Abstract
This study aimed to develop and validate an emergency nursing-care patient satisfaction scale to measure patient satisfaction with emergency room (ER) nursing. Patient satisfaction scales for ER nursing have been validated without considering the perspectives of the healthcare system or cultural background of the country. Moreover, although nursing care is changing with COVID-19, no scale has been specifically designed to assess patient satisfaction with ER nursing. The study population included patients who visited five ERs in Japan (March to December 2021) (n = 135). The rating scales were provided to patients who visited the ER and gave consent, and the patients were asked to reply. In the process of validating the scale, exploratory and confirmatory factor analyses of the construct and criterion validity were conducted. The confirmatory factor analysis results showed a factorial structure consisting of four factors. The domain and summary scores demonstrated good-to-excellent internal reliability (Cronbach’s range = 0.81–0.89). This patient satisfaction scale was designed and validated from the perspective of the Japanese healthcare system and cultural backgrounds. This scale may be useful for developing assessments and interventions to improve patient satisfaction with ER nursing.
1. Introduction
Patient response to healthcare services is one of the best ways to obtain information about the quality of healthcare [1]. In particular, patient satisfaction is an important indicator for evaluating service quality and improving healthcare services, and is a commonly used and valid indicator [2,3]. The field of medicine is divided into specialties, and specialized treatment and care are provided in each field. In measuring patient satisfaction, the development of satisfaction scales for each specialty was reported to help deal with specific problems [4]. In nursing, patient satisfaction is defined as the extent of the gap between patient expectations of ideal nursing care and their perception of the nursing care received [5]. We consider it important to use information obtained from patient satisfaction to improve care and enhance the quality of healthcare services.
Emergency nurses have multiple challenging responsibilities, including dealing with overstressed patients and their relatives, homeless and mentally ill patients, and victims [6]. In addition, emergency nurses play several roles, including triage [7], first aid [7], and early recognition of critically ill patients [8]. In recent years, emergency care has become more urgent worldwide due to the increasing severity of coronavirus disease 2019 (COVID-19) patients, increasing the burden on emergency nurses [9]. However, even during the COVID-19 pandemic, rapid and appropriate responses to emergency patients are required.
Various models have been used to measure satisfaction with emergency care [4,10,11]. The Consumer Emergency Care Satisfaction Scale (CECSS) is one of the most widely used patient satisfaction surveys for emergency patients in many countries [10]. Many studies using existing satisfaction scales have been reported for triage nurses [12,13] and have been conducted in a variety of geographic areas, ranging from urban to rural areas [14]. Factors associated with patient satisfaction with emergency care have been consistently reported in previous studies to be related to staff attitudes, explanations to patients, communication, time spent waiting in the emergency room (ER) [15,16], and environmental factors in the ER [17,18]. Satisfaction with emergency care has also been reported to be related to organizational culture [19] and healthcare professional burnout [20,21]. Therefore, measuring patient satisfaction is of great importance to healthcare professionals in the ER setting, as patient satisfaction measures can be used to identify weaknesses in their respective facilities.
However, patient satisfaction with the healthcare provided is influenced by several characteristics, such as the cultural background of the country or region [22], race [23], the healthcare system [24], the insurance system [25], the educational system for nurses [26], and the economic situation of the country [27]. Even though patient satisfaction is used in many countries, these factors limit the ability to measure patient satisfaction that reflects country-specific characteristics. In addition, a systematic review of patient satisfaction surveys reported that there is no gold standard for measuring patient satisfaction [28], and that it is necessary to develop instruments that are appropriate for the healthcare system of each country and other factors.
There are three levels of emergency hospital designation in Japan: “primary” for patients who can be managed as outpatients, “secondary” for patients who need to be hospitalized, and “tertiary” for patients who need to be managed in an intensive care unit (ICU) [29]. Japan has one of the most aged populations in the world [30], and the number of patients visiting the ER is on the rise because of the COVID-19 pandemic [31]. Moreover, Japan has had a universal health coverage system since 1961, providing equal access to healthcare for all citizens at all times [32]. Furthermore, in terms of nursing specialization, although there are specialists, such as certified nurses and certified nurse specialists, they account for approximately 1% of all nurses, and the current situation is that there is insufficient training of specialists [33]. However, the current situation in Japan differs from that in other countries. Therefore, the patient satisfaction scale for emergency nurses currently in use does not necessarily match the assessment in Japan. Furthermore, the recent COVID-19 pandemic has changed patient satisfaction in the ER. Patient satisfaction with ER staff tended to be high at the beginning of the COVID-19 pandemic. This suggests an overall appreciation for care during the early stages of the COVID-19 pandemic [34]. Furthermore, patient satisfaction with the ER has decreased during the COVID-19 pandemic due to increased workloads, such as infection control measures [15]. In addition, the COVID-19 pandemic would lead to overcrowding in the ER and lower patient satisfaction [35]. However, no scale has been developed to measure patient satisfaction with emergency nurses in Japan to the best of our knowledge. This study aimed to develop and validate a patient satisfaction scale to measure patient satisfaction with ER nursing.
2. Materials and Methods
2.1. Study Design
This study had the following steps to achieve its objectives: (1) Developing items to measure patient satisfaction with ER nursing, (2) examining content validity, (3) selecting items, and (4) examining construct validity.
- (1)
- Development of items to measure patient satisfaction with ER nursing
In this phase, we generated various items according to the different categories established by the CECSS [10] and the Patient Satisfaction Questionnaire Short Form (PSQ-18) [2]. The items were elaborated and written through four consensus meetings with consultations from experts in developing the measuring instruments. The research team consisted of eight experts: two certified nurses in emergency nursing, one certified nurse in operation nursing, three certified nurse specialists in critical care nursing, and a university professor of nursing in critical care [36]. The first version of the questionnaire was developed on the basis of the four dimensions of satisfactory care, with 34 items distributed among the four factors. Additionally, we conducted our review using the keywords “emergency care”, “emergency nursing”, and “patient satisfaction” and searched CINAHL, PubMed, Medline, and other databases in the field. As a result, 12 items were identified, and 46 items in six categories were generated.
- (2)
- Content validation
Previous studies have reported that it is desirable to reflect the opinions of experts in the field as well as patients and healthy people who are involved in the content validation process [37]. Content validation of the first questionnaire version was conducted by an expert panel of 10 healthy individuals who had visited an ER and 9 certified nurses in emergency nursing [38] (Table A1). We sent questionnaires to the panel of 19 people and asked them whether the survey items were valid. The survey items were assessed on a 4-point Likert scale ranging from 1 (“not at all important”) to 4 (“very important”). We also asked about repetition, incomprehensibility, and ease of answering. Following the method proposed by Davis, the item-level content validity index (I-CVI) was calculated by dividing the number of experts who gave a rating of three or four for each item by the total number of experts [39]. Items with an I-CVI lower than 0.78 were eliminated [40]. Numerical codes were assigned to the completed forms to ensure confidentiality and anonymity of the questionnaires. The final version of the questionnaire was established after deleting five items on the basis of content validation research analysis and the results obtained from various consensus meetings between the research team and expert advisors. The 46 items included in the first version were reduced to 39 in the final version of the emergency nursing-care patient satisfaction scale (ENPSS).
