
Health-Related Quality of Life Sleep Score Predicts Transfer to Hemodialysis among Patients on Peritoneal Dialysis

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection, Participant Evaluation, and Biochemical Analyses
2.3. Assessment of Health-Related Quality of Life
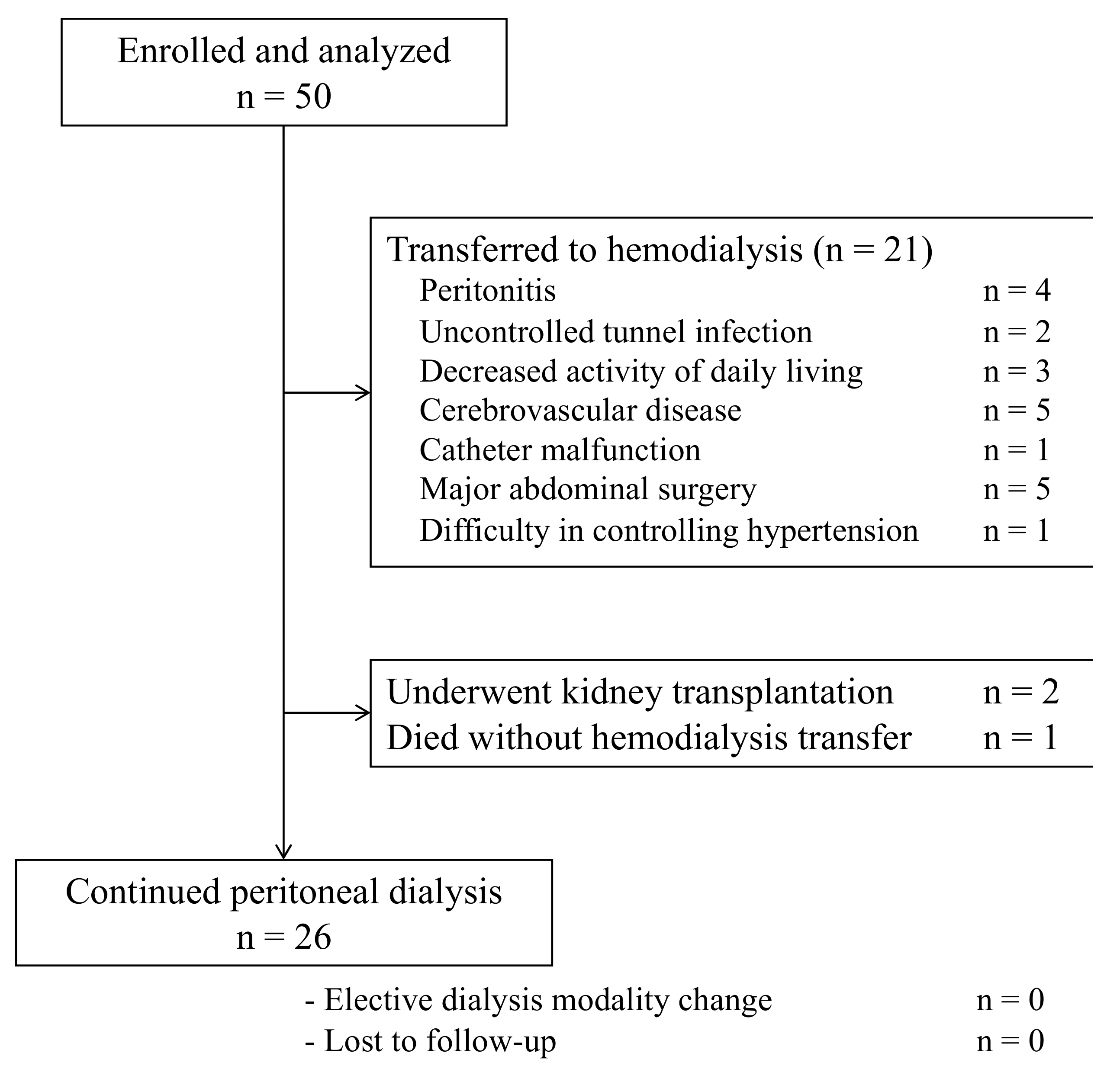
2.4. Follow-Up
2.5. Statistical Analyses
3. Results
3.1. Clinical Characteristics
3.2. Association of HRQOL (KDQOL/SF-36) Components with HD Transfer
3.3. Association of Clinical Parameters with HRQOL Sleep Score
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chuasuwan, A.; Pooripussarakul, S.; Thakkinstian, A.; Ingsathit, A.; Pattanaprateep, O. Comparisons of Quality of Life Between Patients Underwent Peritoneal Dialysis and Hemodialysis: A Systematic Review and Meta-Analysis. Health Qual. Life Outcomes 2020, 18, 191. [Google Scholar] [CrossRef] [PubMed]
- Paniagua, R.; Amato, D.; Vonesh, E.; Guo, A.; Mujais, S.; Mexican Nephrology Collaborative Study Group. Health-Related Quality of Life Predicts Outcomes but Is Not Affected by Peritoneal Clearance: The ADEMEX Trial. Kidney Int. 2005, 67, 1093–1104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bastos, M.A.P.; Reis, I.A.; Cherchiglia, M.L. Health-Related Quality of Life Associated with Risk of Death in Brazilian Dialysis Patients: An Eight-Year Cohort. Qual. Life Res. 2021, 30, 1595–1604. [Google Scholar] [CrossRef]
- Uchiyama, K.; Washida, N.; Muraoka, K.; Morimoto, K.; Kasai, T.; Yamaki, K.; Miyashita, K.; Wakino, S.; Itoh, H. Exercise Capacity and Association with Quality of Life in Peritoneal Dialysis Patients. Perit. Dial. Int. 2019, 39, 66–73. [Google Scholar] [CrossRef] [PubMed]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2016. [Google Scholar]
- JCS Joint Working Group. Guidelines for Rehabilitation in Patients with Cardiovascular Disease (JCS 2012). Circ. J. 2014, 78, 2022–2093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamijo, Y.; Kanda, E.; Ishibashi, Y.; Yoshida, M. Sarcopenia and Frailty in PD: Impact on Mortality, Malnutrition, and Inflammation. Perit. Dial. Int. 2018, 38, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Green, J.; Fukuhara, S.; Shinzato, T.; Miura, Y.; Wada, S.; Hays, R.D.; Tabata, R.; Otsuka, H.; Takai, I.; Maeda, K.; et al. Translation, Cultural Adaptation, and Initial Reliability and Multitrait Testing of the Kidney Disease Quality of Life Instrument for Use in Japan. Qual. Life Res. 2001, 10, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Suzukamo, Y.; Fukuhara, S.; Green, J.; Kosinski, M.; Gandek, B.; Ware, J.E. Validation Testing of a Three-Component Model of Short Form-36 Scores. J. Clin. Epidemiol. 2011, 64, 301–308. [Google Scholar] [CrossRef]
