
Telehealth and Artificial Intelligence Insights into Healthcare during the COVID-19 Pandemic

 ,
,  ,
, 
 , and
, and
Abstract
:
1. Introduction
2. Bibliometric Analysis Methodology
2.1. Source and Search Query
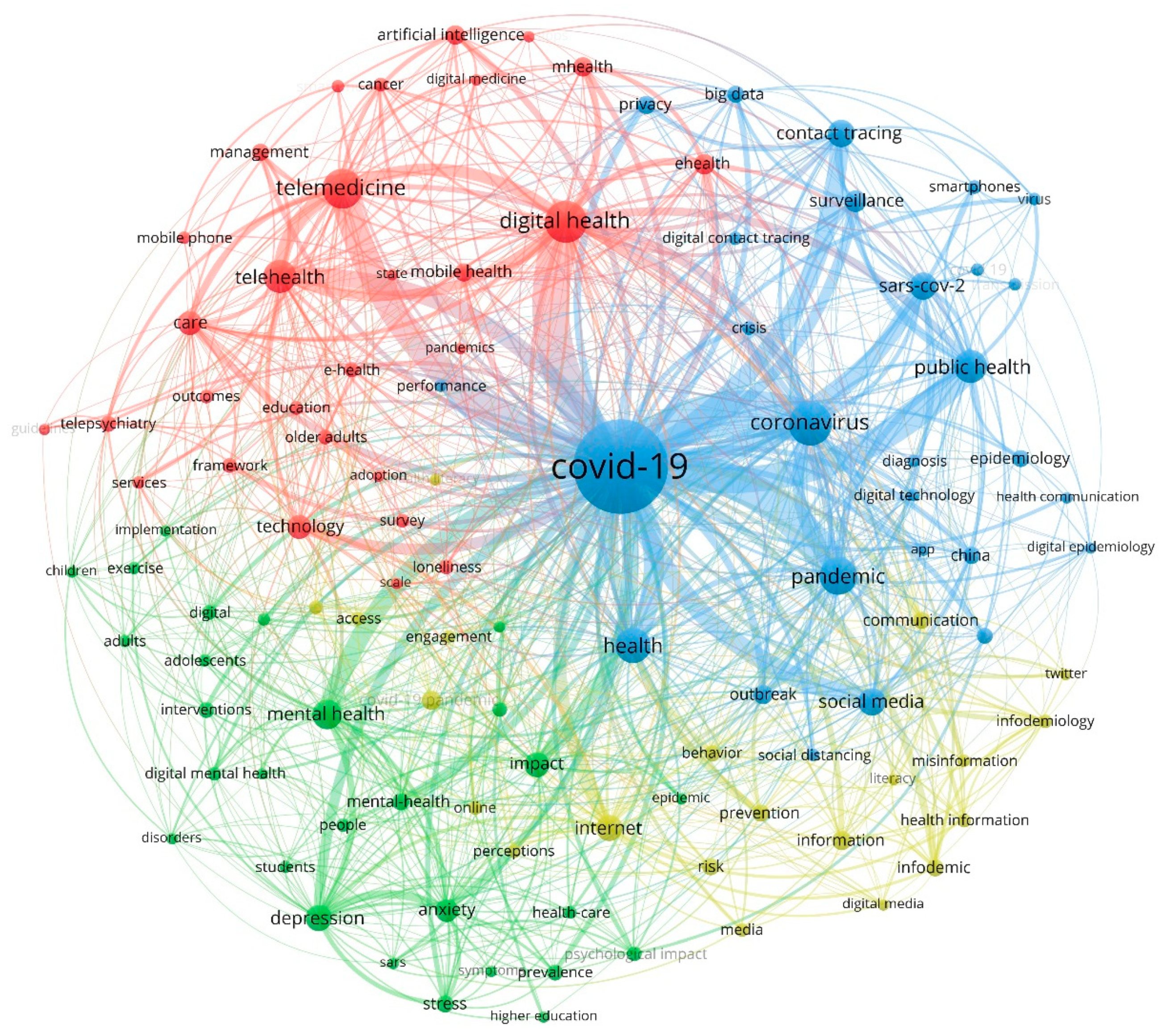
2.2. Bibliometric Maps of Co-Citations
2.3. Hotspots of Papers Related to Digital Health
3. Results
3.1. Source and Search Query
3.2. Bibliometric Maps of Co-Citations
3.3. Hotspots of Papers Related to Digital Health
4. Discussion
4.1. Telemedicine, Telehealth, and Mobile Health (mHealth)
4.2. Telehealthcare’s Role during COVID-19 Pandemic
4.3. Artificial Intelligence in the Healthcare Sector
4.3.1. AI Types and Subgroups
4.3.2. AI Applications
4.3.3. Artificial Intelligence’s Role in COVID-19 Prediction
4.4. Future Perspectives and Potential Challenges Facing Mobile Technologies and Data Sharing in Health and Healthcare
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Abouzid, M.; El-Sherif, D.M.; Al Naggar, Y.; Alshehri, M.M.; Alothman, S.; El-Seedi, H.R.; Trabelsi, R.; Ibrahim, O.M.; Temraz, E.H.; Buimsaedah, A.; et al. Investigating the current environmental situation in the Middle East and North Africa (MENA) region during the third wave of COVID-19 pandemic: Urban vs. rural context. BMC Public Health 2022, 22, 177. [Google Scholar] [CrossRef] [PubMed]
- Abouzid, M.; El-Sherif, D.M.; Eltewacy, N.K.; Dahman, N.B.H.; Okasha, S.A.; Ghozy, S.; Islam, S.M.S. Influence of COVID-19 on lifestyle behaviors in the Middle East and North Africa Region: A survey of 5896 individuals. J. Transl. Med. 2021, 19, 129. [Google Scholar] [CrossRef] [PubMed]
- El-Sherif, D.M.; Abouzid, M.; Gaballah, M.S.; Ahmed, A.A.; Adeel, M.; Sheta, S.M. New approach in SARS-CoV-2 surveillance using biosensor technology: A review. Environ. Sci. Pollut. Res. 2021, 29, 1677–1695. [Google Scholar] [CrossRef] [PubMed]
- Alwashmi, M.F. The Use of Digital Health in the Detection and Management of COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 2906. [Google Scholar] [CrossRef]
- Eloffy, M.G.; El-Sherif, D.M.; Abouzid, M.; Elkodous, M.A.; El-Nakhas, H.S.; Sadek, R.F.; Ghorab, M.A.; Al-Anazi, A.; El-Sayyad, G.S. Proposed approaches for coronaviruses elimination from wastewater: Membrane techniques and nanotechnology solutions. Nanotechnol. Rev. 2021, 11, 1–25. [Google Scholar] [CrossRef]
