
Effects of Rhythm Step Training on Physical and Cognitive Functions in Adolescents: A Prospective Randomized Controlled Trial



Abstract
:
1. Introduction
2. Materials and Methods
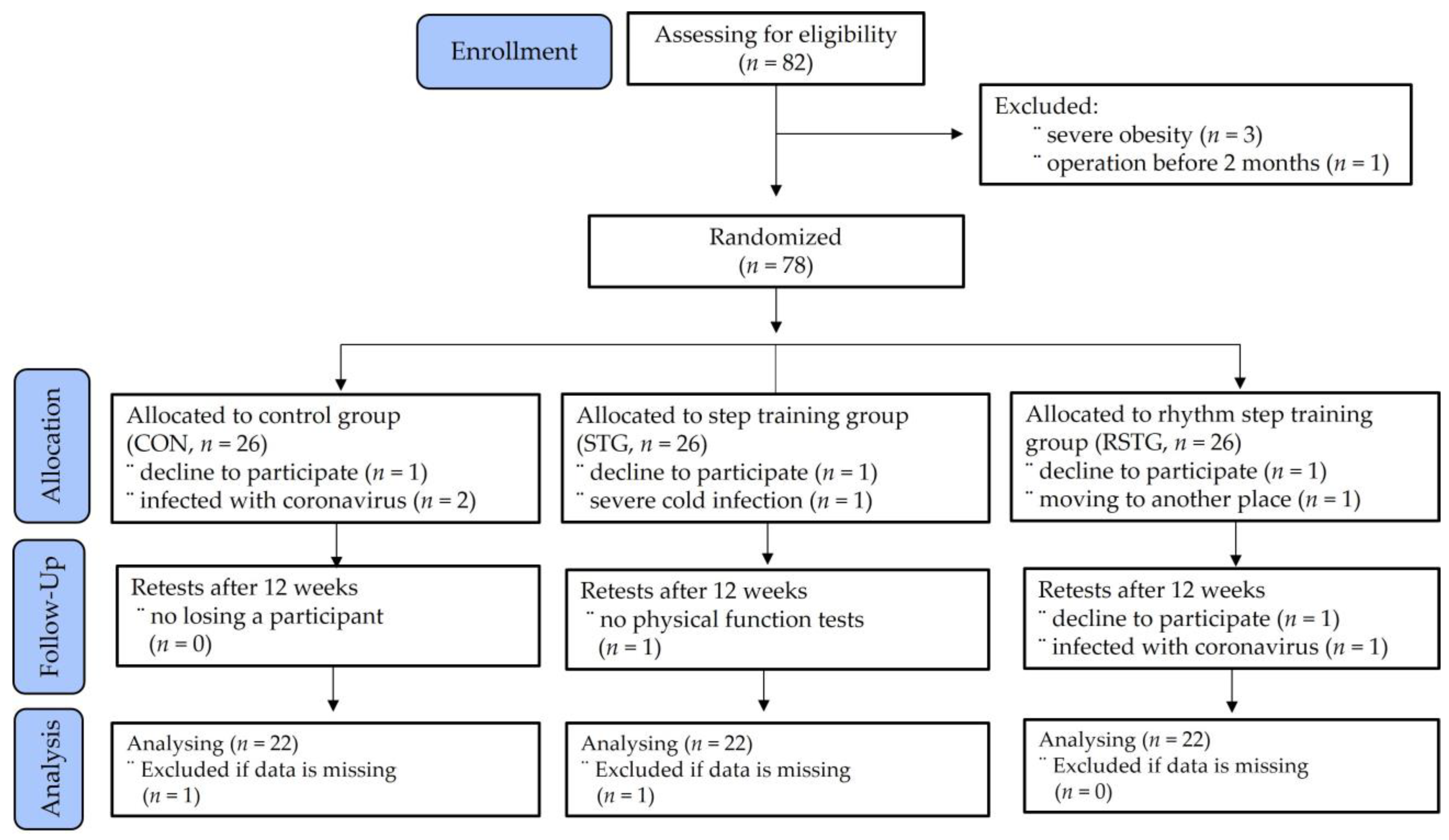
2.1. Study Design and Participants’ Characteristics
2.2. Measurement Methods
2.2.1. RST Measure
2.2.2. Physical Function Measures
2.2.3. Cognitive Function Measures
2.3. RST Program
2.4. Data Process and Statistical Analyses
3. Results
3.1. Comparisons of Demographic Data
3.2. Difference and Change in RST Ability
3.3. Effect of RST on Physical Functions
3.4. Effect of RST on Cognitive Function
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Korea Disease Control and Prevention Agency. 2017 Korea National Health and Nutrition Examination Survey; Korea Disease Control and Prevention Agency: Cheongju, Korea, 2017.