- Mapes, D.L.; Lopes, A.A.; Satayathum, S.; McCullough, K.P.; Goodkin, D.A.; Locatelli, F.; Fukuhara, S.; Young, E.W.; Kurokawa, K.; Saito, A.; et al. Health-Related Quality of Life as a Predictor of Mortality and Hospitalization: The Dialysis Outcomes and Practice Patterns Study (DOPPS). Kidney Int. 2003, 64, 339–349. [Google Scholar] [CrossRef] [Green Version]
- Figueiredo, A.; Goh, B.L.; Jenkins, S.; Johnson, D.W.; Mactier, R.; Ramalakshmi, S.; Shrestha, B.; Struijk, D.; Wilkie, M.; International Society for Peritoneal Dialysis. Clinical Practice Guidelines for Peritoneal Access. Perit. Dial. Int. 2010, 30, 424–429. [Google Scholar] [CrossRef] [Green Version]
- Nakayama, T.; Uchiyama, K.; Washida, N.; Morimoto, K.; Muraoka, K.; Adachi, K.; Kasai, T.; Miyashita, K.; Wakino, S.; Itoh, H. Exercise Parameters Predict Technique Survival in Patients on Peritoneal Dialysis. Blood Purif. 2021, 50, 380–389. [Google Scholar] [CrossRef]
- Chidambaram, M.; Bargman, J.M.; Quinn, R.R.; Austin, P.C.; Hux, J.E.; Laupacis, A. Patient and Physician Predictors of Peritoneal Dialysis Technique Failure: A Population Based, Retrospective Cohort Study. Perit. Dial. Int. 2011, 31, 565–573. [Google Scholar] [CrossRef]
- Boudville, N.; Ullah, S.; Clayton, P.; Sud, K.; Borlace, M.; Badve, S.V.; Chakera, A.; Johnson, D.W. Differences in Peritoneal Dialysis Technique Survival Between Patients Treated with Peritoneal Dialysis Systems from Different Companies. Nephrol. Dial. Transplant. 2019, 34, 1035–1044. [Google Scholar] [CrossRef]
- See, E.J.; Johnson, D.W.; Hawley, C.M.; Pascoe, E.M.; Badve, S.V.; Boudville, N.; Clayton, P.A.; Sud, K.; Polkinghorne, K.R.; Borlace, M.; et al. Risk Predictors and Causes of Technique Failure Within the First Year of Peritoneal Dialysis: An Australia and New Zealand Dialysis and Transplant Registry (ANZDATA) Study. Am. J. Kidney Dis. 2018, 72, 188–197. [Google Scholar] [CrossRef]
- Jung, H.Y.; Jeon, Y.; Park, Y.; Kim, Y.S.; Kang, S.-W.; Yang, C.W.; Kim, N.-H.; Choi, J.-Y.; Cho, J.-H.; Park, S.-H.; et al. Better Quality of Life of Peritoneal Dialysis Compared to Hemodialysis over a Two-Year Period After Dialysis Initiation. Sci. Rep. 2019, 9, 10266. [Google Scholar] [CrossRef]
