
Has the COVID-19 Pandemic Affected the Prevalence of Diabetic Ketoacidosis in Polish Children with Newly Diagnosed Type 1 Diabetes? An Example of the Largest Polish Pediatric Diabetes Center (Upper Silesia—Katowice, Poland)

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lu, X.; Zhang, L.; Du, H.; Zhang, J.; Li, Y.Y.; Qu, J.; Zhang, W.; Wang, Y.; Bao, S.; Li, Y.; et al. SARS-CoV-2 Infection in Children. N. Engl. J. Med. 2020, 382, 1663–1665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ludvigsson, J.F. Systematic Review of COVID-19 in Children Shows Milder Cases and a Better Prognosis than Adults. Acta Paediatr. 2020, 109, 1088–1095. [Google Scholar] [CrossRef] [PubMed]
- Borrelli, M.; Corcione, A.; Castellano, F.; Fiori Nastro, F.; Santamaria, F. Coronavirus Disease 2019 in Children. Front. Pediatr. 2021, 9, 668484. [Google Scholar] [CrossRef] [PubMed]
- Jutzeler, C.R.; Bourguignon, L.; Weis, C.V.; Tong, B.; Wong, C.; Rieck, B.; Pargger, H.; Tschudin-Sutter, S.; Egli, A.; Borgwardt, K.; et al. Comorbidities, Clinical Signs and Symptoms, Laboratory Findings, Imaging Features, Treatment Strategies, and Outcomes in Adult and Pediatric Patients with COVID-19: A Systematic Review and Meta-Analysis. Travel Med. Infect. Dis. 2020, 37, 101825. [Google Scholar] [CrossRef] [PubMed]
- Hoang, A.; Chorath, K.; Moreira, A.; Evans, M.; Burmeister-Morton, F.; Burmeister, F.; Naqvi, R.; Petershack, M.; Moreira, A. COVID-19 in 7780 Pediatric Patients: A Systematic Review. EClinicalMedicine 2020, 24, 100433. [Google Scholar] [CrossRef] [PubMed]
- Williams, R.; Colagiuri, S. International Diabetes Federation IDF Diabetes Atlas, 9th ed.; International Diabetes Federation: Brussels, Belgium, 2019; pp. 32–56. [Google Scholar]
- Cardona-Hernandez, R.; Cherubini, V.; Iafusco, D.; Schiaffini, R.; Luo, X.; Maahs, D.M. Children and Youth with Diabetes Are Not at Increased Risk for Hospitalization Due to COVID-19. Pediatr. Diabetes 2021, 22, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Elbarbary, N.S.; dos Santos, T.J.; de Beaufort, C.; Agwu, J.C.; Calliari, L.E.; Scaramuzza, A.E. COVID-19 Outbreak and Pediatric Diabetes: Perceptions of Health Care Professionals Worldwide. Pediatr. Diabetes 2020, 21, 1083–1092. [Google Scholar] [CrossRef]
- d’Annunzio, G.; Maffeis, C.; Cherubini, V.; Rabbone, I.; Scaramuzza, A.; Schiaffini, R.; Minuto, N.; Piccolo, G.; Maghnie, M. Caring for Children and Adolescents with Type 1 Diabetes Mellitus: Italian Society for Pediatric Endocrinology and Diabetology (ISPED) Statements during COVID-19 Pandemia. Diabetes Res. Clin. Pract. 2020, 168, 108372. [Google Scholar] [CrossRef]
- Cherubini, V.; Gohil, A.; Addala, A.; Zanfardino, A.; Iafusco, D.; Hannon, T.; Maahs, D.M. Unintended Consequences of Coronavirus Disease-2019: Remember General Pediatrics. J. Pediatr. 2020, 223, 197–198. [Google Scholar] [CrossRef]
- Wolfsdorf, J.I.; Allgrove, J.; Craig, M.E.; Edge, J.; Glaser, N.; Jain, V.; Lee, W.W.; Mungai, L.N.; Rosenbloom, A.L.; Sperling, M.A.; et al. Diabetic Ketoacidosis and Hyperglycemic Hyperosmolar State. Pediatr. Diabetes 2014, 15, 154–179. [Google Scholar] [CrossRef]
- Wolfsdorf, J.I.; Glaser, N.; Agus, M.; Fritsch, M.; Hanas, R.; Rewers, A.; Sperling, M.A.; Codner, E. ISPAD Clinical Practice Consensus Guidelines 2018: Diabetic Ketoacidosis and the Hyperglycemic Hyperosmolar State. Pediatr. Diabetes 2018, 19, 155–177. [Google Scholar] [CrossRef] [PubMed]
