
The Effect of Exposure to “Exemption” Video Advertisements for Functional Foods: A Randomized Control Study in Japan

 ,
,
Abstract
:1. Introduction
1.1. What Are “Exemption” Video Advertisements?
1.2. Theoretical Background
1.3. Aim and Hypotheses of the Present Study
- Exposure to “Exemption” video ads increases participants’ belief that “By taking functional foods, I can adopt unhealthy behaviors or I don’t have to adopt healthy behaviors” (FF-CHBs).
- Exposure to “Exemption” video ads increases participants’ intention to take functional foods.
2. Materials and Methods
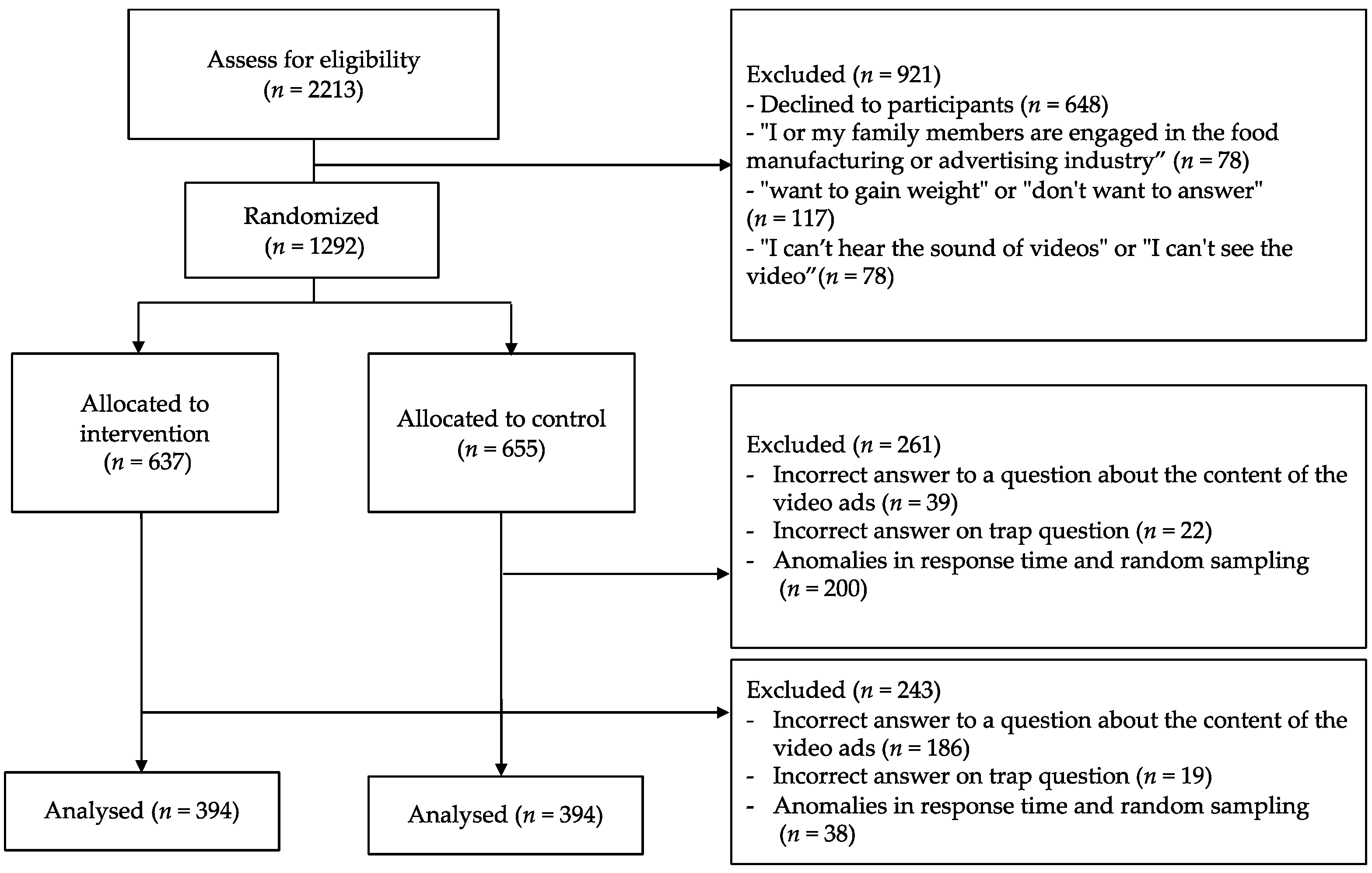
2.1. Participants and Design
2.2. Intervention and Control Videos
2.3. Measures
2.4. Sample Size
2.5. Statistical Analysis
3. Results
3.1. Participants’ Characteristics
3.2. Comparison of Outcomes between Groups
4. Discussion
4.1. Discussion
4.2. Implications for Public Health Institutions and Government
4.3. Implications for Businesses
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Item | Mean | SD | Factor Loading | |
|---|---|---|---|---|
| F1 | F2 | |||
| Factor 1 [By taking functional foods, I can adopt unhealthy behaviors]. | ||||
| When I take functional foods after a meal, I can eat more fat-rich foods. | 2.34 | 0.97 | 0.81 | 0.36 |
| By taking functional foods, I can eat more fat-rich foods in the next meal. | 2.34 | 0.97 | 0.80 | 0.36 |
| By taking functional foods, I can make up for the excess fat intake in my previous meal. | 2.57 | 1.07 | 0.76 | 0.26 |
| By eating functional foods, I can make up for the excessive fat intake of the previous day’s meal. | 2.41 | 1.03 | 0.74 | 0.32 |
| If I take functional foods, I can eat a little too much fat in my diet. | 2.47 | 1.02 | 0.65 | 0.26 |
| Factor 2 [By taking functional foods, I don’t have to adopt healthy behaviors]. | ||||
| If I take functional foods, I don’t need to eat fruits and vegetables to control my weight. | 1.88 | 0.90 | 0.24 | 0.76 |
| If I take functional foods, I don’t have to work out to control my weight. | 1.88 | 0.93 | 0.29 | 0.76 |
| If I take functional foods, I don’t have to restrict my diet to control my weight. | 2.09 | 0.96 | 0.33 | 0.76 |
| Taking functional foods can compensate for lack of exercise. | 1.88 | 0.92 | 0.27 | 0.71 |
