Subsequent Ultrasonographic Non-Visualization of the Ovaries Is Hastened in Women with Only One Ovary Visualized Initially



Abstract
1. Introduction
2. Materials and Methods
- (a)
- Side-to-side movements to achieve sagittal imaging;
- (b)
- 90° rotation to obtain semi-coronal images and angulation of the probe vertically; and
- (c)
- Varying the depth of probe insertion to expose different pelvic structures within the field of view. The pelvis was surveyed by slowly sweeping the beam in a sagittal plane from the midline to the lateral pelvic sidewalls, followed by turning the probe 90 degrees into the coronal plane and sweeping the beam from the cervix to the fundus. Landmarks for proving structure consisted of identifying the iliac vessels in the pelvic sidewall and the tubal vessels located posterior and parallel to the fallopian tubes. Pressure was applied to at least three regions of the abdominal surface to achieve bowel repositioning in order to assist visualizations. All images were reviewed by a physician and by at least one of the authors. The study protocol specified that ovaries be measured in three dimensions. Ovarian volume was calculated using the prolate ellipsoid formula (length × width × height × 0.523) [11,12]. Thus, a visualization event was validated by findings that obtained all three measurements. All screening information was entered into a database (MEDLOG Systems, Crystal Bay, NV, USA) on a local network. Women who had a normal screen were scheduled to return in 12 months for a repeat screen. Only women with one or more visible ovaries on their first TVS encounter were utilized in this study and then followed over the course of annual examinations by TVS. Women who underwent abdominal surgery were censored from the present analysis so that surgical interventions did not influence assessments of visualization outcomes.
Statistical Analyses
3. Results
- A total amount of 29,877 women were identified that had both ovaries visualized on their first TVS exam and were subsequently followed over a course of 202,639 prospective TVS exams. 9703 women were identified that had only one ovary visualized on their first TVS exam and were subsequently followed over a course of 63,697 prospective TVS exams. Demographic characteristics are presented in Table 1.