- Filkins, B.L.; Kim, J.Y.; Roberts, B.; Armstrong, W.; Miller, A.M.; Hultner, M.L.; Castillo, A.P.; Ducom, J.-C.; Topol, E.J.; Steinhubl, S.R. Privacy and security in the era of digital health: What should translational researchers know and do about it? Am. J. Transl. Res. 2016, 8, 1560–1580. [Google Scholar]
- Manogaran, G.; Thota, C.; Lopez, D.; Sundarasekar, R. Big data security intelligence for healthcare industry 4.0. In Cybersecurity for Industry 4.0; Thames, L., Schaefer, D., Eds.; Springer Series in Advanced Manufacturing; Springer International Publishing: Cham, Switzerland, 2017; ISBN 9783319506593. [Google Scholar]
- Pace, P.; Aloi, G.; Gravina, R.; Caliciuri, G.; Fortino, G.; Liotta, A. An Edge-Based Architecture to Support Efficient Applications for Healthcare Industry 4.0. IEEE Trans. Ind. Inform. 2018, 15, 481–489. [Google Scholar] [CrossRef] [Green Version]
- Hathaliya, J.; Sharma, P.; Tanwar, S.; Gupta, R. Blockchain-Based Remote Patient Monitoring in Healthcare 4.0. In Proceedings of the 2019 IEEE 9th International Conference on Advanced Computing, IACC 2019, Tiruchirappalli, India, 13–14 December 2019; pp. 87–91. [Google Scholar]
- Yan, H.; Da Xu, L.; Bi, Z.; Pang, Z.; Zhang, J.; Chen, Y. An emerging technology wearable wireless sensor networks with applications in human health condition monitoring. J. Manag. Anal. 2015, 2, 121–137. [Google Scholar] [CrossRef]
- Reinhardt, I.C.; Oliveira, J.C.; Ring, D.T. Current Perspectives on the Development of Industry 4.0 in the Pharmaceutical Sector. J. Ind. Inf. Integr. 2020, 18, 100131. [Google Scholar] [CrossRef]
- Aceto, G.; Persico, V.; Pescapé, A. Industry 4.0 and Health: Internet of Things, Big Data, and Cloud Computing for Healthcare 4.0. J. Ind. Inf. Integr. 2020, 18, 100129. [Google Scholar] [CrossRef]
- Mavrogiorgou, A.; Kiourtis, A.; Perakis, K.; Miltiadou, D.; Pitsios, S.; Kyriazis, D. Analyzing data and data sources towards a unified approach for ensuring end-to-end data and data sources quality in healthcare 4.0. Comput. Methods Programs Biomed. 2019, 181, 104967. [Google Scholar] [CrossRef] [PubMed]
- Suman, R.; Javaid, M.; Haleem, A.; Vaishya, R.; Bahl, S.; Nandan, D. Sustainability of Coronavirus on Different Surfaces. J. Clin. Exp. Hepatol. 2020, 10, 386–390. [Google Scholar] [CrossRef]