- Iyasere, O.U.; Brown, E.A.; Johansson, L.; Huson, L.; Smee, J.; Maxwell, A.P.; Farrington, K.; Davenport, A. Quality of Life and Physical Function in Older Patients on Dialysis: A Comparison of Assisted Peritoneal Dialysis with Hemodialysis. Clin. J. Am. Soc. Nephrol. 2016, 11, 423–430. [Google Scholar] [CrossRef] [Green Version]
- Finkelstein, F.O.; Foo, M.W. Health-Related Quality of Life and Adequacy of Dialysis for the Individual Maintained on Peritoneal Dialysis. Perit. Dial. Int. 2020, 40, 270–273. [Google Scholar] [CrossRef] [Green Version]
- Bonenkamp, A.A.; van der Sluijs, A.V.E.; Hoekstra, T.; Verhaar, M.C.; van Ittersum, F.J.; Abrahams, A.C.; van Jaarsveld, B.C. Health-Related Quality of Life in Home Dialysis Patients Compared to In-Center Hemodialysis Patients: A Systematic Review and Meta-analysis. Kidney Med. 2020, 2, 139–154. [Google Scholar] [CrossRef]
- Zazzeroni, L.; Pasquinelli, G.; Nanni, E.; Cremonini, V.; Rubbi, I. Comparison of Quality of Life in Patients Undergoing Hemodialysis and Peritoneal Dialysis: A Systematic Review and Meta-Analysis. Kidney Blood Press. Res. 2017, 42, 717–727. [Google Scholar] [CrossRef]
- Ibrahimou, B.; Albatineh, A.N. Predictors of Quality of Life Among Peritoneal Dialysis Patients with End-Stage Renal Disease in Kuwait. Perit. Dial. Int. 2019, 39, 180–182. [Google Scholar] [CrossRef]
- Aguiar, R.; Pei, M.; Qureshi, A.R.; Lindholm, B. Health-Related Quality of Life in Peritoneal Dialysis Patients: A Narrative Review. Semin. Dial. 2019, 32, 452–462. [Google Scholar] [CrossRef]
- Brown, E.A.; Zhao, J.; McCullough, K.; Fuller, D.S.; Figueiredo, A.E.; Bieber, B.; Finkelstein, F.O.; Shen, J.; Kanjanabuch, T.; Kawanishi, H.; et al. Burden of Kidney Disease, Health-Related Quality of Life, and Employment Among Patients Receiving Peritoneal Dialysis and In-Center Hemodialysis: Findings from the DOPPS Program. Am. J. Kidney Dis. 2021, 78, 489–500.e1. [Google Scholar] [CrossRef]
- Tao, X.; Zhang, H.; Huang, J.; Gu, A.; Jin, Y.; He, Y.; Li, N.; Yang, Y. Physical Performance and Health-Related Quality of Life Among Older Adults on Peritoneal Dialysis: A Cross-Sectional Study. Int. Urol. Nephrol. 2021, 53, 1033–1042. [Google Scholar] [CrossRef]
- Uchiyama, K.; Washida, N.; Morimoto, K.; Muraoka, K.; Kasai, T.; Yamaki, K.; Miyashita, K.; Wakino, S.; Itoh, H. Home-Based Aerobic Exercise and Resistance Training in Peritoneal Dialysis Patients: A Randomized Controlled Trial. Sci. Rep. 2019, 9, 2632. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.; Zhang, Y.; Yang, Z.; Wang, J.; Xiong, Z.; Liao, J.; Hao, L.; Liu, G.; Ren, Y.; Wang, Q.; et al. Sleep Disorders and Cognitive Impairment in Peritoneal Dialysis: A Multicenter Prospective Cohort Study. Kidney Blood Press. Res. 2019, 44, 1115–1127. [Google Scholar] [CrossRef]