References
- Iwatani, S.; Yamamoto, N. Functional food products in Japan: A review. Food Sci. Hum. Wellness 2019, 8, 96–101. [Google Scholar] [CrossRef]
- Hasler, C.M. Functional Foods: Benefits, Concerns and Challenges—A Position Paper from the American Council on Science and Health. J. Nutr. 2002, 132, 3772–3781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dietary Supplements Market to Reach USD 210.3 Billion By 2026|Reports and Data. Available online: https://www.globenewswire.com/news-release/2019/03/25/1760423/0/en/Dietary-Supplements-Market-To-Reach-USD-210-3-Billion-By-2026-Reports-And-Data.html (accessed on 11 February 2021).
- Japan Health and Nutrition Food Association; Tomohisa Shimoda, P. Market for FOSHU and Labeling Authorization Status. Available online: http://www.jhnfa.org (accessed on 7 June 2021).
- Yano Research Institute Ltd. Market Status and Prospects for Dietary Supplements in 2020 Consumer Survey; Yano Research Institute Ltd.: Tokyo, Japan, 2020. [Google Scholar]
- Clark, J.E.; Welch, S. Comparing effectiveness of fat burners and thermogenic supplements to diet and exercise for weight loss and cardiometabolic health: Systematic review and meta-analysis. Nutr. Health 2021, 27, 445–459. [Google Scholar] [CrossRef]
- Batsis, J.A.; Apolzan, J.W.; Bagley, P.J.; Blunt, H.B.; Divan, V.; Gill, S.; Golden, A.; Gundumraj, S.; Heymsfield, S.B.; Kahan, S.; et al. A Systematic Review of Dietary Supplements and Alternative Therapies for Weight Loss. Obesity 2021, 29, 1102–1113. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, M.; Risi, R.; Masi, D.; Caputi, A.; Balena, A.; Rossini, G.; Tuccinardi, D.; Mariani, S.; Basciani, S.; Manfrini, S.; et al. Current Evidence to Propose Different Food Supplements for Weight Loss: A Comprehensive Review. Nutrients 2020, 12, 2873. [Google Scholar] [CrossRef]
- Consumer Affairs Agency Guidelines for Ensuring Transparency of Ex Post Facto Regulation (Ex Post Facto Check) Based on Food Labeling and Other Related Laws and Regulations for Foods with Function Claims. Available online: https://www.caa.go.jp/policies/policy/food_labeling/foods_with_function_claims/pdf/about_foods_with_function_claims_200324_0003.pdf (accessed on 12 March 2021).