- Shen, Y.-T.; Chen, L.; Yue, W.-W.; Xu, H.-X. Digital Technology-Based Telemedicine for the COVID-19 Pandemic. Front. Med. 2021, 8, 646506. [Google Scholar] [CrossRef]
- Bhaskar, S.; Bradley, S.; Sakhamuri, S.; Moguilner, S.; Chattu, V.K.; Pandya, S.; Schroeder, S.; Ray, D.; Banach, M. Designing Futuristic Telemedicine Using Artificial Intelligence and Robotics in the COVID-19 Era. Front. Public Health 2020, 8, 556789. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, P.; Tesis, A.; Cymberknop, L.J.; Armentano, R.L. Internet of Things and Artificial Intelligence in Healthcare During COVID-19 Pandemic—A South American Perspective. Front. Public Health 2020, 8, 600213. [Google Scholar] [CrossRef] [PubMed]
- Thuemmler, C.; Bai, C. Health 4.0: Application of Industry 4.0 Design Principles in Future Asthma Management. In Health 4.0: How Virtualization and Big Data are Revolutionizing Healthcare; Springer: Cham, Switzerland, 2017; pp. 23–37. [Google Scholar] [CrossRef]
- Javaid, M.; Haleem, A.; Singh, R.P.; Haq, M.I.U.; Raina, A.; Suman, R. Industry 5.0: Potential Applications in COVID-19. J. Ind. Integr. Manag. 2020, 5, 507–530. [Google Scholar] [CrossRef]
- Qadir, J.; Mujeeb-U.-Rahman, M.; Rehmani, M.H.; Pathan, A.-S.K.; Imran, M.A.; Hussain, A.; Rana, R.; Luo, B. IEEE Access Special Section Editorial: Health Informatics for the Developing World. IEEE Access 2017, 5, 27818–27823. [Google Scholar] [CrossRef]
- Haleem, A.; Javaid, M. Medical 4.0 and Its Role in Healthcare During COVID-19 Pandemic: A Review. J. Ind. Integr. Manag. 2020, 5, 531–545. [Google Scholar] [CrossRef]
- Doraiswamy, S.; Abraham, A.; Mamtani, R.; Cheema, S. Use of Telehealth During the COVID-19 Pandemic: Scoping Review. J. Med. Internet Res. 2020, 22, e24087. [Google Scholar] [CrossRef]
- Kernebeck, S.; Busse, T.S.; Böttcher, M.D.; Weitz, J.; Ehlers, J.; Bork, U. Impact of mobile health and medical applications on clinical practice in gastroenterology. World J. Gastroenterol. 2020, 26, 4182–4197. [Google Scholar] [CrossRef]
- Pires, I.M.; Marques, G.; Garcia, N.M.; Flórez-Revuelta, F.; Ponciano, V.; Oniani, S. A Research on the Classification and Applicability of the Mobile Health Applications. J. Pers. Med. 2020, 10, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garg, V.; Brewer, J. Telemedicine Security: A Systematic Review. J. Diabetes Sci. Technol. 2011, 5, 768–777. