): studies that presented the pre- and post-test results of the Maslach Burnout Inventory.
- Outcomes (O): studies that measured the prevalence of burnout syndrome and factors associated with burnout.
- Study design (S): cross-sectional, observational, prospective, mixed-methods, and multicenter longitudinal descriptive studies.
2.3. Study Selection and Data Extraction
3. Results
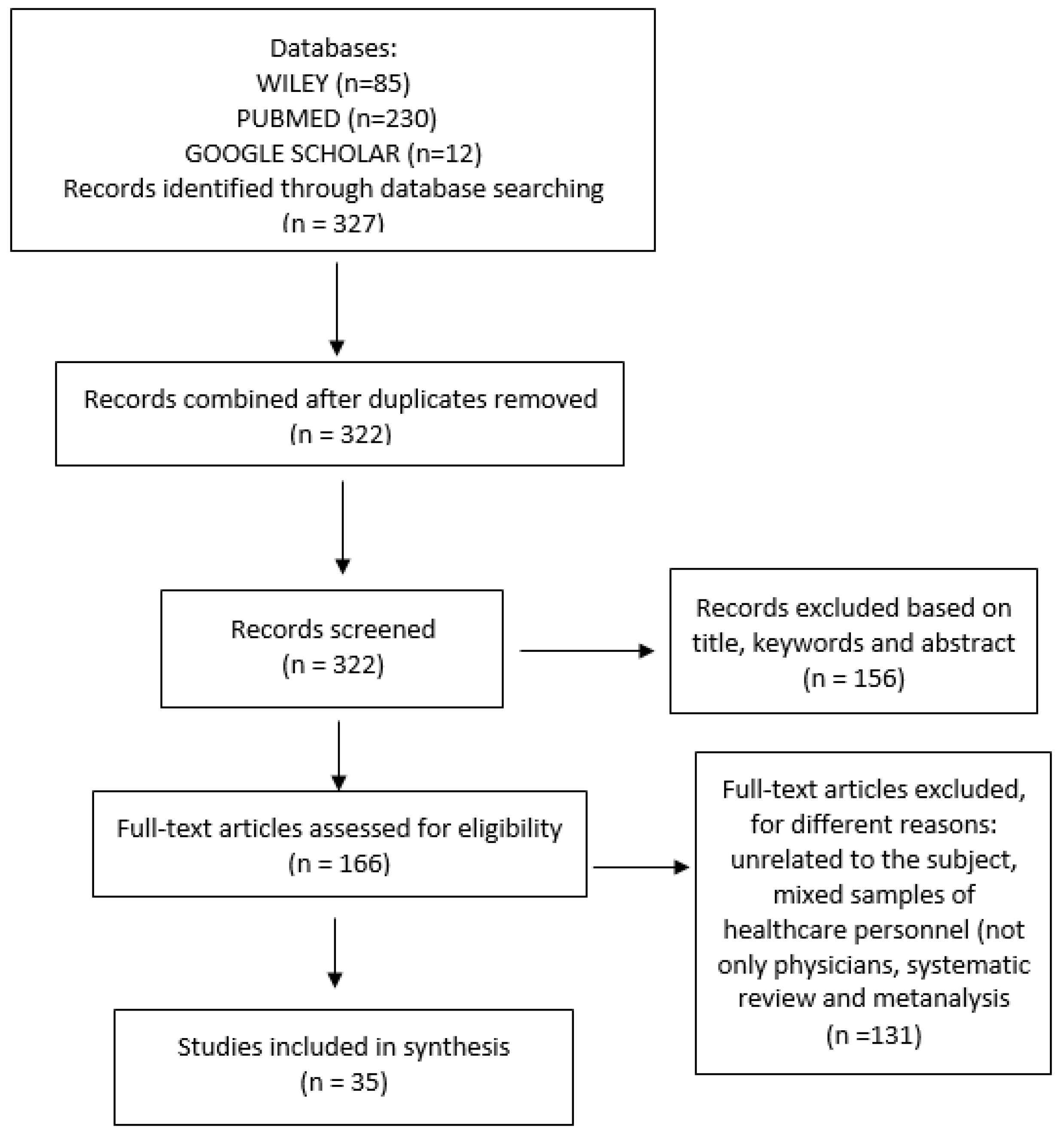
3.1. Study Selection
3.2. Study Characteristics
3.3. Burnout Instruments and Other Tools
3.4. Prevalence of Burnout Syndrome
3.5. Sociodemographic-, Familial-, and Financial-Related Factors
3.6. Institutional and Occupational Factors
3.7. Mental Health and Quality of Life
3.8. Depression, Anxiety, Stress, and Sleep Disorders
3.9. Professional Related Factors
- University teachers—PA was low among research assistants and in participants working in university research hospitals [34].