- de Figueiredo, C.S.; Sandre, P.C.; Portugal, L.C.L.; Mázala-de-Oliveira, T.; da Silva Chagas, L.; Raony, Í.; Ferreira, E.S.; Giestal-de-Araujo, E.; Dos Santos, A.A.; Bomfim, P.O. COVID-19 pandemic impact on children and adolescents’ mental health: Biological, environmental, and social factors. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 106, 110171. [Google Scholar] [CrossRef] [PubMed]
- Francesca, L.; Michele, D.C.; Milena, M.; Roberto, C. The impact of an extracurricular outdoor physical activity program on long-term memory in adolescent during COVID-19 pandemic. J. Hum. Sport Exerc. 2021, 16, S1114–S1125. [Google Scholar] [CrossRef]
- Franco, I.; Bianco, A.; Bonfiglio, C.; Sorino, P.; Mirizzi, A.; Campanella, A.; Buongiorno, C.; Liuzzi, R.; Osella, A.R. Decreased levels of physical activity: Results from a cross-sectional study in southern Italy during the COVID-19 lockdown. J. Sports Med. Phys. Fit. 2021, 61, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Jee, Y.S. How much exercise do we need to improve our immune system?: Second series of scientific evidence. J. Exerc. Rehabil. 2020, 16, 113–114. [Google Scholar] [CrossRef]
- Lee, K.S.; Heo, S.J.; Hyun, G.S.; Park, S.K.; Cha, J.Y.; Jee, Y.S. Elbow plank exercise improves immunocyte function and physical fitness in an elderly male: A case study. J. Mens Health 2022, 18, 84. [Google Scholar] [CrossRef]
- Park, S.K.; Lee, K.S.; Heo, S.J.; Jee, Y.S. Effects of high intensity plank exercise on physical fitness and immunocyte function in a middle-aged man: A case report. Medicina 2021, 57, 845. [Google Scholar] [CrossRef]
- Cataldi, S.; Francavilla, V.C.; Bonavolontà, V.; De Florio, O.; Carvutto, R.; De Candia, M.; Latino, F.; Fischetti, F. Proposal for a Fitness Program in the School Setting during the COVID 19 Pandemic: Effects of an 8-Week CrossFit Program on Psychophysical Well-Being in Healthy Adolescents. Int. J. Environ. Res. Public Health 2021, 18, 3141. [Google Scholar] [CrossRef]
- Wollesen, B.; Janssen, T.I.; Müller, H.; Voelcker-Rehage, C. Effects of cognitive-motor dual task training on cognitive and physical performance in healthy children and adolescents: A scoping review. Acta Psychol. 2022, 224, 103498. [Google Scholar] [CrossRef]
- Xiang, M.; Zhang, Z.; Kuwahara, K. Impact of COVID-19 pandemic on children and adolescents’ lifestyle behavior larger than expected. Prog. Cardiovasc. Dis. 2020, 63, 531. [Google Scholar] [CrossRef]
- Priest, D.L.; Karageorghis, C.I.; Sharp, N.C. The characteristics and effects of motivational music in exercise settings: The possible influence of gender, age, frequency of attendance, and time of attendance. J. Sports Med. Phys. Fit. 2004, 44, 77–86. [Google Scholar]
- Tabei, K.I.; Satoh, M.; Ogawa, J.I.; Tokita, T.; Nakaguchi, N.; Nakao, K.; Kida, H.; Tomimoto, H. Physical Exercise with Music Reduces Gray and White Matter Loss in the Frontal Cortex of Elderly People: The Mihama-Kiho Scan Project. Front. Aging Neurosci. 2017, 9, 174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, F.C.; Li, H.C.; Wang, H.H. The Effect of Group Music Therapy with Physical Activities to Prevent Frailty in Older People Living in the Community. Int. J. Environ. Res. Public Health 2021, 18, 8791. [Google Scholar] [CrossRef] [PubMed]