- (3)
- Selecting items
Participants
The emergency medical care system in Japan is classified into three categories: primary emergency facilities that mainly treat patients who can return home without the need for hospitalization, secondary emergency facilities that mainly treat critically ill patients who require hospitalization, and life-saving emergency centers that treat critically ill patients who require advanced treatment [41]. In this study, patients who visited primary and secondary emergency facilities were included. The patients fulfilled the following criteria to participate in the validation study:
- 1.
- Age ≥ 18 years at the time of recruitment;
- 2.
- Capable of providing consent;
- 3.
- Ability to answer questionnaires;
- 4.
- Cognitive and physical capacity to complete self-administered questionnaires without the need for a proxy.
Participants were recruited from the emergency departments of five facilities in Japan between March 2021 and December 2021. The questionnaire was distributed to patients who visited the ER and met the above criteria. The research collaborator, an emergency nurse, asked each respondent to complete the questionnaire individually.
The sample size was targeted at >100 participants based on the COnsensus-based Standards for the selection of health Measurement Instruments (COSMIN) checklist, a guideline for scale development [37,42].
Survey components
The survey consists of four components. The first was a questionnaire on individual and institutional characteristics. The second part consisted of the number of visits to the ER, the time of day when they visited the ER, and the length of time they waited in the ER. The third component consisted of the 6-item EuroQol 5 dimensions 5-level (EQ-5D-5L) [43,44] to test criterion-related validity and the intensity of distress during the ER visit and overall satisfaction in the ER. The fourth component consisted of a satisfaction survey of the nurses in the ER.
Instruments
The EQ-5D-5L is a validated and standardized instrument that measures health-related quality of life (QOL) [43,44]. A Japanese version of the EQ-5D-5L is available [45]. The EQ-5D-5L consists of the following five dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension has five levels: no problems, slight problems, moderate problems, severe problems, and extreme problems. Health status is represented in 3125 combinations, and each combination of answers can be converted into a QOL score, ranging from 0 (death) to 1 (perfect health), according to a Japanese value set [45]. We compared the scores from our study with those of a previously reported Japanese norm [46]. The EQ-5D-5L also uses a visual analog scale (VAS) ranging from 0 to 100, where 0 represents the worst imaginable health and 100 represents the best imaginable health.
To determine the content of the questions related to patient satisfaction with ER nursing, we first examined the available information from previous studies [47,48,49,50]. Second, we extracted content related to satisfaction with ER nursing. Third, on the basis of these contents, five certified nurses were interviewed. On the basis of these results, the following four items were adopted in this study, and each question was measured using the VAS with “strongly agree” as 100 and “disagree” as 0.
- Confidence in the ER’s physician;
- Satisfaction with the response of ER’s physician;
- Intensity of distress at the time of ER visit;
- Satisfaction with the outcome of treatment in the ER.
For each of the patient satisfaction surveys for nurses in the ER, respondents rated their level of agreement on a standard five-point Likert scale (0 = “not applicable”, 1 = “strongly disagree”, 2 = “slightly disagree”, 3 = “neutral”, 4 = “slightly agree”, and 5 = “strongly agree”).
2.2. Statistical Analysis
Descriptive statistics were derived for the analysis. Categorical data were expressed as numbers and percentages.
We examined some of the questionnaire items for possible exclusion according to the following criteria: items with a 20% rate or higher of “not applicable” [51] and items with an average score of 4.5, 1.5, or lower for each item. Furthermore, one of the items with a correlation coefficient of 0.7 or higher for each item was eliminated [52].
Exploratory factor analysis (EFA) using promax rotation and maximum likelihood extraction methods was conducted to determine the number and type of factors from 38 of the 39 survey items, excluding the question on overall satisfaction. EFA was conducted on the complete data for all 38 items at baseline. The factor solution from the EFA was based on the magnitude of the factor loadings for each item. On the basis of standard psychometric criteria, items with factor loadings of less than 0.35 were eliminated. The researchers assessed whether the elimination or retention of specific items was meaningful for assessing patient satisfaction.
On the basis of the results of the EFA, a confirmatory factor analysis (CFA) was used to evaluate factor solutions. The goal of the CFA was to evaluate the model fit of the factor structure using the root mean square error of approximation (RMSEA: where <0.09 is considered acceptable and <0.06 is considered excellent) and comparative fit index (CFI: where >0.9 is considered acceptable). As a result, we named each factor that represented various aspects of patient satisfaction with nursing in the ER.
The internal consistency reliability of the ENPSS was assessed using Cronbach’s alpha. The estimates of reliability should exceed 0.70 (0.7 ≤ α < 0.8 is acceptable, 0.8 ≤ α < 0.9 is good, and 0.9 ≤ α is excellent) [53,54]. Construct validity was assessed using Pearson correlations of the EFA-yielded domains and the ENPSS summary score with the five validated questionnaires, namely, EQ-5D-5L (using the VAS), anxiety on EQ-5D-5L, distress at ER visit (VAS), confidence in physician (VAS), and satisfaction with treatment (VAS). We hypothesized that the ENPSS would correlate more with QOL [55] since satisfaction with treatment is associated with QOL.
Only questionnaires with complete data were included in the analysis, and there was no imputation of missing data. Statistical significance was set at p ≤ 0.05 (two-sided). Statistical analyses were performed using SPSS Statistics version 27 (IBM Corp., Armonk, NY, USA) and JMP Pro software version 15 (SAS Institute Inc., Cary, NC, USA).
2.3. Ethical Considerations
The protocol for this research project was approved by a suitably constituted Ethics Committee of Sapporo Medical University and conformed to the provisions of the Declaration of Helsinki, Approval No. 1-2-51. Informed consent was obtained from all the respondents. Participants were informed of the purpose and length of the survey, and their participation was voluntary. Consent was obtained from respondents by checking the box on the front page of the questionnaires that they understood the research explanation and agreed to participate according to Institutional Review Board recommendations.
3. Results
3.1. Population
A total of 127 respondent surveys were included in the final analysis after excluding eight surveys with missing data. The characteristics of respondents are presented in Table 1. Patients who were still employed accounted for 66.1%, and those with underlying diseases accounted for 63.0% of the total. Fifty-two percent of the patients visited the ER during the day, and 40.2% visited the ER for the first time.

