
Associations between Measured and Patient-Reported Physical Function and Survival in Advanced NSCLC

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
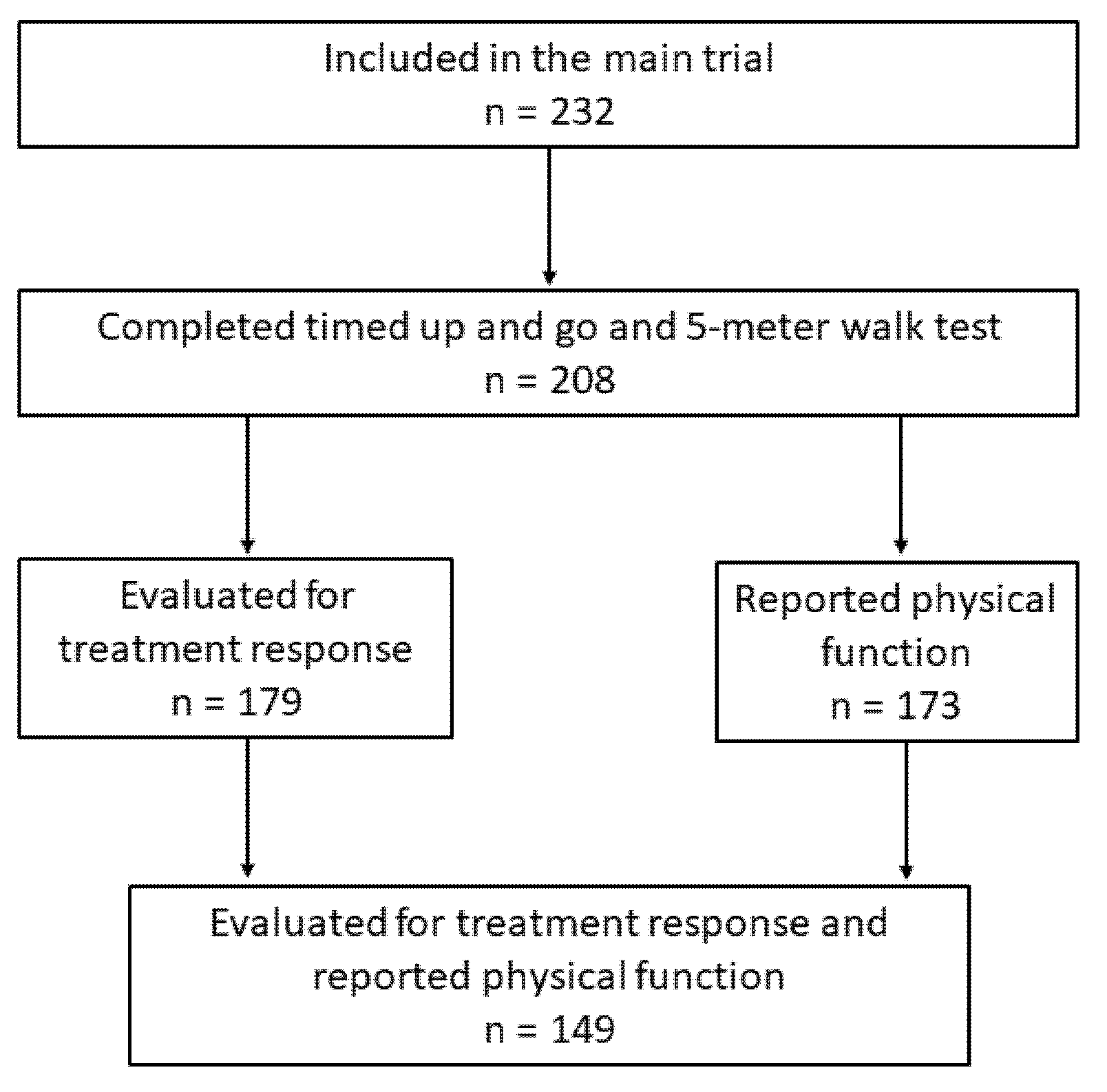
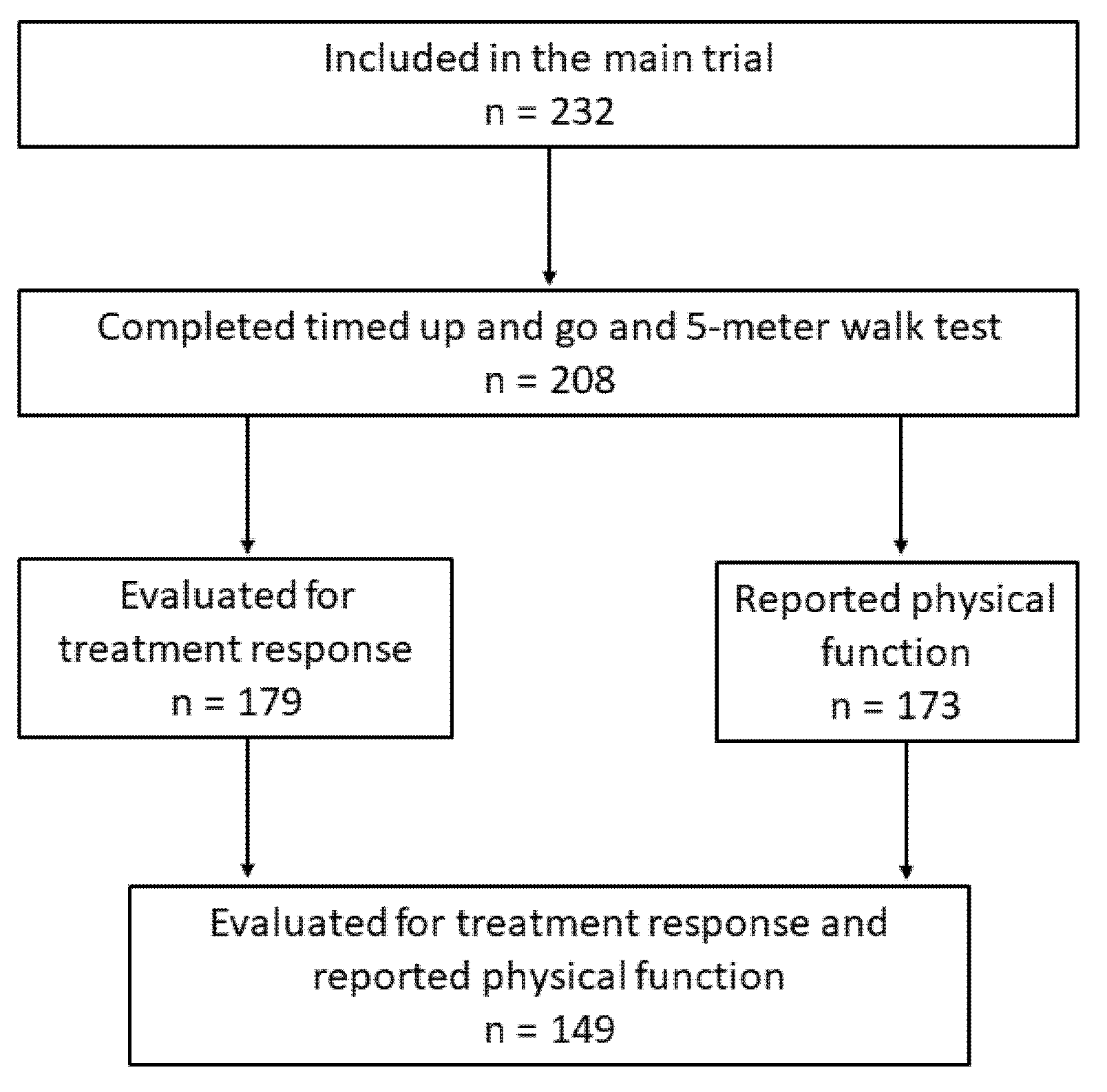