- Jo, G.; Rossow-Kimball, B.; Lee, Y. Effects of 12-week combined exercise program on self-efficacy, physical activity level, and health related physical fitness of adults with intellectual disability. J Exerc Rehabil. 2018, 14, 175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, C.; Yao, M.; Kang, M.; Duan, G. Improving physical fitness of children with intellectual and developmental disabilities through an adapted rhythmic gymnastics program in China. BioMed Res. Int. 2020, 2020, 2345607. [Google Scholar] [CrossRef] [PubMed]
- Yamada, M.; Tanaka, B.; Nagai, K.; Aoyama, T.; Ichihashi, N. Rhythmic stepping exercise under cognitive conditions improves fall risk factors in community-dwelling older adults: Preliminary results of a cluster-randomized controlled trial. Aging Ment. Health 2011, 15, 647–653. [Google Scholar] [CrossRef]
- Shah, T.; Verdile, G.; Sohrabi, H.; Campbell, A.; Putland, E.; Cheetham, C.; Dhaliwal, S.; Weinborn, M.; Maruff, P.; Darby, D.; et al. A combination of physical activity and computerized brain training improves verbal memory and increases cerebral glucose metabolism in the elderly. Transl. Psychiatry 2014, 4, e487. [Google Scholar] [CrossRef] [Green Version]
- Sok, S.; Shin, E.; Kim, S.; Kim, M. Effects of Cognitive/Exercise Dual-Task Program on the Cognitive Function, Health Status, Depression, and Life Satisfaction of the Elderly Living in the Community. Int. J. Environ. Res. Public Health 2021, 18, 7848. [Google Scholar] [CrossRef]
- Park, Y.S.; Koh, K.; Yang, J.S.; Shim, J.K. Efficacy of rhythmic exercise and walking exercise in older adults’ exercise participation rates and physical function outcomes. Geriatr. Gerontol. Int. 2017, 17, 2311–2318. [Google Scholar] [CrossRef]
- Cao, Y.; Zhang, C.; Guo, R.; Zhang, D.; Wang, S. Performances of the Canadian Agility and Movement Skill Assessment (CAMSA), and validity of timing components in comparison with three commonly used agility tests in Chinese boys: An exploratory study. PeerJ 2020, 8, e8784. [Google Scholar] [CrossRef]
- Logan, S.W.; Barnett, L.M.; Goodway, J.D.; Stodden, D.F. Comparison of performance on process- and product-oriented assessments of fundamental motor skills across childhood. J. Sports Sci. 2017, 35, 634–641. [Google Scholar] [CrossRef]
- Longmuir, P.E.; Boyer, C.; Lloyd, M.; Borghese, M.M.; Knight, E.; Saunders, T.J.; Boiarskaia, E.; Zhu, W.; Tremblay, M.S. Canadian Agility and Movement Skill Assessment (CAMSA): Validity, objectivity, and reliability evidence for children 8–12 years of age. J. Sport Health Sci. 2017, 6, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Morita, N.; Yamauchi, J.; Kurihara, T.; Fukuoka, R.; Otsuka, M.; Okuda, T.; Ishizawa, N.; Nakajima, T.; Nakamichi, R.; Matsuno, S.; et al. Toe flexor strength and foot arch height in children. Med. Sci. Sports Exerc. 2015, 47, 350–356. [Google Scholar] [CrossRef] [PubMed]
- Alvim, F.C.; Lucareli, P.R.G.; Menegaldo, L.L. Predicting muscle forces during the propulsion phase of single leg triple hop test. Gait Posture 2018, 59, 298–303. [Google Scholar] [CrossRef]
