
A Time-Dependent Analysis of Association between Acupuncture Utilization and the Prognosis of Ischemic Stroke


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Design and Definition of Acupuncture Utilization
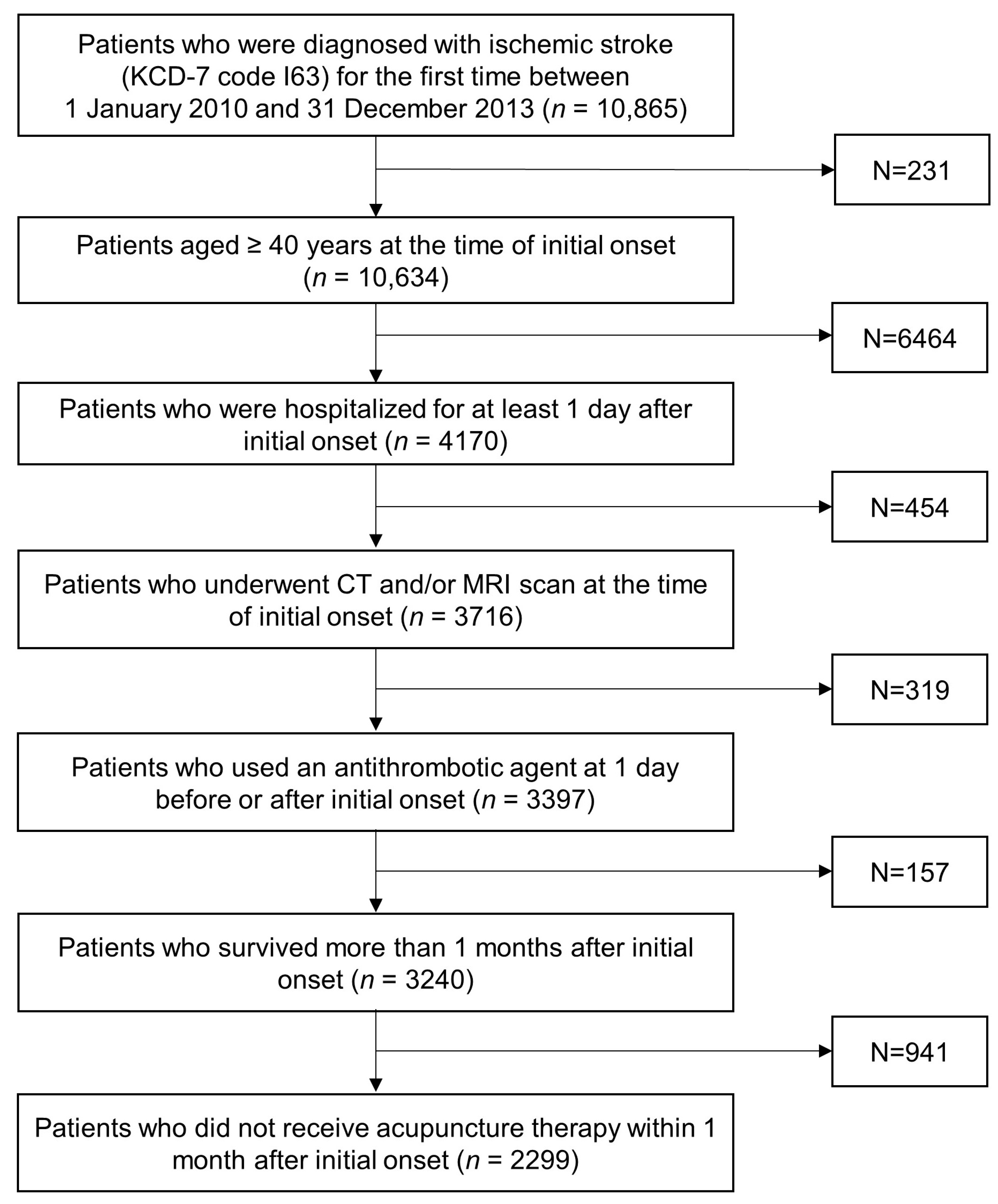
2.3. Study Population
2.4. Covariates
2.5. Outcomes
2.6. Statistical Analysis
2.7. Sensitivity Analysis
3. Results
3.1. Baseline Characteristics
3.2. Acupuncture Treatment
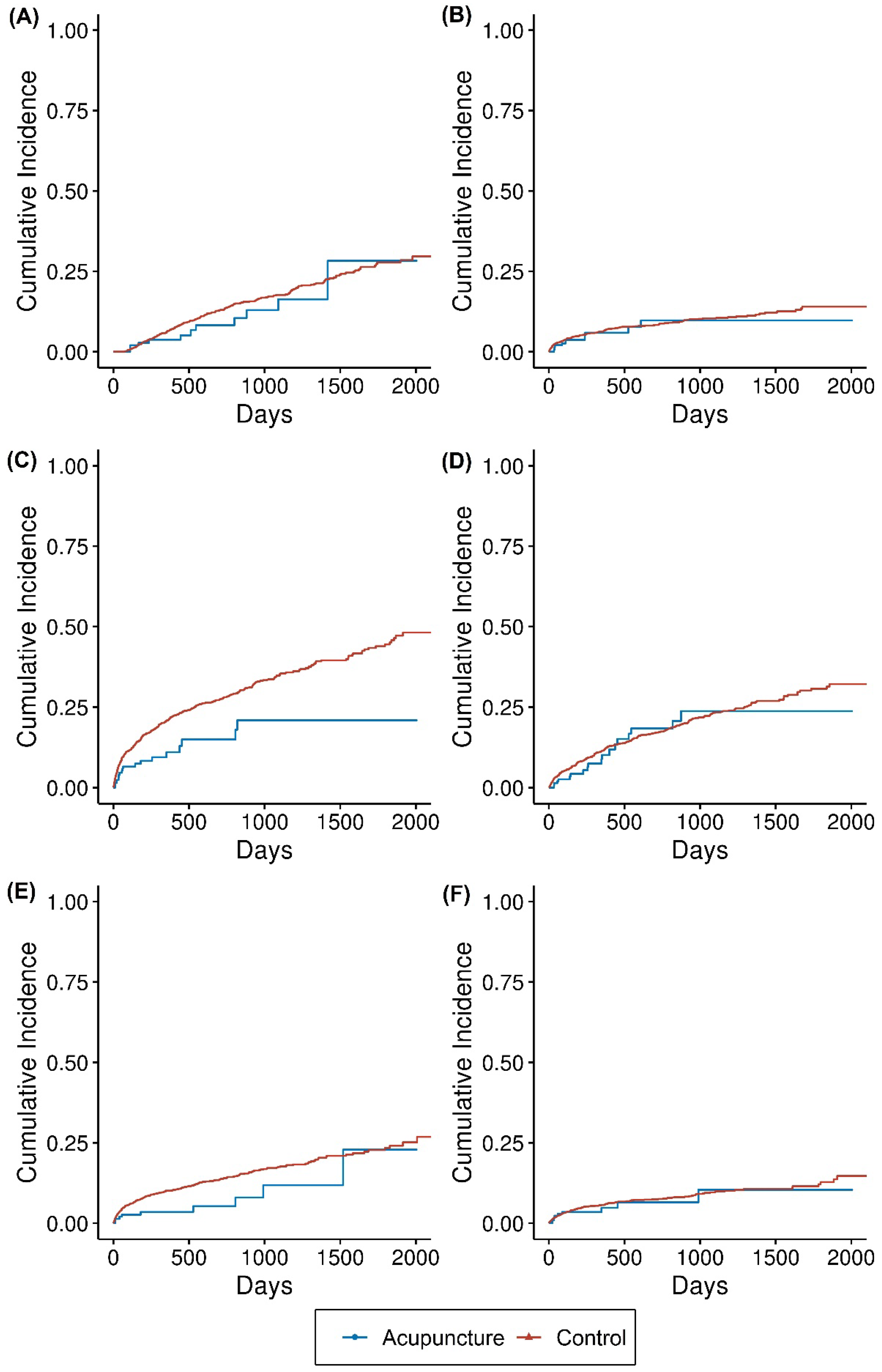
3.3. Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Phipps, M.S.; Cronin, C.A. Management of acute ischemic stroke. BMJ 2020, 368, l6983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korean Statistical Information Service. Cause-of-Death Statistics in 2020 in the Republic of Korea; Statistics Korea: Daejeon, Korea, 2021. [Google Scholar]
- Kim, J.Y.; Kang, K.; Kang, J.; Koo, J.; Kim, D.-H.; Kim, B.J.; Kim, W.-J.; Kim, E.-G.; Kim, J.G.; Kim, J.-M.; et al. Executive summary of stroke statistics in Korea 2018: A report from the epidemiology research council of the Korean Stroke Society. J. Stroke 2019, 21, 42. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.-J.; Chang, W.-L.; Tseng, M.-C. Readmission after stroke in a hospital-based registry: Risk, etiologies, and risk factors. Neurology 2011, 76, 438–443. [Google Scholar] [CrossRef] [PubMed]
- Hannawi, Y.; Hannawi, B.; Rao, C.P.V.; Suarez, J.I.; Bershad, E.M. Stroke-associated pneumonia: Major advances and obstacles. Cerebrovasc. Dis. 2013, 35, 430–443. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.B.; Lee, J.-G.; Kim, B.J.; Kim, J.Y.; Lee, K.-J.; Han, M.-K.; Park, J.-M.; Kang, K.; Cho, Y.-J.; Park, H.-K.; et al. The epidemiology of fracture in patients with acute ischemic stroke in Korea. J. Korean Med. Sci. 2017, 34, e164. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.-Y.; Yang, K.-h.; Kim, Y.N.; Moon, S.-h.; Choi, W.-J.; Kang, D.R.; Park, S.E. Incidence and mortality of hip fracture among the elderly population in South Korea: A population-based study using the national health insurance claims data. BMC Public Health 2010, 10, 230. [Google Scholar] [CrossRef] [Green Version]
- Poisson, S.N.; Johnston, S.C.; Josephson, S.A. Urinary tract infections complicating stroke: Mechanisms, consequences, and possible solutions. Stroke 2010, 41, e180–e184. [Google Scholar] [CrossRef] [Green Version]