Table 1.
Participant sociodemographic and clinical characteristics (n = 127).
3.2. Selecting Items
A total of 127 participants (92%) had complete data on the ENPSS and constituted the population used for factor analysis; this was sufficient for previous EFA studies [37,42,56,57].
First, of the 38 question items, 4 items of which more than 20% were answered as not applicable were deleted. There were 31 pairs with correlation coefficients greater than 0.7. We eliminated one of the items of the pair, and 14 items were excluded. Second, factor analysis was conducted using the maximum likelihood method. In the EFA using promax rotation, one item with a factor loading of less than 0.35 was removed, and finally, 20 items were selected (Table 2).
Table 2.
Individual items and their factor resolutions in a 21-item patient satisfaction questionnaire regarding ER nursing.
The EFA yielded 20 solution items loaded into four factors representing four domains: explanation and response (seven items), hospitality (six items), teamwork (three items), and symptom management (four items). The global satisfaction item was not included in the EFA, which constitutes the ENPSS-21 in English version (see Appendix B) and Japanese version (see Appendix C). This 21-item questionnaire’s factor structure CFA (Figure 1) showed an acceptable fit: RMSEA = 0.1 (90% confidence interval = 0.08–0.11) and CFI = 0.9. EFA, exploratory factor analysis; ENPSS, emergency nursing-care patient satisfaction scale; CFA, confirmatory factor analysis; RMSEA, root mean square error of approximation; CFI, comparative fit index.
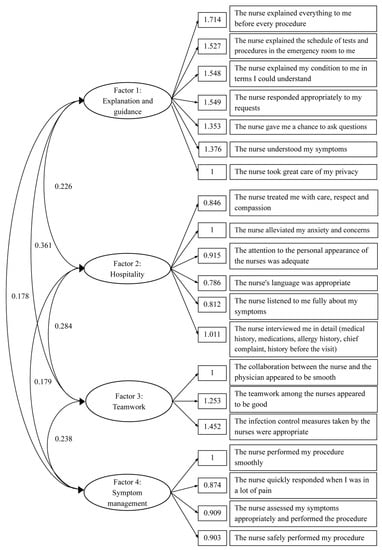
Figure 1.
Confirmatory factor analysis.
3.3. Internal Consistency Reliability
The internal consistency reliability (Cronbach’s alpha) of the four domains of the ENPSS-21 ranged from 0.81 to 0.89 (Table 3), corresponding to good internal reliability.
Table 3.
Internal consistency reliability of ENPSS-21 domains.
3.4. Construct Validity
The correlations of the four domain scores of the ENPSS-21 showed that the EQ-5D-5L VAS (0.59–0.65, p < 0.01), EQ-5D-5L Anxiety (0.55–0.62, p < 0.01), confidence in the ER physicians (0.56–0.63, p < 0.01), satisfaction with the response of ER physicians (0.57–0.66, p < 0.01), and satisfaction with the outcome of treatment in the ER (0.51–0.62, p < 0.01) were in the moderate to high range. The correlation was lower for the intensity of distress at the time of the ER visit (−0.2–−0.29, p < 0.01). As hypothesized, the summary score of ENPSS-21 showed the strongest correlation with EQ-5D-5L (0.68) and satisfaction with the response of the ER physician (0.68). (Figure 2 and Table 4).
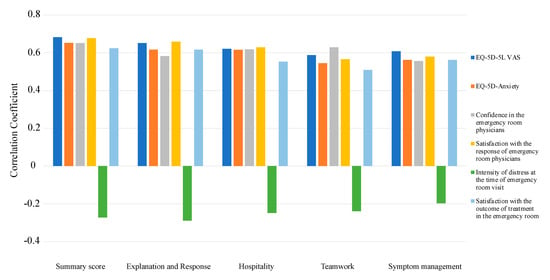
Figure 2.
Construct validity of the 19-item Emergency Nursing-Care Patient Satisfaction Questionnaire (ENPSS-21).
Table 4.
Multitrait–multimethod correlations matrix.
4. Discussion
In this study, we developed a patient satisfaction scale focused on ER nursing, confirmed its validity and reliability, and concluded that it could be used in clinical practice. To the best of our knowledge, there are no reports on developing a patient satisfaction scale that focuses on ER nursing in Japan.
The factor analysis results were composed of four domains: “explanation and response”, “hospitality”, ”teamwork”, and “symptom management”. This multidimensional structure is consistent with many reports on patient satisfaction analysis [2,10,24,58,59]. Furthermore, the specific dimensions obtained in this study are similar to those found in other scales [10,60], which we consider partially supportive of the construct validity of this tool.
A limitation when measuring patient satisfaction is that psychometric properties may not be reflected because cultural factors from different countries and regions are not adequately taken into account [61]. Translation of existing patient satisfaction measures, such as CECSS and others, may lead to differences in the perception of quality of care from the patient’s perspective due to cross-cultural differences [62]. Because of the specific situation in ERs, where patients are more urgent than in general wards and require a variety of responses, a specific scale consistent with the culture of the country is considered essential. Therefore, a patient satisfaction scale in the ER that takes into account the Japanese cultural context was needed.
The ENPSS-21 domain “explanation and response” includes nurse–patient communication and provision of information. In order for the nurse to meet the needs of the patient, a natural and constructive relationship must be established [63]. Nurses can then provide counseling and guidance to patients to improve patient satisfaction [64]. In the ER, providing information and communication to patients is also an important factor in facilitating patient care and is an essential factor in patient satisfaction [65].
The second domain of ENPSS-21 is “hospitality”. The nurse’s concept of compassion and interpersonal relationships is an important element in understanding patient. The hospitality domain also included items, such as courtesy and personal appearance. In Japan, courtesy and personal appearance strongly influence patient satisfaction [66,67], and we consider these cultural factors unique to Japan.
The third domain of ENPSS-21 is “teamwork”. Nurses are part of the healthcare team and are expected to collaborate with other healthcare professionals involved in patient care [63]. Moreover, nurses have an important task to fulfill as intermediaries between multiple healthcare professions. Organizational teamwork has been reported to be associated with satisfaction, and nurses need to practice in the best interest of the patient [68]. Therefore, it is considered a very important perspective for ER nurses to collaborate with ER physicians and co-medical staff to provide medical care.
The last domain of ENPSS-21 is “symptom management”. Patients in the ER have a wide range of distress. Appropriate analgesia affects patient satisfaction [69]. The absence of physical pain increased patient satisfaction with nursing care [70]. Therefore, distress relief is considered by some patients to be equivalent to good nursing care [71]. Namely, symptom management is considered an indispensable item for providing care that is consistent with the needs of ER patients.