- Fu, C.L.A.; Yung, S.H.P.; Law, K.Y.B.; Leung, K.H.H.; Lui, P.Y.P.; Siu, H.K.; Chan, K.M. The effect of early whole-body vibration therapy on neuromuscular control after anterior cruciate ligament reconstruction: A randomized controlled trial. Am. J. Sports Med. 2013, 41, 804–814. [Google Scholar] [CrossRef] [PubMed]
- Buckley, S.L.; Barrack, R.L.; Alexander, A.H. The natural history of conservatively treated partial anterior cruciate ligament tears. Am. J. Sports Med. 1989, 17, 221–225. [Google Scholar] [CrossRef]
- Neto, W.K.; Soares, E.G.; Vieira, T.L.; Aguiar, R.; Chola, T.A.; Sampaio, V.L.; Gama, E.F. Gluteus Maximus Activation during Common Strength and Hypertrophy Exercises: A Systematic Review. J. Sports Sci. Med. 2020, 19, 195–203. [Google Scholar]
- Grinberg, Y.; Berkowitz, S.; Hershkovitz, L.; Malcay, O.; Kalron, A. The ability of the instrumented tandem walking tests to discriminate fully ambulatory people with MS from healthy adults. Gait Posture 2019, 70, 90–94. [Google Scholar] [CrossRef]
- Jaffri, A.H.; Saliba, S. Does verbal encouragement change dynamic balance? The effect of verbal encouragement on Star Excursion Balance Test performance in chronic ankle Instability. Braz. J. Phys. Ther. 2021, 25, 617–622. [Google Scholar] [CrossRef]
- Woo, J.I.; Kim, K.W.; Kim, S.Y.; Kim, J.H.; Woo, S.I.; Yoon, J.C.; Lee, K.W.; Lee, K.H.; Lee, D.Y.; Lee, J.H.; et al. The Korean Version of CERAD Clinical Assessment Battery; Seoul National University Publishing and Culture Center: Seoul, Korea, 2003; pp. 168–193. [Google Scholar]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Wolters Kluwer Health: Philadelphia, PA, USA, 2018. [Google Scholar]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G* Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Pardos-Mainer, E.; Lozano, D.; Torrontegui-Duarte, M.; Cartón-Llorente, A.; Roso-Moliner, A. Effects of Strength vs. Plyometric Training Programs on Vertical Jumping, Linear Sprint and Change of Direction Speed Performance in Female Soccer Players: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 401. [Google Scholar] [CrossRef]
- Aloui, G.; Hermassi, S.; Khemiri, A.; Bartels, T.; Hayes, L.D.; Bouhafs, E.G.; Souhaiel, C.M.; Schwesig, R. An 8-Week Program of Plyometrics and Sprints with Changes of Direction Improved Anaerobic Fitness in Young Male Soccer Players. Int. J. Environ. Res. Public Health 2021, 18, 10446. [Google Scholar] [CrossRef] [PubMed]
- Kraemer, W.J.; Fleck, S.J. Strength Training for Young Athletes; Human Kinetics: Champaign, IL, USA, 2005. [Google Scholar]
- Aloui, G.; Hermassi, S.; Hammami, M.; Cherni, Y.; Gaamouri, N.; Shephard, R.J.; van den Tillaar, R.; Chelly, M.S. Effects of Elastic Band Based Plyometric Exercise on Explosive Muscular Performance and Change of Direction Abilities of Male Team Handball Players. Front. Physiol. 2020, 11, 604983. [Google Scholar] [CrossRef]
- Aloui, G.; Hermassi, S.; Hayes, L.D.; Sanal Hayes, N.E.; Bouhafs, E.G.; Chelly, M.S.; Schwesig, R. Effects of plyometric and short sprint with change-of-direction training in male U17 soccer players. Appl. Sci. 2021, 11, 4767. [Google Scholar] [CrossRef]