2.1. Patients
2.2. Timed Up and Go Test (TUG)
2.3. 5-Meter Walk Test (5 mWT)
2.4. Patient-Reported Physical Function (PRPF)
2.5. Treatment Completion and Endpoints
2.6. Statistical Considerations
2.7. Approvals
3. Results
3.1. Baseline Characteristics
3.2. Treatment Completion
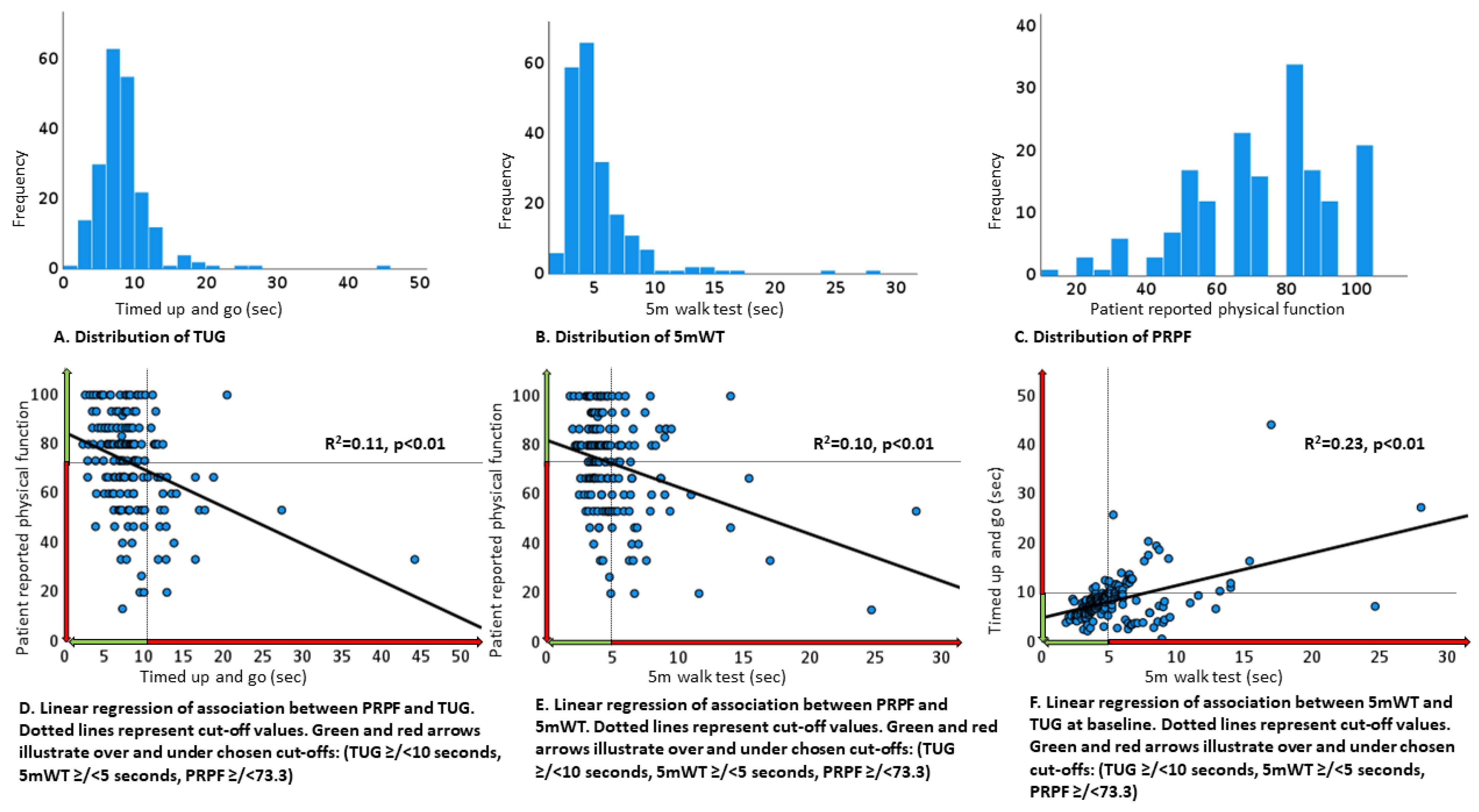
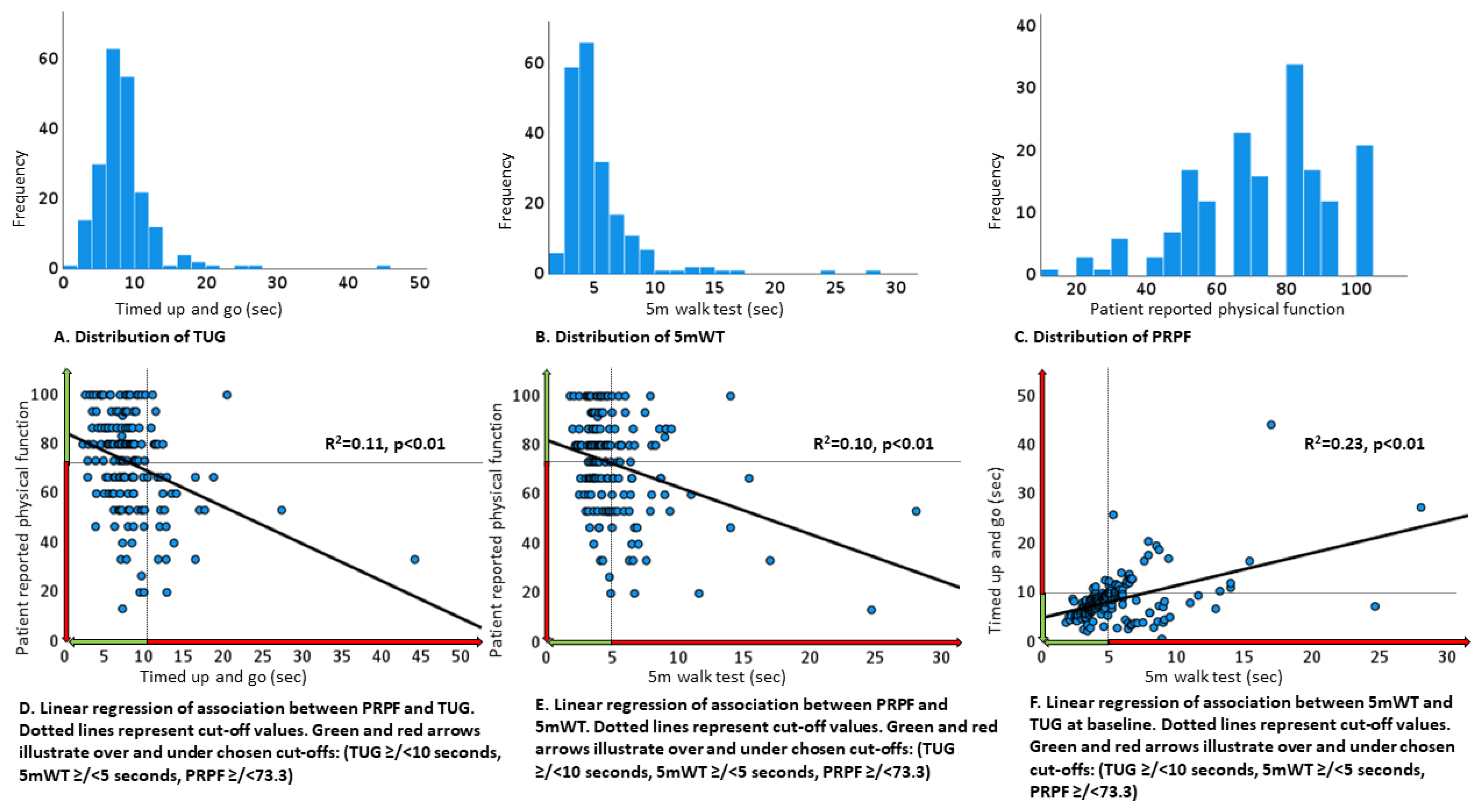
3.3. Timed Up and Go (TUG)
3.4. 5-Meter Walk Test (5 mWT)