- Niechciał, E.; Skowrońska, B.; Michalak, M.; Fichna, P. Ketoacidosis at Diagnosis of Type 1 Diabetes in Children and Adolescents from Wielkopolska Province in Poland: Prevalence, Risk Factors and Clinical Presentation. Clin. Diabetol. 2019, 7, 272–278. [Google Scholar] [CrossRef]
- Szypowska, A.; Dżygało, K.; Wysocka-Mincewicz, M.; Mazur, A.; Lisowicz, L.; Ben-Skowronek, I.; Sieniawska, J.; Klonowska, B.; Charemska, D.; Nawrotek, J.; et al. High Incidence of Diabetic Ketoacidosis at Diagnosis of Type 1 Diabetes among Polish Children Aged 10-12 and under 5 Years of Age: A Multicenter Study. Pediatr. Diabetes 2017, 18, 722–728. [Google Scholar] [CrossRef] [PubMed]
- Wojcik, M.; Sudacka, M.; Wasyl, B.; Ciechanowska, M.; Nazim, J.; Stelmach, M.; Starzyk, J.B. Incidence of Type 1 Diabetes Mellitus during 26 Years of Observation and Prevalence of Diabetic Ketoacidosis in the Later Years. Eur. J. Pediatr. 2015, 174, 1319–1324. [Google Scholar] [CrossRef] [PubMed]
- Olak-Białoń, B.; Deja, G.; Jarosz-Chobot, P.; Buczkowska, E.O. The occurrence and analysis of chosen risk factors of DKA among children with new onset of DMT1. Pediatr. Endocrinol. Diabetes Metab. 2007, 13, 85–90. [Google Scholar]
- Chumięcki, M.; Prokopowicz, Z.; Deja, R.; Jarosz-Chobot, P. Frequency and clinical manifestation of diabetic ketoacidosis in children with newly diagnosed type 1 diabetes. Pediatr. Endocrinol. Diabetes Metab. 2013, 19, 143–147. [Google Scholar]
- Manuwald, U.; Schoffer, O.; Hegewald, J.; Große, J.; Kugler, J.; Kapellen, T.M.; Kiess, W.; Rothe, U. Ketoacidosis at Onset of Type 1 Diabetes in Children up to 14 Years of Age and the Changes over a Period of 18 Years in Saxony, Eastern-Germany: A Population Based Register Study. PLoS ONE 2019, 14, e0218807. [Google Scholar] [CrossRef]
- Ješić, M.D.; Ješić, M.M.; Stanisavljević, D.; Zdravković, V.; Bojić, V.; Vranješ, M.; Trifunović, D.; Necić, S.; Sajić, S. Ketoacidosis at Presentation of Type 1 Diabetes Mellitus in Children: A Retrospective 20-Year Experience from a Tertiary Care Hospital in Serbia. Eur. J. Pediatr. 2013, 172, 1581–1585. [Google Scholar] [CrossRef]
- Choleau, C.; Maitre, J.; Filipovic Pierucci, A.; Elie, C.; Barat, P.; Bertrand, A.-M.; de Kerdanet, M.; Letallec, C.; Levy-Marchal, C.; Nicolino, M.; et al. Ketoacidosis at Diagnosis of Type 1 Diabetes in French Children and Adolescents. Diabetes Metab. 2014, 40, 137–142. [Google Scholar] [CrossRef]
- Schober, E.; Rami, B.; Waldhoer, T. Diabetic Ketoacidosis at Diagnosis in Austrian Children in 1989–2008: A Population-Based Analysis. Diabetologia 2010, 53, 1057–1061. [Google Scholar] [CrossRef] [Green Version]
- Vukovic, R.; Jesic, M.D.; Vorgucin, I.; Stankovic, S.; Folic, N.; Milenkovic, T.; Sajic, S.; Katanic, D.; Zivic, S.; Markovic, S.; et al. First Report on the Nationwide Incidence of Type 1 Diabetes and Ketoacidosis at Onset in Children in Serbia: A Multicenter Study. Eur. J. Pediatr. 2018, 177, 1155–1162. [Google Scholar] [CrossRef] [PubMed]
- SWEET. An International Network for Pediatric Diabetes Centers List of Members by Category—SWEET Certified Centers of Reference. Available online: https://www.sweet-project.org/members-list.php (accessed on 11 January 2022).
