
The Effects of Prior Mammography Screening on the Performance of Breast Cancer Detection in Taiwan

 , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
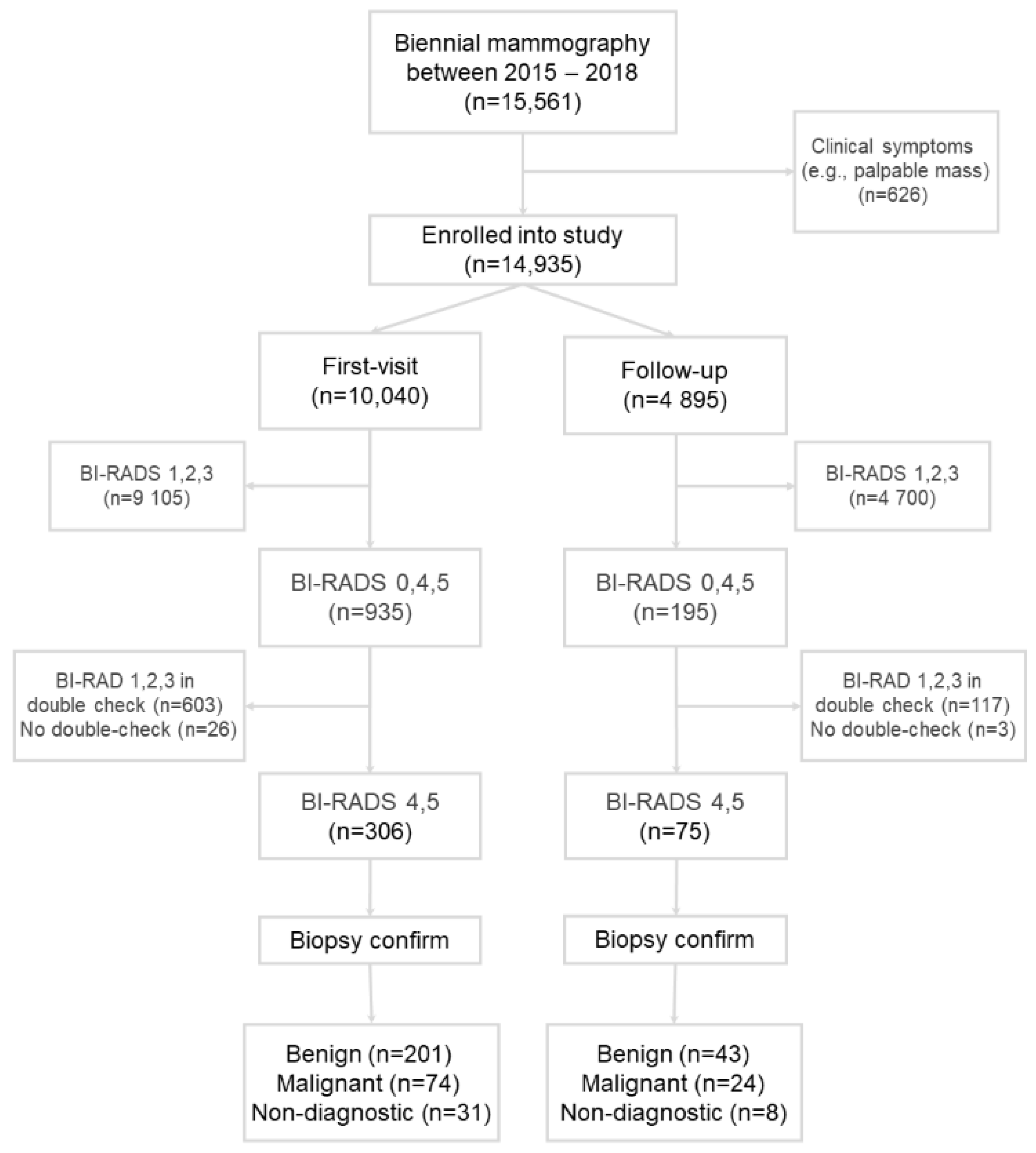
2.1. Screening Population
2.2. Mammography Imaging
2.3. Screening
2.4. Statistical Analysis
3. Results
3.1. Patient Demographics
3.2. Positive and Negative Results
3.3. Biopsy and Pathological Confirmation
3.4. Performance of Mammography Screening
3.4.1. Recall Rate
3.4.2. CDR
3.4.3. PPV
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics, 2017. CA Cancer J. Clin. 2017, 67, 7–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schnitt, S.J. Classification and prognosis of invasive breast cancer: From morphology to molecular taxonomy. Mod. Pathol. 2010, 23 (Suppl. S2), S60–S64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azamjah, N.; Soltan-Zadeh, Y.; Zayeri, F. Global Trend of Breast Cancer Mortality Rate: A 25-Year Study. Asian Pac. J. Cancer Prev. 2019, 20, 2015–2020. [Google Scholar] [CrossRef]
- Su, S.Y. Nationwide mammographic screening and breast cancer mortality in Taiwan: An interrupted time-series analysis. Breast Cancer 2022, 29, 336–342. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.A.; Duffy, S.W.; Gabe, R.; Tabar, L.; Yen, A.M.F.; Chen, T.H.H. The randomized trials of breast cancer screening: What have we learned? Radiol. Clin. North Am. 2004, 42, 793–806. [Google Scholar] [CrossRef] [PubMed]
- Tabár, L.; Yen, A.M.; Wu, W.Y.; Chen, S.L.; Chiu, S.Y.; Fann, J.C.; Ku, M.M.; Smith, R.A.; Duffy, S.W.; Chen, T.H. Insights from the Breast Cancer Screening Trials: How Screening Affects the Natural History of Breast Cancer and Implications for Evaluating Service Screening Programs. Breast J. 2015, 21, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Oeffinger, K.C.; Fontham, E.T.; Etzioni, R.; Herzig, A.; Michaelson, J.S.; Shih, Y.C.; Walter, L.C.; Church, T.R.; Flowers, C.R.; LaMonte, S.J.; et al. Breast Cancer Screening for Women at Average Risk: 2015 Guideline Update from the American Cancer Society. JAMA 2015, 314, 1599–1614. [Google Scholar] [CrossRef]
- Shapiro, S. Periodic Screening for Breast Cancer: The HIP Randomized Controlled Trial. J. Natl. Cancer Inst. Monogr. 1997, 1997, 27–30. [Google Scholar] [CrossRef]
- Nyström, L.; Andersson, I.; Bjurstam, N.; Frisell, J.; Nordenskjöld, B.; Rutqvist, L.E. Long-term effects of mammography screening: Updated overview of the Swedish randomised trials. Lancet 2002, 359, 909–919. [Google Scholar] [CrossRef]