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, U.V.; Von Jan, U. mHealth Apps and Their Risks—Taking Stock. Stud. Health Technol. Inform. 2016, 226, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Akbar, S.; Coiera, E.; Magrabi, F. Safety concerns with consumer-facing mobile health applications and their consequences: A scoping review. J. Am. Med. Inform. Assoc. 2019, 27, 330–340. [Google Scholar] [CrossRef] [Green Version]
- Elgarahy, A.M.; Hammad, A.; El-Sherif, D.M.; Abouzid, M.; Gaballah, M.S.; Elwakeel, K.Z. Thermochemical conversion strategies of biomass to biofuels, techno-economic and bibliometric analysis: A conceptual review. J. Environ. Chem. Eng. 2021, 9, 106503. [Google Scholar] [CrossRef]
- Abouzid, M.; Główka, A.K.; Karaźniewicz-Łada, M. Trend research of vitamin D receptor: Bibliometric analysis. Health Inform. J. 2021, 27. [Google Scholar] [CrossRef]
- Van Eck, N.J.; Waltman, L. Software survey: VOSviewer, a computer program for bibliometric mapping. Scientometrics 2010, 84, 523–538. [Google Scholar] [CrossRef] [Green Version]
- Weinstein, R.S.; Lopez, A.M.; Joseph, B.A.; Erps, K.A.; Holcomb, M.; Barker, G.P.; Krupinski, E.A. Telemedicine, Telehealth, and Mobile Health Applications That Work: Opportunities and Barriers. Am. J. Med. 2014, 127, 183–187. [Google Scholar] [CrossRef]
- Portnoy, J.; Waller, M.; Elliott, T. Telemedicine in the Era of COVID-19. J. Allergy Clin. Immunol. Pract. 2020, 8, 1489–1491. [Google Scholar] [CrossRef]
- Weightman, M. Digital psychotherapy as an effective and timely treatment option for depression and anxiety disorders: Implications for rural and remote practice. J. Int. Med. Res. 2020, 48, 1–7. [Google Scholar] [CrossRef]
- Torous, J.; Keshavan, M. COVID-19, mobile health and serious mental illness. Schizophr. Res. 2020, 218, 36–37. [Google Scholar] [CrossRef] [PubMed]
- Adejoh, S.O.; Boele, F.; Akeju, D.; Dandadzi, A.; Nabirye, E.; Namisango, E.; Namukwaya, E.; Ebenso, B.; Nkhoma, K.; Allsop, M.J. The role, impact, and support of informal caregivers in the delivery of palliative care for patients with advanced cancer: A multi-country qualitative study. Palliat. Med. 2020, 35, 552–562. [Google Scholar] [CrossRef] [PubMed]
- 2022 Amwell Review: Pros, Cons, Cost and More. Available online: https://www.healthline.com/health/mental-health/amwell-reviews (accessed on 8 February 2021).
