
A Psychometric Analysis of the Nurse Satisfaction with the Quality of Care Scale



Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Sample and Setting
2.3. Inclusion/Exclusion Criteria
2.4. Instrumentation
2.5. Analysis
2.6. Ethical Approval
3. Results
3.1. Sample Characteristics
3.2. Descriptive Statistics
3.3. Exploratory Factor Analysis
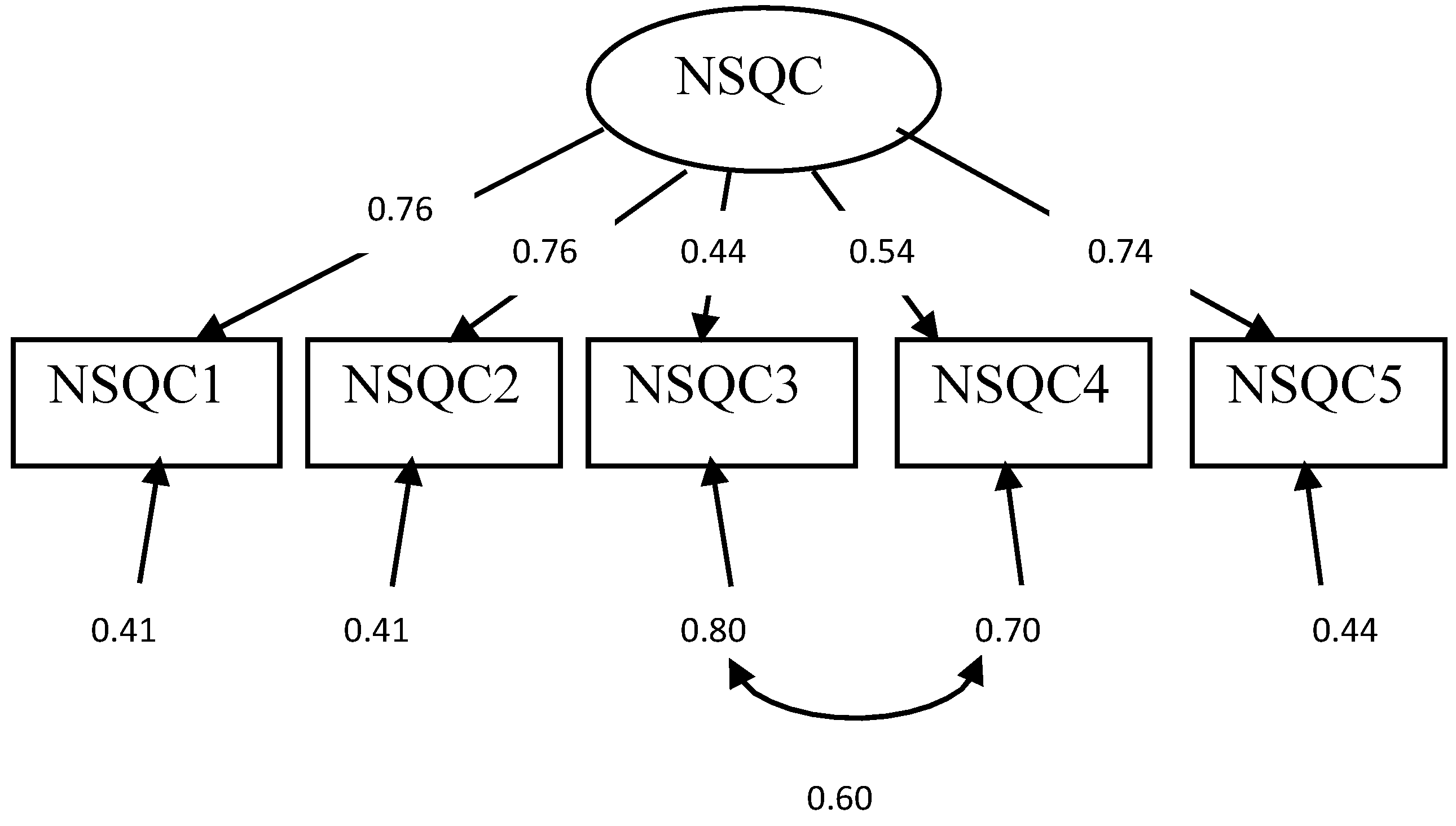
3.4. Confirmatory Factor Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Spence Laschinger, H.K.; Zhu, J.; Read, E. New nurses’ perceptions of professional practice behaviours, quality of care, job satisfaction and career retention. J. Nurs. Manag. 2016, 24, 656–665. [Google Scholar] [CrossRef] [PubMed]
- McHugh, M.D.; Stimpfel, A.W. Nurse reported quality of care: A measure of hospital quality. Res. Nurs. Health 2012, 35, 566–575. [Google Scholar] [CrossRef]
- Grujic, S.D.; O’Sullivan, D.D.; Wehrmacher, W.H. Organizational control of hospital infrastructure determines the quality of care. Qual. Assur. Util. Rev. 1989, 4, 19–24. [Google Scholar] [CrossRef]
- Mudallal, R.H.; Saleh, M.Y.; Al-Modallal, H.M.; Abdel-Rahman, R.Y. Quality of nursing care: The influence of work conditions and burnout. Int. J. Afr. Nurs. Sci. 2017, 7, 24–30. [Google Scholar] [CrossRef]
- Liu, Y.; Aungsuroch, Y. Factors influencing nurse-assessed quality nursing care: A cross-sectional study in hospitals. J. Adv. Nurs. 2018, 74, 935–945. [Google Scholar] [CrossRef] [PubMed]
- Burhans, L.M.; Alligood, M.R. Quality nursing care in the words of nurses. J. Adv. Nurs. 2010, 66, 1689–1697. [Google Scholar] [CrossRef] [PubMed]
- Nobahar, M. Exploring experiences of the quality of nursing care among patients, nurses, caregivers and physicians in a haemodialysis department. J. Ren. Care 2017, 43, 50–59. [Google Scholar] [CrossRef]
- Aiken, L.H.; Sermeus, W.; Van den Heede, K.; Sloane, D.M.; Busse, R.; McKee, M.; Bruyneel, L.; Rafferty, A.M.; Griffiths, P.; Moreno-Casbas, M.T.; et al. Patient safety, satisfaction, and quality of hospital care: Cross sectional surveys of nurses and patients in 12 countries in Europe and the United States. BMJ 2012, 20, 344. [Google Scholar] [CrossRef] [Green Version]
- Rojas Russell, M.; Tirado Gómez, L.L.; Pacheco Domínguez, R.L.; Escamilla Santiago, R.; López Cervantes, M. Work climate in Mexican hemodialysis units: A cross-sectional study. Nefrología 2011, 1, 76–83. [Google Scholar] [CrossRef]