- Tabár, L.; Vitak, B.; Chen, T.H.-H.; Yen, A.M.-F.; Cohen, A.; Tot, T.; Chiu, S.Y.-H.; Chen, S.L.-S.; Fann, J.C.-Y.; Rosell, J.; et al. Swedish Two-County Trial: Impact of Mammographic Screening on Breast Cancer Mortality during 3 Decades. Radiology 2011, 260, 658–663. [Google Scholar] [CrossRef] [Green Version]
- Alexander, F.E.; Anderson, T.J.; Brown, H.K.; Forrest, A.P.; Hepburn, W.; Kirkpatrick, A.E.; Muir, B.B.; Prescott, R.J.; Smith, A. 14 years of follow-up from the Edinburgh randomised trial of breast-cancer screening. Lancet 1999, 353, 1903–1908. [Google Scholar] [CrossRef]
- Broeders, M.; Moss, S.; Nyström, L.; Njor, S.; Jonsson, H.; Paap, E.; Massat, N.; Duffy, S.; Lynge, E.; Paci, E.; et al. The impact of mammographic screening on breast cancer mortality in Europe: A review of observational studies. J. Med. Screen. 2012, 19 (Suppl. 1), 14–25. [Google Scholar] [CrossRef] [PubMed]
- Coldman, A.; Phillips, N.; Wilson, C.; Decker, K.; Chiarelli, A.M.; Brisson, J.; Zhang, B.; Payne, J.; Doyle, G.; Ahmad, R. Pan-Canadian study of mammography screening and mortality from breast cancer. J. Natl. Cancer Inst. 2014, 106, dju261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niell, B.L.; Freer, P.E.; Weinfurtner, R.J.; Arleo, E.K.; Drukteinis, J.S. Screening for Breast Cancer. Radiol. Clin. North Am. 2017, 55, 1145–1162. [Google Scholar] [CrossRef] [PubMed]
- Tabàr, L.; Fagerberg, G.; Duffy, S.W.; Day, N.E.; Gad, A.; Gröntoft, O. Update of the Swedish two-county program of mammographic screening for breast cancer. Radiol. Clin. North Am. 1992, 30, 187–210. [Google Scholar]
- Verbeek, A.L. Mammographic screening: Keeping women alive. Womens Health 2011, 7, 631–633. [Google Scholar]
- Hubbard, R.A.; Kerlikowske, K.; Flowers, C.I.; Yankaskas, B.C.; Zhu, W.; Miglioretti, D.L. Cumulative Probability of False-Positive Recall or Biopsy Recommendation after 10 Years of Screening Mammography. Ann. Intern. Med. 2011, 155, 481–492. [Google Scholar] [CrossRef]
- Harada-Shoji, N.; Suzuki, A.; Ishida, T.; Zheng, Y.F.; Narikawa-Shiono, Y.; Sato-Tadano, A.; Ohta, R.; Ohuchi, N. Evaluation of Adjunctive Ultrasonography for Breast Cancer Detection Among Women Aged 40–49 Years with Varying Breast Density Undergoing Screening Mammography: A Secondary Analysis of a Randomized Clinical Trial. JAMA Netw. Open 2021, 4, e2121505. [Google Scholar] [CrossRef]
- Hendrick, R.E.; Helvie, M.A. United States Preventive Services Task Force screening mammography recommendations: Science ignored. Am. J. Roentgenol. 2011, 196, W112–W116. [Google Scholar] [CrossRef] [Green Version]