- Markovic, G.; Mikulic, P. Neuro-musculoskeletal and performance adaptations to lower-extremity plyometric training. Sports Med. 2010, 40, 859–895. [Google Scholar] [CrossRef] [PubMed]
- Jlid, M.C.; Coquart, J.; Maffulli, N.; Paillard, T.; Bisciotti, G.N.; Chamari, K. Effects of in Season Multi-Directional Plyometric Training on Vertical Jump Performance, Change of Direction Speed and Dynamic Postural Control in U-21 Soccer Players. Front. Physiol. 2020, 11, 374. [Google Scholar] [CrossRef]
- You, S.H.; Jang, S.H.; Kim, Y.H.; Hallett, M.; Ahn, S.H.; Kwon, Y.H.; Kim, J.H.; Lee, M.Y. Virtual reality–induced cortical reorganization and associated locomotor recovery in chronic stroke: An experimenter-blind randomized study. Stroke 2005, 36, 1166–1171. [Google Scholar] [CrossRef] [Green Version]
- Leroux, A.; Fung, J.; Barbeau, H. Postural adaptation to walking on inclined surfaces: I. Normal strategies. Gait Posture 2002, 15, 64–74. [Google Scholar] [CrossRef]
- Karabin, M.J.; Sparto, P.J.; Rosano, C.; Redfern, M.S. Impact of strength and balance on Functional Gait Assessment performance in older adults. Gait Posture 2022, 91, 306–311. [Google Scholar] [CrossRef]
- Cotman, C.W.; Berchtold, N.C. Exercise: A behavioral intervention to enhance brain health and plasticity. Trends Neurosci. 2002, 25, 295–301. [Google Scholar] [CrossRef]
- Gates, N.J.; Valenzuela, M.; Sachdev, P.S.; Singh, N.A.; Baune, B.T.; Brodaty, H.; Suo, C.; Jain, N.; Wilson, G.C.; Wang, Y.; et al. Study of Mental Activity and Regular Training (SMART) in at risk individuals: A randomised double blind, sham controlled, longitudinal trial. BMC Geriatr. 2011, 11, 19. [Google Scholar] [CrossRef] [Green Version]
- Broadhouse, K.M.; Singh, M.F.; Suo, C.; Gates, N.; Wen, W.; Brodaty, H.; Jain, N.; Wilson, G.C.; Meiklejohn, J.; Singh, N.; et al. Hippocampal plasticity underpins long-term cognitive gains from resistance exercise in MCI. NeuroImage Clin. 2020, 25, 102182. [Google Scholar] [CrossRef] [PubMed]
- Griffin, É.W.; Mullally, S.; Foley, C.; Warmington, S.A.; O’Mara, S.M.; Kelly, Á.M. Aerobic exercise improves hippocampal function and increases BDNF in the serum of young adult males. Physiol. Behav. 2011, 104, 934–941. [Google Scholar] [CrossRef] [PubMed]
- Erickson, K.I.; Voss, M.W.; Prakash, R.S.; Basak, C.; Szabo, A.; Chaddock, L.; Kim, J.S.; Heo, S.; Alves, H.; White, S.M.; et al. Exercise training increases size of hippocampus and improves memory. Proc. Natl. Acad. Sci. USA 2011, 108, 3017–3022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hillman, C.H.; Erickson, K.I.; Kramer, A.F. Be smart, exercise your heart: Exercise effects on brain and cognition. Nat. Rev. Neurosci. 2008, 9, 58–65. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Items | Scale | Forward Step | Sidestep | One Leg Step | Side to Sidestep | Zigzag Step |
|---|---|---|---|---|---|---|
| Time (s) | 0 | >10.5 | >11.75 | >8.25 | >11.5 | >16.5 |
| 1 | 9–10.5 | 9.75–11.75 | 7.25–8.25 | 9.5–11.5 | 14.5–16.5 | |
| 2 | 7.5–9 | 7.75–9.75 | 6.25–7.25 | 7.5–9.5 | 12.5–14.5 | |
| 3 | 6–7.5 | 5.75–7.75 | 5.25–6.25 | 5.5–7.5 | 10.5–12.5 | |