- Education and professional opportunities—High levels of burnout were identified in a study conducted among physicians in the USA [59]. Trainees in pathology or radiology had greater odds of concern for missed educational opportunities as compared to trainees in medicine.
4. Discussion
Reflections and Planning
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maslach, C.; Schaufeli, W.B.; Leiter, M.P. Job Burnout. Annu. Rev. Psychol. 2001, 52, 397–422. [Google Scholar] [CrossRef] [PubMed]
- Rabasa, B.; Figueiredo-Ferraz, U.V.H.; Gil-Monte, P.R.; Llorca-Pellicer, M. The Role of Guilt in the Relationship between Teacher’s Job Burnout Syndrome and the Inclination toward Absenteeism. J. Psychodidactics 2015, 21, 103–119. [Google Scholar] [CrossRef]
- Gil-Monte, P.R. Manual de Psicosociología Aplicada al Trabajo y a la Prevención de los Riesgos Laborales; Piramide: Giza, Egypt, 2014. [Google Scholar]
- Maslach, C. Finding solutions to the problem of burnout. Consult. Psychol. J. Pract. Res. 2017, 69, 143–152. [Google Scholar] [CrossRef]
- Iorga, M.; Muraru, I.; Hanganu, B.; Manoilescu, I.; Popa, A.; Ioan, B. Burnout, alexithymia and job satisfaction in autopsy technicians. Rom. J. Leg. Med. 2020, 28, 339–347. [Google Scholar] [CrossRef]
- Real-Ramirez, J.; Alberto Garcia-Bello, L.; Robles-Garcia, R.; Martinez, M.; Adame-Rivas, K.; Balderas-Pliego, M.; Garcia-Alfaro, C.; Perez-Cabanas, E.; Sierra-Medina, S.; Romero-Gonzalez, M.; et al. Well-being status and post-traumatic stress symptoms in health workers attending mindfulness sessions during the early stage of the COVID-19 epidemic in Mexico. Salud Ment. 2020, 43, 303–310. [Google Scholar] [CrossRef]
- Bodenheimer, T.; Sinsky, C. From Triple to Quadruple Aim: Care of the Patient Requires Care of the Provider. Ann. Fam. Med. 2014, 12, 573–576. [Google Scholar] [CrossRef]
- Magnavita, N.; Soave, P.M.; Antonelli, M. A one-year prospective study of work-related mental health in the intensivists of a COVID-19 hub hospital. Int. J. Environ. Res. Public Health 2021, 18, 9888. [Google Scholar] [CrossRef]
- Czabanowska, K.; Kuhlmann, E. Public health competences through the lens of the COVID-19 pandemic: What matters for health workforce preparedness for global health emergencies. Int. J. Health Plan. Manag. 2021, 36, 14–19. [Google Scholar] [CrossRef]
- Azzopardi-Muscat, N. A public health approach to health workforce policy development in Europe. Eur. J. Public Health 2020, 30 (Suppl. S4), iv3–iv4. [Google Scholar] [CrossRef]
- Iorga, M.; Soponaru, C.; Socolov, R.-V.; Cărăuleanu, A.; Socolov, D.-G. How the SARS-CoV-2 Pandemic Period Influenced the Health Status and Determined Changes in Professional Practice among Obstetrics and Gynecology Doctors in Romania. Medicina 2021, 57, 325. [Google Scholar] [CrossRef]
- Rose, D.M.; Seidler, A.; Nübling, M.; Latza, U.; Brähler, E.; Klein, E.M.; Wiltink, J.; Michal, M.; Nickels, S.; Wild, P.S.; et al. Associations of fatigue to work-related stress, mental and physical health in an employed community sample. BMC Psychiatry 2017, 17, 167. [Google Scholar] [CrossRef] [PubMed]
- Van der Colff, J.J.; Rothmann, S. Occupational stress, sense of coherence, coping, burnout and work engagement of registered nurses in South Africa. SA J. Ind. Psychol. 2009, 35, a423. [Google Scholar] [CrossRef]
- Ilić, I.; Arandjelović, M.; Jovanović, J.; Nešić, M. Relationships of work-related psychosocial risks, stress, individual factors and burnout—Questionnaire survey among emergency physicians and nurses. Med. Pracy 2017, 68, 167–168. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Giménez-Espert, M.D.C.; Prado-Gascó, V.; Soto-Rubio, A. Psychosocial Risks, Work Engagement, and Job Satisfaction of Nurses during COVID-19 Pandemic. Front. Public Health 2020, 8, 566896. [Google Scholar] [CrossRef] [PubMed]
- WHO CoronaVirus (COVID-19) Dashboard. 2021. Available online: https://covid19.who.int/?mapFilter=cases (accessed on 22 November 2021).