- Kerlikowske, K.; Zhu, W.; Hubbard, R.A.; Geller, B.; Dittus, K.; Braithwaite, D.; Wernli, K.J.; Miglioretti, D.L.; O’Meara, E.S.; Breast Cancer Surveillance Consortium. Outcomes of Screening Mammography by Frequency, Breast Density, and Postmenopausal Hormone Therapy. JAMA Intern. Med. 2013, 173, 807–816. [Google Scholar] [CrossRef] [Green Version]
- Tosteson, A.N.; Fryback, D.G.; Hammond, C.S.; Hanna, L.G.; Grove, M.R.; Brown, M.; Wang, Q.; Lindfors, K.; Pisano, E.D. Consequences of false-positive screening mammograms. JAMA Intern. Med. 2014, 174, 954–961. [Google Scholar] [CrossRef] [PubMed]
- Schell, M.J.; Yankaskas, B.C.; Ballard-Barbash, R.; Qaqish, B.F.; Barlow, W.E.; Rosenberg, R.D.; Smith-Bindman, R. Evidence-based target recall rates for screening mammography. Radiology 2007, 243, 681–689. [Google Scholar] [CrossRef] [Green Version]
- D’Orsi, C.J.; Sickles, E.A.; Mendelson, E.B.; Morris, E.A. ACR BI-RADS Atlas, Breast Imaging Reporting and Data System; American College of Radiology: Reston, VA, USA, 2013. [Google Scholar]
- Lee, C.S.; Bhargavan-Chatfield, M.; Burnside, E.S.; Nagy, P.; Sickles, E.A. The National Mammography Database: Preliminary Data. Am. J. Roentgenol. 2016, 206, 883–890. [Google Scholar] [CrossRef] [PubMed]
- Miglioretti, D.L.; Ichikawa, L.; Smith, R.A.; Bassett, L.W.; Feig, S.A.; Monsees, B.; Parikh, J.R.; Rosenberg, R.D.; Sickles, E.A.; Carney, P.A. Criteria for Identifying Radiologists with Acceptable Screening Mammography Interpretive Performance on Basis of Multiple Performance Measures. Am. J. Roentgenol. 2015, 204, W486–W491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carney, P.A.; Miglioretti, D.L.; Yankaskas, B.C.; Kerlikowske, K.; Rosenberg, R.; Rutter, C.M.; Geller, B.M.; Abraham, L.A.; Taplin, S.H.; Dignan, M.; et al. Individual and Combined Effects of Age, Breast Density, and Hormone Replacement Therapy Use on the Accuracy of Screening Mammography. Ann. Intern. Med. 2003, 138, 168–175. [Google Scholar] [CrossRef]
- Van der Waal, D.; Ripping, T.M.; Verbeek, A.L.M.; Broeders, M.J.M. Breast cancer screening effect across breast density strata: A case–control study. Int. J. Cancer 2017, 140, 41–49. [Google Scholar] [CrossRef] [Green Version]
- Mandelson, M.T.; Oestreicher, N.; Porter, P.L.; White, D.; Finder, C.A.; Taplin, S.H.; White, E. Breast density as a predictor of mammographic detection: Comparison of interval- and screen-detected cancers. J. Natl. Cancer Inst. 2000, 92, 1081–1087. [Google Scholar] [CrossRef]
- Brem, R.F.; Lenihan, M.J.; Lieberman, J.; Torrente, J. Screening Breast Ultrasound: Past, Present, and Future. Am. J. Roentgenol. 2015, 204, 234–240. [Google Scholar] [CrossRef]