3.5. Patient-Reported Physical Function (PRPF)
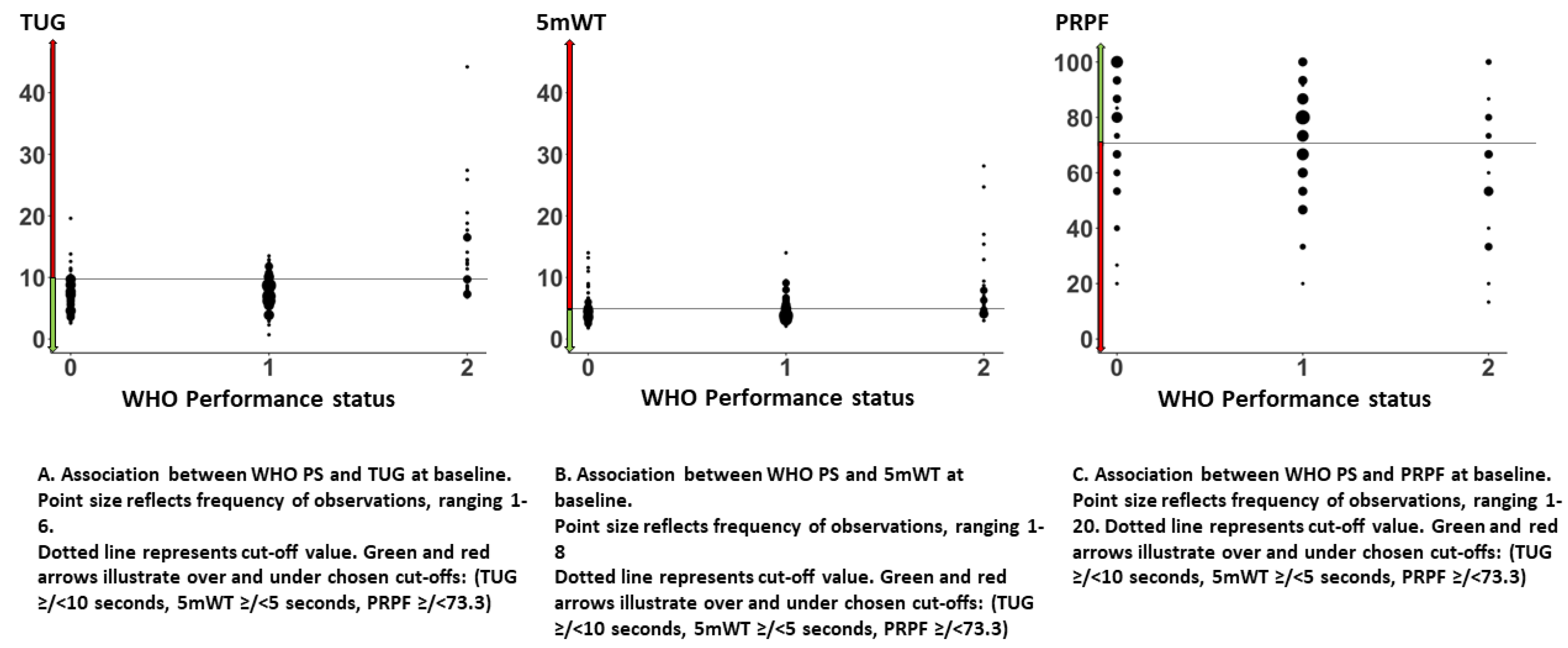
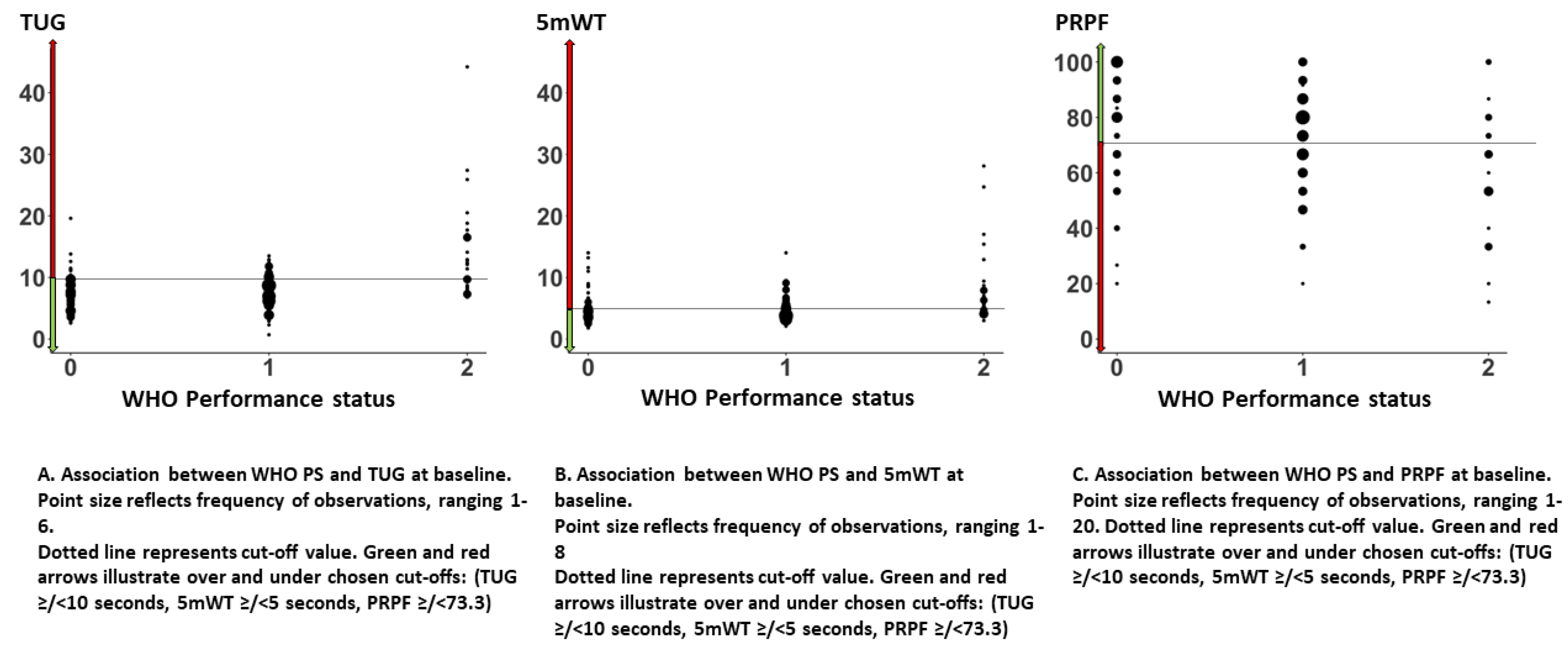
3.6. Association between TUG, 5 mWT, PRPF, and WHO PS
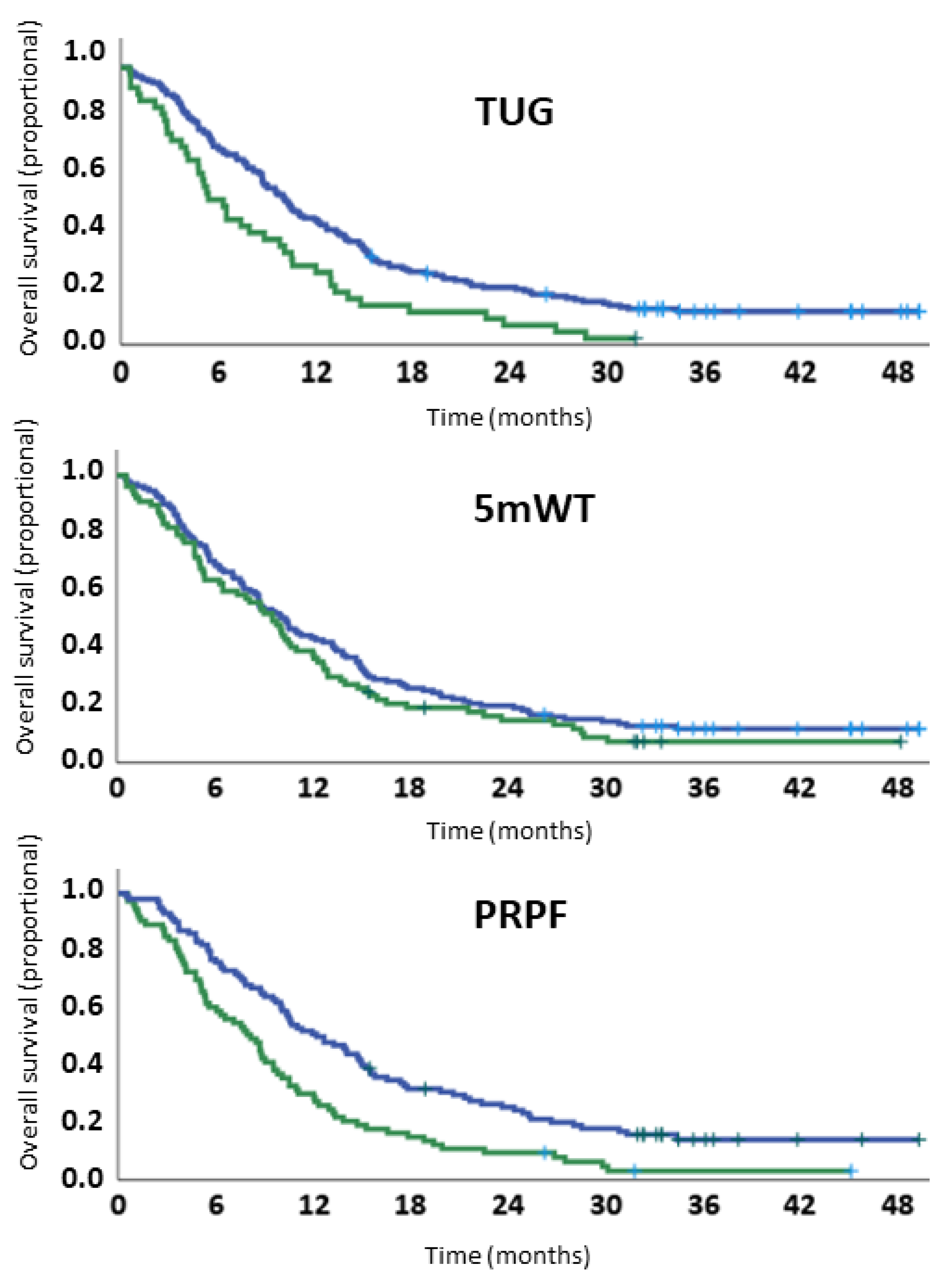