- Aafjes-van Doorn, K.; Békés, V.; Prout, T.A.; Hoffman, L. Psychotherapists’ Vicarious Traumatization during the COVID-19 Pandemic. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, S148. [Google Scholar] [CrossRef] [PubMed]
- Ghahramani, S.; Lankarani, K.B.; Yousefi, M.; Heydari, K.; Shahabi, S.; Azmand, S. A Systematic Review and Meta-Analysis of Burnout among Healthcare Workers during COVID-19. Front. Psychiatry 2021, 12, 758849. [Google Scholar] [CrossRef]
- Sharifi, M.; Asadi-Pooya, A.A.; Mousavi-Roknabadi, R.S. Burnout among Healthcare Providers of COVID-19; a Systematic Review of Epidemiology and Recommendations: Burnout in healthcare providers. Arch. Acad. Emerg. Med. 2020, 9, e7. [Google Scholar] [CrossRef]
- Silva, J.A.M.; Silva, L.E.O.; Araújo, Y.L.; de Bottacin, W.E.; Souza, T.T.; Reis, W.C.T. Prevalência de Burnout em profissionais de saúde no enfrentamento da COVID-19: Uma revisão sistemática. Res. Soc. Dev. 2021, 10, e167101623591. [Google Scholar] [CrossRef]
- Fiest, K.M.; Parsons Leigh, J.; Krewulak, K.D.; Plotnikoff, K.M.; Kemp, L.G.; Ng-Kamstra, J.; Stelfox, H.T. Experiences and management of physician psychological symptoms during infectious disease outbreaks: A rapid review. BMC Psychiatry 2021, 21, 91. [Google Scholar] [CrossRef]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef]
- Pines, A.M.; Aronson, E. Career Burnout; Free Press: New York, NY, USA, 1988. [Google Scholar]
- Malach-Pines, A. The Burnout Measure, Short Version. Int. J. Stress Manag. 2005, 12, 78–88. [Google Scholar] [CrossRef]
- Olson, K.; Sinsky, C.; Rinne, S.T.; Long, T.; Vender, R.; Mukherjee, S.; Bennick, M.; Linzer, M. Cross-sectional survey of workplace stressors associated with physician burnout measured by the Mini-Z and the Maslach Burnout Inventory. Stress Health 2019, 35, 157–175. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, T.S.; Borritz, M.; Villadsen, E.; Christensen, K.B. The Copenhagen burnout inventory: A new tool for the assessment of burnout. Work Stress 2005, 19, 192–207. [Google Scholar] [CrossRef]
- Trockel, M.; Bohman, B.; Lesure, E.; Hamidi, M.S.; Welle, D.; Roberts, L.; Shanafelt, T. A brief instrument to assess both burnout and professional fulfillment in physicians: Reliability and validity, including correlation with self-reported medical errors, in a sample of resident and practicing physicians. Acad. Psychiatry 2018, 42, 11–24. [Google Scholar] [CrossRef]
- Asghar, M.S.; Yasmin, F.; Alvi, H.; Shah, S.M.I.; Malhotra, K.; Farhan, S.A.; Ali Naqvi, S.A.; Yaseen, R.; Anwar, S.; Rasheed, U. Assessing the Mental Impact and Burnout among Physicians during the COVID-19 Pandemic: A Developing Country Single-Center Experience. Am. J. Trop. Med. Hyg. 2021, 104, 2185–2189. [Google Scholar] [CrossRef]
- Mendonça, V.S.; Steil, A.; Teixeira de Gois, A.F. COVID-19 pandemic in São Paulo: A quantitative study on clinical practice and mental health among medical residency specialties. Sao Paulo Med. J. 2021, 139, 489–495. [Google Scholar] [CrossRef]