- Kurtzman, G.W.; Keshav, M.A.; Satish, N.P.; Patel, M.S. Scheduling primary care appointments online: Differences in availability based on health insurance. Healthcare 2018, 6, 186–190. [Google Scholar] [CrossRef]
- Jiang, X.; Xie, H.; Tang, R.; Du, Y.; Li, T.; Gao, J.; Xu, X.; Jiang, S.; Zhao, T.; Zhao, W.; et al. Characteristics of Online Health Care Services from China’s Largest Online Medical Platform: Cross-sectional Survey Study. J. Med. Internet Res. 2021, 23, e25817. [Google Scholar] [CrossRef] [PubMed]
- Salisbury, C.; Quigley, A.; Hex, N.; Aznar, C. Private Video Consultation Services and the Future of Primary Care. J. Med. Internet Res. 2020, 22, e19415. [Google Scholar] [CrossRef]
- Ahmed, S.; Sanghvi, K.; Yeo, D. Telemedicine takes centre stage during COVID-19 pandemic. BMJ Innov. 2020, 6, 252–254. [Google Scholar] [CrossRef]
- Bhaskar, S.; Bradley, S.; Chattu, V.K.; Adisesh, A.; Nurtazina, A.; Kyrykbayeva, S.; Sakhamuri, S.; Yaya, S.; Sunil, T.; Thomas, P.; et al. Telemedicine Across the Globe-Position Paper From the COVID-19 Pandemic Health System Resilience PROGRAM (REPROGRAM) International Consortium (Part 1). Front. Public Health 2020, 8, 556720. [Google Scholar] [CrossRef]
- Qare—Téléconsultation Médicale en Ligne 7j/7. Available online: https://www.qare.fr/ (accessed on 8 February 2021).
- Home—Doctor Care Anywhere Ireland. Available online: https://shop.doctorcareanywhere.ie/pages/home?gclsrc=aw.ds&gclid=CjwKCAiAgbiQBhAHEiwAuQ6Bkp12eybwGNAgzO2GDe3s8b8rdWxgIzIlrBrskExQJotKCtJofWD7NRoCfT0QAvD_BwE (accessed on 8 February 2021).
- Rutherford, E.; Noray, R.; Hearráin, C.; Quinlan, K.; Hegarty, A.; Ekpotu, L.; Arize, C.; Fabamwo, F.; Alrubaiaan, A.; Bhupalan, A.; et al. Potential Benefits and Drawbacks of Virtual Clinics in General Surgery: Pilot Cross-Sectional Questionnaire Study. JMIR Perioper. Med. 2020, 3, e12491. [Google Scholar] [CrossRef]
- Book an Appointment with Your Doctor Online|Okadoc. Available online: https://www.okadoc.com/ (accessed on 8 February 2021).
- Maple: Online Doctors, Virtual Health & Prescriptions in Canada. Available online: https://www.getmaple.ca (accessed on 8 February 2021).
- TeleClinic +Ihr Online-Arzt: Arztgespräch, Rezept & Krankschreibung in Minuten. Available online: https://www.teleclinic.com/ (accessed on 8 February 2021).
- Digital health and COVID-19. Bull. World Health Organ. 2020, 98, 731–732. [CrossRef]
- Narla, N.P.; Surmeli, A.; Kivlehan, S.M. Agile Application of Digital Health Interventions during the COVID-19 Refugee Response. Ann. Glob. Health 2020, 86, 135. [Google Scholar] [CrossRef]
- LittleDot-Stručni Medicinski Savjeti za Zdravlje-Dostupno 0–24. Available online: https://littledotapp.com/hr/ (accessed on 8 February 2021).
- Alanzi, T. A Review of Mobile Applications Available in the App and Google Play Stores Used During the COVID-19 Outbreak. J. Multidiscip. Health 2021, 14, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, N.; Jain, P.; Pathak, R.; Gupta, R. Telemedicine in India: A tool for transforming health care in the era of COVID-19 pandemic. J. Educ. Health Promot. 2020, 9, 190. [Google Scholar] [CrossRef] [PubMed]
- Онлайн-кoнсультация врача–задать вoпрoс дoктoру в Яндекс Здoрoвь е. Available online: https://health.yandex.ru/BwE (accessed on 8 February 2021).
- Book Online Doctor|DoctorCam|Telehealth Service. Available online: https://doctorcam.com.au/?gclid=CjwKCAiAgbiQBhAHEiwAuQ6Bkl_hk1DPuD-syAaIW8ljVyzrn4rm6eNRcW4A5UD1ZXOOXYy_U0QGuRoC0VEQAvD_BwE (accessed on 8 February 2021).
- Farid, S.F. Conceptual Framework of the Impact of Health Technology on Healthcare System. Front. Pharmacol. 2019, 10, 933. [Google Scholar] [CrossRef] [PubMed]
- Udok|Online Medical Consultations and Mobile Covid Testing. Available online: https://udok.co.za/ (accessed on 8 February 2021).
