
Sudden Sensorineural Hearing Loss May Increase the Risk of Retinal Vein Occlusion: A Nationwide Cohort Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Independent Variables
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wilson, W.R.; Byl, F.M.; Laird, N. The Efficacy of Steroids in the Treatment of Idiopathic Sudden Hearing Loss. A Double-Blind Clinical Study. Arch. Otolaryngol. 1980, 106, 772–776. [Google Scholar] [CrossRef] [PubMed]
- Byl, F.M., Jr. Sudden Hearing Loss: Eight Years’ Experience and Suggested Prognostic Table. Laryngoscope 1984, 94, 647–661. [Google Scholar] [CrossRef] [PubMed]
- Fetterman, B.L.; Saunders, J.E.; Luxford, W.M. Prognosis and Treatment of Sudden Sensorineural Hearing Loss. Am. J. Otol. 1996, 17, 529–536. [Google Scholar] [PubMed]
- Kuhn, M.; Heman-Ackah, S.E.; Shaikh, J.A.; Roehm, P.C. Sudden Sensorineural Hearing Loss: A Review of Diagnosis, Treatment, and Prognosis. Trends Amplif. 2011, 15, 91–105. [Google Scholar] [CrossRef] [PubMed]
- Chau, J.K.; Lin, J.R.; Atashband, S.; Irvine, R.A.; Westerberg, B.D. Systematic Review of the Evidence for the Etiology of Adult Sudden Sensorineural Hearing Loss. Laryngoscope 2010, 120, 1011–1021. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Lopez, I.; Ishiyama, A.; Baloh, R.W. Can Migraine Damage the Inner Ear? Arch. Neurol. 2000, 57, 1631–1634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urban, G.E., Jr. Reversible Sensori-Neural Hearing Loss Associated With Sickle Cell Crisis. Laryngoscope 1973, 83, 633–638. [Google Scholar] [CrossRef]
- Ostchega, Y.; Dillon, C.F.; Hughes, J.P.; Carroll, M.; Yoon, S. Trends in Hypertension Prevalence, Awareness, Treatment, and Control in Older U.S. Adults: Data from the National Health and Nutrition Examination Survey 1988 to 2004. J. Am. Geriatr. Soc. 2007, 55, 1056–1065. [Google Scholar] [CrossRef]
- Wild, S.; Roglic, G.; Green, A.; Sicree, R.; King, H. Global Prevalence of Diabetes: Estimates for the Year 2000 and Projections for 2030. Diabetes Care 2004, 27, 1047–1053. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention (CDC). State-Specific Prevalence of Cigarette Smoking among Adults and Quitting among Persons Aged 18–35 Years—United States, 2006. MMWR Morb. Mortal. Wkly. Rep. 2007, 56, 993–996. [Google Scholar]
- Marcucci, R.; Alessandrello Liotta, A.; Cellai, A.P.; Rogolino, A.; Berloco, P.; Leprini, E.; Pagnini, P.; Abbate, R.; Prisco, D. Cardiovascular and Thrombophilic Risk Factors for Idiopathic Sudden Sensorineural Hearing Loss. J. Thromb. Haemost. 2005, 3, 929–934. [Google Scholar] [CrossRef]
- Lin, H.C.; Chao, P.Z.; Lee, H.C. Sudden Sensorineural Hearing Loss Increases the Risk of Stroke: A 5-Year Follow-up Study. Stroke 2008, 39, 2744–2748. [Google Scholar] [CrossRef] [Green Version]