- The U.S. Food and Drug Administration. Health Fraud Scams|FDA. Available online: https://www.fda.gov/consumers/health-fraud-scams (accessed on 24 January 2022).
- The Health Sciences Authority SG. Getting Savvy with Health Supplements. Available online: https://www.hsa.gov.sg/consumer-safety/articles/details/health-supplement-regulations (accessed on 24 January 2022).
- Federal Trade Commission. The Truth Behind Weight Loss Ads|FTC Consumer Information. Available online: https://www.consumer.ftc.gov/articles/truth-behind-weight-loss-ads-0#spot (accessed on 4 November 2021).
- Dentsu Inc. Consumer Awareness Survey on Foods with Functional Claims 2016; Dentsu Inc.: Tokyo, Japan, 2016. [Google Scholar]
- Fuji Keizai Group Company Ltd. Results of a Survey on the Domestic Market for Health-Oriented Foods (Foods and Drinks); Fuji Keizai Group Company Ltd.: Tokyo, Japan, 2021. [Google Scholar]
- Kshetri, N. 5G in E-Commerce Activities. IT Prof. 2018, 20, 73–77. [Google Scholar] [CrossRef]
- Iye, R.; Okuhara, T.; Okada, H.; Yokota, R.; Kiuchi, T. A Content Analysis of Video Advertisements for Dietary Supplements in Japan. Healthcare 2021, 9, 742. [Google Scholar] [CrossRef]
- Food Safety Division; Pharmaceutical and Food Safety Bureau; Ministry of Health, Labour and Welfare. How to Use Dietary Supplements Correctly. Available online: https://www.mhlw.go.jp/topics/bukyoku/iyaku/syoku-anzen/dl/kenkou_shokuhin00.pdf (accessed on 12 March 2021).
- Centers for Disease Control and Prevention. Benefits of Physical Activity|Physical Activity|CDC. Available online: https://www.cdc.gov/physicalactivity/basics/pa-health/index.htm (accessed on 1 November 2021).
- Centers for Disease Control and Prevention. Benefits of Healthy Eating|Nutrition|DNPAO|CDC. Available online: https://www.cdc.gov/nutrition/resources-publications/benefits-of-healthy-eating.html (accessed on 16 May 2021).
- Chiou, W.-B.; Yang, C.-C.; Wan, C.-S. Ironic Effects of Dietary Supplementation: Illusory Invulnerability Created by Taking Dietary Supplements Licenses Health-Risk Behaviors. Psychol. Sci. 2011, 22, 1081–1086. [Google Scholar] [CrossRef]
- Chang, Y.Y.C.; Chiou, W. Bin Taking weight-loss supplements may elicit liberation from dietary control. A laboratory experiment. Appetite 2014, 72, 8–12. [Google Scholar] [CrossRef]
- Chang, Y.Y.; Chiou, W. Bin The liberating effect of weight loss supplements on dietary control: A field experiment. Nutrition 2014, 30, 1007–1010. [Google Scholar] [CrossRef]
- Chiou, W.-B.; Wan, C.-S.; Wu, W.-H.; Lee, K.-T. A randomized experiment to examine unintended consequences of dietary supplement use among daily smokers: Taking supplements reduces self-regulation of smoking. Addiction 2011, 106, 2221–2228. [Google Scholar] [CrossRef] [PubMed]
- Karbownik, M.S.; Horne, R.; Paul, E.; Kowalczyk, E.; Szemraj, J. Determinants of Knowledge About Dietary Supplements Among Polish Internet Users: Nationwide Cross-sectional Study. J. Med. Internet Res. 2021, 23, e25228. [Google Scholar] [CrossRef] [PubMed]
- Alowais, M.A.; Selim, M.A.E.-H. Knowledge, attitude, and practices regarding dietary supplements in Saudi Arabia. J. Fam. Med. Prim. Care 2019, 8, 365. [Google Scholar] [CrossRef] [PubMed]
- Rabiau, M.; Knäuper, B.; Miquelon, P. The eternal quest for optimal balance between maximizing pleasure and minimizing harm: The compensatory health beliefs model. Br. J. Health Psychol. 2006, 11, 139–153. [Google Scholar] [CrossRef]
- Zhao, K.; Xu, X.; Zhu, H.; Xu, Q. Compensatory Belief in Health Behavior Management: A Concept Analysis. Front. Psychol. 2021, 12, 3765. [Google Scholar] [CrossRef]
- Knäuper, B.; Rabiau, M.; Cohen, O.; Patriciu, N. Compensatory health beliefs: Scale development and psychometric properties. Psychol. Health 2004, 19, 607–624. [Google Scholar] [CrossRef]
- Hartmann, C.; Keller, C.; Siegrist, M. Compensatory beliefs, nutrition knowledge and eating styles of users and non-users of meal replacement products. Appetite 2016, 105, 775–781. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. 2010. Available online: http://www.consort-statement.org/ (accessed on 30 November 2021).