- Nigeria’s #1 Telemedicine Provider|Health Connect 24x7. Available online: https://www.healthconnect247.com/ (accessed on 8 February 2021).
- Caetano, R.; Silva, A.B.; Guedes, A.C.C.M.; Paiva, C.C.N.; Ribeiro, G.D.R.; Santos, D.L.; Silva, R.M.D. Challenges and opportunities for telehealth during the COVID-19 pandemic: Ideas on spaces and initiatives in the Brazilian context. Cad. Saude Publica 2020, 36, e00088920. [Google Scholar] [CrossRef]
- McCarthy, J.; Minsky, M.L.; Rochester, N.; Shannon, C.E. A proposal for the Dartmouth summer research project on artificial intelligence. AI Mag. 2006, 27, 12–14. [Google Scholar]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef]
- Robot, I. Artificial Intelligence. Philos. Through Film. 2014, 102–129. [Google Scholar] [CrossRef]
- Hassani, H.; Silva, E.S.; Unger, S.; Tajmazinani, M.; Mac Feely, S. Artificial Intelligence (AI) or Intelligence Augmentation (IA): What Is the Future? AI 2020, 1, 143–155. [Google Scholar] [CrossRef]
- Cuzzolin, F.; Morelli, A.; Cîrstea, B.; Sahakian, B.J. Knowing me, knowing you: Theory of mind in AI. Psychol. Med. 2020, 50, 1057–1061. [Google Scholar] [CrossRef]
- Chatila, R.; Renaudo, E.; Andries, M.; Chavez-Garcia, R.-O.; Luce-Vayrac, P.; Gottstein, R.; Alami, R.; Clodic, A.; Devin, S.; Girard, B.; et al. Toward Self-Aware Robots. Front. Robot. AI 2018, 5. [Google Scholar] [CrossRef] [Green Version]
- Rivoltella, P.C. The third age of the media. Res. Educ. Media 2018, 10, 1–2. [Google Scholar] [CrossRef] [Green Version]
- Zhang, C.; Lu, Y. Study on artificial intelligence: The state of the art and future prospects. J. Ind. Inf. Integr. 2021, 23, 100224. [Google Scholar] [CrossRef]
- Reddy, P.P. EasyChair Preprint Artificial Superintelligence: An AI That Makes Better AI’ s Recursively. EasyChair Prepr. 2020, 4077, 11. [Google Scholar]
- Zhang, Y.; Balochian, S.; Agarwal, P.; Bhatnagar, V.; Housheya, O.J. Artificial intelligence and its applications. Math. Probl. Eng. 2014, 2014, 840491. [Google Scholar] [CrossRef] [Green Version]
- Venna, S.R.; Tavanaei, A.; Gottumukkala, R.N.; Raghavan, V.V.; Maida, A.S.; Nichols, S. A Novel Data-Driven Model for Real-Time Influenza Forecasting. IEEE Access 2018, 7, 7691–7701. [Google Scholar] [CrossRef]
- Ahmed, A.A.; Abouzid, M. Arbidol targeting influenza virus A Hemagglutinin; A comparative study. Biophys. Chem. 2021, 277, 106663. [Google Scholar] [CrossRef]
- Hu, H.; Wang, H.; Wang, F.; Langley, D.; Avram, A.; Liu, M. Prediction of influenza-like illness based on the improved artificial tree algorithm and artificial neural network. Sci. Rep. 2018, 8, 4895. [Google Scholar] [CrossRef]
- Lu, F.S.; Hattab, M.W.; Clemente, C.L.; Biggerstaff, M.; Santillana, M. Improved state-level influenza nowcasting in the United States leveraging Internet-based data and network approaches. Nat. Commun. 2019, 10, 147. [Google Scholar] [CrossRef]
- Boulos, M.N.K.; Peng, G.; VoPham, T. An overview of GeoAI applications in health and healthcare. Int. J. Health Geogr. 2019, 18, 7. [Google Scholar] [CrossRef]
- Shamout, F.E.; Shen, Y.; Wu, N.; Kaku, A.; Park, J.; Makino, T.; Jastrzębski, S.; Witowski, J.; Wang, D.; Zhang, B.; et al. An artificial intelligence system for predicting the deterioration of COVID-19 patients in the emergency department. NPJ Digit. Med. 2021, 4, 80. [Google Scholar] [CrossRef]
