
Evaluating Long-Term Outcomes of a High School-Based Impaired and Distracted Driving Prevention Program

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
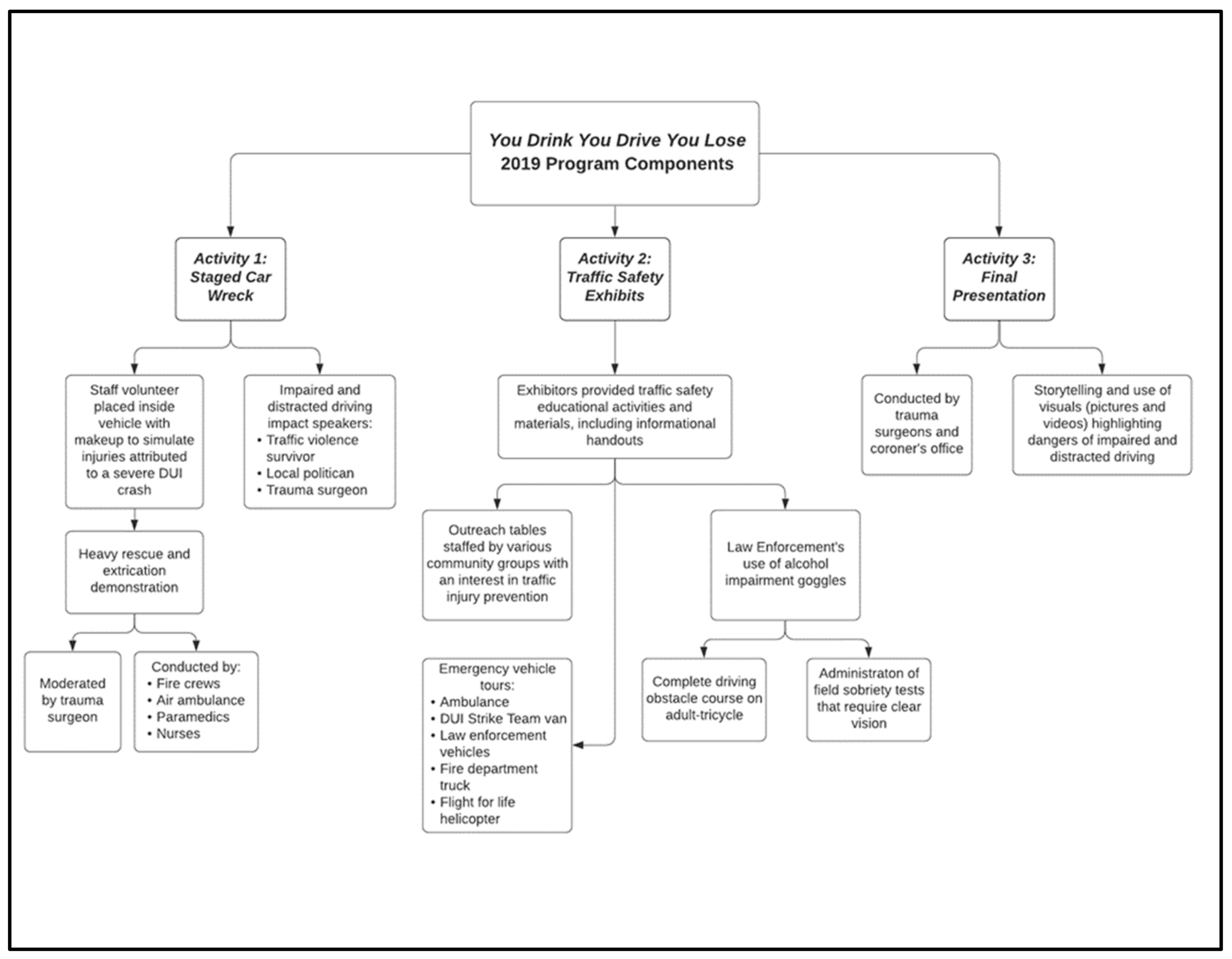
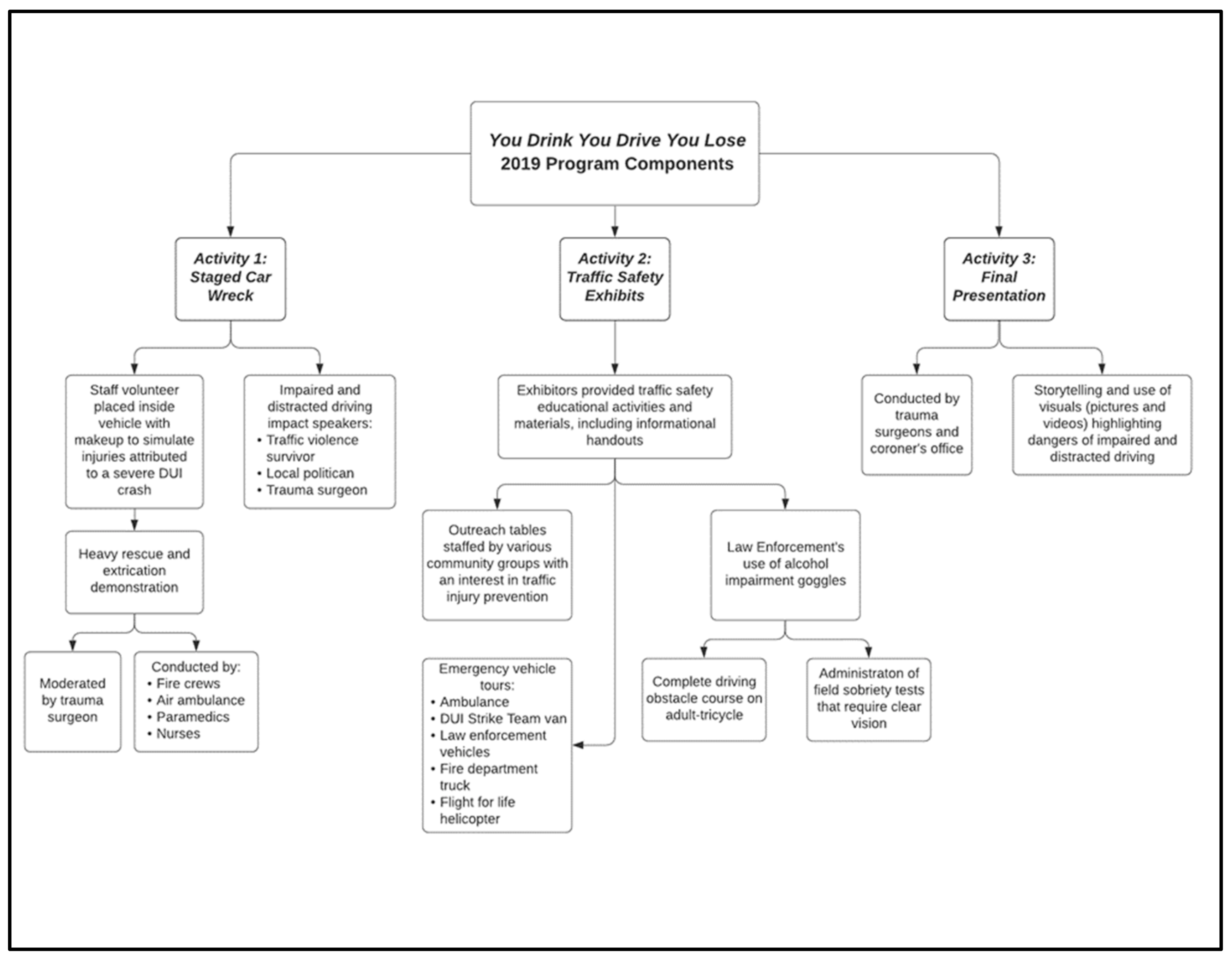
2.1. Program Description
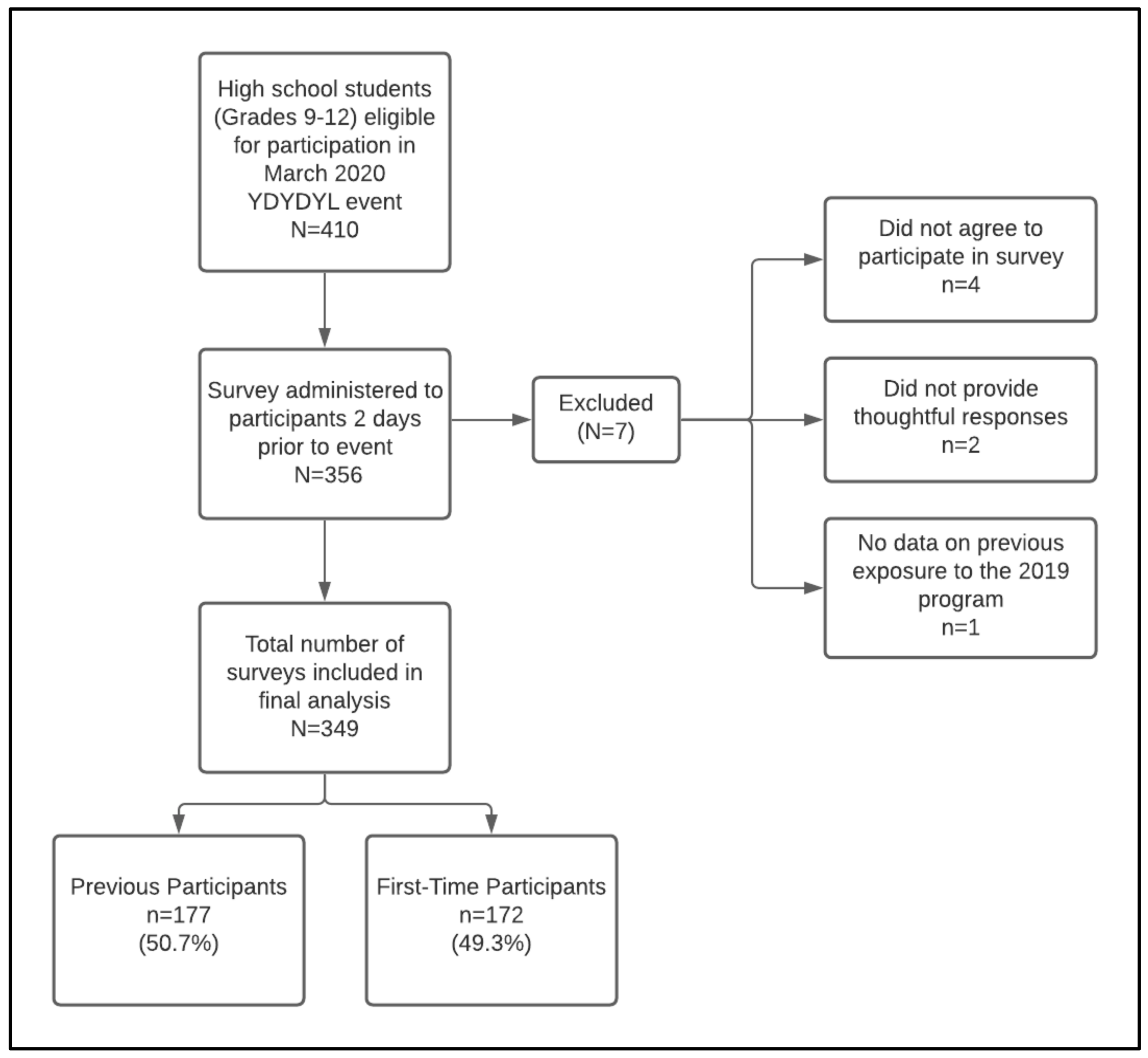
2.2. Study Type and Data Source
2.3. Ethical Considerations
2.4. Sample Size Justification
2.5. Statistical Analysis