- Kuo, C.L.; Shiao, A.S.; Wang, S.J.; Chang, W.P.; Lin, Y.Y. Risk of Sudden Sensorineural Hearing Loss in Stroke Patients: A 5-Year Nationwide Investigation of 44,460 Patients. Medicine 2016, 95, e4841, Erratum in Medicine 2017, 96, e6217. [Google Scholar] [CrossRef]
- Kim, J.Y.; Hong, J.Y.; Kim, D.K. Association of Sudden Sensorineural Hearing Loss with Risk of Cardiocerebrovascular disease: A study Using Data from the Korea National Health Insurance Service. JAMA Otolaryngol. Head Neck Surg. 2018, 144, 129–135. [Google Scholar] [CrossRef]
- Karia, N. Retinal Vein Occlusion: Pathophysiology and Treatment Options. Clin. Ophthalmol. 2010, 4, 809–816. [Google Scholar] [CrossRef] [Green Version]
- Rehak, J.; Rehak, M. Branch Retinal Vein Occlusion: Pathogenesis, Visual Prognosis, and Treatment Modalities. Curr. Eye Res. 2008, 33, 111–131. [Google Scholar] [CrossRef]
- Klein, R.; Klein, B.E.; Moss, S.E.; Meuer, S.M. The Epidemiology of Retinal Vein Occlusion: The Beaver Dam Eye Study. Trans. Am. Ophthalmol. Soc. 2000, 98, 133–141. [Google Scholar]
- McIntosh, R.L.; Rogers, S.L.; Lim, L.; Cheung, N.; Wang, J.J.; Mitchell, P.; Kowalski, J.W.; Nguyen, H.P.; Wong, T.Y. Natural History of Central Retinal Vein Occlusion: An Evidence-Based Systematic Review. Ophthalmology 2010, 117, 1113–1123.e15. [Google Scholar] [CrossRef]
- Rogers, S.L.; McIntosh, R.L.; Lim, L.; Mitchell, P.; Cheung, N.; Kowalski, J.W.; Nguyen, H.P.; Wang, J.J.; Wong, T.Y. Natural History of Branch Retinal Vein Occlusion: An Evidence-Based Systematic Review. Ophthalmology 2010, 117, 1094–1101.e5. [Google Scholar] [CrossRef]
- Rim, T.H.; Oh, J.; Kang, S.M.; Kim, S.S. Association between Retinal Vein Occlusion and Risk of Heart Failure: A 12-Year Nationwide Cohort Study. Int. J. Cardiol. 2016, 217, 122–127. [Google Scholar] [CrossRef]
- Rim, T.H.; Kim, D.W.; Han, J.S.; Chung, E.J. Retinal Vein Occlusion and the Risk of Stroke Development: A 9-Year Nationwide Population-Based Study. Ophthalmology 2015, 122, 1187–1194. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Ko, I.; Kim, M.S.; Kim, D.W.; Cho, B.J.; Kim, D.K. Relationship of Chronic Rhinosinusitis with Asthma, Myocardial Infarction, Stroke, Anxiety, and Depression. J. Allergy Clin. Immunol. Pract. 2020, 8, 721–727.e3. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Kim, Y.S.; Ko, I.; Kim, D.K. Association Between Burning Mouth Syndrome and the Development of Depression, Anxiety, Dementia, and Parkinson Disease. JAMA Otolaryngol. Head Neck Surg. 2020, 146, 561–569. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Ko, I.; Kim, D.K. Association of Obstructive Sleep Apnea with the Risk of Affective Disorders. JAMA Otolaryngol. Head Neck Surg. 2019, 145, 1020–1026. [Google Scholar] [CrossRef]