Moreover, this patient satisfaction scale was developed during the COIVD-19 pandemic. During the COVID-19 pandemic, healthcare professionals have reported that adequate infection control measures are important for reducing the risk of viral infection and patient anxiety about the virus [72]. The questionnaire items used in this study included items related to infection control among nurses, which may include an important domain of recent emergency care. In addition, the compassion and interpersonal relationships of nurses are important factors for patient satisfaction [25,73,74].
Cronbach’s alpha for all domains of the ENPSS-21 scale was greater than 0.8. It was found that the ENPSS-21 had similar values to previous patient satisfaction scales, which were verified for internal consistency [59,75]. This means that each factor showed appropriate homogeneity.
Of all the hypotheses used for construct validity, the “EQ-5D-5” and “satisfaction with the response of ER physicians” were highly correlated with each of the four domains of the ENPSS-21 and summary score. Previous reports have shown an association between treatment satisfaction and QOL [55,58]. Patients with anxiety were also reported to be less satisfied with their healthcare [76], consistent with the results of this scale. In addition, satisfaction with physicians is related to overall satisfaction with healthcare [74], consistent with the hypothesis validation in this study. In contrast, a high ENPSS-21 score was not associated with the intensity of distress at the time of the emergency room visit. Although this was low compared to the intensity of distress at the emergency room visit in this study [71], it is consistent with the reported finding that VAS pain scores in the ER do not correlate with patient satisfaction [77].
5. Limitations
The current study has several limitations. First, test–retest reliability was not validated in this study. Having good test–retest reliability implies internal consistency of the test and ensures that the measurements obtained are representative [42]. In the future, a test–retest should be conducted to confirm reliability. Second, there are concerns about the time when data collection took place. In this study, data were collected during the COVID-19 pandemic period. As a result, the ER system was probably different from normal, which could have affected the assessment of patients. Third, this study used a minimum sample size of 100 for factor analysis from previous studies [37,42]. However, for CFA, a minimum sample of 150 is required [78]. This study did not meet that requirement, thus limiting the results of the analysis. In the future, it will be an issue to refine the items of the scale while taking the sample size into consideration.
6. Implications for Clinical Practice
ENPSS-21 is a brief, reliable, and valid instrument that can obtain information about patient satisfaction with ER nursing. The instrument has direct clinical utility for improving the quality of nursing care in the ER in Japan by providing a patient-centered perspective on satisfaction. The ENPSS-21 also helps address the weaknesses of the organization by measuring satisfaction regularly and comparing patient satisfaction levels relative to each other.
7. Conclusions
This study found that the ENPSS-21 was a robust measure of patient satisfaction, suggesting that it is possible to measure satisfaction with ER nursing. The ENPSS-21 is designed to focus on the nursing perspective of the ER. In creating the items, the ENPSS was designed to represent the emergency nursing care sought by patients on the basis of an extensive literature search and content validity. The ENPSS-21 consists of 21 items in four domains. It showed the highest correlation with the EQ-5D-5L and satisfaction with the response of ER physicians in criterion-related validity. By measuring patient-centered perspectives of satisfaction with ER nursing, factors lacking in each organization’s ER can be identified and addressed to improve the quality of nursing care in the ER.
Author Contributions
Conceptualization, J.H., N.M. (Naomi Minamoto), Y.T. and N.M. (Natsuko Makino); data curation, N.M. (Naomi Minamoto), M.S. and N.M. (Natsuko Makino); formal analysis, J.H.; funding acquisition, M.S.; investigation, J.H.; methodology, J.H., M.S. and N.K.; writing—original draft, J.H.; writing—review and editing, J.H., N.M. (Naomi Minamoto), M.S., Y.T., N.M. (Natsuko Makino), N.K. and H.U. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by a Research Grant from Sapporo Medical University (Mizue Shiromaru, project CD: 2100188).
Institutional Review Board Statement
Approval of the research protocol: The protocol for this research project was approved by a suitably constituted Ethics Committee of the Sapporo Medical University and conforms to the provisions of Declaration of Helsinki, Approval No. 1-2-51.
Informed Consent Statement
Informed consent was obtained from all the respondents. Participants were informed of the purpose and length of the survey, and their participation was voluntary. Checking the box at the beginning of the questionnaire stating that they understood the study description and agreed to participate was considered consent.
Data Availability Statement
All data from this research have been included within the manuscript.
Acknowledgments
We thank Junichi Hattori, Fumitaka Arisawa, Hideaki Okamura, Momoe Tanima, and Keiko Shimazu for data collection.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Table A1.
Characteristics of expert panel, n = 19.
Table A1.
Characteristics of expert panel, n = 19.
| Characteristic | n |
|---|---|
| Certified nurses in emergency nursing, n = 10 | |
| Sex, male | 3 |
| Age, mean (SD) | 40.6 (4.9) |
| Work experience in emergency care | 13.5 (3.2) |
| Healthy individuals who had visited an ER, n = 9 | |
| Sex, male | 3 |
| Age, mean (SD) | 42.8 (9.0) |
ER, emergency room; SD, standard deviation.
Appendix B. Nursing Emergency-Care Patient Satisfaction Scale—21 (ENPSS-21) English Version
The following questionnaire asks about the patient level of satisfaction with emergency room nurses. The goal of this questionnaire is to measure your level of satisfaction or dissatisfaction with the nurses on the basis of what you currently feel. Please place a check mark in the appropriate box for each question.
The following 20 questions relate to satisfaction with emergency room nurses.
- 1.
- The nurse explained everything to me before every procedure.□ Strongly disagree□ Slightly disagree□ Neutral□ Slightly agree□ Strongly agree□ Not applicable
- 2.
- The nurse explained the schedule of tests and procedures in the emergency room to me.□ Strongly disagree□ Slightly disagree□ Neutral□ Slightly agree□ Strongly agree□ Not applicable
- 3.
- The nurse explained my condition to me in terms I could understand.□ Strongly disagree□ Slightly disagree□ Neutral□ Slightly agree□ Strongly agree□ Not applicable
- 4.
- The nurse responded appropriately to my requests.□ Strongly disagree□ Slightly disagree□ Neutral□ Slightly agree□ Strongly agree□ Not applicable
- 5.
- The nurse gave me a chance to ask questions.□ Strongly disagree□ Slightly disagree□ Neutral□ Slightly agree□ Strongly agree□ Not applicable
- 6.
- The nurse understood my symptoms.□ Strongly disagree□ Slightly disagree□ Neutral□ Slightly agree□ Strongly agree□ Not applicable
- 7.