- Fryc, J.; Kalisz, P.; Przybyła, M. Population Vital Statistics and Migrations in Śląskie Voivodship in 2020; Statistical Office in Katowice: Katowice, Poland, 2021; pp. 1–35. [Google Scholar]
- Wolfgram, P.; MacDonald, M. Severe Hypertriglyceridemia Causing Acute Pancreatitis in a Child with New Onset Type I Diabetes Mellitus Presenting in Ketoacidosis. J. Pediatr. Intensive Care 2015, 2, 77–80. [Google Scholar] [CrossRef]
- Gasler, N.; Barnett, P.; McCaslin, I.; Nelson, D.; Trainor, J.; Louie, J.; Kaufman, F.; Quayle, K.; Roback, M.; Malley, R.; et al. Risk Factors for Cerebral Edema in Children with Diabetic Ketoacidosis. N. Engl. J. Med. 2001, 344, 264–269. [Google Scholar]
- Edge, J.A. The Risk and Outcome of Cerebral Oedema Developing during Diabetic Ketoacidosis. Arch. Dis. Child. 2001, 85, 16–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edge, J.A.; Ford-Adams, M.E.; Dunger, D.B. Causes of Death in Children with Insulin Dependent Diabetes 1990–96. Arch. Dis. Child. 1999, 81, 318–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamrath, C.; Mönkemöller, K.; Biester, T.; Rohrer, T.R.; Warncke, K.; Hammersen, J.; Holl, R.W. Ketoacidosis in Children and Adolescents with Newly Diagnosed Type 1 Diabetes During the COVID-19 Pandemic in Germany. JAMA 2020, 324, 801. [Google Scholar] [CrossRef]
- Jacob, R.; Weiser, G.; Krupik, D.; Takagi, D.; Peled, S.; Pines, N.; Hashavya, S.; Gur-Soferman, H.; Gamsu, S.; Kaplan, O.; et al. Diabetic Ketoacidosis at Emergency Department Presentation During the First Months of the SARS-CoV-2 Pandemic in Israel: A Multicenter Cross-Sectional Study. Diabetes 2021, 12, 1569–1574. [Google Scholar] [CrossRef]