- Tang, S.C.; Lai, K.N. Sleep Disturbances and Sleep Apnea in Patients on Chronic Peritoneal Dialysis. J. Nephrol. 2009, 22, 318–325. [Google Scholar]
- Zhang, H.; Yang, Y.; Huang, J.; Lailan, S.; Tao, X. Correlates of Objective Sleep Quality in Older Peritoneal Dialysis Patients. Ren. Fail. 2021, 43, 180–187. [Google Scholar] [CrossRef]
- Tang, S.C.; Lam, B.; Ku, P.P.; Leung, W.S.; Chu, C.M.; Ho, Y.W.; Ip, M.S.; Lai, K.N. Alleviation of Sleep Apnea in Patients with Chronic Renal Failure by Nocturnal Cycler-Assisted Peritoneal Dialysis Compared with Conventional Continuous Ambulatory Peritoneal Dialysis. J. Am. Soc. Nephrol. 2006, 17, 2607–2616. [Google Scholar] [CrossRef] [Green Version]
- Ling, L.L.; Chan, Y.M.; Mat Daud, Z.A. Serum Potassium and Handgrip Strength as Predictors of Sleep Quality Among Hemodialysis Patients in Malaysia. Asia Pac. J. Clin. Nutr. 2019, 28, 401–410. [Google Scholar] [CrossRef] [PubMed]
- Unruh, M.L.; Buysse, D.J.; Dew, M.A.; Evans, I.V.; Wu, A.W.; Fink, N.E.; Powe, N.R.; Meyer, K.B.; for the Choices for Healthy Outcomes in Caring for End-Stage Renal Disease (CHOICE) Study. Sleep Quality and its Correlates in the First Year of Dialysis. Clin. J. Am. Soc. Nephrol. 2006, 1, 802–810. [Google Scholar] [CrossRef]
- Han, Q.; Liu, B.; Lin, S.; Li, J.; Liang, P.; Fu, S.; Zheng, G.; Yang, S.; Li, B.; Yang, Q. Pittsburgh Sleep Quality Index Score Predicts All-Cause Mortality in Chinese Dialysis Patients. Int. Urol. Nephrol. 2021, 53, 2369–2376. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.Y.; Cui, Z.; Su, C.Y.; Li, J.; Liang, P.; Fu, S.; Zheng, G.; Yang, S.; Li, B.; Yang, Q. Prognostic Implications of Predialysis Patients’ Symptoms in Peritoneal Dialysis Patients. Ren. Fail. 2021, 43, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Natale, P.; Ruospo, M.; Saglimbene, V.M.; Palmer, S.C.; Strippoli, G.F. Interventions for Improving Sleep Quality in People with Chronic Kidney Disease. Cochrane Database Syst. Rev. 2019, 5, Cd012625. [Google Scholar] [CrossRef] [PubMed]
- Fabbri, M.; Beracci, A.; Martoni, M.; Meneo, D.; Tonetti, L.; Natale, V. Measuring Subjective Sleep Quality: A Review. Int. J. Environ. Res. Public Health 2021, 18, 1082. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Total (n = 50) | Continued PD (n = 29) | Transferred to HD (n = 21) |
|---|---|---|---|
| Age, year | 63 (59–71) | 63 (58–70) | 63 (60–70) |
