
Efficacy of Four-Channel Functional Electrical Stimulation on Moderate Arm Paresis in Subacute Stroke Patients—Results from a Randomized Controlled Trial

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Inclusion Criteria
2.3. Exclusion Criteria
- Implanted defibrillators, brain stimulators, pacemakers, and drug pumps;
- Severe contractures in the treatment area;
- Wounds in the stimulation area;
- Pregnancy.
2.4. Randomization
2.5. Intervention
2.6. EMG-MES
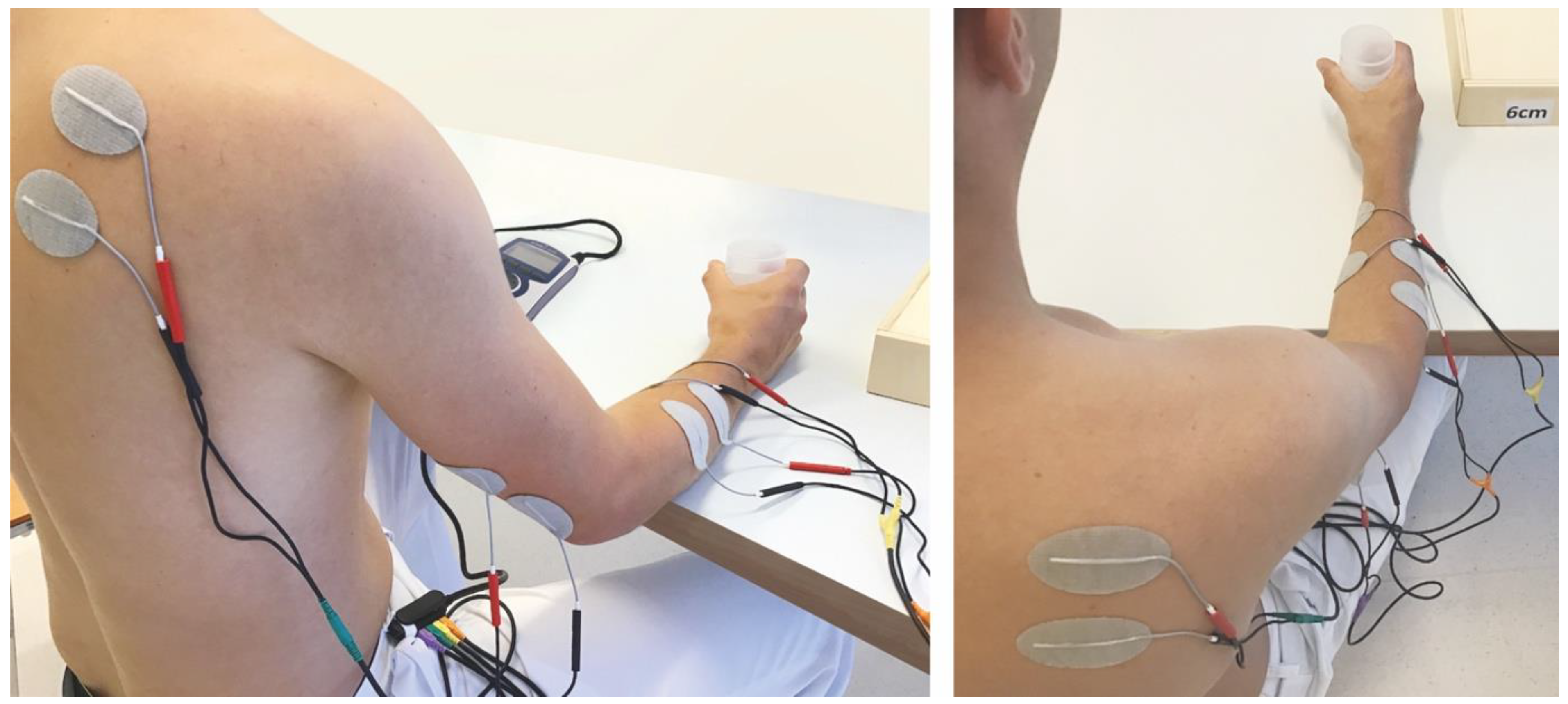
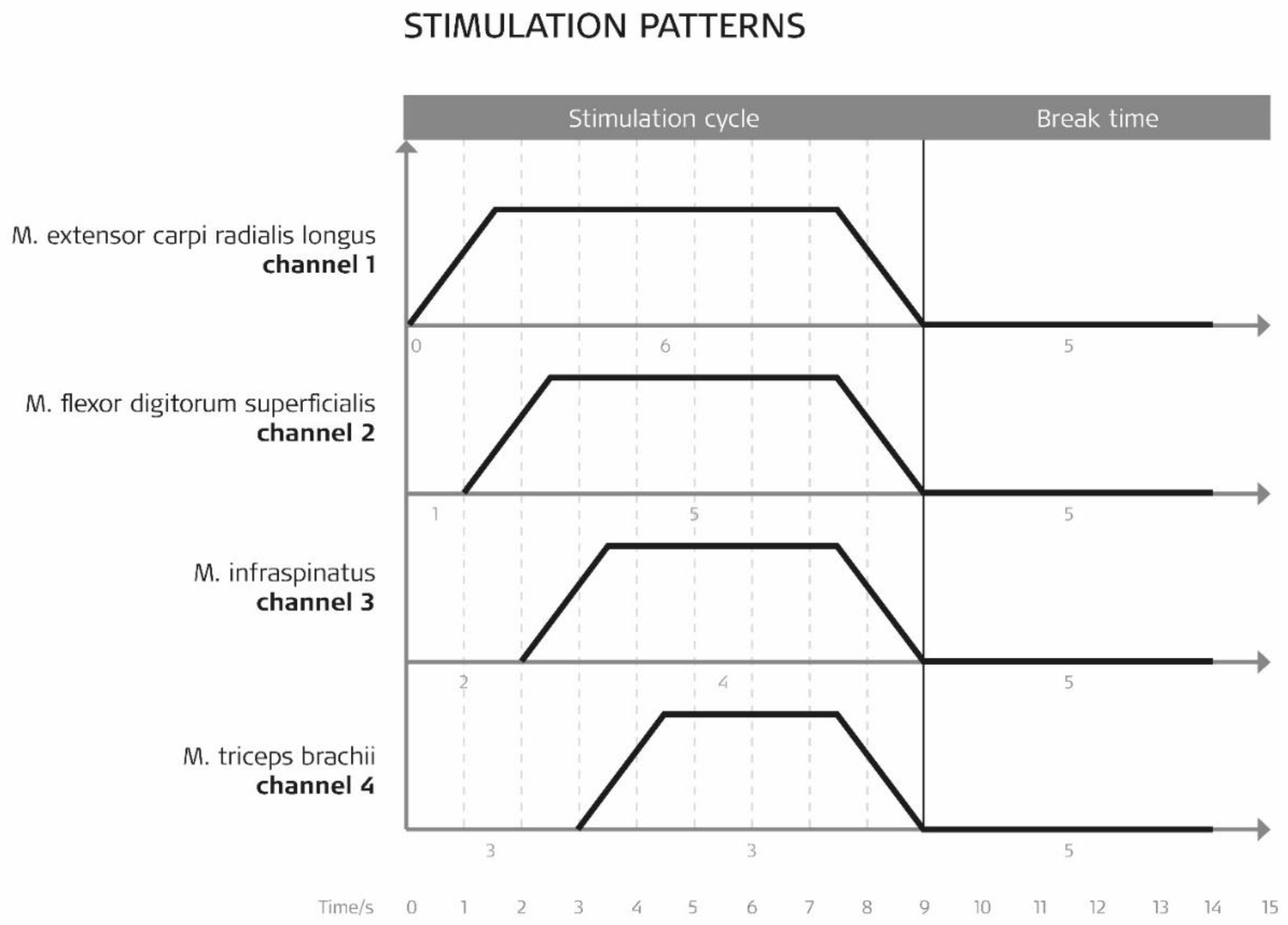
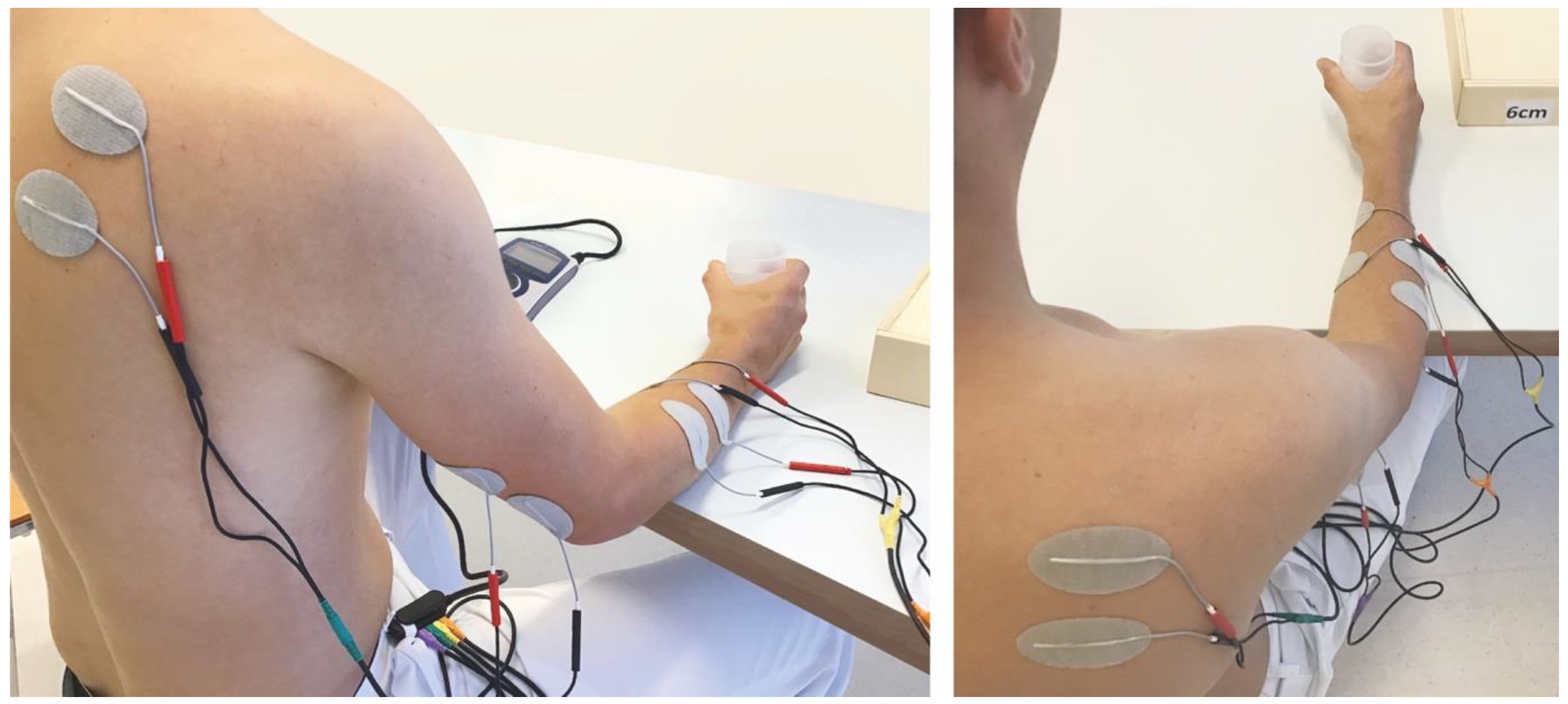