- Amir, Y.; Halfens, R.; Lohrmann, C.; Schols, J. Pressure ulcer prevalence and quality of care in stroke patients in an Indonesian hospital. J. Wound Care 2013, 22, 254–260. [Google Scholar] [CrossRef]
- Kumar, S.; Selim, M.H.; Caplan, L.R. Medical complications after stroke. Lancet Neurol. 2010, 9, 105–118. [Google Scholar] [CrossRef]
- Yang, A.; Wu, H.M.; Tang, J.L.; Xu, L.; Yang, M.; Liu, G.J. Acupuncture for stroke rehabilitation. Cochrane Database Syst. Rev. 2016, 2016, CD004131. [Google Scholar] [CrossRef]
- Wang, H.-Q.; Hou, M.; Li, H.; Bao, C.-L.; Min, L.; Dong, G.-R.; Jiao, Z.-H. Effects of acupuncture treatment on motor function in patients with subacute hemorrhagic stroke: A randomized controlled study. Complementary Ther. Med. 2020, 49, 102296. [Google Scholar] [CrossRef] [PubMed]
- Chavez, L.M.; Huang, S.-S.; MacDonald, I.; Lin, J.-G.; Lee, Y.-C.; Chen, Y.-H. Mechanisms of acupuncture therapy in ischemic stroke rehabilitation: A literature review of basic studies. Int. J. Mol. Sci. 2017, 18, 2270. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.; Wu, B.; Liu, M.; Li, N.; Zeng, X.; Liu, H.; Yang, Q.; Han, Z.; Rao, P.; Wang, D. Acupuncture efficacy on ischemic stroke recovery: Multicenter randomized controlled trial in China. Stroke 2015, 46, 1301–1306. [Google Scholar] [CrossRef] [Green Version]
- Beyersmann, J.; Gastmeier, P.; Wolkewitz, M.; Schumacher, M. An easy mathematical proof showed that time-dependent bias inevitably leads to biased effect estimation. J. Clin. Epidemiol. 2008, 61, 1216–1221. [Google Scholar] [CrossRef] [PubMed]
- van Walraven, C.; Davis, D.; Forster, A.J.; Wells, G.A. Time-dependent bias was common in survival analyses published in leading clinical journals. J. Clin. Epidemiol. 2004, 57, 672–682. [Google Scholar] [CrossRef] [PubMed]
- Dekker, F.W.; De Mutsert, R.; Van Dijk, P.C.; Zoccali, C.; Jager, K.J. Survival analysis: Time-dependent effects and time-varying risk factors. Kidney Int. 2008, 74, 994–997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolkewitz, M.; Allignol, A.; Harbarth, S.; de Angelis, G.; Schumacher, M.; Beyersmann, J. Time-dependent study entries and exposures in cohort studies can easily be sources of different and avoidable types of bias. J. Clin. Epidemiol. 