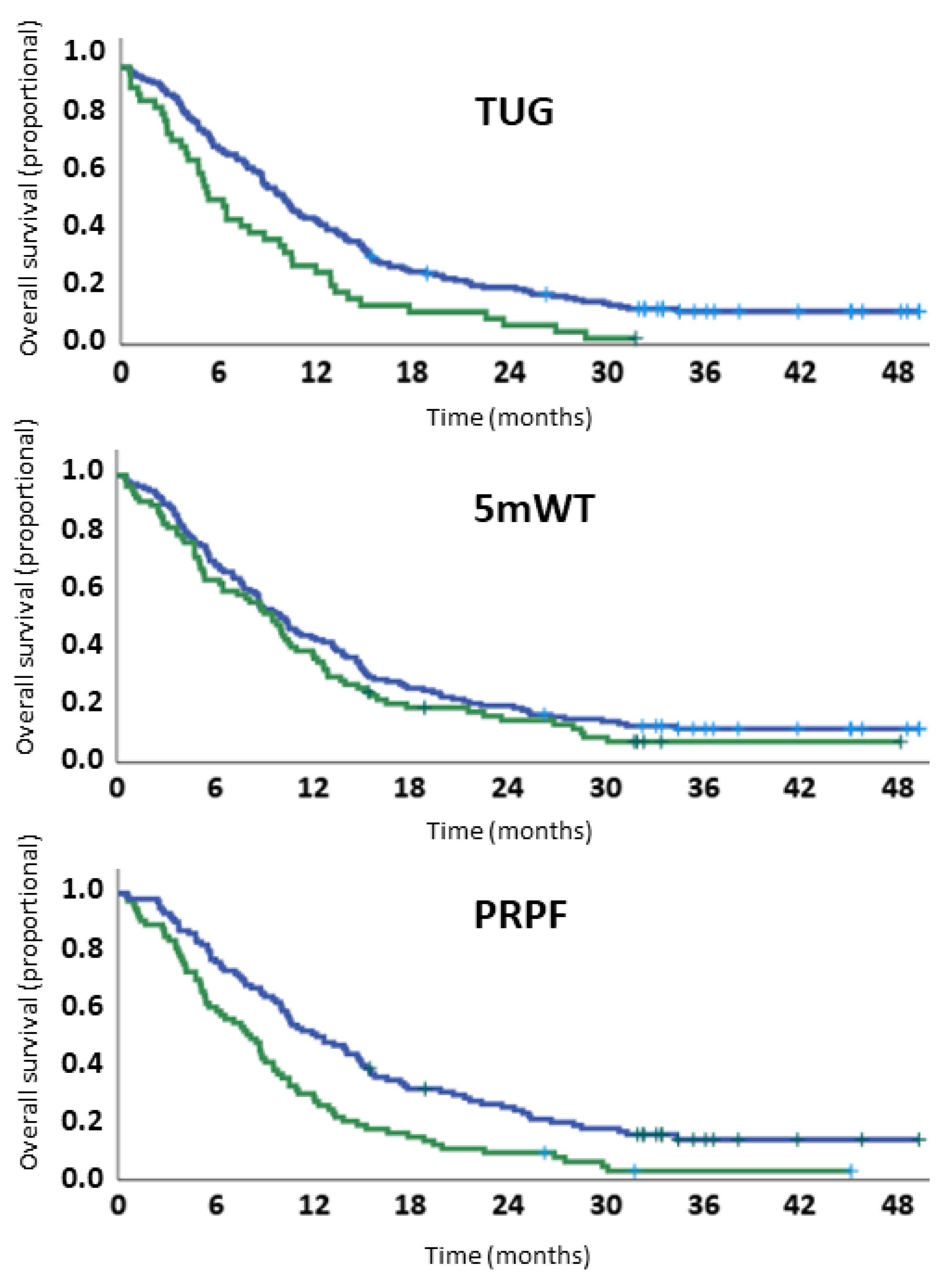
3.7. Overall Survival
3.8. Disease Control
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cancer in Norway. Available online: https://www.kreftregisteret.no/ (accessed on 26 January 2022).