- Esposito, A.; Casiraghi, E.; Chiaraviglio, F.; Scarabelli, A.; Stellato, E.; Plensich, G.; Lastella, G.; Di Meglio, L.; Fusco, S.; Avola, E.; et al. Artificial Intelligence in Predicting Clinical Outcome in COVID-19 Patients from Clinical, Biochemical and a Qualitative Chest X-Ray Scoring System. Rep. Med. Imaging 2021, 14, 27–39. [Google Scholar] [CrossRef]
- Zoabi, Y.; Deri-Rozov, S.; Shomron, N. Machine learning-based prediction of COVID-19 diagnosis based on symptoms. NPJ Digit. Med. 2021, 4, 3. [Google Scholar] [CrossRef] [PubMed]
- Hjelm, N.M. Benefits and drawbacks of telemedicine. J. Telemed. Telecare 2005, 11, 60–70. [Google Scholar] [CrossRef] [PubMed]
- Anane-Sarpong, E.; Wangmo, T.; Ward, C.L.; Sankoh, O.; Tanner, M.; Elger, B.S. You cannot collect data using your own resources and put It on open access: Perspectives from Africa about public health data-sharing. Dev. World Bioeth. 2017, 18, 394–405. [Google Scholar] [CrossRef]
- Luxton, D.D.; Kayl, R.A.; Mishkind, M.C. mHealth Data Security: The Need for HIPAA-Compliant Standardization. Telemed. E-Health 2012, 18, 284–288. [Google Scholar] [CrossRef]
- Pisani, E.; AbouZahr, C. Sharing health data: Good intentions are not enough. Bull. World Health Organ. 2010, 88, 462–466. [Google Scholar] [CrossRef]
- Privacy Code of Conduct on Mobile Health Apps|Shaping Europe’s Digital Future. Available online: https://ec.europa.eu/digital-single-market/en/privacy-code-conduct-mobile-health-apps (accessed on 8 February 2021).
- Rumbold, B.; Wenham, C.; Wilson, J. Self-tests for influenza: An empirical ethics investigation. BMC Med. Ethics 2017, 18, 33. [Google Scholar] [CrossRef] [Green Version]
- Van Panhuis, W.G.; Paul, P.; Emerson, C.; Grefenstette, J.; Wilder, R.; Herbst, A.J.; Heymann, D.; Burke, D.S. A systematic review of barriers to data sharing in public health. BMC Public Health 2014, 14, 1144. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Technology | Feature |
|---|---|
| Telemedicine |
|
| Biosensors |
|
| MIoT |
|
| Robotics |
|
| Cloud storage platform |
|
| Data security |
|
| AI |
|
| Analytics of big data |
|
| Bioactuators |
|
| Blockchain |
|
| Information technology |
|
| Imaging technologies |
|
| Additive manufacturing |
|
| Nanomedicine |
|
| App Name | Country | Launch Date | Description |
|---|---|---|---|
| Amwell | USA | June 2006 | Amwell is a telehealth platform that offers telemedicine services for healthcare providers and their patients [36]. |
| Zocdoc | USA | April 2007 | Zocdoc is a technology company that provides an online appointment scheduling platform [37]. |
| Ping An Good Doctor | China | April 2015 | A mobile platform for online consultations, hospital referrals, and appointments (Internet hospital) providing online healthcare services [38]. |
| Babylon | UK | January 2013 | Babylon is a teleconsultation app that provides many services on behalf of general practice in London [39]. |
| KRY | Sweden | April 2014 | KRY is a health tech company that provides consultations via smartphone instead of conventional face-to-face appointments for primary care [39]. |
| Doctor Anywhere | Singapore | 2016 | Doctor Anywhere is a digital platform offering quick access to health services [40]. |
| Qare | France | 2016 | Qare is a platform that provides medical video consultation services [41,42]. |
| Videodoc | Ireland | July 2014 | VideoDoc is a healthcare and medical service that offers scaled access to online healthcare services [43,44]. |
| Okadoc | UAE | 2018 | Okadoc is an online appointment booking platform to connect healthcare professionals with their patients [45]. |