{kind=link}
{kind=link}
| All Subjects (n = 29,877) | All Encounters (n = 202,639) | |
|---|---|---|
| Age (y) | 55.0, 55 (20–91) | 60.1, 60 (20–95) |
| Weight (kg) | 73, 70.3 (38–204) | 72.3, 69.4 (36–205) |
| Height (cm) | 163.5, 162.6 (119–198) | 163.6, 162.6 (119–198) |
| BMI | 27.3, 26 (13–80) | 27, 26 (13–80) |
| Pre-menopausal | 5966 (20.9%) | 28,618 (14.3%) |
| Peri-menopausal | 1262 (4.4%) | 5820 (2.9%) |
| Post-menopausal | 21,251 (74.6%) | 165,390 (82.8%) |
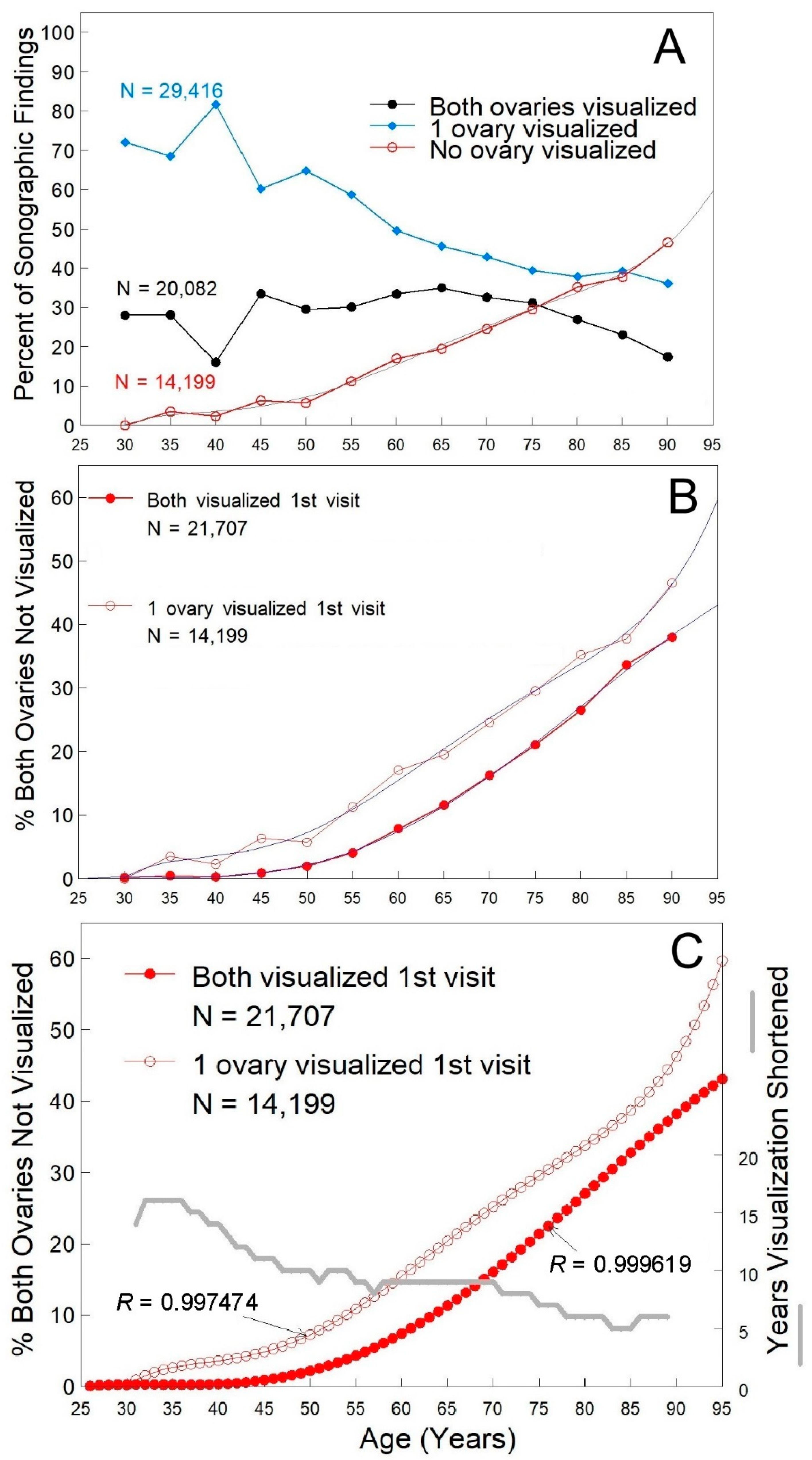
- Age–non-visualization incidence increased with age (Figure 1A, open red symbols), while visualization of one ovary decreased with age (Figure 1A, solid blue diamonds). Despite selection for women with only one ovary visualized on their first visit, both ovaries were reported about a third of the time subsequently (Figure 1A, solid black symbols). When the women that had neither ovary visualized on the first ultrasound exam were examined (n = 7975), a similar fraction was found to have both ovaries reported as visualized subsequently, indicating that there is variability in the identification of ovarian structures over time. Visualization of one or both ovaries decreased with age, but one or both ovaries could be visualized in two out of every three women at 80 years of age and more than 50% of women over 80 years of age (Figure 1A).

- Body Habitus–Neither weight (Figure 2A, p > 0.2) nor BMI (Figure 2B, p > 0.12) was independently associated with ovarian visualization since across all weights and BMIs, non-visualization of both ovaries was ~20–25%. Both ovaries were visualized in 25–30% of women that weighed 180–275 lbs, in 17–23% of women that weighed over 300 lbs (Figure 2A), and in >25% of women with a BMI over 40 (Figure 2B).
- Menopausal Status–Menopausal status was self-reported. Non-visualization was ~7% in pre-menopausal women and ~25% of postmenopausal women (Figure 2C, p < 0.001) that initially had only one ovary visualized.
4. Discussion
4.1. Clinical Implications
4.2. Research Implications
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ovarian Cancer Including Fallopian Tube Cancer and Primary Peritoneal Cancer. Available online: https://www.nccn.org/professionals/physician_gls/pdf/ovarian.pdf (accessed on 22 February 2022).