| 4 | <6 | <5.75 | <5.25 | <5.5 | <10.5 | |
| Inaccuracy (reps.) | 0 | ≥4 | ≥4 | ≥4 | ≥4 | ≥7 |
| 1 | 3 | 3 | 3 | 3 | 5–6 | |
| 2 | 2 | 2 | 2 | 2 | 3–4 | |
| 3 | 1 | 1 | 1 | 1 | 1–2 | |
| 4 | 0 | 0 | 0 | 0 | 0 |
| Exercise Types | ET | RPE | |
|---|---|---|---|
| Warmup | Stretching for whole body | 10 min | 7–9 |
| Workout | ① Forward direction: jump step, two feet jump step ② Backward direction: jump step, two feet jump step ③ Side direction: jump step, two feet jump step, sit to jump ④ Hop and two feet jump step ⑤ Cross direction: jump step, two feet jump step ⑥ Parallel cross: jump step, two feet jump step ⑦ Parallel direction: jump step, two feet jump step ⑧ Turn 360°: jump step, two feet jump step ⑨ Side to side: jump step, two feet jump step ⑩ Heel-up and two feet jump step ⑪ Creative rhythm jump step | 25 min | 12–14 |
| Cooldown | Stretching for whole body | 10 min | 7–9 |
| Groups | |||||
|---|---|---|---|---|---|
| CON (n = 22) | STG (n = 22) | RSTG (n = 22) | F | p | |
| Age (y) | 14.82 ± 0.80 | 14.68 ± 0.84 | 14.41 ± 0.96 | 2.652 | 0.078 |
| Height (cm) | 158.23 ± 5.44 | 158.55 ± 4.48 | 159.68 ± 4.29 | 0.567 | 0.570 |
| Weight (kg) | 60.36 ± 12.29 | 55.64 ± 9.60 | 54.73 ± 9.20 | 1.850 | 0.166 |
| Percent fat (%) | 24.14 ± 5.03 | 22.00 ± 3.52 | 21.45 ± 3.66 | 2.597 | 0.082 |
| BMI (kg/m2) | 20.60 ± 8.20 | 19.81 ± 5.92 | 23.31 ± 5.74 | 1.655 | 0.199 |
| Time (T) | Groups (G) | F (p) | ||||||
|---|---|---|---|---|---|---|---|---|
| CON | STG | RSTG | T | G | G × T | η2 | ||
| RST ability | pre | 28.36 ± 4.34 | 29.59 ± 4.34 | 30.64 ± 5.94 | 114.506 | 2.705 | 7.570 | 0.036 |
| post | 29.45 ± 4.58 | 32.00 ± 4.58 *** | 33.59 ± 4.76 *** | (<0.001) | (0.075) | (<0.001) | 0.136 | |
| Time (T) | Groups (G) | F (p) | ||||||
|---|---|---|---|---|---|---|---|---|
| CON | STG | RSTG | T | G | G × T | |||
| One leg hop (cm) | pre | 413.41 ± 56.49 | 443.14 ± 56.49 | 432.32 ± 81.15 | 334.261 (<0.001) | 1.255 (0.292) | 45.920 (<0.001) | |
| post | 416.00 ± 56.92 *** | 447.82 ± 56.92 *** | 441.95 ± 80.24 *** | |||||
| Carioca (s) | pre | 14.15 ± 4.55 | 14.25 ± 4.55 | 15.60 ± 3.99 | 367.167 (<0.001) | 0.217 (0.805) | 71.845 (<0.001) | |
| post | 13.72 ± 4.40 *** | 13.46 ± 4.40 *** | 13.61 ± 3.96 *** | |||||
| Cross over step up (rep/min) | pre | 69.71 ± 7.77 | 69.59 ± 7.14 | 71.32 ± 12.71 | 365.150 (<0.001) | 0.468 (0.628) | 15.812 (<0.001) | |
| post | 71.32 ± 7.63 *** | 72.05 ± 6.85 *** | 74.73 ± 12.36 *** | |||||
| Tandem walk (s) | pre | 21.34 ± 6.05 | 18.56 ± 6.05 | 19.94 ± 4.65 | 279.514 (<0.001) | 3.035 (0.055) | 37.188 (<0.001) | |
| post | 20.99 ± 5.86 * | 17.01 ± 5.86 *** | 18.10 ± 4.27 *** | |||||
| SEBT (cm) | Anterior | pre | 57.18 ± 4.56 | 58.73 ± 4.56 | 57.86 ± 4.37 | 413.799 (<0.001) | 0.980 (0.381) | 19.934 (<0.001) |
| post | 58.07 ± 4.52 *** | 60.25 ± 4.52 *** | 59.86 ± 4.26 *** | |||||
| Anterolateral | pre | 58.32 ± 5.56 | 58.34 ± 5.56 | 57.64 ± 5.79 | 233.837 (<0.001) | 0.031 (0.970) | 16.975 (<0.001) | |
| post | 59.23 ± 5.31 *** | 59.91 ± 5.31 *** | 60.07 ± 5.15 *** | |||||
| Lateral | pre | 58.07 ± 6.06 | 58.20 ± 6.06 | 57.89 ± 7.25 | 398.957 (<0.001) | 0.087 (0.917) | 13.335 (<0.001) | |