- The nurse took great care of my privacy.□ Strongly disagree□ Slightly disagree□ Neutral□ Slightly agree□ Strongly agree□ Not applicable
- 8.
- The nurse treated me with care, respect, and compassion.□ Strongly disagree□ Slightly disagree□ Neutral□ Slightly agree□ Strongly agree□ Not applicable
- 9.
- The nurse alleviated my anxiety and concerns.□ Strongly disagree□ Slightly disagree□ Neutral□ Slightly agree□ Strongly agree□ Not applicable
- 10.
- The attention to the personal appearance of the nurses was adequate.□ Strongly disagree□ Slightly disagree□ Neutral□ Slightly agree□ Strongly agree□ Not applicable
- 11.
- The nurse’s language was appropriate.□ Strongly disagree□ Slightly disagree□ Neutral□ Slightly agree□ Strongly agree□ Not applicable
- 12.
- The nurse listened to me fully about my symptoms.□ Strongly disagree□ Slightly disagree□ Neutral□ Slightly agree□ Strongly agree□ Not applicable
- 13.
- The nurse interviewed me in detail (medical history, medications, allergy history, chief complaint, and medical history before the visit).□ Strongly disagree□ Slightly disagree□ Neutral□ Slightly agree□ Strongly agree□ Not applicable
- 14.
- The collaboration between the nurse and the physician appeared to be smooth.□ Strongly disagree□ Slightly disagree□ Neutral□ Slightly agree□ Strongly agree□ Not applicable
- 15.
- The teamwork among the nurses appeared to be good.□ Strongly disagree□ Slightly disagree□ Neutral□ Slightly agree□ Strongly agree□ Not applicable
- 16.
- The infection control measures taken by the nurses were appropriate.□ Strongly disagree□ Slightly disagree□ Neutral□ Slightly agree□ Strongly agree□ Not applicable
- 17.
- The nurse performed my procedure smoothly.□ Strongly disagree□ Slightly disagree□ Neutral□ Slightly agree□ Strongly agree□ Not applicable
- 18.
- The nurse quickly responded when I was in a lot of pain.□ Strongly disagree□ Slightly disagree□ Neutral□ Slightly agree□ Strongly agree□ Not applicable
- 19.
- The nurse assessed my symptoms appropriately and performed the procedure.□ Strongly disagree□ Slightly disagree□ Neutral□ Slightly agree□ Strongly agree□ Not applicable
- 20.
- The nurse safely performed my procedure.□ Strongly disagree□ Slightly disagree□ Neutral□ Slightly agree□ Strongly agree□ Not applicableThe following question is about your overall satisfaction with emergency room nurses.Please place a check mark in the appropriate box.
- 21.
- I felt that the overall quality of nursing care I received in the emergency room was good.□ Strongly disagree□ Slightly disagree□ Neutral□ Slightly agree□ Strongly agree□ Not applicable
Appendix C. Nursing Emergency-Care Patient Satisfaction Scale—21 (ENPSS-21) Japanese Version
以下のアンケートは、救急外来の看護師に対するあなたの満足度を調査するものです。このアンケートの目的は、あなたが現在感じている、看護師に対する満足感を測定することです。 各質問について、該当するボックスにチェックマークを入れてください。
以下の20の質問は、救急外来の看護師に対する満足度に関するものです。
- 看護師は全ての処置の前に説明してくれましたか。□ 全くそう思わない□ そう思わない□ どちらでもない□ そう思う□ とてもそう思う□ 該当なし
- 看護師は、救急外来での検査や処置の予定について説明しましたか。□ 全くそう思わない□ そう思わない□ どちらでもない□ そう思う□ とてもそう思う□ 該当なし
- 看護師は、あなたの病状に関して理解できる言葉で説明しましたか。□ 全くそう思わない□ そう思わない□ どちらでもない□ そう思う□ とてもそう思う□ 該当なし
- 看護師は、あなたの要望に適切に対応しましたか。□ 全くそう思わない□ そう思わない□ どちらでもない□ そう思う□ とてもそう思う□ 該当なし
- 看護師は、あなたに質問する機会を与えてくれましたか。□ 全くそう思わない□ そう思わない□ どちらでもない□ そう思う□ とてもそう思う□ 該当なし
- 看護師は、あなたの症状を理解していましたか。□ 全くそう思わない□ そう思わない□ どちらでもない□ そう思う□ とてもそう思う□ 該当なし
- 看護師は、あなたのプライバシーに対して十分に考慮しましたか。□ 全くそう思わない□ そう思わない□ どちらでもない□ そう思う□ とてもそう思う□ 該当なし
- 看護師は、あなたに丁寧かつ敬意や思いやりのある対応をしましたか。□ 全くそう思わない□ そう思わない□ どちらでもない□ そう思う□ とてもそう思う□ 該当なし
- 看護師によって、あなたの不安や心配事は軽減されましたか。□ 全くそう思わない□ そう思わない□ どちらでもない□ そう思う□ とてもそう思う□ 該当なし
- 看護師の身だしなみへの配慮は十分でしたか。□ 全くそう思わない□ そう思わない□ どちらでもない□ そう思う□ とてもそう思う□ 該当なし
- 看護師の言葉遣いは適切でしたか。□ 全くそう思わない□ そう思わない□ どちらでもない□ そう思う□ とてもそう思う□ 該当なし
- 看護師は、あなたの症状について十分に話を聞いていましたか。□ 全くそう思わない□ そう思わない□ どちらでもない□ そう思う□ とてもそう思う□ 該当なし
- 看護師は、あなたに対して詳しく問診(既往歴、内服薬、アレルギー歴、主訴、受診前の経緯などの聴取)をしていましたか。□ 全くそう思わない□ そう思わない□ どちらでもない□ そう思う□ とてもそう思う□ 該当なし
- 看護師と医師との連携はスムーズでしたか。□ 全くそう思わない□ そう思わない□ どちらでもない□ そう思う□ とてもそう思う□ 該当なし
- 看護師同士のチームワークは良かったですか。□ 全くそう思わない□ そう思わない□ どちらでもない□ そう思う□ とてもそう思う□ 該当なし
- 看護師の感染対策は十分と感じましたか。□ 全くそう思わない□ そう思わない□ どちらでもない□ そう思う□ とてもそう思う□ 該当なし
- 看護師は、あなたの処置をスムーズに行っていましたか。□ 全くそう思わない□ そう思わない□ どちらでもない□ そう思う□ とてもそう思う□ 該当なし
- 看護師は、あなたの苦痛が強いとき迅速に対応してくれましたか。□ 全くそう思わない□ そう思わない□ どちらでもない□ そう思う□ とてもそう思う□ 該当なし
- 看護師は、あなたの症状を適切に判断して処置を行なっていましたか。□ 全くそう思わない□ そう思わない□ どちらでもない□ そう思う□ とてもそう思う□ 該当なし
- 看護師は、処置を行う際、安全に配慮していましたか。□ 全くそう思わない□ そう思わない□ どちらでもない□ そう思う□ とてもそう思う□ 該当なし次の質問は、救急外来の看護師に対するあなたの総合的な満足度についてです。該当するボックスにチェックマークを入れてください。
- 救急外来受診中に受けた看護ケアの全体的な質は良いと感じましたか。□ 全くそう思わない□ そう思わない□ どちらでもない□ そう思う□ とてもそう思う□ 該当なし
References
- Kamimura, A.; Ashby, J.; Myers, K.; Nourian, M.M.; Christensen, N. Satisfaction with healthcare services among free clinic patients. J. Community Health 2015, 40, 62–72. [Google Scholar] [CrossRef] [PubMed]
- Marshall, G.N.; Hays, R.D. The Patient Satisfaction Questionnaire Short-Form (PSQ-18); Rand: Santa Monica, CA, USA, 1994. [Google Scholar]
- Fufa, B.D.; Negao, E.B. Satisfaction of Outpatient Service Consumers and Associated Factors Towards the Health Service Given at Jimma Medical Center, South West Ethiopia. Patient Relat. Outcome Meas. 2019, 10, 347–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahmqvist, M.; Bara, A.-C. Patient characteristics and quality dimensions related to patient satisfaction. Int. J. Qual. Health Care 2010, 22, 86–92. [Google Scholar] [CrossRef]