2012, 65, 1171–1180. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Lee, J.S.; Park, S.-H.; Shin, S.A.; Kim, K. Cohort profile: The national health insurance service–national sample cohort (NHIS-NSC), South Korea. Int. J. Epidemiol. 2017, 46, e15. [Google Scholar] [CrossRef]
- Lu, C.-Y.; Huang, H.-C.; Chang, H.-H.; Yang, T.-H.; Chang, C.-J.; Chang, S.-W.; Chen, P.-C. Acupuncture therapy and incidence of depression after stroke. Stroke 2017, 48, 1682–1684. [Google Scholar] [CrossRef]
- Lee, Y.-S.; Kwon, S.; Chae, Y.; Jang, B.-H.; Ko, S.-G. A retrospective cohort study on the outcomes of ischemic stroke patients with adjuvant Korean Medicine treatment. Sci. Rep. 2018, 8, 1656. [Google Scholar] [CrossRef]
- Shih, C.-C.; Liao, C.-C.; Sun, M.-F.; Su, Y.-C.; Wen, C.-P.; Morisky, D.E.; Sung, F.-C.; Hsu, C.Y.; Lin, J.-G. A retrospective cohort study comparing stroke recurrence rate in ischemic stroke patients with and without acupuncture treatment. Medicine 2015, 94, e1572. [Google Scholar] [CrossRef] [PubMed]
- Wayne, P.M.; Krebs, D.E.; Macklin, E.A.; Schnyer, R.; Kaptchuk, T.J.; Parker, S.W.; Scarborough, D.M.; McGibbon, C.A.; Schaechter, J.D.; Stein, J.; et al. Acupuncture for upper-extremity rehabilitation in chronic stroke: A randomized sham-controlled study. Arch. Phys. Med. Rehabil. 2005, 86, 2248–2255. [Google Scholar] [CrossRef]
- Hernán, M.A.; Sauer, B.C.; Hernández-Díaz, S.; Platt, R.; Shrier, I. Specifying a target trial prevents immortal time bias and other self-inflicted injuries in observational analyses. J. Clin. Epidemiol. 2016, 79, 70–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snapinn, S.M.; Jiang, Q.; Iglewicz, B. Illustrating the impact of a time-varying covariate with an extended Kaplan-Meier estimator. Am. Stat. 2005, 59, 301–307. [Google Scholar] [CrossRef]
- Yang, J.-L.; Chen, T.-L.; Yeh, C.-C.; Hu, C.-J.; Liao, C.-C.; Lane, H.-L.; Shih, C.-C. Acupuncture treatment and the risk of urinary tract infection in stroke patients: A nationwide matched cohort study. Acupunct. Med. 2019, 37, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.-C.; Chen, T.-L.; Lin, C.-S.; Chung, C.-L.; Yeh, C.-C.; Hu, C.-J.; Lane, H.-L.; Liao, C.-C.; Shih, C.-C. Decreased risk of pneumonia in stroke patients receiving acupuncture: A nationwide matched-pair retrospective cohort study. PLoS ONE 2018, 13, e0196094. [Google Scholar] [CrossRef]