- McGlacken-Byrne, S.M.; Drew, S.E.V.; Turner, K.; Peters, C.; Amin, R. The SARS-CoV-2 Pandemic Is Associated with Increased Severity of Presentation of Childhood Onset Type 1 Diabetes Mellitus: A Multi-Centre Study of the First COVID-19 Wave. Diabet Med. 2021, 38, e14640. [Google Scholar] [CrossRef]
- Boboc, A.A.; Novac, C.N.; Ilie, M.T.; Ieșanu, M.I.; Galoș, F.; Bălgrădean, M.; Berghea, E.C.; Ionescu, M.D. The Impact of SARS-CoV-2 Pandemic on the New Cases of T1DM in Children. A Single-Centre Cohort Study. JPM 2021, 11, 551. [Google Scholar] [CrossRef]
- Dżygało, K.; Nowaczyk, J.; Szwilling, A.; Kowalska, A. Increased Frequency of Severe Diabetic Ketoacidosis at Type 1 Diabetes Onset among Children during COVID-19 Pandemic Lockdown: An Observational Cohort Study. pedm 2020, 26, 167–175. [Google Scholar] [CrossRef]
- Zubkiewicz-Kucharska, A.; Seifert, M.; Stępkowski, M.; Noczyńska, A. Diagnosis of Type 1 Diabetes during the SARS-CoV-2 Pandemic: Does Lockdown Affect the Incidence and Clinical Status of Patients? Adv. Clin. Exp. Med. 2021, 30, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, C.; Seckold, R.; Smart, C.; King, B.R.; Howley, P.; Feltrin, R.; Smith, T.A.; Roy, R.; Lopez, P. Increased Paediatric Presentations of Severe Diabetic Ketoacidosis in an Australian Tertiary Centre during the COVID-19 Pandemic. Diabet. Med. 2021, 38, e14417. [Google Scholar] [CrossRef] [PubMed]
- Alaqeel, A.; Aljuraibah, F.; Alsuhaibani, M.; Huneif, M.; Alsaheel, A.; Dubayee, M.A.; Alsaedi, A.; Bakkar, A.; Alnahari, A.; Taha, A.; et al. The Impact of COVID-19 Pandemic Lockdown on the Incidence of New-Onset Type 1 Diabetes and Ketoacidosis Among Saudi Children. Front. Endocrinol. 2021, 12, 669302. [Google Scholar] [CrossRef]