- Gandhi, L.; Rodríguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus Chemotherapy in Metastatic Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef] [PubMed]
- Hesketh, P.J.; Lilenbaum, R.C.; Chansky, K.; Dowlati, A.; Graham, P.; Chapman, R.A.; Crowley, J.J.; Gandara, D.R. Chemotherapy in patients > or =80 with advanced non-small cell lung cancer: Combined results from SWOG 0027 and LUN 6. J. Thorac. Oncol. 2007, 2, 494–498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Waart, H.; Stuiver, M.M.; van Harten, W.H.; Geleijn, E.; Kieffer, J.M.; Buffart, L.M.; de Maaker-Berkhof, M.; Boven, E.; Schrama, J.; Geenen, M.M.; et al. Effect of Low-Intensity Physical Activity and Moderate- to High-Intensity Physical Exercise During Adjuvant Chemotherapy on Physical Fitness, Fatigue, and Chemotherapy Completion Rates: Results of the PACES Randomized Clinical Trial. J. Clin. Oncol. 2015, 33, 1918–1927. [Google Scholar] [CrossRef] [Green Version]
- Hardikar, S.; Newcomb, P.A.; Campbell, P.T.; Win, A.K.; Lindor, N.M.; Buchanan, D.D.; Makar, K.W.; Jenkins, M.A.; Potter, J.D.; Phipps, A.I. Prediagnostic Physical Activity and Colorectal Cancer Survival: Overall and Stratified by Tumor Characteristics. Cancer Epidemiol. Biomarkers Prev. 2015, 24, 1130–1137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Honecker, F.U.; Wedding, U.; Rettig, K.; Huschens, S.; Bokemeyer, C. Use of the Comprehensive Geriatric Assessment (CGA) in elderly patients (pts) with solid tumors to predict mortality. J. Clin. Oncol. 2009, 27 (Suppl. 15), 9549. [Google Scholar] [CrossRef]
- Ezzatvar, Y.; Ramírez-Vélez, R.; Sáez de Asteasu, M.L.; Martínez-Velilla, N.; Zambom-Ferraresi, F.; Izquierdo, M.; García-Hermoso, A. Physical Function and All-Cause Mortality in Older Adults Diagnosed With Cancer: A Systematic Review and Meta-Analysis. J. Gerontol. A Biol. Sci. Med. Sci. 2021, 76, 1447–1453. [Google Scholar] [CrossRef]
- Verweij, N.M.; Schiphorst, A.H.W.; Pronk, A.; Bos, F.V.D.; Hamaker, M.E. Physical performance measures for predicting outcome in cancer patients: A systematic review. Acta Oncol. 2016, 55, 1386–1391. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Mathias, S.; Nayak, U.S.; Isaacs, B. Balance in elderly patients: The “get-up and go” test. Arch. Phys. Med. Rehabil. 1986, 67, 387–389. [Google Scholar]
- Soubeyran, P.; Fonck, M.; Blanc-Bisson, C.; Blanc, J.-F.; Ceccaldi, J.; Mertens, C.; Imbert, Y.; Cany, L.; Vogt, L.; Dauba, J.; et al. Predictors of early death risk in older patients treated with first-line chemotherapy for cancer. J. Clin. Oncol. 2012, 30, 1829–1834. [Google Scholar] [CrossRef]
- Halvorsen, T.O.; Stokke, K.; Killingberg, K.T.; Raj, S.X.; Sørhaug, S.; Brustugun, O.T.; Fløtten, Ø.; Helbekkmo, N.; Hornslien, K.; Madebo, T.; et al. Randomized phase III trial comparing switch-maintenance pemetrexed with observation followed by pemetrexed at progression in advanced NSCLC. Acta Oncol. 2020, 59, 1051–1057. [Google Scholar] [CrossRef] [PubMed]
- Wilson, C.M.; Kostsuca, S.R.; Boura, J.A. Utilization of a 5-Meter Walk Test in Evaluating Self-selected Gait Speed during Preoperative Screening of Patients Scheduled for Cardiac Surgery. Cardiopulm. Phys. Ther. J. 2013, 24, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Fayers, P.M.; Aaronson, N.K.; Bjordal, K.; Groenvold, M.; Curran, D.; Bottomley, A.; on behalf of the EORTC Quality of Life Group. The EORTC QLQ-C30 Scoring Manual, 3rd ed.; European Organisation for Research and Treatment of Cancer: Brussels, Belgium, 2001. [Google Scholar]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C.; et al. The European Organization for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Cesari, M.; Kritchevsky, S.B.; Penninx, B.W.; Nicklas, B.J.; Simonsick, E.M.; Newman, A.B.; Tylavsky, F.A.; Brach, J.S.; Satterfield, S.; Bauer, D.C.; et al. Prognostic value of usual gait speed in well-functioning older people—Results from the Health, Aging and Body Composition Study. J. Am. Geriatr. Soc. 2005, 53, 1675–1680. [Google Scholar] [CrossRef] [Green Version]
- Bohannon, R.W. Reference values for the timed up and go test: A descriptive meta-analysis. J. Geriatr. Phys. Ther. 2006, 29, 64–68. [Google Scholar] [CrossRef] [Green Version]
- Osoba, D.; Bezjak, A.; Brundage, M.; Zee, B.; Tu, D.; Pater, J. Quality of Life Committee of the NCIC CTG. Analysis and interpretation of health-related quality-of-life data from clinical trials: Basic approach of The National Cancer Institute of Canada Clinical Trials Group. Eur. J. Cancer 2005, 41, 280–287. [Google Scholar] [CrossRef]