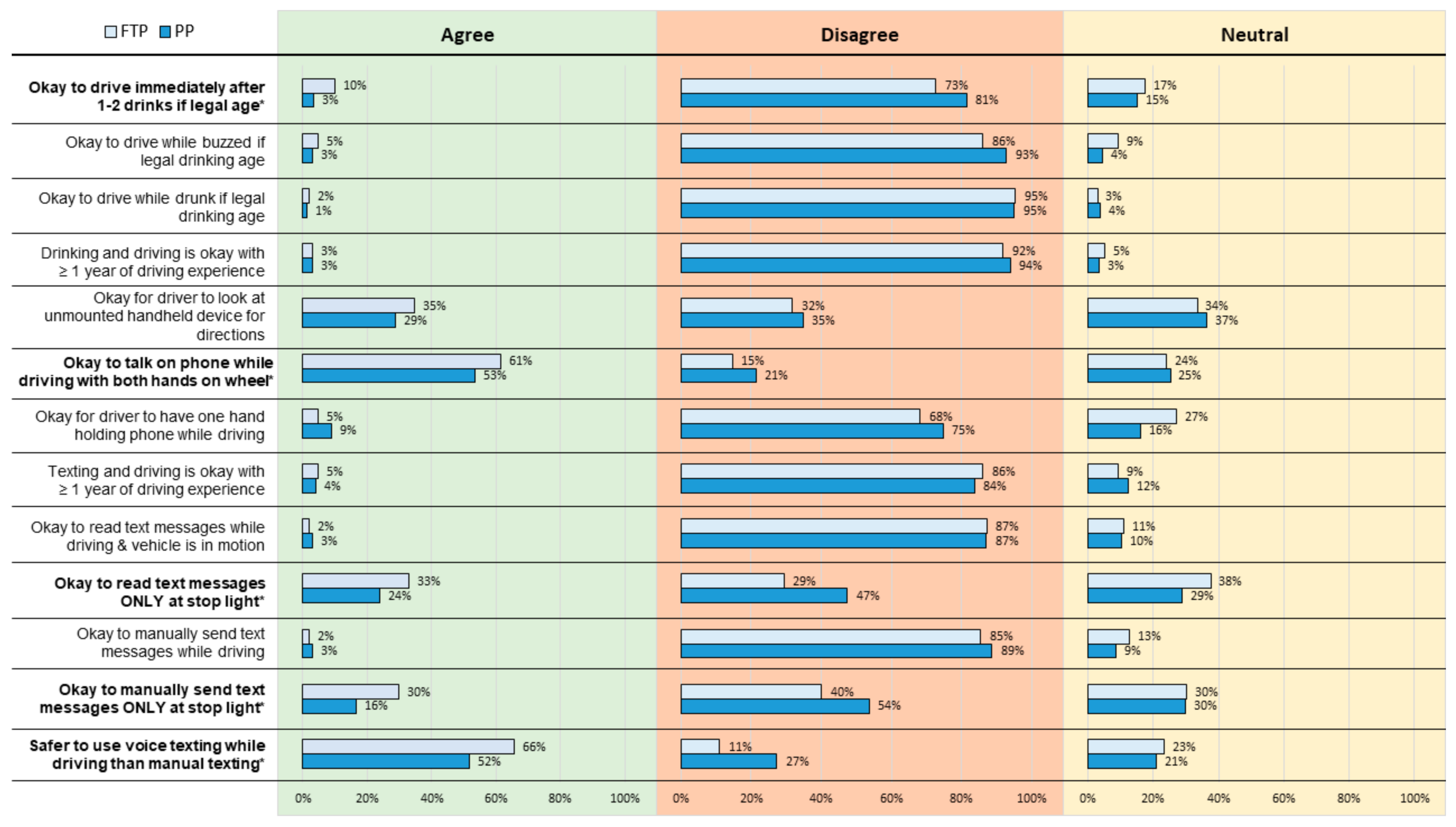
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Future Research Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Web-Based Injury Statistics Query and Reporting System (WISQARS). Available online: https://www.cdc.gov/injury/wisqars/index.html (accessed on 6 July 2020).
- Curtin, S.C.; Heron, M.; Miniño, A.M.; Warner, M. Recent Increases in Injury Mortality among Children and Adolescents Aged 10–19 Years in the United States: 1999–2016. Natl. Vital Stat. Rep. 2018, 67, 1–16. Available online: https://www.ncbi.nlm.nih.gov/pubmed/29874162 (accessed on 30 June 2020). [PubMed]
- Fatality Facts 2019: Teenagers. IIHS. Available online: https://www.iihs.org/topics/fatality-statistics/detail/teenagers (accessed on 7 April 2021).
- Alcohol Impaired Driving. GHSA. Available online: https://www.ghsa.org/state-laws/issues/alcohol%20impaired%20driving (accessed on 7 April 2021).
- Teen Drinking and Driving. Available online: https://www.cdc.gov/vitalsigns/teendrinkinganddriving/index.html#:~:text=*Blood%20alcohol%20concentration.,alcohol%20in%20all%20US%20states (accessed on 7 April 2021).
- Alcohol and Drugs. IIHS. Available online: https://www.iihs.org/topics/alcohol-and-drugs (accessed on 7 April 2021).