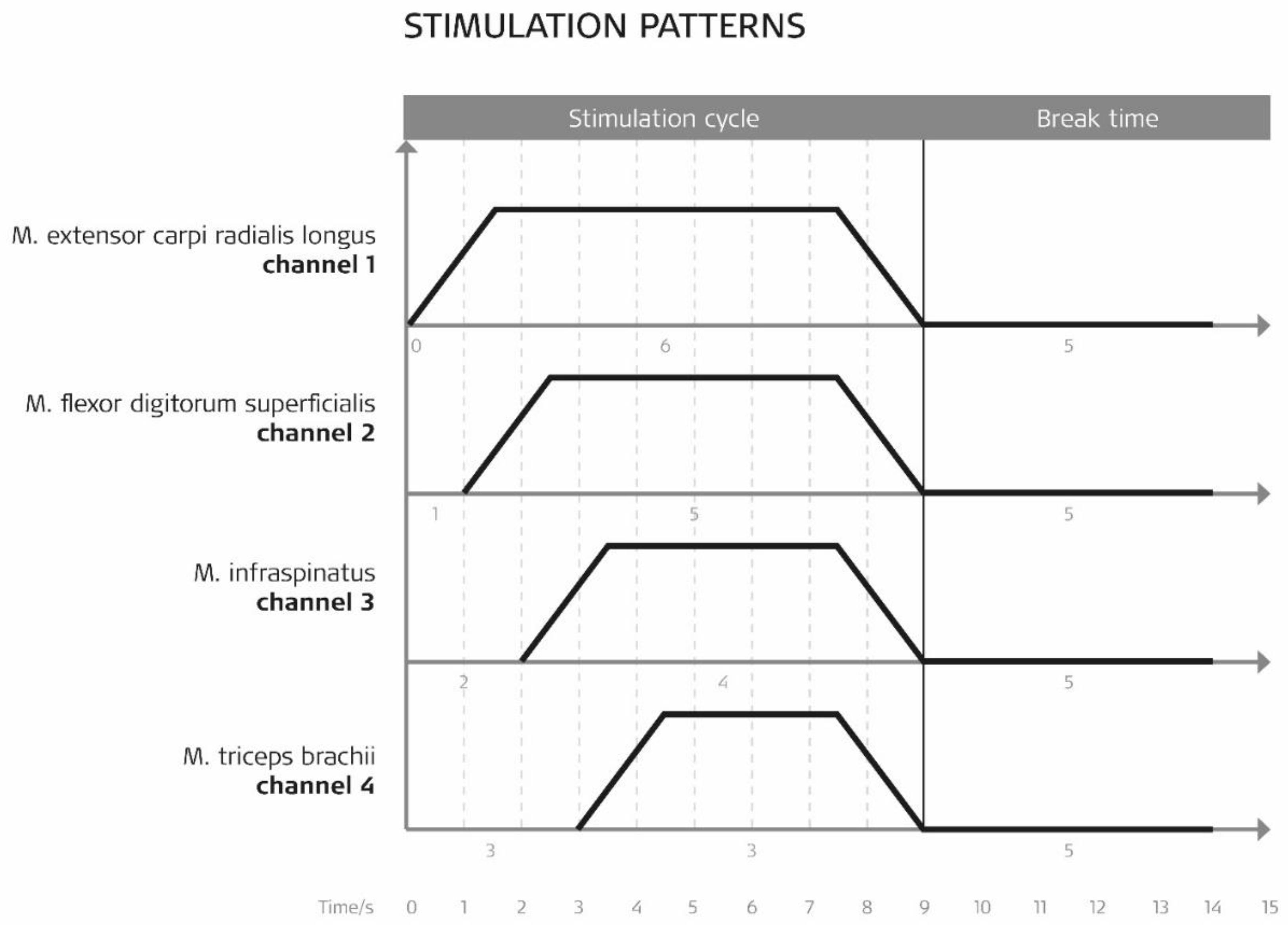
2.7. cNMES
2.8. Outcome Measures
- Fugl-Meyer Assessment Arm Section Score (FMA-AS)—blinded video rating;
- Box and Block Test (BBT);
- Stroke Impact Scale (SIS)—German version.