- Fu, S.-P.; He, S.-Y.; Xu, B.; Hu, C.-J.; Lu, S.-F.; Shen, W.-X.; Huang, Y.; Hong, H.; Li, Q.; Wang, N.; et al. Acupuncture promotes angiogenesis after myocardial ischemia through H3K9 acetylation regulation at VEGF gene. PLoS ONE 2014, 9, e94604. [Google Scholar] [CrossRef]
- Fu, Y.; Li, J.; Wu, S.; Wang, H. Electroacupuncture pretreatment promotes angiogenesis via hypoxia-inducible factor 1α and vascular endothelial growth factor in a rat model of chronic myocardial ischemia. Acupunct. Med. 2021, 39, 367–375. [Google Scholar] [CrossRef]
- Longhurst, J.C.; Tjen-A-Looi, S. Acupuncture regulation of blood pressure: Two decades of research. Int. Rev. Neurobiol. 2013, 111, 257–271. [Google Scholar]
- Ding, N.; Jiang, J.; Xu, A.; Tang, Y.; Li, Z. Manual acupuncture regulates behavior and cerebral blood flow in the SAMP8 mouse model of Alzheimer’s disease. Front. Neurosci. 2019, 13, 37. [Google Scholar] [CrossRef] [Green Version]
- Zhu, W.; Ye, Y.; Liu, Y.; Wang, X.-R.; Shi, G.-X.; Zhang, S.; Liu, C.-Z. Mechanisms of acupuncture therapy for cerebral ischemia: An evidence-based review of clinical and animal studies on cerebral ischemia. J. Neuroimmune Pharmacol. 2017, 12, 575–592. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-H.; Hsieh, C.-L. Effect of acupuncture on oxidative stress induced by cerebral ischemia-reperfusion injury. Antioxidants 2020, 9, 248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, W.; Longhurst, J.C. Neuroendocrine mechanisms of acupuncture in the treatment of hypertension. Evid. -Based Complementary Altern. Med. 2012, 2012, 878673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuang, X.; Fan, W.; Hu, J.; Wu, L.; Yi, W.; Lu, L.; Xu, N. Acupuncture for post-stroke cognitive impairment: A systematic review and meta-analysis. Acupunct. Med. 2021, 39, 577–588. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Zhang, C.S.; Cai, Y.; Guo, X.; Zhang, A.L.; Xue, C.C.; Lu, C. Acupuncture for post-stroke shoulder-hand syndrome: A systematic review and meta-analysis. Front. Neurol. 2019, 10, 433. [Google Scholar] [CrossRef]