- Yao, K.A.; Attai, D.; Bleicher, R.; Kuchta, K.; Moran, M.; Boughey, J.; Wilke, L.G.; Dietz, J.R.; Stevens, R.; Pesce, C.; et al. COVID-19 related oncologist’s concerns about breast cancer treatment delays and physician well-being (the CROWN study). Breast Cancer Res. Treat. 2021, 186, 625–635. [Google Scholar] [CrossRef]
- Kase, S.M.; Gribben, J.L.; Guttmann, K.F.; Waldman, E.D.; Weintraub, A.S. Compassion fatigue, burnout, and compassion satisfaction in pediatric subspecialists during the SARS-CoV-2 pandemic. Pediatr. Res. 2022, 91, 143–148. [Google Scholar] [CrossRef]
- Tzur Bitan, D.; Grossman-Giron, A.; Bloch, Y.; Mayer, Y.; Shiffman, N.; Mendlovic, S. Fear of COVID-19 scale: Psychometric characteristics, reliability and validity in the Israeli population. Psychiatry Res. 2020, 289, 113100. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Tuna, T.; Özdin, S. Levels and Predictors of Anxiety, Depression, and Burnout Syndrome in Physicians during the COVID-19 Pandemic. Int. J. Ment. Health Addict. 2021, 19, 2470–2483. [Google Scholar] [CrossRef] [PubMed]
- Lazarides, A.L.; Belay, E.S.; Anastasio, A.T.; Cook, C.E.; Anakwenze, O.A. Physician burnout and professional satisfaction in orthopedic surgeons during the COVID-19 Pandemic. Work 2021, 69, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Kim, B.; Jung, D.S.; Jung, S.I.; Oh, W.S.; Kim, S.-W.; Peck, K.R.; Chang, H.-H.; Diseases, T.K.S. Psychological distress among infectious disease physicians during the response to the COVID-19 outbreak in the Republic of Korea. BMC Public Health 2020, 20, 1811. [Google Scholar] [CrossRef] [PubMed]
- Alwashmi, A.H.; Alkhamees, A.A. Burnout and the Psychological Impact among Physiatrists in Saudi Arabia during COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 9621. [Google Scholar] [CrossRef]
- Doherty, A.M.; Colleran, G.C.; Durcan, L.; Irvine, A.D.; Barrett, E. A pilot study of burnout and long covid in senior specialist doctors. Ir. J. Med. Sci. 2022, 191, 133–137. [Google Scholar] [CrossRef]
- Nguyen, J.; Liu, A.; McKenney, M.; Liu, H.; Ang, D.; Elkbuli, A. Impacts and challenges of the COVID-19 pandemic on emergency medicine physicians in the United States. Am. J. Emerg. Med. 2021, 48, 38–47. [Google Scholar] [CrossRef]
- Civantos, A.M.; Bertelli, A.; Gonçalves, A.; Getzen, E.; Chang, C.; Long, Q.; Rajasekaran, K. Mental health among head and neck surgeons in Brazil during the COVID-19 pandemic: A national study. Am. J. Otolaryngol. 2020, 41, 102694. [Google Scholar] [CrossRef]
- Al-Humadi, S.; Bronson, B.; Muhlrad, S.; Paulus, M.; Hong, H.; Cáceda, R. Depression, Suicidal Thoughts, and Burnout among Physicians during the COVID-19 Pandemic: A Survey-Based Cross-Sectional Study. Acad. Psychiatry 2021, 45, 557–565. [Google Scholar] [CrossRef]
- Khan, N.; Palepu, A.; Dodek, P.; Salmon, A.; Leitch, H.; Ruzycki, S.; Townson, A.; Lacaille, D. Cross-sectional survey on physician burnout during the COVID-19 pandemic in Vancouver, Canada: The role of gender, ethnicity and sexual orientation. BMJ Open 2021, 11, e050380. [Google Scholar] [CrossRef]