- Moorthy, R.S. Transvaginal sonography. Med. J. Armed Forces India 2000, 56, 181–183. [Google Scholar] [CrossRef]
- Jacobs, I.; Gentry-Maharaj, A.; Burnell, M.; Manchanda, R.; Singh, N.; Sharma, A.; Ryan, A.; Seif, M.W.; Amso, N.N.; Turner, G.; et al. Sensitivity of transvaginal ultrasound screening for endometrial cancer in postmenopausal women: A case-control study within the UKCTOCS cohort. Lancet Oncol. 2011, 12, 38–48. [Google Scholar] [CrossRef]
- van Nagell, J.; Burgess, B.; Miller, R.; Baldwin, L.; DeSimone, C.; Ueland, F.; Huang, B.; Chen, Q.; Kryscio, R.; Pavlik, E. Survival of women with type I and II epithelial ovarian cancer detected by ultrasound screening. Obstet. Gynecol. 2018, 132, 1091–1100. [Google Scholar] [CrossRef] [PubMed]
- Carter, J.; Fowler, J.; Carson, L.; Carlson, J.; Twiggs, L.B. How accurate is the pelvic examination as compared to transvaginal sonography? A prospective, comparative study. J. Reprod. Med. 1994, 39, 32–34. [Google Scholar] [PubMed]
- Ueland, F.R.; DePriest, P.D.; DeSimone, C.P.; Pavlik, E.J.; Lele, S.M.; Kryscio, R.J.; van Nagell, J.R. The accuracy of examination under anesthesia and transvaginal sonography in evaluating ovarian size. Gynecol. Oncol. 2005, 99, 400–403. [Google Scholar] [CrossRef] [PubMed]
- Pavlik, E.J.; DePriest, P.D.; Gallion, H.H.; Ueland, F.R.; Reedy, M.B.; Kryscio, R.J.; van Nagell, J.R. Ovarian volume related to age. Gynecol. Oncol. 2000, 77, 410–412. [Google Scholar] [CrossRef] [PubMed]
- Pavlik, E.J.; Liu, C.; DePriest, P.D.; Gallion, H.H.; Ueland, F.R.; Kryscio, R.J.; van Nagell, J.R. Relating ovarian size to age, menopausal status, and use of hormones. Gynecol. Oncol. 2001, 80, 333–334. [Google Scholar] [CrossRef] [PubMed]
- Pavlik, E.J.; Brekke, E.; Gorski, J.; Baldwin-Branch, L.; Miller, R.; DeSimone, C.P.; Dietrich, C.S.; Gallion, H.S.; Ueland, F.R.; van Nagell, J.R., Jr. Ultrasonographic visualization of the ovaries to detect ovarian cancer according to age, menopausal status and body type. Diagnostics 2022, 12, 128. [Google Scholar] [CrossRef] [PubMed]
- National Institute on Aging. Available online: https://www.nia.nih.gov/health/what-menopause (accessed on 22 February 2022).
- Higgins, R.V.; van Nagell, J.R., Jr.; Woods, C.H.; Thompson, E.A.; Kryscio, R.J. Interobserver variation in ovarian measurements using transvaginal sonography. Gynecol. Oncol. 1990, 39, 69–71. [Google Scholar] [CrossRef]
- Raine-Fenning, N.J.; Campbell, B.K.; Clewes, J.S.; Johnson, I.R. The interobserver reliability of ovarian volume measurement is improved with three-dimensional ultrasound, but dependent upon technique. Ultrasound Med. Biol. 2003, 29, 1685–1690. [Google Scholar] [CrossRef]
- VassarStats: Website for Statistical Computation. Available online: http://vassarstats.net/index.html (accessed on 22 February 2022).
- National Institute of Diabetes and Digestive and Kidney Diseases: Overweight & Obesity Statistics. Available online: https://www.niddk.nih.gov/health-information/health-statistics/overweight-obesity#estimation (accessed on 22 February 2022).
- Glanc, P.; O’Hayon, B.E.; Singh, D.K.; Bokhari, S.A.J.; Maxwell, C.V. Challenges of pelvic imaging in obese women. RadioGraphics 2012, 32, 1839–1862. [Google Scholar] [CrossRef] [PubMed]
- Your Guide to Menopause. Available online: https://www.webmd.com/menopause/guide/menopause-information#1-2 (accessed on 22 February 2022).
- Age at Menopause. Available online: https://www.cdc.gov/nchs/data/series/sr_11/sr11_019.pdf (accessed on 22 February 2022).
- Gold, E.B. The timing of the age at which natural menopause occurs. Obstet. Gynecol. Clin. 2011, 38, 425–440. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pavlik, E.J.; Fancher, H.; Dietrich, C.S.; van Nagell, J.R., Jr. Subsequent Ultrasonographic Non-Visualization of the Ovaries Is Hastened in Women with Only One Ovary Visualized Initially. Healthcare 2022, 10, 433. https://doi.org/10.3390/healthcare10030433
Pavlik EJ, Fancher H, Dietrich CS, van Nagell JR Jr. Subsequent Ultrasonographic Non-Visualization of the Ovaries Is Hastened in Women with Only One Ovary Visualized Initially. Healthcare. 2022; 10(3):433. https://doi.org/10.3390/healthcare10030433
Chicago/Turabian StylePavlik, Edward J., Hannah Fancher, Charles S. Dietrich, and John R. van Nagell, Jr. 2022. "Subsequent Ultrasonographic Non-Visualization of the Ovaries Is Hastened in Women with Only One Ovary Visualized Initially" Healthcare 10, no. 3: 433. https://doi.org/10.3390/healthcare10030433
APA StylePavlik, E. J., Fancher, H., Dietrich, C. S., & van Nagell, J. R., Jr. (2022). Subsequent Ultrasonographic Non-Visualization of the Ovaries Is Hastened in Women with Only One Ovary Visualized Initially. Healthcare, 10(3), 433. https://doi.org/10.3390/healthcare10030433