- Aiken, L.H.; Clarke, S.P.; Sloane, D.M. International Hospital Outcomes Research Consortium. Hospital staffing, organization, and quality of care: Cross-national findings. Int. J. Qual. Health Care 2002, 1, 5–14. [Google Scholar] [CrossRef] [Green Version]
- Phillips, J.M.; Mossop, P.; Bartol, C.; Hodgson, B. When medical devices fail: Lessons learned in a hemodialysis unit. CANNT J. 2015, 1, 36–39. [Google Scholar]
- Laschinger, H.K. Job and career satisfaction and turnover intentions of newly graduated nurses. J. Nurs. Manag. 2012, 20, 472–484. [Google Scholar] [CrossRef] [PubMed]
- Laschinger, H.K.; Fida, R. Linking nurses’ perceptions of patient care quality to job satisfaction. J. Nurs. Adm. 2015, 1, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.W.; You, L.M.; Zheng, J.; Liu, K.E.; Fang, J.B.; Hou, S.X.; Lu, M.M.; Lv, A.L.; Ma, W.G.; Wang, H.H.; et al. Nurse staffing levels make a difference on patient outcomes: A multisite study in Chinese hospitals. J. Nurs. Scholarsh. 2012, 44, 266–273. [Google Scholar] [CrossRef]
- Freitas, J.S.; Silva, A.E.; Minamisava, R.; Bezerra, A.L.; Sousa, M.R. Quality of nursing care and satisfaction of patients attended at a teaching hospital. Rev. Lat.-Am. Enferm. 2014, 22, 454–460. [Google Scholar] [CrossRef] [Green Version]
- Kalisch, B.J.; Tschannen, D.; Lee, K.H. Do staffing levels predict missed nursing care? Int. J. Qual. Health Care 2011, 1, 302–308. [Google Scholar] [CrossRef] [Green Version]
- Van Bogaert, P.; van Heusden, D.; Timmermans, O.; Franck, E. Nurse work engagement impacts job outcome and nurse-assessed quality of care: Model testing with nurse practice environment and nurse work characteristics as predictors. Front. Psychol. 2014, 5, 1261. [Google Scholar] [CrossRef] [Green Version]
- Andrews, D.R.; Burr, J.; Bushy, A. Nurses’ self-concept and perceived quality of care: A narrative analysis. J. Nurs. Care Qual. 2011, 1, 69–77. [Google Scholar] [CrossRef]
- Baernholdt, M.; Jennings, B.M.; Lewis, E.J. A pilot study of staff nurses’ perceptions of factors that influence quality of care in critical access hospitals. J. Nurs. Care Qual. 2013, 28, 352. [Google Scholar] [CrossRef]
- Disch, J.O. From the Guest Editor: Creating Healthy Work Environments. Creat Nurs. 2002, 1, 3–4. [Google Scholar] [CrossRef]
- Walker, A. Nursing Satisfaction Impacts Patient Outcomes, Mortality. Nurse.org. 2018, Volume 2. Available online: https://nurse.org/articles/nursing-satisfaction-patient-results/ (accessed on 20 June 2020).