- Wang, A.T.; Vachon, C.M.; Brandt, K.R.; Ghosh, K. Breast Density and Breast Cancer Risk: A Practical Review. Mayo Clin. Proc. 2014, 89, 548–557. [Google Scholar] [CrossRef] [Green Version]
- DiPrete, O.; Lourenco, A.P.; Baird, G.L.; Mainiero, M.B. Screening Digital Mammography Recall Rate: Does It Change with Digital Breast Tomosynthesis Experience? Radiology 2018, 286, 838–844. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| First-Visit | Follow-Up | p-Value | ||||
|---|---|---|---|---|---|---|
| BI-RADS | Mammography | % | Mammography | % | ||
| Negative | 1 | 1343 | 90.7 | 586 | 96.0 | <0.0001 |
| 2 | 7726 | 4105 | ||||
| 3 | 36 | 9 | ||||
| Positive | 4 | 35 | 9.3 | 11 | 4.0 | <0.0001 |
| 5 | 2 | 0 | ||||
| 0 | 898 | 184 | ||||
| Total | 10,040 | 100 | 4895 | 100 | ||
| First-Visit | Follow-Up | p-Value | |||
|---|---|---|---|---|---|
| Mammography | % | Mammography | % | ||
| Benign | 201 | 73.1 | 43 | 64.2 | 0.1491 |
| Malignant | 74 | 26.9 | 24 | 35.8 | |
| Total | 275 | 100 | 67 | 100 | |
| First-Visit + Follow-Up | First-Visit | Follow-Up | p-Value | |
|---|---|---|---|---|
| Recall rate (%) | 7.9 | 9.7 | 4.2 | <0.0001 |
| CDR (per 1000) | 6.6 | 7.4 | 4.9 | 0.0761 |
| PPV1 (%) | 8.3 | 7.6 | 11.8 | <0.0001 |
| PPV2 (%) | 25.7 | 24.2 | 32.0 | <0.0001 |
| PPV3 (%) | 28.7 | 27.0 | 35.8 | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, C.-C.; Ho, T.-C.; Lien, C.-Y.; Shen, D.H.-Y.; Chuang, K.-P.; Chan, H.-P.; Yang, M.-H.; Tyan, Y.-C. The Effects of Prior Mammography Screening on the Performance of Breast Cancer Detection in Taiwan. Healthcare 2022, 10, 1037. https://doi.org/10.3390/healthcare10061037
Chang C-C, Ho T-C, Lien C-Y, Shen DH-Y, Chuang K-P, Chan H-P, Yang M-H, Tyan Y-C. The Effects of Prior Mammography Screening on the Performance of Breast Cancer Detection in Taiwan. Healthcare. 2022; 10(6):1037. https://doi.org/10.3390/healthcare10061037
Chicago/Turabian StyleChang, Chin-Chuan, Tzu-Chuan Ho, Chih-Ying Lien, Daniel Hueng-Yuan Shen, Kuo-Pin Chuang, Hung-Pin Chan, Ming-Hui Yang, and Yu-Chang Tyan. 2022. "The Effects of Prior Mammography Screening on the Performance of Breast Cancer Detection in Taiwan" Healthcare 10, no. 6: 1037. https://doi.org/10.3390/healthcare10061037
APA StyleChang, C.-C., Ho, T.-C., Lien, C.-Y., Shen, D. H.-Y., Chuang, K.-P., Chan, H.-P., Yang, M.-H., & Tyan, Y.-C. (2022). The Effects of Prior Mammography Screening on the Performance of Breast Cancer Detection in Taiwan. Healthcare, 10(6), 1037. https://doi.org/10.3390/healthcare10061037