- Kim, J.Y.; Ko, I.; Kim, M.S.; Yu, M.S.; Cho, B.J.; Kim, D.K. Association of Chronic Rhinosinusitis with Depression and Anxiety in a Nationwide Insurance Population. JAMA Otolaryngol. Head Neck Surg. 2019, 145, 313–319. [Google Scholar] [CrossRef]
- Fusconi, M.; Chistolini, A.; de Virgilio, A.; Greco, A.; Massaro, F.; Turchetta, R.; Benincasa, A.T.; Tombolini, M.; de Vincentiis, M. Sudden Sensorineural Hearing Loss: A Vascular Cause? Analysis of Prothrombotic Risk Factors in Head and Neck. Int. J. Audiol. 2012, 51, 800–805. [Google Scholar] [CrossRef]
- Lan, M.Y.; Shiao, J.Y.; Hsu, Y.B.; Lin, F.Y.; Lin, J.C. A Preliminary Study on the Role of Inherited Prothrombotic Risk Factors in Taiwanese Patients with Sudden Sensorineural Hearing Loss. Eur. Arch. Otorhinolaryngol. 2011, 268, 817–822. [Google Scholar] [CrossRef]
- Fusconi, M.; Chistolini, A.; Angelosanto, N.; Pignoloni, P.; Tombolini, M.; De Virgilio, A.; Pagliarella, M.; de Vincentiis, M. Role of Genetic and Acquired Prothrombotic Risk Factors in Genesis of Sudden Sensorineural Hearing Loss. Audiol. Neurootol. 2011, 16, 185–190. [Google Scholar] [CrossRef]
- Wong, T.Y.; Larsen, E.K.; Klein, R.; Mitchell, P.; Couper, D.J.; Klein, B.E.; Hubbard, L.D.; Siscovick, D.S.; Sharrett, A.R. Cardiovascular Risk Factors for Retinal Vein Occlusion and Arteriolar Emboli: The Atherosclerosis Risk in Communities & Cardiovascular Health Studies. Ophthalmology 2005, 112, 540–547. [Google Scholar]
- Rogers, S.; McIntosh, R.L.; Cheung, N.; Lim, L.; Wang, J.J.; Mitchell, P.; Kowalski, J.W.; Nguyen, H.; Wong, T.Y.; International Eye Disease Consortium. The Prevalence of Retinal Vein Occlusion: Pooled Data from Population Studies from the United States, Europe, Asia, and Australia. Ophthalmology 2010, 117, 313–319.e1. [Google Scholar] [CrossRef] [Green Version]
- Shin, Y.U.; Cho, H.; Kim, J.M.; Bae, K.; Kang, M.H.; Shin, J.P.; Nam, E.; Kang, S.W.; Epidemiologic Survey Committee of the Korean Ophthalmological Society. Prevalence and Associated Factors of Retinal Vein Occlusion in the Korean National Health and Nutritional Examination Survey, 2008–2012: A Cross-Sectional Observational Study. Medicine 2016, 95, e5185. [Google Scholar] [CrossRef]
- Guclu, H.; Ozal, S.A.; Pelitli Gurlu, V.; Özgün, G.S.; Özgün, E. Increased Fibrinogen to Albumin Ratio in Ischemic Retinal Vein Occlusions. Eur. J. Ophthalmol. 2017, 27, 735–739. [Google Scholar] [CrossRef]
- Cayir, S.; Kayabasi, S.; Hizli, O. Predictor parameters for poor prognosis in patients with sudden sensorineural hearing loss: Fibrinogen to albumin ratio vs C-reactive protein to albumin ratio. Braz. J. Otorhinolaryngol. 2021, 87, 457–461. [Google Scholar] [CrossRef]