- Ho, J.; Rosolowsky, E.; Pacaud, D.; Huang, C.; Lemay, J.; Brockman, N.; Rath, M.; Doulla, M. Diabetic Ketoacidosis at Type 1 Diabetes Diagnosis in Children during the COVID-19 Pandemic. Pediatr. Diabetes 2021, 22, 552–557. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J. Effect of COVID-19 Pandemic on Treatment of Type 1 Diabetes in Children. Acta Paediatr. 2020, 110, 933–934. [Google Scholar] [CrossRef] [PubMed]
- Bogale, K.T.; Urban, V.; Schaefer, E.; Bangalore Krishna, K. The Impact of COVID-19 Pandemic on Prevalence of Diabetic Ketoacidosis at Diagnosis of Type 1 Diabetes: A Single-Centre Study in Central Pennsylvania. Endocrinol. Diabetes Metab. 2021, 4, e00235. [Google Scholar] [CrossRef]
- Research Report by the Public Opinion Research Center No. 88/2020—Healthcare during the Epidemic 2020. Available online: https://www.cbos.pl/PL/publikacje/public_opinion.php (accessed on 11 January 2022).




{kind=link}
{kind=link}
{kind=link}
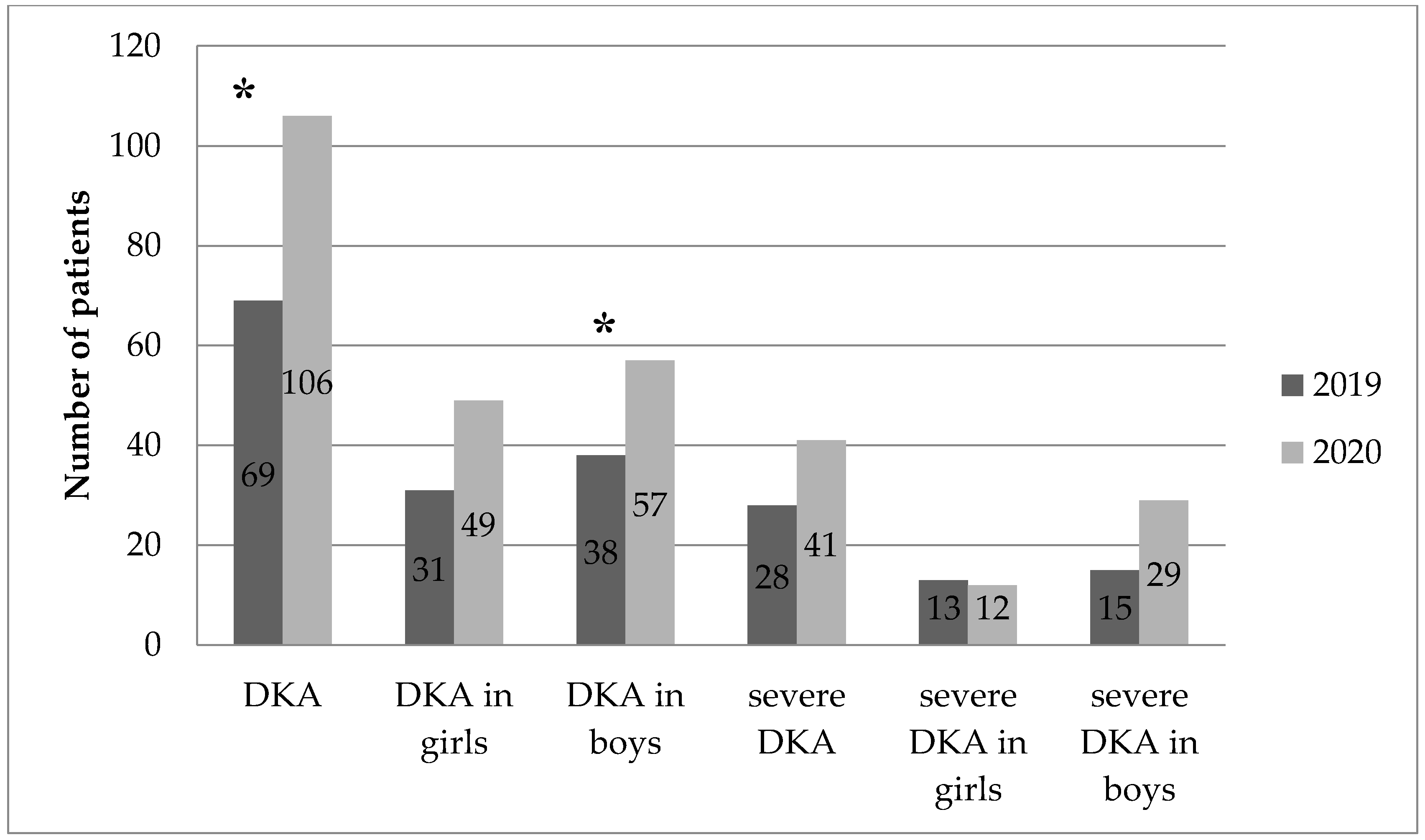
| Variable | Year 2019 | Year 2020 | p | ||
|---|---|---|---|---|---|
| N | % | N | % | ||
| Number of girls | 89 | 45.41 | 113 | 50.67 | 0.091 |
| Number of boys | 107 | 54.59 | 110 | 49.33 | 0.840 |
| Total number of children | 196 | 100 | 223 | 100 | 0.187 |
| Number of girls with DKA | 31 | 15.82 | 49 | 21.97 | 0.248 |
| Number of boys with DKA | 38 | 19.39 | 57 | 25.56 | 0.016 |
| Total number of children with DKA | 69 | 35.20 | 106 | 47.53 | 0.005 |
| Number of girls with severe DKA | 13 | 6.63 | 12 | 5.38 | 0.721 |
| Number of boys with severe DKA | 15 | 7.65 | 29 | 13.00 | 0.108 |
| Total number of children with severe DKA | 28 | 14.07 | 41 | 18.39 | 0.118 |
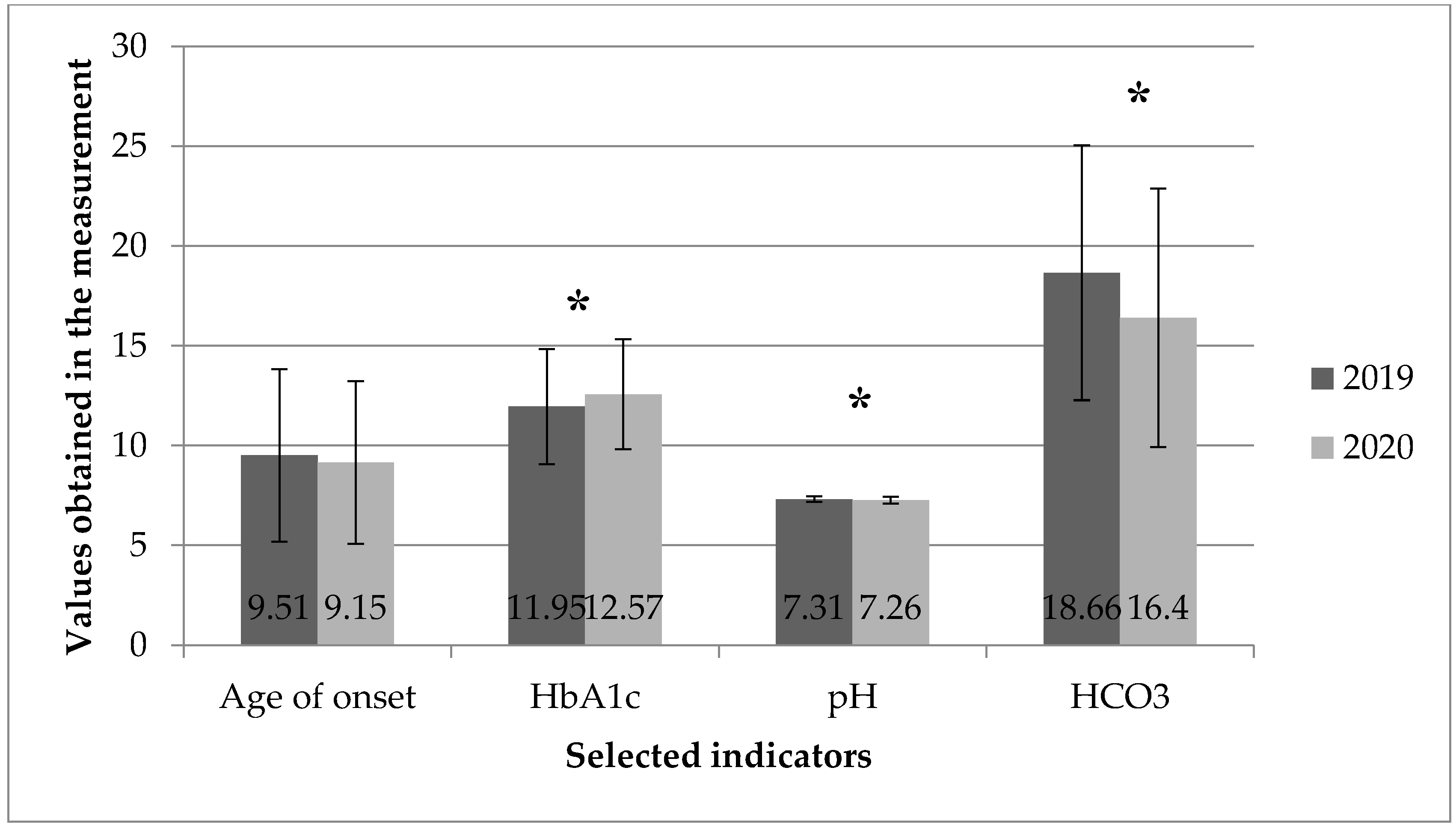
| Testing Variable | Year 2019 | Year 2020 | p | ||||
|---|---|---|---|---|---|---|---|
| N | M | SD | N | M | SD | ||
| Age of onset | 196 | 9.51 | 4.32 | 222 | 9.15 | 4.08 | 0.372 |