- Vila, R.C.B.; Burgos, L.M.; Sigal, A.; Costabel, J.P.; de Lima, A.A. Burnout syndrome in cardiology residents. Impact of the COVID-19 pandemic on burnout syndrome in cardiology residents. Curr. Probl. Cardiol. 2022, 47, 100873. [Google Scholar] [CrossRef]
- Macía-Rodríguez, C.; Alejandre de Oña, Á.; Martín-Iglesias, D.; Barrera-López, L.; Pérez-Sanz, M.T.; Moreno-Diaz, J.; González-Munera, A. Burn-out syndrome in Spanish internists during the COVID-19 outbreak and associated factors: A cross-sectional survey. BMJ Open 2021, 11, e042966. [Google Scholar] [CrossRef] [PubMed]
- Abdelhafiz, A.S.; Ali, A.; Ziady, H.H.; Maaly, A.M.; Alorabi, M.; Sultan, E.A. Prevalence, associated factors, and consequences of burnout among Egyptian physicians during COVID-19 pandemic. Front. Public Health 2020, 8, 590190. [Google Scholar] [CrossRef] [PubMed]
- De Paiva Faria, A.R.Q.; Coelho, H.F.C.; Silva, A.B.; Damascena, L.C.L.; Carneiro, R.R.; Lopes, M.T.; Araújo, K.D.T.; Lima, C.M.B.L. Impact of the COVID-19 pandemic on the development of burnout syndrome in frontline physicians: Prevalence and associated factors. Rev. Assoc. Méd. Bras. 2021, 67, 942–949. [Google Scholar] [CrossRef]
- Khalafallah, A.M.; Lam, S.; Gami, A.; Dornbos, D.L.; Sivakumar, W.; Johnson, J.N.; Mukherjee, D. Burnout and career satisfaction among attending neurosurgeons during the COVID-19 pandemic. Clin. Neurol. Neurosurg. 2020, 198, 106193. [Google Scholar] [CrossRef]
- Alrawashdeh, H.M.; Al-Tammemi, A.A.B.; Alzawahreh, M.K.; Al-Tamimi, A.; Elkholy, M.; Al Sarireh, F.; Abusamak, M.; Elehamer, N.M.K.; Malkawi, A.; Al-Dolat, W.; et al. Occupational burnout and job satisfaction among physicians in times of COVID-19 crisis: A convergent parallel mixed-method study. BMC Public Health 2021, 21, 811–829. [Google Scholar] [CrossRef] [PubMed]
- Baptista, S.; Teixeira, A.; Castro, L.; Cunha, M.; Serrão, C.; Rodrigues, A.; Duarte, I. Physician Burnout in Primary Care during the COVID-19 Pandemic: A Cross-Sectional Study in Portugal. J. Prim. Care Community Health 2021, 12, 1–8. [Google Scholar] [CrossRef]
- Buran, F.; Altın, Z. Burnout among physicians working in a pandemic hospital during the COVID-19 pandemic. Leg. Med. 2021, 5, 101881. [Google Scholar] [CrossRef]
- Kannampallil, T.G.; Goss, C.W.; Evanoff, B.A.; Strickland, J.R.; McAlister, R.P.; Duncan, J. Exposure to COVID-19 patients increases physician trainee stress and burnout. PLoS ONE 2020, 15, e0237301. [Google Scholar] [CrossRef]
- Dinibutun, S.R. Factors Associated with Burnout Among Physicians: An Evaluation during a Period of COVID-19 Pandemic. J. Healthc. Leadersh. 2020, 12, 85–94. [Google Scholar] [CrossRef]
- Guercovich, A.; Piazzioni, G.; Waisberg, F.; Mandó, P.; Angel, M. Burn-out syndrome in medical oncologists during the COVID-19 pandemic: Argentinian national survey. E Cancer Med. Sci. 2021, 15, 1213. [Google Scholar] [CrossRef]
- Jha, S.; Shah, S.; Calderon, M.D.; Soin, A.; Manchikanti, L. The effect of COVID-19 on interventional pain management practices: A physician burnout survey. Pain Physician 2020, 23, 271–282. [Google Scholar]