2.9. Data Analysis
2.10. A-Posteriori Power Calculation
3. Results
3.1. Participant Characteristics
3.2. Therapy Effects: Primary Outcomes
3.3. Therapy Effects: Secondary Outcomes
3.4. Adverse Events
4. Discussion
4.1. Limitation of the Study
4.2. Directions for Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Feigin, V.L.; Forouzanfar, M.H.; Krishnamurthi, R.; Mensah, G.A.; Connor, M.; Bennett, D.A.; Moran, A.E.; Sacco, R.L.; Anderson, L.; Truelsen, T.; et al. Global and regional burden of stroke during 1990–2010: Findings from the Global Burden of Disease Study 2010. Lancet 2014, 383, 245–255. [Google Scholar] [CrossRef]
- Houwink, A.; Nijland, R.H.; Geurts, A.C.; Kwakkel, G. Functional Recovery of the Paretic Upper Limb After Stroke: Who Regains Hand Capacity? Arch. Phys. Med. Rehabil. 2013, 94, 839–844. [Google Scholar] [CrossRef]
- Sullivan, K.J.; Tilson, J.K.; Cen, S.Y.; Rose, D.K.; Hershberg, J.; Correa, A.; Gallichio, J.; McLeod, M.; Moore, C.; Wu, S.S.; et al. Fugl-Meyer assessment of sensorimotor function after stroke: Standardized training procedure for clinical practice and clinical trials. Stroke 2011, 42, 427–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fugl-Meyer, A.R.; Jääskö, L.; Leyman, I.; Olsson, S.; Steglind, S. The post-stroke hemiplegic patient. 1. a method for evaluation of physical performance. Scand. J. Rehabil. Med. 1975, 7, 13–31. [Google Scholar] [PubMed]
- Eraifej, J.; Clark, W.; France, B.; Desando, S.; Moore, D. Effectiveness of upper limb functional electrical stimulation after stroke for the improvement of activities of daily living and motor function: A systematic review and meta-analysis. Syst. Rev. 2017, 6, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.-D.; Liao, C.-D.; Huang, S.-W.; Tam, K.-W.; Liou, T.-H.; Lee, Y.-H.; Lin, C.-Y.; Chen, H.-C. Effectiveness of electrical stimulation therapy in improving arm function after stroke: A systematic review and a meta-analysis of randomised controlled trials. Clin. Rehabil. 2019, 33, 1286–1297. [Google Scholar] [CrossRef]
- Silva, K.M.; Piscitelli, D.; Norouzi-Gheidari, N.; Batalla, M.A.P.; Archambault, P.S.; Levin, M.F. Electromyogram-Related Neuromuscular Electrical Stimulation for Restoring Wrist and Hand Movement in Poststroke Hemiplegia: A Systematic Review and Meta-Analysis. Neurorehabilit. Neural Repair 2019, 33, 96–111. [Google Scholar] [CrossRef] [PubMed]
- Howlett, O.A.; Lannin, N.; Ada, L.; McKinstry, C. Functional Electrical Stimulation Improves Activity After Stroke: A Systematic Review with Meta-Analysis. Arch. Phys. Med. Rehabil. 2015, 96, 934–943. [Google Scholar] [CrossRef]
- Cauraugh, J.; Light, K.; Kim, S.; Thigpen, M.; Behrman, A. Chronic motor dysfunction after stroke: Recovering wrist and finger extension by electromyography-triggered neuromuscular stimulation. Stroke 2000, 31, 1360–1364. [Google Scholar] [CrossRef]
- Hara, Y.; Obayashi, S.; Tsujiuchi, K.; Muraoka, Y. The effects of electromyography-controlled functional electrical stimulation on upper extremity function and cortical perfusion in stroke patients. Clin. Neurophysiol. 2013, 124, 2008–2015. [Google Scholar] [CrossRef]
- Thrasher, T.A.; Zivanovic, V.; McIlroy, W.; Popovic, M.R. Rehabilitation of Reaching and Grasping Function in Severe Hemiplegic Patients Using Functional Electrical Stimulation Therapy. Neurorehabilit. Neural Repair 2008, 22, 706–714. [Google Scholar] [CrossRef] [PubMed]
- Kapadia, N.; Moineau, B.; Popovic, M.R. Functional Electrical Stimulation Therapy for Retraining Reaching and Grasping After Spinal Cord Injury and Stroke. Front. Neurosci. 2020, 14, 718. [Google Scholar] [CrossRef] [PubMed]