| Sex (% male) | 37 (74%) | 21 (81%) | 16 (76%) |
| DM | 15 (30%) | 5 (19%) | 10 (48%) |
| CCI | 3.0 (2.0–4.0) | 2.5 (2.0–3.0) | 3.7 (3.0–5.0) |
| APD/CAPD | 13/37 (26/74%) | 8/18 (31/69%) | 5/16 (24/76%) |
| Cardiovascular disease | 16 (32%) | 4 (15%) | 12 (57%) |
| Smoking history | 28 (56%) | 15 (58%) | 13 (62%) |
| PD vintage, year | 3.5 (1.3–6.5) | 3.7 (1.2–5.8) | 4.0 (1.5–6.6) |
| Urine output, mL/day | 410 (0–1,050) | 732 (7–1,150) | 485 (0–900) |
| Renal, Kt/V | 0.19 (0–0.80) | 0.43 (0–0.84) | 0.39 (0–0.73) |
| BMI, kg/m2 | 23.8 ± 4.0 | 23.5 ± 4.0 | 24.2 ± 4.1 |
| SMI, kg/m2 | 7.3 ± 1.3 | 7.4 ± 1.2 | 7.1 ± 1.3 |
| PD, Kt/V | 1.29 (1.01–1.57) | 1.27 (0.97–1.55) | 1.39 (1.07–1.58) |
| Total, Kt/V | 1.70 (1.44–1.89) | 1.70 (1.47–1.87) | 1.76 (1.43–1.91) |
| Mean blood pressure, mmHg | 96.9 ± 13.8 | 97.3 ± 13.0 | 96.4 ± 15.2 |
| Hemoglobin, g/dL | 10.6 ± 1.3 | 10.5 ± 1.3 | 10.8 ± 1.2 |
| Albumin, mg/dL | 3.4 ± 0.5 | 3.4 ± 0.5 | 3.4 ± 0.4 |
| Potassium, mEq/L | 4.6 ± 0.6 | 4.6 ± 0.6 | 4.6 ± 0.7 |
| Calcium, mg/dL | 9.6 ± 1.6 | 9.7 ± 2.0 | 9.5 ± 0.6 |
| Phosphorus, mg/dL | 5.5 ± 1.1 | 5.2 ± 1.2 | 5.8 ± 1.0 |
| PTH, pmol/L | 184.0 (106.3–270.8) | 224.1 (101–271) | 216.1 (110–270) |
| CRP, mg/L | 0.09 (0.03–0.23) | 0.24 (0.02–0.22) | 0.28 (0.04–0.23) |
| hANP, pg/mL | 70.4 (49.1–118.8) | 87.7 (41.6–120) | 117.8 (50.2–115) |
| ISWT, m | 312.0 ± 138.2 | 353.2 ± 132.7 | 255.2 ± 124.0 |
| Handgrip strength, kg | 28.5 (23.3–31.0) | 28.1 (25.9–31.7) | 26.6 (21.6–30.7) |
| Quadriceps strength, kg | 22.3 (14.5–31.1) | 24.8 (15.7–34.6) | 21.2 (14.5–27.7) |
| HRQOL Components | Total (n = 50) | Continued PD (n = 29) | Transferred to HD (n = 21) |
|---|---|---|---|
| KDQOL | |||
| Symptoms/problems | 77.6 ± 12.5 | 80.9 ± 11.4 | 73.0 ± 12.8 |
| Effects of kidney disease | 76.7 ± 14.4 | 80.0 ± 14.3 | 72.1 ± 13.6 |
| Burden of kidney disease | 43.3 ± 21.5 | 47.4 ± 23.5 | 37.5 ± 17.2 |
| Cognitive function | 90.4 ± 12.2 | 92.4 ± 12.8 | 87.5 ± 11.0 |
| Quality of social interaction | 87.8 ± 15.8 | 89.4 ± 14.5 | 85.6 ± 17.8 |
| Sleep | 62.2 ± 18.2 | 67.2 ± 17.5 | 55.3 ± 17.3 |
| Social support | 80.0 ± 20.2 | 79.3 ± 21.2 | 80.9 ± 19.2 |
| Encouragement from staff | 82.8 ± 19.3 | 86.0 ± 15.9 | 78.4 ± 23.0 |
| Satisfaction for care | 80.6 ± 16.2 | 82.7 ± 17.3 | 77.5 ± 14.6 |
| KDCS | 74.1 ± 9.9 | 76.4 ± 9.8 | 71.0 ± 9.2 |
| SF-36 | |||
| Physical function | 73.7 ± 21.5 | 74.5 ± 23.2 | 72.6 ± 19.3 |
| Physical Role Functioning | 68.5 ± 24.0 | 72.8 ± 23.4 | 62.5 ± 24.0 |