| MediQuo | Spain | 2017 | MediQuo is a 24/7 medical chat app for healthcare providers and their patients [41]. |
| Maple | Canada | July 2015 | Maple is a virtual care platform. Through Maple, you can speak with doctors through text or video, receive diagnosis and prescriptions. [46]. |
| TeleClinic | Germany | 2015 | TeleClinic is a telemedicine platform that enables simple and secure communication between healthcare providers and patients [47]. |
| SehatPedia | Indonesia | February 2019 | The Indonesian MOH launched SehatPedia App to facilitate access to healthcare providers [48]. |
| HERA | Turkey | 2018 | The HERA App is a health platform for the Syrian refugee population in Turkey. It provides services in the three most commonly spoken local languages: Arabic, Turkish, and English [49]. |
| Little Dot | Croatia | 2006 | Little Dot is a health platform for remote video consultations from the user’s home [50]. |
| Al-Sehha | Saudi Arabia | Dec. 2017 | The Saudi Arabian MOH created the Al-Sehha mobile app. It provides e-consultations in audio and video modes for users at home [51]. |
| Practo | India | 2008 | Practo is a mHealth platform that provides access to a vast network of doctors and clinics in India. It connects patients with healthcare providers through calls or chats [52]. |
| Yandex Health | Russia | November 2016 | Yandex Health is an online consultation with doctors (all specialists) [53]. |
| Instant Consult | Australia | 2017 | Instant Consult connects doctors with patients instantly for online health consultations via video call [54]. |
| Vezeeta | Egypt | February 2012 | Vezeeta is a digital healthcare platform that provides teleconsultations and booking services for private clinics [55]. |
| Udok | South Africa | 2018 | Udok ia developed a telehealthcare system to connect medical practitioners with patients remotely [56]. |
| Health Connect | Nigeria | 2018 | Health Connect is a telemedicine app [57]. |
| AI Type | Properties | Ref. |
|---|---|---|
| Functionality based | ||
| Reactive Machines |
| [61] |
| Limited Memory |
| [62] |
| Theory of Mind |
| [63] |
| Self-Aware |
| [64] |
| Technology-based | ||
| Artificial Narrow Intelligence (ANI) |
| [65] |
| Artificial General Intelligence |
| [66] |
| Artificial Super Intelligence (ASI) |
| [67]. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
El-Sherif, D.M.; Abouzid, M.; Elzarif, M.T.; Ahmed, A.A.; Albakri, A.; Alshehri, M.M. Telehealth and Artificial Intelligence Insights into Healthcare during the COVID-19 Pandemic. Healthcare 2022, 10, 385. https://doi.org/10.3390/healthcare10020385
El-Sherif DM, Abouzid M, Elzarif MT, Ahmed AA, Albakri A, Alshehri MM. Telehealth and Artificial Intelligence Insights into Healthcare during the COVID-19 Pandemic. Healthcare. 2022; 10(2):385. https://doi.org/10.3390/healthcare10020385
Chicago/Turabian StyleEl-Sherif, Dina M., Mohamed Abouzid, Mohamed Tarek Elzarif, Alhassan Ali Ahmed, Ashwag Albakri, and Mohammed M. Alshehri. 2022. "Telehealth and Artificial Intelligence Insights into Healthcare during the COVID-19 Pandemic" Healthcare 10, no. 2: 385. https://doi.org/10.3390/healthcare10020385
APA StyleEl-Sherif, D. M., Abouzid, M., Elzarif, M. T., Ahmed, A. A., Albakri, A., & Alshehri, M. M. (2022). Telehealth and Artificial Intelligence Insights into Healthcare during the COVID-19 Pandemic. Healthcare, 10(2), 385. https://doi.org/10.3390/healthcare10020385