- Glacet-Bernard, A.; Roquet, W.; Coste, A.; Peynègre, R.; Coscas, G.; Soubrane, G. Central retinal vein occlusion and sudden deafness: A possible common pathogenesis. Eur. J. Ophthalmol. 2001, 11, 197–199. [Google Scholar] [CrossRef]
- Lin, R.J.; Krall, R.; Westerberg, B.D.; Chadha, N.K.; Chau, J.K. Systematic Review and Meta-Analysis of the Risk Factors for Sudden Sensorineural Hearing Loss in Adults. Laryngoscope 2012, 122, 624–635. [Google Scholar] [CrossRef]
- Kim, S.H.; Kim, S.J.; Im, H.; Kim, T.H.; Song, J.J.; Chae, S.W. A Trend in Sudden Sensorineural Hearing Loss: Data from a Population-Based Study. Audiol. Neurootol. 2017, 22, 311–316. [Google Scholar] [CrossRef]
- Cheung, N.; Klein, R.; Wang, J.J.; Cotch, M.F.; Islam, A.F.; Klein, B.E.; Cushman, M.; Wong, T.Y. Traditional and Novel Cardiovascular Risk Factors for Retinal Vein Occlusion: The Multiethnic Study of Atherosclerosis. Investig. Ophthalmol. Vis. Sci. 2008, 49, 4297–4302. [Google Scholar] [CrossRef]
- Lee, J.; Lee, J.S.; Park, S.H.; Shin, S.A.; Kim, K. Cohort Profile: The National Health Insurance Service-National Sample Cohort (NHIS-NSC), South Korea. Int. J. Epidemiol. 2017, 46, e15. [Google Scholar] [CrossRef]
- Kim, D.K.; Lee, B.C.; Park, K.J.; Son, G.M. Effect of Obstructive Sleep Apnea on Immunity in Cases of Chronic Rhinosinusitis with Nasal Polyps. Clin. Exp. Otorhinolaryngol. 2021, 14, 390–398. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Comparison (n = 49,584) | SSNHL (n = 49,584) | p Value |
|---|---|---|---|
| Sex | 0.984 | ||
| Male | 16,641 (33.6%) | 16,645 (33.6%) | |
| Female | 32,943 (66.4%) | 32,939 (66.4%) | |
| Ages (years) | 0.995 | ||
| <45 | 19,375 (39.1%) | 19,373 (39.1%) | |
| 45–64 | 18,787 (37.9%) | 18,777 (37.9%) | |
| >64 | 11,422 (23.0%) | 11,434 (23.1%) | |
| Residence | 0.999 | ||
| Seoul (metropolitan) | 9402 (19.0%) | 9399 (19.0%) | |
| Second area (Other metropolitan) | 12,598 (25.4%) | 12,595 (25.4%) | |
| Third area | 27,584 (55.6%) | 27,590 (55.6%) | |
| Household income | 0.999 | ||
| Low (0–30%) | 10,211 (20.6%) | 10,214 (20.6%) | |
| Middle (30–70%) | 18,011 (36.3%) | 18,003 (36.3%) | |
| High (70–100%) | 21,362 (43.1%) | 21,367 (43.1%) | |
| Disability | 1.000 | ||
| No | 47,612 (96.0%) | 47,613 (96.0%) | |
| Yes | 1972 (4.0%) | 1971 (4.0%) | |
| Comorbidities | 0.970 | ||
| No | 25,276 (51.0%) | 25,269 (51.0%) | |
| Yes | 24,308 (49.0%) | 24,315 (49.0%) |
| Variables | N | Case | Incidence | Unadjusted HR (95% CI) | Adjusted HR (95% CI) |
|---|---|---|---|---|---|
| Group | |||||
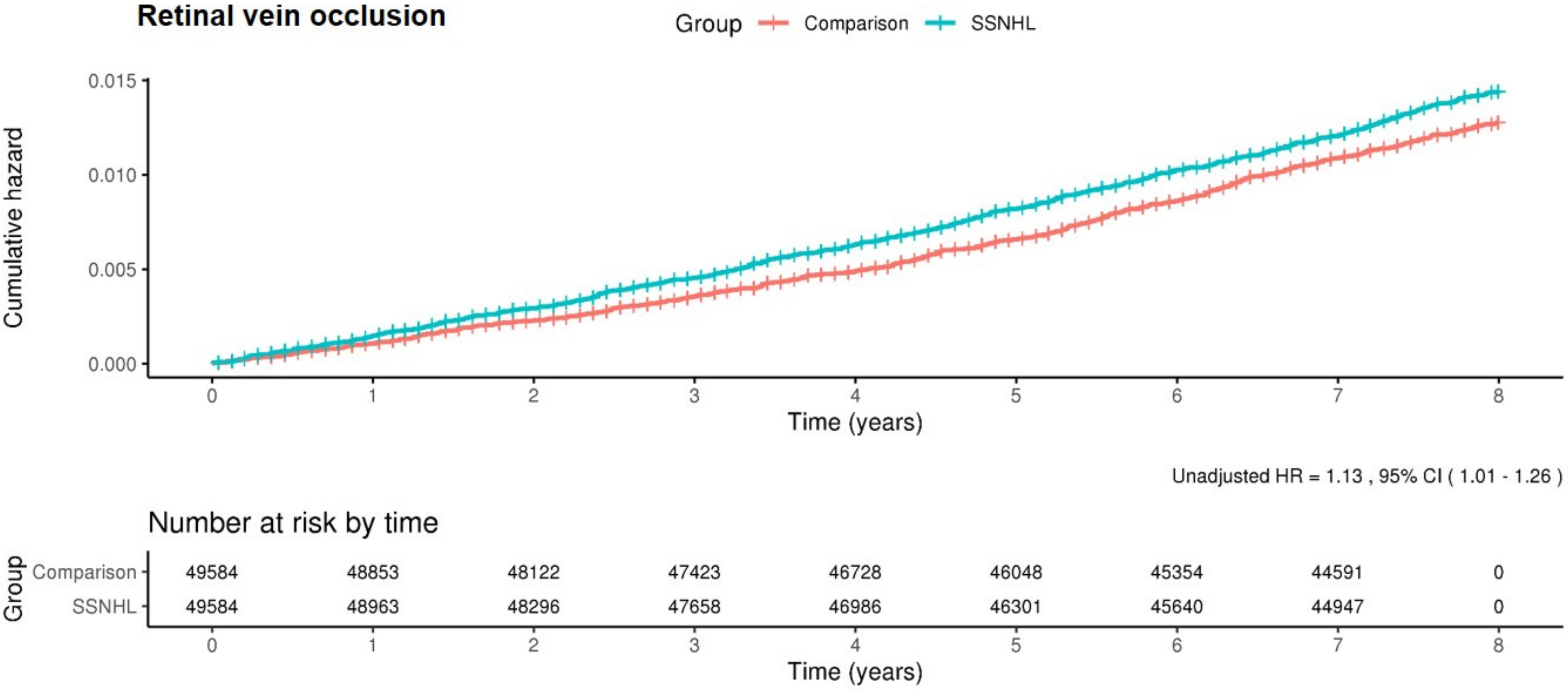
| Comparison group | 49,584 | 592 | 1.6 | 1 (ref) | 1 (ref) |