- Karaca, A.; Durna, Z. Patient satisfaction with the quality of nursing care. Nurs Open 2019, 6, 535–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kvist, T.; Voutilainen, A.; Mäntynen, R.; Vehviläinen-Julkunen, K. The relationship between patients’ perceptions of care quality and three factors: Nursing staff job satisfaction, organizational characteristics and patient age. BMC Health Serv. Res. 2014, 14, 466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- SPSS Inc.; IBM Corp. Released, Statistics for Windows, version 25.0; IBM Corp.: Armonk, NY, USA, 2017.
- Muthén, L.; Muthén, B. Mplus User’s Guide, 8th ed.; Computer Software Manual: Los Angeles, CA, USA, 2017. [Google Scholar]
- Byrne, B.M. A Primer of LISREL: Basic Applications and Programming for Confirmatory Factor Analytic Models; Springer Science & Business Media: New York, NY, USA, 2012. [Google Scholar]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E.; Tatham, R.L. Multivariate Data Analysis: A Global Perspective, 7th ed.; Pearson Education, Upper Saddle Rider: London, UK, 2010. [Google Scholar]
- Brown, T.A. Confirmatory Factor Analysis for Applied Research; Guilford Publications: New York, NY, USA, 2015. [Google Scholar]
- Pahlavanzadeh, S.; Asgari, Z.; Alimohammadi, N. Effects of stress management program on the quality of nursing care and intensive care unit nurses. Iran. J. Nurs. Midwifery Res. 2016, 21, 213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aiken, L.H.; Sloane, D.M.; Bruyneel, L.; Van den Heede, K.; Sermeus, W. Nurses’ reports of working conditions and hospital quality of care in 12 countries in Europe. Int. J. Nurs. Stud. 2013, 1, 143–153. [Google Scholar] [CrossRef]
- Alharbi, M.F.; Alahmadi, B.A.; Alali, M.; Alsaedi, S. Quality of nursing work life among hospital nurses in Saudi Arabia: A cross-sectional study. J. Nurs. Manag. 2019, 27, 1722–1730. [Google Scholar] [CrossRef]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics; Allyn and Bacon: Boston, MA, USA, 2007. [Google Scholar]
- Aron, S. Relationship between Nurses’ Job Satisfaction and Quality of Healthcare They Deliver; Minnesota State University: Mankato, MN, USA, 2015. [Google Scholar]
- Fitzpatrick, J.J. The international nursing focus on mental health. Arch. Psychiatr. Nurs. 2017, 1, 31–329. [Google Scholar] [CrossRef]
- Bennett, P.N. Technological intimacy in haemodialysis nursing. Nurs. Inq. 2011, 18, 247–252. [Google Scholar] [CrossRef]
- Aiken, L.H.; Sloane, D.M.; Clarke, S.; Poghosyan, L.; Cho, E.; You, L.; Finlayson, M.; Kanai-Pak, M.; Aungsuroch, Y. Importance of work environments on hospital outcomes in nine countries. Int. J. Qual. Health Care 2011, 1, 357–364. [Google Scholar] [CrossRef] [Green Version]