- Biesma, B.; Wymenga, A.N.; Vincent, A.; Dalesio, O.; Smit, H.J.; Stigt, J.A.; Smit, E.F.; van Felius, C.L.; van Putten, J.W.; Slaets, J.P.; et al. Quality of life, geriatric assessment and survival in elderly patients with non-small-cell lung cancer treated with carboplatin-gemcitabine or carboplatin-paclitaxel: NVALT-3 a phase III study. Ann. Oncol. 2011, 22, 1520–1527. [Google Scholar] [CrossRef]
- Kanesvaran, R.; Li, H.; Koo, K.-N.; Poon, D. Analysis of prognostic factors of comprehensive geriatric assessment and development of a clinical scoring system in elderly Asian patients with cancer. J. Clin. Oncol. 2011, 29, 3620–3627. [Google Scholar] [CrossRef]
- Klepin, H.D.; Geiger, A.M.; Tooze, J.A.; Newman, A.B.; Colbert, L.H.; Bauer, D.C.; Satterfield, S.; Pavon, J.; Kritchevsky, S. Physical performance and subsequent disability and survival in older adults with malignancy: Results from the health, aging and body composition study. J. Am. Geriatr. Soc. 2010, 58, 76–82. [Google Scholar] [CrossRef] [Green Version]
- Pamoukdjian, F.; Aparicio, T.; Zebachi, S.; Zelek, L.; Paillaud, E.; Canoui-Poitrine, F. Comparison of Mobility Indices for Predicting Early Death in Older Patients With Cancer: The Physical Frailty in Elderly Cancer Cohort Study. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Puts, M.T.; Monette, J.; Girre, V.; Pepe, C.; Monette, M.; Assouline, S.; Panasci, L.; Basik, M.; Miller, W.H.; Batist, G.; et al. Are frailty markers useful for predicting treatment toxicity and mortality in older newly diagnosed cancer patients? Results from a prospective pilot study. Crit. Rev. Oncol. Hematol. 2011, 78, 138–149. [Google Scholar] [CrossRef] [PubMed]
- Aregui, A.; Pluvy, J.; Sanchez, M.; Israel, T.; Esnault, H.; Guyard, A.; Meyer, M.; Khalil, A.; Zalcman, G.; Raynaud Simon, A.; et al. Measuring Walking Speed Failed to Predict Early Death and Toxicity in Elderly Patients with Metastatic Non-Small-Cell Lung Cancer (NSCLC) Selected for Undergoing First-Line Systemic Treatment: An Observational Exploratory Study. Cancers 2022, 14, 1344. [Google Scholar] [CrossRef] [PubMed]
- Kenny, R.A.; Coen, R.F.; Frewen, J.; Donoghue, O.A.; Cronin, H.; Savva, G.M. Normative values of cognitive and physical function in older adults: Findings from the Irish Longitudinal Study on Ageing. J. Am. Geriatr. Soc. 2013, 61 (Suppl. 2), S279–S290. [Google Scholar] [CrossRef]
- de Mol, M.; Visser, S.; Aerts, J.; Lodder, P.; van Walree, N.; Belderbos, H.; den Oudsten, B. The association of depressive symptoms, personality traits, and sociodemographic factors with health-related quality of life and quality of life in patients with advanced-stage lung cancer: An observational multi-center cohort study. BMC Cancer 2020, 20, 431. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TUG | 5 mWT | PRPF | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| <10 s | ≥10 s | <5 s | ≥5 s | ≥73.3 | <73.3 | ||||||||||||||||
| n | % | Median (Range) | n | % | n | % | p | Median (Range) | n | % | n | % | p | Mean (95% CI) | n | % | n | % | p | ||
| TUG | 208 | (100%) | 7.8 (0.7–44.2) | 166 | (80%) | 42 | (20%) | ||||||||||||||
| 5 mWT | 208 | (100%) | 4.5 (1.8–28.1) | 131 | (63%) | 77 | (37%) | ||||||||||||||
| PRPF | 173 | (83%) | 72.2 (69.3–75.2) | 100 | (58%) | 73 | (42%) | ||||||||||||||
| Age | Median (range) | 67 | (46–83) | 66 | (46–83) | 69 | (55–83) | 0.03 | 66 | (46–83) | 69 | (51–83) | 0.03 | 68 | (66–69) | 66 | (65–67) | 0.17 | |||
| Sex | Male | 96 | (46%) | 8.0 (2.6–27.4) | 78 | (47%) | 18 | (43%) | 4.2 (1.8–28.1) | 62 | (47%) | 34 | (44%) | 75.9 (71.8–79.9) | 48 | (48%) | 31 | (42%) | |||
| Female | 112 | (54%) | 7.6 (0.7–44.2) | 88 | (53%) | 24 | (57%) | 0.63 | 4.5 (2.0–24.7) | 69 | (53%) | 43 | (56%) | 0.66 | 69.2 (65.0–73.3) | 52 | (52%) | 42 | (58%) | 0.47 | |
| Stage | IIIB | 13 | (6%) | 7.7 (3.6–10.0) | 13 | (15%) | - | - | 4.2 (2.6–9.5) | 9 | (7%) | 4 | (5%) | 83.0 (74.2–91.8) | 9 | (9%) | 2 | (3%) | |||
| IV | 195 | (94%) | 7.8 (0.7–44.2) | 153 | (85%) | 42 | (100%) | 0.08 | 4.5 (1.8–28.1) | 122 | (93%) | 73 | (95%) | 0.63 | 71.5 (68.4–74.6) | 91 | (91%) | 71 | (97%) | 0.10 | |
| WHO PS | 0 | 66 | (32%) | 7.2 (2.6–19.6) | 58 | (35%) | 8 | (19%) | 4.4 (1.8–14.0) | 44 | (34%) | 22 | (29%) | 78.5(72.9–84.2) | 36 | (36%) | 16 | (22%) | |||
| 1 | 112 | (54%) | 7.8 (0.7–13.5) | 93 | (56%) | 19 | (45%) | 4.1 (2.1–14.0) | 77 | (59%) | 35 | (45%) | 72.7 (69.3–76.2) | 56 | (56%) | 37 | (51%) | ||||
| 2 | 30 | (14%) | 10.7 (6.8–44.2) | 15 | (9%) | 15 | (36%) | <0.01 | 6.1 (3.0–28.1) | 10 | (7%) | 20 | (26%) | <0.01 | 58.8 (50.3–67.3) | 8 | (8%) | 20 | (27%) | <0.01 | |