| Pain | 71.1 ± 24.3 | 73.3 ± 25.7 | 68.1 ± 22.4 |
| General health | 44.5 ± 17.7 | 46.3 ± 19.4 | 42.1 ± 15.2 |
| Vitality | 54.8 ± 20.8 | 59.5 ± 19.3 | 48.5 ± 21.6 |
| Social Functioning | 69.0 ± 28.0 | 67.7 ± 31.3 | 70.8 ± 23.5 |
| Emotional Role Functioning | 77.5 ± 21.6 | 81.0 ± 20.0 | 72.6 ± 23.4 |
| Mental health | 71.3 ± 18.1 | 74.9 ± 18.0 | 66.4 ± 17.6 |
| PCS | 39.8 ± 13.8 | 40.5 ± 15.0 | 38.8 ± 12.3 |
| MCS | 50.0 ± 8.9 | 51.4 ± 8.3 | 48.2 ± 9.6 |
| RCS | 44.3 ± 12.4 | 45.2 ± 12.0 | 43.1 ± 13.2 |
| HRQOL Domains (per 10) | Model A | Model B | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Cause-specific hazards | ||||||
| KDQOL | ||||||
| Symptoms/problems | 0.82 | 0.53–1.28 | 0.39 | 0.72 | 0.47–1.11 | 0.14 |
| Effects of kidney disease | 1.08 | 0.77–1.52 | 0.65 | 1.00 | 0.71–1.40 | 0.99 |
| Burden of kidney disease | 1.11 | 0.79–1.54 | 0.56 | 0.97 | 0.73–1.28 | 0.81 |
| Cognitive function | 1.03 | 0.68–1.55 | 0.91 | 0.91 | 0.62–1.35 | 0.65 |
| Quality of social interaction | 0.96 | 0.72–1.29 | 0.80 | 0.97 | 0.72–1.30 | 0.81 |
| Sleep | 0.69 | 0.52–0.92 | 0.01 | 0.72 | 0.55–0.94 | 0.02 |
| Social support | 1.20 | 0.92–1.56 | 0.18 | 1.16 | 0.89–1.49 | 0.27 |
| Encouragement from staff | 0.87 | 0.66–1.14 | 0.30 | 0.87 | 0.65–1.17 | 0.36 |
| Satisfaction for care | 0.78 | 0.54–1.12 | 0.18 | 0.87 | 0.63–1.21 | 0.41 |
| KDCS | 0.90 | 0.46–1.75 | 0.76 | 0.93 | 0.52–1.66 | 0.81 |
| SF-36 | ||||||
| Physical function | 1.22 | 0.97–1.54 | 0.09 | 1.16 | 0.92–1.45 | 0.21 |
| Physical Role Functioning | 0.91 | 0.69–1.20 | 0.50 | 0.91 | 0.70–1.18 | 0.48 |
| Pain | 0.98 | 0.79–1.20 | 0.81 | 0.96 | 0.79–1.18 | 0.71 |
| General health | 1.36 | 0.92–2.02 | 0.12 | 1.13 | 0.81–1.58 | 0.46 |
| Vitality | 0.89 | 0.64–1.22 | 0.47 | 0.86 | 0.64–1.14 | 0.29 |
| Social Functioning | 1.08 | 0.89–1.31 | 0.45 | 1.06 | 0.89–1.27 | 0.51 |
| Emotional Role Functioning | 0.82 | 0.63–1.07 | 0.14 | 0.85 | 0.67–1.09 | 0.20 |
| Mental health | 0.84 | 0.64–1.10 | 0.21 | 0.89 | 0.70–1.13 | 0.34 |
| PCS | 1.35 | 0.95–1.93 | 0.10 | 1.23 | 0.86–1.76 | 0.25 |
| MCS | 0.81 | 0.45–1.46 | 0.49 | 0.79 | 0.45–1.38 | 0.41 |
| RCS | 0.71 | 0.43–1.16 | 0.17 | 0.83 | 0.54–1.28 | 0.40 |
| Subdistribution hazards | ||||||
| KDQOL | ||||||
| Symptoms/problems | 0.84 | 0.52–1.35 | 0.47 | 0.76 | 0.48–1.18 | 0.22 |
| Effects of kidney disease | 1.12 | 0.81–1.53 | 0.50 | 1.04 | 0.75–1.43 | 0.83 |
| Burden of kidney disease | 1.14 | 0.76–1.72 | 0.53 | 1.00 | 0.75–1.34 | 1 |
| Cognitive function | 1.02 | 0.67–1.57 | 0.92 | 0.90 | 0.60–1.34 | 0.61 |