- Van Bogaert, P.; Clarke, S.; Roelant, E.; Meulemans, H.; Van de Heyning, P. Impacts of unit-level nurse practice environment and burnout on nurse-reported outcomes: A multilevel modelling approach. J. Clin. Nurs. 2010, 19, 1664–1674. [Google Scholar] [CrossRef]
- Tervo-Heikkinen, T.; Kvist, T.; Partanen, P.; Vehviläinen-Julkunen, K.; Aalto, P. Patient satisfaction as a positive nursing outcome. J. Nurs. Care Qual. 2008, 1, 58–65. [Google Scholar] [CrossRef]
- Charalambous, A.; Beadsmoore, A. Quality nursing care: A selective review of the literature of patients’ and nurses’ interpretations. Sci. J. Hell Regul. Body Nurses 2009, 2, 75–82. [Google Scholar]


{kind=link}
{kind=link}
| Items | Mean | Std. Deviation | N | Skewness | Kurtosis |
|---|---|---|---|---|---|
| 3.76 | 0.84 | 200 | −1.08 | 1.94 |
| 3.64 | 0.85 | 200 | −0.77 | 0.93 |
| 2.75 | 1.19 | 200 | 0.07 | −1.00 |
| 3.04 | 1.03 | 200 | −0.10 | −0.63 |
| 3.51 | 0.94 | 200 | −0.62 | 0.53 |
| Model | Summary of Modifications | χ2 (df) | p | RMSEA | CFI | SRMR |
|---|---|---|---|---|---|---|
| Original | N/A | 89.96 (5) | 0.001 | 0.29 CI: 0.24–0.34 | 0.77 | 0.08 |
| Modification 1 | Allowing the correlation of errors between the residuals of items 3 and 4 | 9.92 (4) | 0.04 | 0.08 CI: 0.01–0.15 | 0.98 | 0.02 |
| Observed Variables | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| 1. NSQC 1 | _ | _ | _ | _ | _ |
| 2. NSQC 2 | 0.58 ** | _ | _ | _ | _ |
| 3. NSQC 3 | 0.34 ** | 0.34 ** | _ | _ | _ |
| 4. NSQC 4 | 0.41 ** | 0.41 ** | 0.70 ** | _ | _ |
| 5. NSQC 5 | 0.56 ** | 0.57 ** | 0.33 ** | 0.40 ** | _ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alilyyani, B.; Kerr, M.; Wong, C.; Wazqar, D. A Psychometric Analysis of the Nurse Satisfaction with the Quality of Care Scale. Healthcare 2022, 10, 1145. https://doi.org/10.3390/healthcare10061145
Alilyyani B, Kerr M, Wong C, Wazqar D. A Psychometric Analysis of the Nurse Satisfaction with the Quality of Care Scale. Healthcare. 2022; 10(6):1145. https://doi.org/10.3390/healthcare10061145
Chicago/Turabian StyleAlilyyani, Bayan, Michael Kerr, Carol Wong, and Dhuha Wazqar. 2022. "A Psychometric Analysis of the Nurse Satisfaction with the Quality of Care Scale" Healthcare 10, no. 6: 1145. https://doi.org/10.3390/healthcare10061145
APA StyleAlilyyani, B., Kerr, M., Wong, C., & Wazqar, D. (2022). A Psychometric Analysis of the Nurse Satisfaction with the Quality of Care Scale. Healthcare, 10(6), 1145. https://doi.org/10.3390/healthcare10061145