- Drug-Impaired Driving. NHTSA. Available online: https://www.nhtsa.gov/risky-driving/drug-impaired-driving (accessed on 7 April 2021).
- Schauer, G.L.; Clayton, H.B.; Njai, R.; Grant, A.M. Adolescent marijuana use and related risk behaviors, national findings from 2015 to 2017. Am. J. Prev. Med. 2020, 59, 714–724. [Google Scholar] [CrossRef] [PubMed]
- Teen Driving. NHTSA. Available online: https://www.nhtsa.gov/road-safety/teen-driving (accessed on 7 April 2021).
- Investigation and Prosecution of Distracted Driving Cases. NHTSA. Available online: https://www.nhtsa.gov/sites/nhtsa.dot.gov/files/documents/812407-distracteddrivingreport.pdf (accessed on 7 April 2021).
- Guo, F.; Klauer, S.G.; Fang, Y.; Hankey, J.M.; Antin, J.F.; Perez, M.A.; Lee, S.E.; Dingus, T.A. The effects of age on crash risk associated with driver distraction. Int. J. Epidemiol. 2017, 46, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Highway Statistics 2015. FHWA. Available online: https://www.fhwa.dot.gov/policyinformation/statistics/2015/dl20.cfm (accessed on 28 April 2021).
- Distracted Driving 2015. NHTSA. Available online: https://crashstats.nhtsa.dot.gov/Api/Public/ViewPublication/812381 (accessed on 7 April 2021).
- Youth Risk Behavior Surveillance- United States, 2017. Available online: https://www.cdc.gov/healthyyouth/data/yrbs/pdf/2017/ss6708.pdf (accessed on 7 April 2021).
- Miech, R.; Johnston, L.; O’Malley, P.M.; Bachman, J.G.; Patrick, M.E. Trends in adolescent vaping, 2017–2019. N. Engl. J. Med. 2019, 381, 1490–1491. [Google Scholar] [CrossRef] [PubMed]
- Bordin, J.; Bumpus, M.; Hunt, S. Every 15 minutes. Calif. J. Health Promot. 2003, 1, 1–5. [Google Scholar] [CrossRef]
- King, K.A.; Vidourek, R.A.; Love, J.; Wegley, S.; Alles-White, M. Teaching adolescents safe driving and passenger behaviors: Effectiveness of the you hold the key teen driving countermeasure. J. Saf. Res. 2008, 39, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Shope, J.T.; Elliott, M.R.; Raghunathan, T.E.; Waller, P.F. Long-term follow-up of a high school alcohol misuse prevention program’s effect on students’ subsequent driving. Alcohol. Clin. Exp. Res. 2001, 25, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Cutello, C.A.; Hellier, E.; Stander, J.; Hanoch, Y. Evaluating the effectiveness of a young driver-education intervention: Learn2Live. Transp. Res. Part F Traffic Psychol. Behav. 2020, 69, 375–384. [Google Scholar] [CrossRef]
- Elder, R.W.; Nichols, J.L.; Shults, R.A.; Sleet, D.A.; Barrios, L.C.; Compton, R. Effectiveness of school-based programs for reducing drinking and driving and riding with drinking drivers. Am. J. Prev. Med. 2005, 28, 288–304. [Google Scholar] [CrossRef] [PubMed]
- Linden, P.L.; Endee, L.M.; Flynn, E.; Johnson, L.M.; Miller, C.A.; Rozensky, R.; Smith, S.G.; Verderosa, C. High school student driving perceptions following participation in a distracted driving curriculum. Health Promot. Pract. 2019, 20, 703–710. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioural Sciences; Lawrence Earlbaum Associates: Hillside, NJ, USA, 1988. [Google Scholar]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical Power Analyses Using G*Power 3.1: Tests for Correlation and Regression Analyses. Behav. Res. Meth. 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mansournia, M.A.; Collins, G.S.; Nielsen, R.O.; Nazemipour, M.; Jewell, N.P.; Altman, D.G.; Campbell, M.J. A Checklist for Statistical Assessment of Medical Papers (the CHAMP Statement): Explanation and Elaboration. Br. J. Sports Med. 2021, 55, 1009–1017. [Google Scholar] [CrossRef] [PubMed]