- Turris, S.A. Unpacking the concept of patient satisfaction: A feminist analysis. J. Adv. Nurs. 2005, 50, 293–298. [Google Scholar] [CrossRef]
- Ak, M.; Cinar, O.; Sutcigil, L.; Congologlu, E.D.; Haciomeroglu, B.; Canbaz, H.; Yaprak, H.; Jay, L.; Ozmenler, K.N. Communication skills training for emergency nurses. Int. J. Med. Sci. 2011, 8, 397–401. [Google Scholar] [CrossRef] [Green Version]
- Dilig-Ruiz, A.; MacDonald, I.; Demery Varin, M.; Vandyk, A.; Graham, I.D.; Squires, J.E. Job satisfaction among critical care nurses: A systematic review. Int. J. Nurs. Stud. 2018, 88, 123–134. [Google Scholar] [CrossRef]
- Harley, A.; Johnston, A.N.B.; Denny, K.J.; Keijzers, G.; Crilly, J.; Massey, D. Emergency nurses’ knowledge and understanding of their role in recognising and responding to patients with sepsis: A qualitative study. Int. Emerg. Nurs. 2019, 43, 106–112. [Google Scholar] [CrossRef]
- An, Y.; Yang, Y.; Wang, A.; Li, Y.; Zhang, Q.; Cheung, T.; Ungvari, G.S.; Qin, Z.M.; An, F.-R.; Xiang, Y.-T. Prevalence of depression and its impact on quality of life among frontline nurses in emergency departments during the COVID-19 outbreak. J. Affect. Disord. 2020, 276, 312–315. [Google Scholar] [CrossRef] [PubMed]
- Davis, B.A.; Bush, H.A. Developing effective measurement tools: A case study of the Consumer Emergency Care Satisfaction Scale. J. Nurs. Care Qual. 1995, 9, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Abidova, A.; da Silva, P.A.; Moreira, S. The mediating role of patient satisfaction and perceived quality of healthcare in the emergency department. Medicine 2021, 100, e25133. [Google Scholar] [CrossRef]
- Chan, J.N.H.; Chau, J. Patient satisfaction with triage nursing care in Hong Kong. J. Adv. Nurs. 2005, 50, 498–507. [Google Scholar] [CrossRef]
- Elder, R.; Neal, C.; Davis, B.A.; Almes, E.; Whitledge, L.; Littlepage, N. Patient satisfaction with triage nursing in a rural hospital emergency department. J. Nurs. Care Qual. 2004, 19, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Davis, B.A.; Bush, H.A. Patient satisfaction of emergency nursing care in the United States, Slovenia, and Australia. J. Nurs. Care Qual. 2003, 18, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Deák, A.; Fusz, K.; Kanizsai, P. Patient satisfaction during the COVID-19 pandemic in an emergency department. Orv. Hetil. 2020, 161, 1819–1823. [Google Scholar] [CrossRef] [PubMed]
- Sonis, J.D.; Aaronson, E.L.; Lee, R.Y.; Philpotts, L.L.; White, B.A. Emergency Department Patient Experience: A Systematic Review of the Literature. J. Patient Exp. 2018, 5, 101–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aaronson, E.L.; Mort, E.; Sonis, J.D.; Chang, Y.; White, B.A. Overall Emergency Department Rating: Identifying the Factors That Matter Most to Patient Experience. J. Health Qual. 2018, 40, 367–376. [Google Scholar] [CrossRef] [PubMed]
- Phiri, M.; Heyns, T.; Coetzee, I. Patients’ experiences of triage in an emergency department: A phenomenographic study. Appl. Nurs. Res. 2020, 54, 151271. [Google Scholar] [CrossRef]
- Meterko, M.; Mohr, D.C.; Young, G.J. Teamwork culture and patient satisfaction in hospitals. Med. Care 2004, 42, 492–498. [Google Scholar] [CrossRef] [PubMed]
- Vahey, D.C.; Aiken, L.H.; Sloane, D.M.; Clarke, S.P.; Vargas, D. Nurse burnout and patient satisfaction. Med. Care. 2004, 42, II57–II66. [Google Scholar] [CrossRef] [Green Version]
- Lu, D.W.; Weygandt, P.L.; Pinchbeck, C.; Strout, T.D. Emergency Medicine Trainee Burnout Is Associated With Lower Patients’ Satisfaction With Their Emergency Department Care. AEM Educ. Train. 2018, 2, 86–90. [Google Scholar] [CrossRef]
- Nápoles-Springer, A.M.; Santoyo, J.; Houston, K.; Pérez-Stable, E.J.; Stewart, A.L. Patients’ perceptions of cultural factors affecting the quality of their medical encounters. Health Expect. 2005, 8, 4–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woods, S.E.; Bivins, R.; Oteng, K.; Engel, A. The influence of ethnicity on patient satisfaction. Ethn. Health 2005, 10, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Xesfingi, S.; Vozikis, A. Patient satisfaction with the healthcare system: Assessing the impact of socio-economic and healthcare provision factors. BMC Health Serv. Res. 2016, 16, 94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prakash, B. Patient satisfaction. J. Public Health 2010, 3, 151–155. [Google Scholar] [CrossRef]
- McCleery, E.; Christensen, V.; Peterson, K.; Humphrey, L.; Helfand, M. Evidence Brief: The Quality of Care Provided by Advanced Practice Nurses. VA Evidence Synthesis Program Evidence Briefs; Department of Veterans Affairs (US): Washington, DC, USA, 2014. [Google Scholar]
- Evans, D.K.; Welander Tärneberg, A. Health-care quality and information failure: Evidence from Nigeria. Health Econ. 2018, 27, e90–e93. [Google Scholar] [CrossRef]
- Almeida RS de Bourliataux-Lajoinie, S.; Martins, M. Satisfaction measurement instruments for healthcare service users: A systematic review. Cad. Saúde Pública 2015, 31, 11–25. [Google Scholar]
- Shimizu, K.; Hibino, S.; Biros, M.H.; Irisawa, T.; Shimazu, T. Emergency medicine in Japan: Past, present, and future. Int. J. Emerg. Med. 2021, 14, 2. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. The Ageing Society: Current Situation and Implementation Measures FY 2017. Available online: https://www8.cao.go.jp/kourei/english/annualreport/2018/pdf/c1-1.pdf (accessed on 28 January 2022).