- De Wit, K.; Mercuri, M.; Wallner, C.; Clayton, N.; Archambault, P.; Ritchie, K.; Gérin-Lajoie, C.; Gray, S.; Schwartz, L.; Chan, T.; et al. Canadian emergency physician psychological distress and burnout during the first 10 weeks of COVID-19: A mixed-methods study. J. Am. Coll. Emerg. Physicians Open 2020, 1, 1030–1038. [Google Scholar] [CrossRef] [PubMed]
- Appiani, F.J.; Cairoli, F.R.; Sarotto, L.; Yaryour, C.; Basile, M.E.; Duarte, J.M. Prevalence of stress, burnout syndrome, anxiety and depression among physicians of a teaching hospital during the COVID-19 pandemic. Arch. Argent. Pediatr. 2021, 119, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Ofei-Dodoo, S.; Loo-Gross, C.; Kellerman, R. Burnout, Depression, Anxiety, and Stress among Family Physicians in Kansas Responding to the COVID-19 Pandemic. J. Am. Board Fam. Med. 2021, 34, 522–530. [Google Scholar] [CrossRef] [PubMed]
- Cravero, A.L.; Kim, N.J.; Feld, L.D.; Berry, K.; Rabiee, A.; Bazarbashi, N.; Bassin, S.; Lee, T.-H.; Moon, A.M.; Qi, X.; et al. Impact of exposure to patients with COVID-19 on residents and fellows: An international survey of 1420 trainees. Postgrad. Med. J. 2021, 97, 706–715. [Google Scholar] [CrossRef] [PubMed]
- Lou, S.S.; Goss, C.W.; Evanoff, B.A.; Duncan, J.G.; Kannampallil, T. Risk factors associated with physician trainee concern over missed educational opportunities during the COVID-19 pandemic. BMC Med. Educ. 2021, 21, 216. [Google Scholar] [CrossRef]
- Rodriguez, R.M.; Montoy, J.C.C.; Hoth, K.F.; Talan, D.A.; Harland, K.K.; Eyck, P.T.; Mower, W.; Krishnadasan, A.; Santibanez, S.; Mohr, N.; et al. Symptoms of anxiety, burnout, and PTSD and the mitigation effect of serologic testing in emergency department personnel during the COVID-19 pandemic. Ann. Emerg. Med. 2021, 78, 35–43. [Google Scholar] [CrossRef]
- Chalhub, R.Á.; Menezes, M.S.; Aguiar, C.V.N.; Santos-Lins, L.S.; Martins Netto, E.; Brites, C.; Lins-Kusterer, L. Anxiety, health-related quality of life, and symptoms of burnout in frontline physicians during the COVID-19 pandemic. Braz. J. Infect. Dis. 2021, 25, 101618. [Google Scholar] [CrossRef]
- Abdelghani, M.; El-Gohary, H.M.; Fouad, E.; Hassan, M.S. Addressing the relationship between perceived fear of COVID-19 virus infection and emergence of burnout symptoms in a sample of Egyptian physicians during COVID-19 pandemic: A cross-sectional study. Middle East Curr. Psychiatry 2020, 27, 70. [Google Scholar] [CrossRef]
- Civantos, A.M.; Byrnes, Y.; Chang, C.; Prasad, A.; Chorath, K.; Poonia, S.K.; Jenks, C.M.; Bur, A.M.; Thakkar, P.; Graboyes, E.M.; et al. Mental health among otolaryngology resident and attending physicians during the COVID-19 pandemic: National study. Head Neck 2020, 42, 1597–1609. [Google Scholar] [CrossRef]
- Seda-Gombau, G.; Montero-Alía, J.J.; Moreno-Gabriel, E.; Torán-Monserrat, P. Impact of the COVID-19 Pandemic on Burnout in Primary Care Physicians in Catalonia. Int. J. Environ. Res. Public Health 2021, 18, 9031. [Google Scholar] [CrossRef] [PubMed]
- Miller, C. What Is the Price of Physician Stress and Burnout? Available online: http://www.medicaleconomics.com/medical-economics/news/what-price-physician-stress-and-burnout (accessed on 1 March 2022).