- Vickers, A.J.; Vertosick, E.A.; Lewith, G.; MacPherson, H.; Foster, N.E.; Sherman, K.J.; Irnich, D.; Witt, C.M.; Linde, K.; Acupuncture Trialists’ Collaboration. Acupuncture for chronic pain: Update of an individual patient data meta-analysis. J. Pain 2018, 19, 455–474. [Google Scholar] [CrossRef] [Green Version]
- Ye, Q.; Xie, Y.; Shi, J.; Xu, Z.; Ou, A.; Xu, N. Systematic review on acupuncture for treatment of dysphagia after stroke. Evid. -Based Complementary Altern. Med. 2017, 2017, 6421852. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Baseline Characteristics | Control Group | Acupuncture Group |
|---|---|---|
| (n = 2104; 91.5%) | (n = 195; 8.5%) | |
| Sex | ||
| Female | 892 (42.4) | 82 (42.1) |
| Male | 1212 (57.6) | 113 (57.9) |
| Age | ||
| Age in years | 68.5 ± 11.8 | 69.0 ± 11.1 |
| 40–50 | 137 (6.5) | 9 (4.6) |
| 50–60 | 388 (18.4) | 35 (17.9) |
| 60–70 | 500 (23.8) | 41 (21.0) |
| 70–80 | 661 (31.4) | 79 (40.5) |
| 80 and above | 418 (19.9) | 31 (15.9) |
| Income | ||
| High | 831 (39.5) | 81 (41.5) |
| Low | 608 (28.9) | 50 (25.6) |
| Mid | 665 (31.6) | 64 (32.8) |
| Residence | ||
| Metropolitan | 842 (40.0) | 84 (43.1) |
| Rural | 345 (16.4) | 25 (12.8) |
| Urban | 917 (43.6) | 86 (44.1) |
| Insurance | ||
| Beneficiary | 186 (8.8) | 16 (8.2) |
| Nonworker | 1270 (60.4) | 110 (56.4) |
| Worker | 648 (30.8) | 69 (35.4) |
| Disability | 342 (16.3) | 31 (15.9) |
| Comorbidity † | ||
| CCI | 4.3 ± 2.4 | 4.7 ± 2.1 |
| Diabetes | 1124 (53.4) | 109 (55.9) |
| Hypertension | 1665 (79.1) | 167 (85.6) |
| Hyperlipidemia | 1524 (72.4) | 143 (73.3) |
| Renal failure | 105 (5.0) | 10 (5.1) |
| Heart failure | 202 (9.6) | 24 (12.3) |
| Cancer | 644 (30.6) | 63 (32.3) |
| Mental disorder | 1117 (53.1) | 124 (63.6) |
| Cardiac arrhythmia | 130 (6.2) | 19 (9.7) |
| Osteoarthritis | 709 (33.7) | 68 (34.9) |
| Rheumatoid arthritis | 99 (4.7) | 12 (6.2) |
| Lumbar disc herniation | 225 (10.7) | 18 (9.2) |
| Pneumonia | 290 (13.8) | 34 (17.4) |
| Urinary tract infection | 186 (8.8) | 22 (11.3) |
| Intervention ‡ | ||
| Admission in tertiary hospitals | 720 (34.2) | 70 (35.9) |
| Admission day > 7 | 1328 (63.1) | 149 (76.4) |
| Nasogastric intubation | 327 (15.5) | 54 (27.7) |