| Completed 4 induction courses | No | 62 | (30%) | 8.2 (0.7–25.9) | 43 | (26%) | 19 | (42%) | 4.6 (2.5–24.7) | 36 | (27%) | 26 | (34%) | 67.8 (61.6–73.9) | 26 | (26%) | 28 | (38%) | |||
| Yes | 146 | (70%) | 7.7 (2.3–44.2) | 123 | (74%) | 23 | (58%) | 0.01 | 4.3 (1.8–28.1) | 95 | (63%) | 51 | (66%) | 0.34 | 74.2 (71.0–77.5) | 74 | (74%) | 45 | (62%) | 0.08 | |
| Randomization | No | 111 | (53%) | 8.2 (0.7–44.2) | 80 | (48%) | 31 | (74%) | 4.6 (1.8–24.7) | 66 | (50%) | 45 | (58%) | 69.3 (65.1–73.6) | 46 | (46%) | 44 | (60%) | |||
| Yes | 97 | (47%) | 7.7 (2.3–27.4) | 86 | (52%) | 11 | (27%) | <0.01 | 4.2 (2.0–28.1) | 65 | (50%) | 32 | (42%) | 0.26 | 75.4 (71.3–79.4) | 54 | (54%) | 29 | (40%) | 0.06 | |
| -Observation | 47 | (23%) | 7.7 (2.9–12.6) | 43 | (26%) | 4 | (10%) | 4.2 (2.5–11.6) | 30 | (23%) | 17 | (22%) | 75.2 (68.6–81.9) | 26 | (26%) | 14 | (19%) | ||||
| -Maintenance | 50 | (24%) | 7.4 (2.3–27.4) | 43 | (26%) | 7 | (17%) | 0.39 | 4.3 (2.0–28.1) | 35 | (27%) | 15 | (20%) | 0.52 | 75.5 (70–5–80.5) | 28 | (28%) | 15 | (21%) | 1.00 | |
| Post-study immunotherapy | No | 163 | (78%) | 7.9 (0.7–44.2) | 126 | (76%) | 37 | (88%) | 4.5 (1.8–28.1) | 100 | (76%) | 63 | (82%) | 69.9 (66.6–73.2) | 72 | (72%) | 64 | (83%) | |||
| Yes | 45 | (22%) | 7.0 (2.3–12.6) | 40 | (24%) | 5 | (12%) | 0.09 | 4.2 (2.1–13.2) | 31 | (24%) | 14 | (18%) | 0.35 | 80.9 (75.0–86.7) | 28 | (28%) | 9 | (17%) | 0.01 | |
| Univariable Analysis | Multivariable Model with TUG | Multivariable Model with 5 mWT | Multivariable Model with PRPF | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | (%) | HR | 95% CI | p-Value | HR | 95% CI | p-Value | HR | 95% CI | p-Value | HR | 95% CI | p-Value | ||
| TUG * | 208 | (100%) | 1.05 | 1.02–1.08 | <0.01 | 1.03 | 0.99–1.07 | 0.18 | |||||||
| 5 mWT * | 208 | (100%) | 1.05 | 1.01–1.10 | 0.03 | 1.04 | 0.99–1.09 | 0.13 | |||||||
| PRPF * | 173 | (83%) | 1.01 | 1.01–1.02 | <0.01 | 1.01 | 1.00–1.02 | 0.03 | |||||||
| Age * | 208 | (100%) | 1.00 | 0.98–1.02 | 0.94 | 0.99 | 0.97–1.01 | 0.99 | 0.99 | 0.97–1.01 | 0.99 | 0.96 | 0.97–1.02 | 0.67 | |
| Sex | Male | 96 | (46%) | 1 | 1 | 1 | 1 | ||||||||
| Female | 112 | (54%) | 1.13 | 0.84–1.50 | 0.42 | 1.09 | 0.81–1.45 | 0.58 | 1.08 | 0.81–1.45 | 0.61 | 1.06 | 0.76–1.49 | 0.73 | |
| Stage of disease | IIIB | 13 | (6%) | 1 | 1 | 1 | 1 | ||||||||
| IV | 195 | (94%) | 1.55 | 0.86–2.78 | 0.14 | 1.51 | 0.82–2.76 | 0.19 | 1.50 | 0.82–2.74 | 0.19 | 1.21 | 0.65–2.28 | 0.55 | |
| WHO PS | 0 | 66 | (32%) | 1 | 1 | 1 | 1 | ||||||||
| 1 | 112 | (54%) | 1.45 | 1.04–2.02 | 0.03 | 1.51 | 1.07–2.12 | 0.02 | 1.56 | 1.11–2.19 | 0.01 | 1.38 | 0.94–2.02 | 0.10 | |
| 2 | 30 | (14%) | 2.57 | 1.63–4.06 | <0.01 | 2.25 | 1.32–3.83 | <0.01 | 2.44 | 1.51–3.96 | <0.01 | 2.11 | 1.23–3.62 | <0.01 | |
| Median OS | 95% CI | HR Univariable Model | 95% CI | p | HR Multivariable Model | 95% CI | p | |
|---|---|---|---|---|---|---|---|---|
| TUG < 10 sek | 10.4 | 8.6–12.2 | 1 | 1 | ||||
| TUG ≥ 10 sek | 6.3 | 3.9–8.7 | 1.74 | 1.23–2.47 | <0.01 | 1.43 | 0.97–2.10 | 0.07 |
| 5 mWT < 5 sek | 10.4 | 8.4–12.3 | 1 | 1 | ||||
| 5 mWT ≥ 5 sek | 9.6 | 7.6–11.5 | 1.21 | 0.90–1.63 | 0.21 | 1.14 | 0.84–1.55 | 0.41 |
| PRPF ≥ median | 12.2 | 8.6–15.6 | 1 | 1 | ||||
| PRPF < median | 8.2 | 6.1–10.2 | 1.8 | 1.31–2.49 | <0.01 | 1.6 | 1.14–2.24 | <0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stokke, K.; Halvorsen, T.O.; Grønberg, B.H.; Saltvedt, I.; Slaaen, M.; Kirkevold, Ø.; Killingberg, K.T.; Sandvei, M.S. Associations between Measured and Patient-Reported Physical Function and Survival in Advanced NSCLC. Healthcare 2022, 10, 922. https://doi.org/10.3390/healthcare10050922
Stokke K, Halvorsen TO, Grønberg BH, Saltvedt I, Slaaen M, Kirkevold Ø, Killingberg KT, Sandvei MS. Associations between Measured and Patient-Reported Physical Function and Survival in Advanced NSCLC. Healthcare. 2022; 10(5):922. https://doi.org/10.3390/healthcare10050922
Chicago/Turabian StyleStokke, Kristin, Tarje Onsøien Halvorsen, Bjørn Henning Grønberg, Ingvild Saltvedt, Marit Slaaen, Øyvind Kirkevold, Kristin Toftaker Killingberg, and Marie Søfteland Sandvei. 2022. "Associations between Measured and Patient-Reported Physical Function and Survival in Advanced NSCLC" Healthcare 10, no. 5: 922. https://doi.org/10.3390/healthcare10050922
APA StyleStokke, K., Halvorsen, T. O., Grønberg, B. H., Saltvedt, I., Slaaen, M., Kirkevold, Ø., Killingberg, K. T., & Sandvei, M. S. (2022). Associations between Measured and Patient-Reported Physical Function and Survival in Advanced NSCLC. Healthcare, 10(5), 922. https://doi.org/10.3390/healthcare10050922