| HBA1c | 189 | 11.95 | 2.89 | 221 | 12.57 | 2.75 | 0.025 |
| pH | 180 | 7.31 | 0.14 | 222 | 7.26 | 0.17 | 0.002 |
| HCO3 | 175 | 18.66 | 6.39 | 203 | 16.40 | 6.48 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rusak, E.; Seget, S.; Macherski, M.; Furgał, N.; Dyś, P.; Jarosz-Chobot, P. Has the COVID-19 Pandemic Affected the Prevalence of Diabetic Ketoacidosis in Polish Children with Newly Diagnosed Type 1 Diabetes? An Example of the Largest Polish Pediatric Diabetes Center (Upper Silesia—Katowice, Poland). Healthcare 2022, 10, 348. https://doi.org/10.3390/healthcare10020348
Rusak E, Seget S, Macherski M, Furgał N, Dyś P, Jarosz-Chobot P. Has the COVID-19 Pandemic Affected the Prevalence of Diabetic Ketoacidosis in Polish Children with Newly Diagnosed Type 1 Diabetes? An Example of the Largest Polish Pediatric Diabetes Center (Upper Silesia—Katowice, Poland). Healthcare. 2022; 10(2):348. https://doi.org/10.3390/healthcare10020348
Chicago/Turabian StyleRusak, Ewa, Sebastian Seget, Maksymilian Macherski, Natalia Furgał, Przemysław Dyś, and Przemysława Jarosz-Chobot. 2022. "Has the COVID-19 Pandemic Affected the Prevalence of Diabetic Ketoacidosis in Polish Children with Newly Diagnosed Type 1 Diabetes? An Example of the Largest Polish Pediatric Diabetes Center (Upper Silesia—Katowice, Poland)" Healthcare 10, no. 2: 348. https://doi.org/10.3390/healthcare10020348
APA StyleRusak, E., Seget, S., Macherski, M., Furgał, N., Dyś, P., & Jarosz-Chobot, P. (2022). Has the COVID-19 Pandemic Affected the Prevalence of Diabetic Ketoacidosis in Polish Children with Newly Diagnosed Type 1 Diabetes? An Example of the Largest Polish Pediatric Diabetes Center (Upper Silesia—Katowice, Poland). Healthcare, 10(2), 348. https://doi.org/10.3390/healthcare10020348