| Urinary catheterization | 579 (27.5) | 86 (44.1) |
| ICU stay | 233 (11.1) | 40 (20.5) |
| Readmission after onset | 163 (7.7) | 30 (15.4) |
| Outcomes | Cases (n) | Incidence (100,000 Person-Days) | ||||
|---|---|---|---|---|---|---|
| Total | Acupuncture | Control | Total | Acupuncture | Control | |
| All-cause death | 389 | 11 | 378 | 25.1 | 13.6 | 25.7 |
| Readmission | 190 | 8 | 182 | 13 | 11 | 13.1 |
| Composite of complications | 664 | 20 | 644 | 54.2 | 35.7 | 55.1 |
| Pneumonia | 422 | 23 | 399 | 30.9 | 33.8 | 30.7 |
| Urinary tract infection | 325 | 8 | 317 | 23.4 | 11.7 | 24 |
| Decubitus ulcer | 213 | 9 | 204 | 14.5 | 12.4 | 14.6 |
| Gastrointestinal hemorrhage | 48 | 1 | 47 | 3.1 | 1.2 | 3.2 |
| Femur fracture | 48 | 1 | 47 | 3.1 | 1.3 | 3.2 |
| Outcomes | Crude HR (95% CI) | Multivariate-Adjusted HR |
|---|---|---|
| All-cause death | 0.48 (0.26–0.88) | 0.32 (0.18–0.60) |
| Readmission | 0.79 (0.39–1.62) | 0.53 (0.25–1.09) |
| Composite complications | 0.62 (0.40–0.97) | 0.34 (0.21–0.53) |
| Pneumonia | 1.09 (0.71–1.66) | 0.68 (0.44–1.04) |
| Urinary tract infection | 0.46 (0.23–0.94) | 0.24 (0.11–0.54) |
| Decubitus ulcer | 0.78 (0.40–1.53) | 0.48 (0.22–1.04) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, S.-R.; Kim, E.-S.; Jang, B.-H.; Jung, B.; Ha, I.-H. A Time-Dependent Analysis of Association between Acupuncture Utilization and the Prognosis of Ischemic Stroke. Healthcare 2022, 10, 756. https://doi.org/10.3390/healthcare10050756
Choi S-R, Kim E-S, Jang B-H, Jung B, Ha I-H. A Time-Dependent Analysis of Association between Acupuncture Utilization and the Prognosis of Ischemic Stroke. Healthcare. 2022; 10(5):756. https://doi.org/10.3390/healthcare10050756
Chicago/Turabian StyleChoi, Sung-Ryul, Eun-San Kim, Bo-Hyoung Jang, Boyoung Jung, and In-Hyuk Ha. 2022. "A Time-Dependent Analysis of Association between Acupuncture Utilization and the Prognosis of Ischemic Stroke" Healthcare 10, no. 5: 756. https://doi.org/10.3390/healthcare10050756
APA StyleChoi, S.-R., Kim, E.-S., Jang, B.-H., Jung, B., & Ha, I.-H. (2022). A Time-Dependent Analysis of Association between Acupuncture Utilization and the Prognosis of Ischemic Stroke. Healthcare, 10(5), 756. https://doi.org/10.3390/healthcare10050756