| post | 59.27 ± 5.86 *** | 60.45 ± 5.86 *** | 60.64 ± 6.44 *** | |||||
| Posterolateral | pre | 60.80 ± 7.14 | 60.68 ± 7.14 | 62.32 ± 7.37 | 161.165 (<0.001) | 0.820 (0.445) | 9.601 (<0.001) | |
| post | 61.75 ± 6.71 *** | 62.43 ± 6.71 *** | 64.70 ± 6.36 *** | |||||
| Posterior | pre | 63.86 ± 8.82 | 66.45 ± 8.82 | 64.64 ± 9.21 | 116.612 (<0.001) | 0.775 (0.465) | 6.648 (0.002) | |
| post | 64.93 ± 7.98 *** | 68.20 ± 7.98 *** | 67.18 ± 8.22 *** | |||||
| Posteromedial | pre | 61.95 ± 8.24 | 64.20 ± 8.24 | 63.16 ± 11.16 | 87.397 (<0.001) | 0.656 (0.522) | 5.665 (0.005) | |
| post | 62.91 ± 7.79 *** | 66.20 ± 7.79 *** | 65.70 ± 10.01 *** | |||||
| Medial | pre | 54.68 ± 8.12 | 56.23 ± 8.12 | 55.70 ± 9.83 | 179.408 (<0.001) | 0.404 (0.670) | 5.503 (0.006) | |
| post | 56.18 ± 8.01 *** | 58.75 ± 8.01 *** | 58.52 ± 8.70 *** | |||||
| Anteromedial | pre | 53.59 ± 5.50 | 52.16 ± 5.50 | 52.50 ± 7.72 | 233.340 (<0.001) | 0.218 (0.804) | 4.303 (0.018) | |
| post | 55.25 ± 5.26 *** | 54.34 ± 5.26 *** | 55.18 ± 6.87 *** | |||||
| Gait ability | Cadence (rep/min) | pre | 113.20 ± 10.85 | 115.04 ± 5.50 | 109.95 ± 9.18 | 96.761 (<0.001) | 2.195 (0.120) | 20.885 (<0.001) |
| post | 114.52 ± 10.63 *** | 115.74 ± 5.48 *** | 110.11 ± 9.13 | |||||
| Velocity (m/sec) | pre | 1.06 ± 0.15 | 1.14 ± 0.14 | 1.13 ± 0.22 | 98.975 (<0.001) | 1.377 (0.260) | 6.789 (0.002) | |
| post | 1.07 ± 0.15 *** | 1.15 ± 0.14 *** | 1.15 ± 0.22 *** | |||||
| Stride length (m) | pre | 1.18 ± 0.16 | 1.18 ± 0.12 | 1.15 ± 0.14 | 1.189 (0.280) | 0.055 (0.947) | 0.469 (0.628) | |
| post | 1.18 ± 0.10 | 1.20 ± 0.12 | 1.21 ± 0.15 | |||||
| Time (T) | Groups (G) | F (p) | ||||||
|---|---|---|---|---|---|---|---|---|
| CON | STG | RSTG | T | G | G × T | η2 | ||
| Verbal memory | pre | 67.50 ± 12.03 | 65.91 ± 12.03 | 65.95 ± 11.61 | 105.178 | 0.021 | 6.576 | 0.005 |
| post | 69.27 ± 10.53 * | 69.64 ± 10.53 *** | 70.59 ± 10.84 *** | (<0.001) | (0.980) | (0.003) | 0.003 | |
| Attention (s) | pre | 22.55 ± 3.79 | 22.45 ± 3.79 | 25.14 ± 5.63 | 207.471 | 1.355 | 14.355 | 0.066 |
| post | 21.23 ± 3.69 *** | 21.18 ± 3.69 *** | 22.45 ± 4.65 *** | (<0.001) | (0.265) | (<0.001) | 0.019 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.-K.; Jee, Y.-S. Effects of Rhythm Step Training on Physical and Cognitive Functions in Adolescents: A Prospective Randomized Controlled Trial. Healthcare 2022, 10, 712. https://doi.org/10.3390/healthcare10040712
Park S-K, Jee Y-S. Effects of Rhythm Step Training on Physical and Cognitive Functions in Adolescents: A Prospective Randomized Controlled Trial. Healthcare. 2022; 10(4):712. https://doi.org/10.3390/healthcare10040712
Chicago/Turabian StylePark, Sang-Kyun, and Yong-Seok Jee. 2022. "Effects of Rhythm Step Training on Physical and Cognitive Functions in Adolescents: A Prospective Randomized Controlled Trial" Healthcare 10, no. 4: 712. https://doi.org/10.3390/healthcare10040712
APA StylePark, S.-K., & Jee, Y.-S. (2022). Effects of Rhythm Step Training on Physical and Cognitive Functions in Adolescents: A Prospective Randomized Controlled Trial. Healthcare, 10(4), 712. https://doi.org/10.3390/healthcare10040712