- Katayama, Y.; Kiyohara, K.; Kitamura, T.; Hayashida, S.; Shimazu, T. Influence of the COVID-19 pandemic on an emergency medical service system: A population-based, descriptive study in Osaka, Japan. Acute Med. Surg. 2020, 7, e534. [Google Scholar] [CrossRef]
- Ikegami, N.; Yoo, B.-K.; Hashimoto, H.; Matsumoto, M.; Ogata, H.; Babazono, A.; Watanabe, R.; Shibuya, K.; Yang, B.-M.; Reich, M.R.; et al. Japanese universal health coverage: Evolution, achievements, and challenges. Lancet 2011, 378, 1106–1115. [Google Scholar] [CrossRef]
- Minarik, P.A.; Chan, G.K.; Usami, S. CNS Role and Practice in Japan. In Clinical Nurse Specialist Role and Practice: An International Perspective; Fulton, J.S., Holly, V.W., Eds.; Springer: Cham, Denmark, 2021; pp. 171–181. [Google Scholar]
- Grissom, M.O.; Farra, M.; Cruzen, E.S.; Barlow, E.; Gupta, S. What can COVID-19 teach us about patient satisfaction in the emergency department? A mixed-methods approach. J. Am. Coll. Emerg. Physicians Open 2021, 2, e12436. [Google Scholar] [CrossRef]
- King, D.M.; Vakkalanka, J.P.; Junker, C.; Harland, K.K.; Nugent, A.S. Emergency Department Overcrowding Lowers Patient Satisfaction Scores. Acad. Emerg. Med. 2021, 28, 363–366. [Google Scholar] [CrossRef] [PubMed]
- Romero-García, M.; de la Cueva-Ariza, L.; Jover-Sancho, C.; Delgado-Hito, P.; Acosta-Mejuto, B.; Sola-Ribo, M.; Juandó-Prats, C.; Ricart-Basagaña, M.T.; Sola-Sole, N. La percepción del paciente crítico sobre los cuidados enfermeros: Una aproximación al concepto de satisfacción. Enferm. Intensiv. 2013, 24, 51–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anthoine, E.; Moret, L.; Regnault, A.; Sébille, V.; Hardouin, J.-B. Sample size used to validate a scale: A review of publications on newly-developed patient reported outcomes measures. Health Qual. Life Outcomes 2014, 12, 176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bilsbury, C.D.; Richman, A. A staging approach to measuring patient-centred subjective outcomes. Acta Psychiatr. Scand. 2002, 106, 5–40. [Google Scholar] [CrossRef] [PubMed]
- Davis, L.L. Instrument review: Getting the most from a panel of experts. Appl. Nurs. Res. 1992, 5, 194–197. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T. The content validity index: Are you sure you know what’s being reported? Critique and recommendations. Res. Nurs. Health 2006, 29, 489–497. [Google Scholar] [CrossRef] [Green Version]
- Tanigawa, K.; Tanaka, K. Emergency medical service systems in Japan: Past, present, and future. Resuscitation 2006, 69, 365–370. [Google Scholar] [CrossRef] [Green Version]
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; Bouter, L.M. COSMIN Checklist Manual. Amsterdam: University Medical Center. 2012. Available online: http://fac.ksu.edu.sa/sites/default/files/cosmin_checklist_manual_v9.pdf (accessed on 3 January 2022).
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [Green Version]
- Janssen, M.F.; Pickard, A.S.; Golicki, D.; Gudex, C.; Niewada, M.; Scalone, L.; Swinburn, P.; Busschbach, J. Measurement properties of the EQ-5D-5L compared to the EQ-5D-3L across eight patient groups: A multi-country study. Qual. Life Res. 2013, 22, 1717–1727. [Google Scholar] [CrossRef] [Green Version]
- Shiroiwa, T.; Ikeda, S.; Noto, S.; Igarashi, A.; Fukuda, T.; Saito, S.; Shimozuma, K. Comparison of Value Set Based on DCE and/or TTO Data: Scoring for EQ-5D-5L Health States in Japan. Value Health 2016, 19, 648–654. [Google Scholar] [CrossRef] [Green Version]
- Shiroiwa, T.; Fukuda, T.; Ikeda, S.; Igarashi, A.; Noto, S.; Saito, S.; Shimozuma, K. Japanese population norms for preference-based measures: EQ-5D-3L, EQ-5D-5L, and SF-6D. Qual. Life Res. 2016, 25, 707–719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nirel, N.; Goldwag, R.; Feigenberg, Z.; Abadi, D.; Halpern, P. Stress, work overload, burnout, and satisfaction among paramedics in Israel. Prehospital Disaster Med. 2008, 23, 537–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avraham, N.; Goldblatt, H.; Yafe, E. Paramedics’ experiences and coping strategies when encountering critical incidents. Qual. Health Res. 2014, 24, 194–208. [Google Scholar] [CrossRef] [PubMed]
- Crowe, R.P.; Bower, J.K.; Cash, R.E.; Panchal, A.R.; Rodriguez, S.A.; Olivo-Marston, S.E. Association of Burnout with Workforce-Reducing Factors among EMS Professionals. Prehospital Emerg. Care 2018, 22, 229–236. [Google Scholar] [CrossRef]
- Lawn, S.; Roberts, L.; Willis, E.; Couzner, L.; Mohammadi, L.; Goble, E. The effects of emergency medical service work on the psychological, physical, and social well-being of ambulance personnel: A systematic review of qualitative research. BMC Psychiatry 2020, 20, 348. [Google Scholar] [CrossRef]
- Streiner, D.L.; Norman, G.R.; Cairney, J. Health Measurement Scales: A Practical Guide to Their Development and Use; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Ferketich, S. Focus on psychometrics. Aspects of item analysis. Res. Nurs. Health 1991, 14, 165–168. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Cronbach’s alpha. BMJ 1997, 314, 572. [Google Scholar] [CrossRef] [Green Version]
- Nunnally, J.C. Psychometric Theory 3E; Tata McGraw-Hill Education: New York, NY, USA, 1994. [Google Scholar]