- Drummond, D. Physician Burnout: Its Origin, Symptoms, and Five Main Causes. Fam. Pract. Manag. 2015, 22, 42–47. [Google Scholar] [PubMed]
- Southwick, F.S.; Southwick, S.M. The Loss of a Sense of Control as a Major Contributor to Physician Burnout: A Neuropsychiatric Pathway to Prevention and Recovery. JAMA Psychiatry 2018, 75, 665–666. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.S.; Bachu, R.; Adikey, A.; Malik, M.; Shah, M. Factors related to physician burnout and its consequences: A review. Behav. Sci. 2018, 8, 98. [Google Scholar] [CrossRef] [PubMed]
- Iurcov, R.; Pop, L.M.; Ciavoi, G.; Iorga, M. Evaluating the Practice of Preventive Behaviors and the Fear of COVID-19 among Dentists in Oradea Metropolitan Area after the First Wave of Pandemic; a Cross-Sectional Study. Healthcare 2021, 9, 443. [Google Scholar] [CrossRef]
- Van Dam, A. Subgroup analysis in burnout: Relations between fatigue, anxiety, and depression. Front. Psychol. 2016, 7, 90. [Google Scholar] [CrossRef]
- Zhou, J.; Yang, Y.; Qiu, X.; Yang, X.; Pan, H.; Ban, B.; Qiao, Z.; Wang, L.; Wang, W. Relationship between anxiety and burnout among Chinese physicians: A moderated mediation model. PLoS ONE 2016, 11, e0157013. [Google Scholar] [CrossRef]
- Pereira-Lima, K.; Loureiro, S.R. Burnout, anxiety, depression, and social skills in medical residents. Psychol. Health Med. 2015, 20, 353–362. [Google Scholar] [CrossRef]
- Gallego-Alberto, L.; Losada, A.; Vara, C.; Olazarán, J.; Muñiz, R.; Pillemer, K. Psychosocial predictors of anxiety in nursing home staff. Clin. Gerontol. 2018, 41, 282–289. [Google Scholar] [CrossRef]
- Glasberg, A.L.; Eriksson, S.; Norberg, A. Burnout and ‘stress of conscience’ among healthcare personnel. J. Adv. Nurs. 2007, 57, 392–2403. [Google Scholar] [CrossRef]
- Suñer-Soler, R.; Grau-Martín, A.; Font-Mayolas, S.; Gras, M.E.; Bertran, C.; Sullman, M.J. Burnout and quality of life among Spanish healthcare personnel. J. Psychiatr. Ment. Health Nurs. 2013, 20, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Lluch, C.; Galiana, L.; Doménech, P.; Sansó, N. The Impact of the COVID-19 Pandemic on Burnout, Compassion Fatigue, and Compassion Satisfaction in Healthcare Personnel: A Systematic Review of the Literature Published during the First Year of the Pandemic. Healthcare 2022, 10, 364. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Claponea, R.M.; Pop, L.M.; Iorga, M.; Iurcov, R. Symptoms of Burnout Syndrome among Physicians during the Outbreak of COVID-19 Pandemic—A Systematic Literature Review. Healthcare 2022, 10, 979. https://doi.org/10.3390/healthcare10060979
Claponea RM, Pop LM, Iorga M, Iurcov R. Symptoms of Burnout Syndrome among Physicians during the Outbreak of COVID-19 Pandemic—A Systematic Literature Review. Healthcare. 2022; 10(6):979. https://doi.org/10.3390/healthcare10060979
Chicago/Turabian StyleClaponea, Roxana Mihaela, Lavinia Maria Pop, Magdalena Iorga, and Raluca Iurcov. 2022. "Symptoms of Burnout Syndrome among Physicians during the Outbreak of COVID-19 Pandemic—A Systematic Literature Review" Healthcare 10, no. 6: 979. https://doi.org/10.3390/healthcare10060979
APA StyleClaponea, R. M., Pop, L. M., Iorga, M., & Iurcov, R. (2022). Symptoms of Burnout Syndrome among Physicians during the Outbreak of COVID-19 Pandemic—A Systematic Literature Review. Healthcare, 10(6), 979. https://doi.org/10.3390/healthcare10060979