- Wickman, M.E.; Anderson, N.L.; Smith Greenberg, C. The adolescent perception of invincibility and its influence on teen acceptance of health promotion strategies. J. Pediatric Nurs. 2008, 23, 460–468. [Google Scholar] [CrossRef] [PubMed]
- Dang, J.; King, K.M.; Inzlicht, M. Why Are Self-Report and Behavioral Measures Weakly Correlated? Trends Cogn. Sci. 2020, 24, 267–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kruger, J. Lake Wobegon be gone! The “below-average effect” and the egocentric nature of comparative ability judgments. J. Personal. Soc. Psychol. 1999, 77, 221–232. [Google Scholar] [CrossRef]
- Baddeley, M. Herding, social influence and economic decision-making: Socio-psychological and neuroscientific analyses. Philos. Trans. R. Soc. B Biol. Sci. 2010, 365, 281–290. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Previous Participants (n = 177, 50.7%) | First-time Participants (n = 172, 49.3%) | Test Statistics p-Value | |
|---|---|---|---|
| n (%) | n (%) | Chi-Square p-Value | |
| Gender: | Χ2 = 5.30 p = 0.151 | ||
| Male | 85 (48.0) | 94 (54.7) | Χ2 = 1.19 p = 0.236 |
| Female | 87 (49.2) | 75 (43.6) | Χ2 = 1.09 p = 0.276 |
| Non-binary | 3 (1.7) | 0 (0.0) | Χ2 = 1.72 p = 0.085 |
| Prefer not to say | 1 (0.6) | 3 (1.7) | Χ2 = 1.03 p = 0.303 |
| Race/Ethnicity: | Χ2 = 0.76 p = 0.682 | ||
| White | 63 (35.6) | 60 (34.9) | Χ2 = 0.10 p = 0.921 |
| Non-White * | 75 (42.4) | 79 (45.9) | Χ2 = 0.72 p = 0.473 |
| Hispanic or Latino | 39 (22.0) | 32 (18.6) | Χ2 = 0.77 p = 0.442 |
| Licensure Status: | Χ2 = 66.40 p ≤ 0.001 | ||
| Driver’s license | 47 (26.6) | 11 (6.4) | Χ2 = 5.06 p ≤ 0.001 |
| Learner’s permit | 54 (30.5) | 15 (8.7) | Χ2 = 5.11 p ≤ 0.001 |
| Neither | 76 (42.9) | 146 (84.9) | Χ2 = 8.14 p ≤ 0.001 |
| Survey Questions | Previous Participants (n = 177) | First-Time Participants (n = 172) | Chi-Square p-Value |
|---|---|---|---|
| Yes n (%) | Yes n (%) | ||
| Have ever tried: | 177 | 172 | |
| Alcohol | 52 (29.4) | 41 (23.8) | Χ2 = 1.37 p = 0.242 |
| Marijuana | 18 (10.2) | 13 (7.6) | Χ2 = 0.71 p = 0.401 |
| Vaping (any substance) | 19 (10.7) | 19 (11.0) | Χ2 = 0.01 p = 0.925 |
| Other Illegal substances | 4 (2.3) | 4 (2.3) | Χ2 = 0.00 p = 0.622 * |
| Ridden in a vehicle driven by someone who had been drinking alcohol | 58 (32.8) | 43 (25.0) | Χ2 = 2.56 p = 0.110 |
| ≤30 days, rode in a vehicle with a driver who had been drinking alcohol | 14 (7.9) | 18 (10.5) | Χ2 = 3.58 p = 0.06 |
| Survey Questions | Previous Participants (n = 101) | First-Time Participants (n = 26) | Chi-Square p-Value |
|---|---|---|---|
| Yes n (%) | Yes n (%) | ||
| Drivers who have ever driven | |||
| Buzzed/drunk | 0 (0.0) | 2 (7.7) | Χ2 = 7.82 p = 0.041 * |
| After using marijuana | 1 (1.0) | 1 (3.8) | Χ2 = 1.14 p = 0.361 * |
| While vaping any substance | 6 (5.9) | 1 (3.8) | Χ2 = 0.19 p = 0.662 |
| ≤30 days, driven while buzzed/drunk | 0 (0.0) | 1 (3.8) | Χ2 = 3.80 p = 0.210 * |
| ≤30 days, driven after using marijuana | 0 (0.0) | 1 (3.8) | Χ2 = 3.91 p = 0.205 * |