- Chuang, L.-L.; Chen, Y.-L.; Chen, C.-C.; Li-Ling, C.; Wong, A.M.-K.; Hsu, A.-L.; Chang, Y.-J. Effect of EMG-triggered neuromuscular electrical stimulation with bilateral arm training on hemiplegic shoulder pain and arm function after stroke: A randomized controlled trial. J. Neuroeng. Rehabil. 2017, 14, 122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von Lewinski, F.; Hofer, S.; Kaus, J.; Merboldt, K.D.; Rothkegel, H.; Schweizer, R.; Liebetanz, D.; Frahm, J.; Paulus, W. Efficacy of EMG-triggered electrical arm stimulation in chronic hemiparetic stroke patients. Restor. Neurol. Neurosci. 2009, 27, 189–197. [Google Scholar] [CrossRef]
- Schick, T.; Schlake, H.-P.; Kallusky, J.; Hohlfeld, G.; Steinmetz, M.; Tripp, F.; Krakow, K.; Pinter, M.; Dohle, C. Synergy effects of combined multichannel EMG-triggered electrical stimulation and mirror therapy in subacute stroke patients with severe or very severe arm/hand paresis. Restor. Neurol. Neurosci. 2017, 35, 319–332. [Google Scholar] [CrossRef] [PubMed]
- Jonsdottir, J.; Thorsen, R.; Aprile, I.; Galeri, S.; Spannocchi, G.; Beghi, E.; Bianchi, E.; Montesano, A.; Ferrarin, M. Arm rehabilitation in post stroke subjects: A randomized controlled trial on the efficacy of myoelectrically driven FES applied in a task-oriented approach. PLoS ONE 2017, 12, e0188642. [Google Scholar] [CrossRef]
- Doucet, B.M.; Lam, A.; Griffin, L. Neuromuscular electrical stimulation for skeletal muscle function. Yale J. Biol. Med. 2012, 85, 201–215. [Google Scholar]
- Wilson, R.D.; Page, S.J.; Delahanty, M.; Knutson, J.S.; Gunzler, D.D.; Sheffler, L.R.; Chae, J. Upper-Limb Recovery After Stroke: A Randomized Controlled Trial Comparing EMG-Triggered, Cyclic, and Sensory Electrical Stimulation. Neurorehabil. Neural Repair 2016, 30, 978–987. [Google Scholar] [CrossRef] [Green Version]
- Woodbury, M.L.; Velozo, C.A.; Richards, L.G.; Duncan, P. Rasch Analysis Staging Methodology to Classify Upper Extremity Movement Impairment After Stroke. Arch. Phys. Med. Rehabil. 2013, 94, 1527–1533. [Google Scholar] [CrossRef]
- Bernhardt, J.; Hayward, K.; Kwakkel, G.; Ward, N.; Wolf, S.L.; Borschmann, K.; Krakauer, J.W.; Boyd, L.A.; Carmichael, S.T.; Corbett, D.; et al. Agreed definitions and a shared vision for new standards in stroke recovery research: The Stroke Recovery and Rehabilitation Roundtable taskforce. Int. J. Stroke 2017, 12, 444–450. [Google Scholar] [CrossRef]
- Schulz, K.F.; Grimes, D.A. Unequal group sizes in randomised trials: Guarding against guessing. Lancet 2002, 359, 966–970. [Google Scholar] [CrossRef]
- Rosenberger, W.F.; Lachin, J.M. Randomization in Clinical Trials: Theory and Practice; John Wiley & Sons: Hoboken, NJ, USA, 2015. [Google Scholar]
- Platz, T.; Pinkowski, C.; Van Wijck, F.; Kim, I.-H.; Di Bella, P.; Johnson, G. Reliability and validity of arm function assessment with standardized guidelines for the Fugl-Meyer Test, Action Research Arm Test and Box and Block Test: A multicentre study. Clin. Rehabil. 2005, 19, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Wirz, M.; Köhler, B.; Marks, D.; Kool, J.; Sattelmayer, M.; Oesch, P.; Hilfiker, R.; Rogan, S.; Schädler, S.; Verra, M.; et al. Assessments in der Rehabilitation, 3rd ed.; Neurologie; Verlag Hans Huber: Bern, Switzerland, 2012. [Google Scholar]
- Petersen, C.; Morfeld, M.; Bullinger, M. Testing and validation of the German version of the Stroke Impact Scale. Fortschr. Neurol Psychiatr. 2001, 69, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Platz, T.; Fheodoroff, K.; Jea, M. S3-Leitlinie Rehabilitative Therapie bei Armparese nach Schlaganfall. 2020. Available online: https://www.awmf.org/uploads/tx_szleitlinien/080-001l_S3_Rehabilitative_Therapie_bei_Armparese_nach_Schlaganfall_2020-07.pdf (accessed on 2 November 2020).