| SSNHL group | 49,584 | 673 | 1.8 | 1.13 (1.01–1.26) * | 1.13 (1.01–1.26) * |
| Sex | |||||
| Male | 33,286 | 390 | 1.6 | 1 (ref) | 1 (ref) |
| Female | 65,882 | 875 | 1.7 | 1.1 (0.98–1.24) | 1.05 (0.93–1.18) |
| Ages (years) | |||||
| <45 | 38,748 | 112 | 0.4 | 1 (ref) | 1 (ref) |
| 45–64 | 37,564 | 693 | 2.4 | 6.61 (5.42–8.08) *** | 4.88 (3.96–6.03) *** |
| >64 | 22,856 | 460 | 3 | 8.52 (6.93–10.48) *** | 5.73 (4.59–7.16) *** |
| Residence | |||||
| Seoul | 18,801 | 212 | 1.5 | 1 (ref) | 1 (ref) |
| 2nd area | 25,193 | 297 | 1.6 | 1.06 (0.89–1.26) | 1.07 (0.9–1.28) |
| 3rd area | 55,174 | 756 | 1.8 | 1.24 (1.06–1.44) ** | 1.16 (0.99–1.35) |
| Household income | |||||
| Low (0–30%) | 20,425 | 274 | 1.8 | 1 (ref) | 1 (ref) |
| Middle (30–70%) | 36,014 | 458 | 1.7 | 0.93 (0.8–1.08) | 1.04 (0.9–1.21) |
| High (70–100%) | 42,729 | 533 | 1.7 | 0.92 (0.79–1.06) | 0.94 (0.82–1.09) |
| Disability | |||||
| No | 95,225 | 1196 | 1.7 | 1 (ref) | 1 (ref) |
| Yes | 3943 | 69 | 2.5 | 1.52 (1.19–1.93) ** | 1.14 (0.89–1.46) |
| Comorbidities | |||||
| No | 50,545 | 306 | 0.8 | 1 (ref) | 1 (ref) |
| Yes | 48,623 | 959 | 2.7 | 3.53 (3.11–4.02) *** | 1.91 (1.66–2.19) *** |
| Age (Years) | <45 | 45–64 | >64 | |||
|---|---|---|---|---|---|---|
| Comparison | SSNHL | Comparison | SSNHL | Comparison | SSNHL | |
| uHR (95% CI) | 1.00 (ref) | 0.87 (0.6–1.25) | 1.00 (ref) | 1.12 (0.97–1.3) | 1.00 (ref) | 1.21 (1.01–1.46) * |
| aHR (95% CI) | 1.00 (ref) | 0.86 (0.6–1.25) | 1.00 (ref) | 1.12 (0.97–1.3) | 1.00 (ref) | 1.21 (1.01–1.46) * |
| Sex | Male | Female | ||
|---|---|---|---|---|
| Comparison | SSNHL | Comparison | SSNHL | |
| uHR (95% CI) | 1.00 (ref) | 1.18 (1.03–1.35) * | 1.00 (ref) | 1.03 (0.84–1.25) |
| aHR (95% CI) | 1.00 (ref) | 1.18 (1.03–1.34) * | 1.00 (ref) | 1.03 (0.84–1.25) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.-Y.; Ko, I.; Kim, D.-K. Sudden Sensorineural Hearing Loss May Increase the Risk of Retinal Vein Occlusion: A Nationwide Cohort Study. Healthcare 2022, 10, 408. https://doi.org/10.3390/healthcare10020408
Kim J-Y, Ko I, Kim D-K. Sudden Sensorineural Hearing Loss May Increase the Risk of Retinal Vein Occlusion: A Nationwide Cohort Study. Healthcare. 2022; 10(2):408. https://doi.org/10.3390/healthcare10020408
Chicago/Turabian StyleKim, Jong-Yeup, Inseok Ko, and Dong-Kyu Kim. 2022. "Sudden Sensorineural Hearing Loss May Increase the Risk of Retinal Vein Occlusion: A Nationwide Cohort Study" Healthcare 10, no. 2: 408. https://doi.org/10.3390/healthcare10020408
APA StyleKim, J.-Y., Ko, I., & Kim, D.-K. (2022). Sudden Sensorineural Hearing Loss May Increase the Risk of Retinal Vein Occlusion: A Nationwide Cohort Study. Healthcare, 10(2), 408. https://doi.org/10.3390/healthcare10020408