| ≤30 days, driven while vaping (any substance) | 1 (1.0) | 1 (3.8) | Χ2 = 1.03 p = 0.377 * |
| ≤7 days, sent text message(s) while driving &vehicle was in motion | 30 (29.7) | 7 (26.9) | Χ2 = 0.08 p = 0.781 |
| Survey Questions | Likely | Neutral | Not-Likely |
|---|---|---|---|
| n (%) | n (%) | n (%) | |
| How likely you would stop a friend from practicing the following behaviors | |||
| Driving when they are intoxicated from alcohol | 159 (89.3) | 8 (4.5) | 11 (6.2) |
| Driving 30 min after consuming two alcoholic drinks | 153 (86.0) | 11 (6.2) | 14 (7.9) |
| Driving after using marijuana | 148 (83.6) | 14 (7.9) | 15 (8.5) |
| Driving after using illegal drugs | 156 (88.6) | 6 (3.4) | 14 (8.0) |
| How likely you would stop a family member from practicing the following behaviors | |||
| Driving when they are intoxicated from alcohol | 157 (88.2) | 11 (6.2) | 10 (5.6) |
| Driving 30 min after consuming two alcoholic drinks | 154 (86.5) | 12 (6.7) | 12 (6.7) |
| Driving after using marijuana | 150 (84.3) | 14 (7.9) | 14 (7.9) |
| Driving after using illegal drugs | 159 (89.3) | 8 (4.5) | 11 (6.2) |
| Survey Questions | Likely | Neutral | Not-Likely |
|---|---|---|---|
| n (%) | n (%) | n (%) | |
| How likely you would stop a friend from practicing the following behaviors | |||
| Driving when they are intoxicated from alcohol | 160 (92.3) | 3 (1.7) | 10 (5.8) |
| Driving 30 min after consuming two alcoholic drinks | 145 (83.8) | 11 (6.4) | 17(9.8) |
| Driving after using marijuana | 143 (82.7) | 12(6.9) | 18 (10.4) |
| Driving after using illegal drugs | 156 (90.2) | 4 (2.3) | 13 (7.5) |
| How likely you would stop a family member from practicing the following behaviors | |||
| Driving when they are intoxicated from alcohol | 155 (89.6) | 6 (3.5) | 12 (6.9) |
| Driving 30 min after consuming two alcoholic drinks | 141 (82.0) | 16 (9.3) | 15 (8.7) |
| Driving after using marijuana | 144 (83.7) | 8 (4.7) | 20 (11.6) |
| Driving after using illegal drugs | 155 (90.1) | 6 (3.5) | 11 (6.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buczek, L.; Gryder, L.K.; Slinkard-Barnum, S.; Batra, K.; Trummel, C.; McNickle, A.G.; Fraser, D.R.; Kuhls, D.A.; Chestovich, P.J. Evaluating Long-Term Outcomes of a High School-Based Impaired and Distracted Driving Prevention Program. Healthcare 2022, 10, 474. https://doi.org/10.3390/healthcare10030474
Buczek L, Gryder LK, Slinkard-Barnum S, Batra K, Trummel C, McNickle AG, Fraser DR, Kuhls DA, Chestovich PJ. Evaluating Long-Term Outcomes of a High School-Based Impaired and Distracted Driving Prevention Program. Healthcare. 2022; 10(3):474. https://doi.org/10.3390/healthcare10030474
Chicago/Turabian StyleBuczek, Lindsay, Laura K. Gryder, Samantha Slinkard-Barnum, Kavita Batra, Cassandra Trummel, Allison G. McNickle, Douglas R. Fraser, Deborah A. Kuhls, and Paul J. Chestovich. 2022. "Evaluating Long-Term Outcomes of a High School-Based Impaired and Distracted Driving Prevention Program" Healthcare 10, no. 3: 474. https://doi.org/10.3390/healthcare10030474
APA StyleBuczek, L., Gryder, L. K., Slinkard-Barnum, S., Batra, K., Trummel, C., McNickle, A. G., Fraser, D. R., Kuhls, D. A., & Chestovich, P. J. (2022). Evaluating Long-Term Outcomes of a High School-Based Impaired and Distracted Driving Prevention Program. Healthcare, 10(3), 474. https://doi.org/10.3390/healthcare10030474