- Chipchase, L.; Schabrun, S.; Hodges, P. Peripheral electrical stimulation to induce cortical plasticity: A systematic review of stimulus parameters. Clin. Neurophysiol. 2011, 122, 456–463. [Google Scholar] [CrossRef] [Green Version]
- Golaszewski, S.M.; Bergmann, J.; Christova, M.; Kunz, A.B.; Kronbichler, M.; Rafolt, D.; Gallasch, E.; Staffen, W.; Trinka, E.; Nardone, R. Modulation of motor cortex excitability by different levels of whole-hand afferent electrical stimulation. Clin. Neurophysiol. 2012, 123, 193–199. [Google Scholar] [CrossRef]
- Alon, G. Functional electrical stimulation (FES): The science is strong, the clinical practice not yet—A review of evidence. Ann. Phys. Rehabil. Med. 2016, 59, e26–e27. [Google Scholar] [CrossRef]
- Alon, G.; Levitt, A.F.; McCarthy, P.A. Functional Electrical Stimulation Enhancement of Upper Extremity Functional Recovery During Stroke Rehabilitation: A Pilot Study. Neurorehabilit. Neural Repair 2007, 21, 207–215. [Google Scholar] [CrossRef]
- Vafadar, A.K.; Côté, J.N.; Archambault, P.S. Effectiveness of Functional Electrical Stimulation in Improving Clinical Outcomes in the Upper Arm following Stroke: A Systematic Review and Meta-Analysis. BioMed Res. Int. 2015, 2015, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Fheodoroff, K.; Kossmehl, P.; Wissel, J. Validity and Reliability of the Spasticity-Associated Arm Pain Scale. J. Pain Manag. Med. 2017, 3, 127–133. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Mean (±SD) | ||||
|---|---|---|---|---|
| IG | CG | Total | ||
| Sex | Male | 4 | 4 | 8 |
| Female | 2 | 2 | 4 | |
| Age | 68 (7) | 62 (9) | ||
| Type of stroke | Ischemic | 6 | 6 | 12 |
| Hemorrhagic | 0 | 0 | 0 | |
| Lesion | Left | 3 | 4 | 7 |
| Right | 3 | 2 | 5 | |
| Affected hand | Dominant | 3 | 4 | 7 |
| Not dominant | 3 | 2 | 5 | |
| Degree of arm paresis | Severe to moderate | 2 | 4 | 6 |
| Moderate to mild | 4 | 2 | 6 | |
| Localization of infarction | Cortical | 5 | 4 | 9 |
| Subcortical | 1 | 2 | 3 | |
| Time since stroke | Days | 63 (15) | 147 (192) * | |
| Net intervention time | Min | 23.5 (2) | 24 (1) | |
| IG (n = 6) CG (n = 6) Total (n = 12) | Mean (±SD) | Wilcoxon Signed-Rank Test *** | Mann–Whitney U-Test **** | ||||
|---|---|---|---|---|---|---|---|
| Pre | Post | Diff | Z-Value | p-Values (2-Sided) | U-Value | p-Values (2-Sided) | |
| FMA-AS total | |||||||
| IG | 33.5 (11.9) | 40.67 (10.9) | 7.17 (2.2) | −2.232 | 0.026 * | 14.500 | 0.926 |
| CG | 31.67 (5.4) | 37.67 (5.2) | 6.33 (4.5) | −2.003 | 0.045 * | ||
| FMA-AS A | |||||||
| IG | 18.83 (5.9) | 22.67 (5.7) | 4.00 (2.2) | −2.226 | 0.026 ** | 12.000 | 0.576 |
| CG | 19.50 (2.3) | 21.67 (4.2) | 2.17 (3.4) | −1.476 | 0.140 | ||
| FMA-AS B | |||||||
| IG | 5.00 (1.9) | 6.17 (1.3) | 1.17 (1.6) | −1.604 | 0.109 | 7.000 | 0.129 |
| CG | 5.00 (2.1) | 6.50 (2.7) | 1.67 (1.2) | −2.041 | 0.041 | ||
| FMA-AS C | |||||||
| IG | 7.33 (3.5) | 9.17 (3.7) | 2.33 (2.1) | −2.041 | 0.041 ** | 14.500 | 0.926 |