| Quality of social interaction | 0.97 | 0.70–1.34 | 0.85 | 0.97 | 0.71–1.32 | 0.84 |
| Sleep | 0.70 | 0.55–0.88 | 0.002 | 0.73 | 0.60–0.90 | 0.004 |
| Social support | 1.17 | 0.94–1.46 | 0.17 | 1.13 | 0.87–1.47 | 0.37 |
| Encouragement from staff | 0.89 | 0.73–1.09 | 0.25 | 0.90 | 0.68–1.19 | 0.46 |
| Satisfaction for care | 0.81 | 0.63–1.04 | 0.10 | 0.91 | 0.71–1.18 | 0.48 |
| KDCS | 0.96 | 0.46–2.01 | 0.91 | 1.00 | 0.59–1.70 | 1 |
| SF-36 | ||||||
| Physical function | 1.20 | 0.98–1.48 | 0.07 | 1.14 | 0.93–1.41 | 0.22 |
| Physical Role Functioning | 0.92 | 0.65–1.31 | 0.65 | 0.92 | 0.69–1.25 | 0.61 |
| Pain | 0.98 | 0.78–1.24 | 0.88 | 0.97 | 0.70–1.20 | 0.80 |
| General health | 1.33 | 0.89–1.98 | 0.17 | 1.13 | 0.81–1.58 | 0.47 |
| Vitality | 0.91 | 0.62–1.34 | 0.63 | 0.87 | 0.63–1.21 | 0.41 |
| Social Functioning | 1.09 | 0.89–1.32 | 0.42 | 1.07 | 0.91–1.26 | 0.41 |
| Emotional Role Functioning | 0.84 | 0.61–1.14 | 0.26 | 0.88 | 0.69–1.12 | 0.29 |
| Mental health | 0.83 | 0.63–1.09 | 0.18 | 0.88 | 0.70–1.10 | 0.26 |
| PCS | 1.34 | 1.00–1.78 | 0.05 | 1.21 | 0.87–1.70 | 0.26 |
| MCS | 0.82 | 0.45–1.49 | 0.51 | 0.79 | 0.45–1.40 | 0.42 |
| RCS | 0.72 | 0.39–1.36 | 0.32 | 0.86 | 0.53–1.38 | 0.53 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nagasaka, T.; Washida, N.; Uchiyama, K.; Hama, E.Y.; Kusahana, E.; Nakayama, T.; Yasuda, I.; Morimoto, K.; Itoh, H. Health-Related Quality of Life Sleep Score Predicts Transfer to Hemodialysis among Patients on Peritoneal Dialysis. Healthcare 2022, 10, 1030. https://doi.org/10.3390/healthcare10061030
Nagasaka T, Washida N, Uchiyama K, Hama EY, Kusahana E, Nakayama T, Yasuda I, Morimoto K, Itoh H. Health-Related Quality of Life Sleep Score Predicts Transfer to Hemodialysis among Patients on Peritoneal Dialysis. Healthcare. 2022; 10(6):1030. https://doi.org/10.3390/healthcare10061030
Chicago/Turabian StyleNagasaka, Tomoki, Naoki Washida, Kiyotaka Uchiyama, Eriko Yoshida Hama, Ei Kusahana, Takashin Nakayama, Itaru Yasuda, Kohkichi Morimoto, and Hiroshi Itoh. 2022. "Health-Related Quality of Life Sleep Score Predicts Transfer to Hemodialysis among Patients on Peritoneal Dialysis" Healthcare 10, no. 6: 1030. https://doi.org/10.3390/healthcare10061030
APA StyleNagasaka, T., Washida, N., Uchiyama, K., Hama, E. Y., Kusahana, E., Nakayama, T., Yasuda, I., Morimoto, K., & Itoh, H. (2022). Health-Related Quality of Life Sleep Score Predicts Transfer to Hemodialysis among Patients on Peritoneal Dialysis. Healthcare, 10(6), 1030. https://doi.org/10.3390/healthcare10061030