- Revicki, D.A. Patient assessment of treatment satisfaction: Methods and practical issues. Gut 2004, 53 (Suppl. S4), iv40–iv44. [Google Scholar] [CrossRef]
- de Winter, J.C.F.; Dodou, D.; Wieringa, P.A. Exploratory Factor Analysis With Small Sample Sizes. Multivar. Behav. Res. 2009, 44, 147–181. [Google Scholar] [CrossRef]
- Kline, P. An Easy Guide to Factor Analysis; Routledge: London, UK, 2014. [Google Scholar]
- Wiebe, S.; Wahby, S.; Lawal, O.A.; Sajobi, T.T.; Keezer, M.R.; Nguyen, D.K.; Malmgren, K.; Tellez-Zenteno, J.; Atkinson, M.J.; Hader, W.J.; et al. Development and validation of the Epilepsy Surgery Satisfaction Questionnaire (ESSQ-19). Epilepsia 2020, 61, 2729–2738. [Google Scholar] [CrossRef]
- Romero-García, M.; De La Cueva-Ariza, L.; Benito-Aracil, L.; Lluch-Canut, T.; Trujols-Albet, J.; Martínez, M.A.; Juvé-Udina, M.-E.; Delgado-Hito, P.; Benito-Aracil, L.; Lluch-Canut, T. Nursing Intensive-Care Satisfaction Scale [NICSS]: Development and validation of a patient-centred instrument. J. Adv. Nurs. 2018, 74, 1423–1435. [Google Scholar] [CrossRef] [PubMed]
- Naidoo, T.; Tomita, A.; Paruk, S. Burnout, anxiety and depression risk in medical doctors working in KwaZulu-Natal Province, South Africa: Evidence from a multi-site study of resource-constrained government hospitals in a generalised HIV epidemic setting. PLoS ONE 2020, 15, e0239753. [Google Scholar] [CrossRef] [PubMed]
- Horne, R.; Hankins, M.; Jenkins, R. The Satisfaction with Information about Medicines Scale (SIMS): A new measurement tool for audit and research. BMJ Qual. Saf. 2001, 10, 135–140. [Google Scholar] [CrossRef]
- Grimshaw, J.M.; Eccles, M.P.; Lavis, J.N.; Hill, S.J.; Squires, J.E. Knowledge translation of research findings. Implement. Sci. 2012, 7, 50. [Google Scholar] [CrossRef] [PubMed]
- Johansson, P.; Oléni, M.; Fridlund, B. Patient satisfaction with nursing care in the context of health care: A literature study. Scand. J. Caring Sci. 2002, 16, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Morgan, A.K. Client education experiences in professional nursing practice—A phenomenological perspective. J. Adv. Nurs. 1994, 19, 792–801. [Google Scholar] [CrossRef] [PubMed]
- Abdel Maqsood, A.S.; Oweis, A.I.; Hasna, F.S. Differences between patients’ expectations and satisfaction with nursing care in a private hospital in Jordan. Int. J. Nurs. Pr. 2012, 18, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Elleuch, A. Patient satisfaction in Japan. Int. J. Health Care Qual. Assur. 2008, 21, 692–705. [Google Scholar] [CrossRef] [PubMed]
- Tokunaga, J.; Imanaka, Y.; Nobutomo, K. Effects of patient demands on satisfaction with Japanese hospital care. Int. J. Qual. Health Care 2000, 12, 395–401. [Google Scholar] [CrossRef] [Green Version]
- Leiter, M.P.; Harvie, P.; Frizzell, C. The correspondence of patient satisfaction and nurse burnout. Soc. Sci. Med. 1998, 47, 1611–1617. [Google Scholar] [CrossRef]
- Megivern, K.; Halm, M.A.; Jones, G. Measuring patient satisfaction as an outcome of nursing care. J. Nurs. Care Qual. 1992, 6, 9–24. [Google Scholar] [CrossRef] [PubMed]
- Redmond, G.M.; Sorrell, J.M. Studying patient satisfaction: Patient voices of quality. Outcomes Manag. Nurs. Pract. 1999, 3, 67–72. [Google Scholar]
- Lövgren, G.; Engström, B.; Norberg, A. Patients’ narratives concerning good and bad caring. Scand. J. Caring Sci. 1996, 10, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Aashima Nanda, M.; Sharma, R. A Review of Patient Satisfaction and Experience with Telemedicine: A Virtual Solution During and Beyond COVID-19 Pandemic. Telemed. e-Health 2021, 27, 1325–1331. [Google Scholar] [CrossRef]
- Batbaatar, E.; Dorjdagva, J.; Luvsannyam, A.; Savino, M.M.; Amenta, P. Determinants of patient satisfaction: A systematic review. Perspect. Public Health 2017, 137, 89–101. [Google Scholar] [CrossRef]
- Schoenfelder, T.; Klewer, J.; Kugler, J. Determinants of patient satisfaction: A study among 39 hospitals in an in-patient setting in Germany. Int. J. Qual. Health Care 2011, 23, 503–509. [Google Scholar] [CrossRef]
- Laschinger, H.S.; Hall, L.M.; Pedersen, C.; Almost, J.A. Psychometric analysis of the patient satisfaction with nursing care quality questionnaire: An actionable approach to measuring patient satisfaction. J. Nurs. Care Qual. 2005, 20, 220–230. [Google Scholar] [CrossRef]
- Abtahi, A.M.; Brodke, D.S.; Lawrence, B.D.; Zhang, C.; Spiker, W.R. Association between patient-reported measures of psychological distress and patient satisfaction scores after spine surgery. J. Bone Jt. Surg. Am. Vol. 2015, 97, 824–828. [Google Scholar] [CrossRef] [Green Version]
- Kelly, A.M. Patient satisfaction with pain management does not correlate with initial or discharge VAS pain score, verbal pain rating at discharge, or change in VAS score in the Emergency Department. J. Emerg. Med. 2000, 19, 113–116. [Google Scholar] [CrossRef]
- Kyriazos, T.A. Applied psychometrics: Sample size and sample power considerations in factor analysis (EFA, CFA) and SEM in general. Psychology 2018, 9, 2207–2230. [Google Scholar] [CrossRef] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).