| CG | 6.67 (2.7) | 8.83 (2.8) | 2.33 (2.1) | −1.897 | 0.058 | ||
| FMA-AS D | |||||||
| IG | 2.33 (2.1) | 2.67 (2.5) | 0.33 (0.8) | −1.000 | 0.317 | 15.000 | 1.000 |
| CG | 0.50 (1.2) | 0.50 (1.2) | 0.00 (0.0) | 0.000 | 1.000 | ||
| IG (n = 6) CG (n = 6) Total (n = 12) | Mean (±SD) | Wilcoxon Signed-Rank Test *** | Mann-Whitney U-Test **** | ||||
|---|---|---|---|---|---|---|---|
| Pre | Post | Diff | Z-Value | p-Values (2-Sided) | U-Value | p-Values (2-Sided) | |
| BBT affected hand | |||||||
| IG | 26.00 (11.4) | 32.33 (13.1) | 7.17 (4.1) | −2.023 | 0.043 * | 14.000 | 0.520 |
| CG | 16.83 (7.1) | 27.00 (3.6) | 9.67 (5.6) | −2.207 | 0.027 * | ||
| SIS Strength | |||||||
| IG | 55.00 (22.3) | 64.58 (6.5) | 10.00 (25.2) | −0.730 | 0.465 | 12.000 | 0.579 |
| CG | 48.96 (16.5) | 51.04 (19.1) | 1.04 (12.8) | −0.557 | 0.577 | ||
| SIS ADL/IADL | |||||||
| IG | 51.67 (17.3) | 70.83 (18.1) | 19.17 (14.4) | −2.207 | 0.027 ** | 16.000 | 0.744 |
| CG | 50.42 (11.5) | 65.83 (12.5) | 15.42 (5.3) | −2.226 | 0.026 | ||
| SIS Mobility | |||||||
| IG | 64.33 (38.2) | 80.08 (26.02) | 15.75 (18.9) | −2.023 | 0.043 ** | 12.000 | 0.584 |
| CG | 75.46 (18.4) | 86.57 (10.8) | 11.11 (11.5) | −1.892 | 0.058 | ||
| SIS Hand function | |||||||
| IG | 30.83 (27.1) | 45.83 (23.5) | 15.00 (14.8) | −2.023 | 0.042 ** | 11.000 | 0.459 |
| CG | 22.50 (21.6) | 36.67 (40.5) | 14.17 (19.9) | −1.473 | 0.141 | ||
| SIS Recovery | |||||||
| IG | 49.17 (11.1) | 66.67 (13.7) | 17.50 (10.8) | −2.214 | 0.027 ** | 7.500 | 0.086 |
| CG | 47.50 (18.1) | 51.67 (20.2) | 4.17 (9.1) | −1.063 | 0.288 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schick, T.; Kolm, D.; Leitner, A.; Schober, S.; Steinmetz, M.; Fheodoroff, K. Efficacy of Four-Channel Functional Electrical Stimulation on Moderate Arm Paresis in Subacute Stroke Patients—Results from a Randomized Controlled Trial. Healthcare 2022, 10, 704. https://doi.org/10.3390/healthcare10040704
Schick T, Kolm D, Leitner A, Schober S, Steinmetz M, Fheodoroff K. Efficacy of Four-Channel Functional Electrical Stimulation on Moderate Arm Paresis in Subacute Stroke Patients—Results from a Randomized Controlled Trial. Healthcare. 2022; 10(4):704. https://doi.org/10.3390/healthcare10040704
Chicago/Turabian StyleSchick, Thomas, Daniela Kolm, Andreas Leitner, Sandra Schober, Maria Steinmetz, and Klemens Fheodoroff. 2022. "Efficacy of Four-Channel Functional Electrical Stimulation on Moderate Arm Paresis in Subacute Stroke Patients—Results from a Randomized Controlled Trial" Healthcare 10, no. 4: 704. https://doi.org/10.3390/healthcare10040704
APA StyleSchick, T., Kolm, D., Leitner, A., Schober, S., Steinmetz, M., & Fheodoroff, K. (2022). Efficacy of Four-Channel Functional Electrical Stimulation on Moderate Arm Paresis in Subacute Stroke Patients—Results from a Randomized Controlled Trial. Healthcare, 10(4), 704. https://doi.org/10.3390/healthcare10040704