- Consumer Affairs Agency. About Foods for Specified Health Use. Available online: https://www.caa.go.jp/policies/policy/food_labeling/foods_for_specified_health_uses/ (accessed on 21 March 2021).
- Consumer Affairs Agency. Notified Information Search for Foods with Function Claims. Available online: https://www.caa.go.jp/policies/policy/food_labeling/foods_with_function_claims/search/ (accessed on 21 March 2021).
- Kaklamanou, D.; Armitage, C.J.; Jones, C.R. A further look into compensatory health beliefs: A think aloud study. Br. J. Health Psychol. 2013, 18, 139–154. [Google Scholar] [CrossRef]
- Radtke, T.; Scholz, U.; Keller, R.; Knäuper, B.; Hornung, R. Smoking-specific compensatory health beliefs and the readiness to stop smoking in adolescents. Br. J. Health Psychol. 2011, 16, 610–625. [Google Scholar] [CrossRef]
- Neter, E.; Bagants, L. Compensatory Health Beliefs on Breastfeeding Varying by Breastfeeding Status; A Scale Development. Int. J. Environ. Res. Public Health 2020, 17, 5759. [Google Scholar] [CrossRef]
- Gollwitzer, P.M.; Brandstätter, V. Implementation Intentions and Effective Goal Pursuit. J. Personal. Soc. Psychol. 1997, 73, 186–199. [Google Scholar] [CrossRef]
- Okuhara, T.; Ishikawa, H.; Okada, M.; Kato, M.; Kiuchi, T. Persuasiveness of statistics and patients’ and mothers’ narratives in human papillomavirus vaccine recommendation messages: A randomized controlled study in Japan. Front. Public Health 2018, 6, 105. [Google Scholar] [CrossRef] [PubMed]
- Okuhara, T.; Okada, H.; Kiuchi, T. Examining persuasive message type to encourage staying at home during the COVID-19 pandemic and social lockdown: A randomized controlled study in Japan. Patient Educ. Couns. 2020, 103, 2588. [Google Scholar] [CrossRef] [PubMed]
- Richard, F.D.; Charles, F.; Bond, J.; Stokes-Zoota, J.J. One Hundred Years of Social Psychology Quantitatively Described. Rev. Gen. Psychol. 2003, 7, 331–363. [Google Scholar] [CrossRef] [Green Version]
- Wan, F. Statistical analysis of two arm randomized pre-post designs with one post-treatment measurement. BMC Med. Res. Methodol. 2021, 21, 150. [Google Scholar] [CrossRef]
- Lenhard, W.; Lenhard, A. Computation of Effect Sizes. Available online: https://www.psychometrica.de/effect_size.html (accessed on 10 November 2021).
- Funder, D.C.; Ozer, D.J. Evaluating Effect Size in Psychological Research: Sense and Nonsense. Adv. Methods Pract. Psychol. Sci. 2019, 2, 156–168. [Google Scholar] [CrossRef]
- Federal Trade Commission. Dietary Supplements: An Advertising Guide for Industry|Federal Trade Commission. Available online: https://www.ftc.gov/tips-advice/business-center/guidance/dietary-supplements-advertising-guide-industry#A (accessed on 11 February 2021).
- Tokyo Metropolitan Institute of Health and Safety. About the Workshop for Business Handling Dietary Supplements. Available online: http://www.tokyo-eiken.go.jp/kj_shoku/kenkounavi/koushukai20pr/ (accessed on 20 March 2021).
- Japan Health Food and Nutrition Food Association. Available online: https://www.jhnfa.org/ (accessed on 20 March 2021).
| Intervention (n = 394) n (%) | Control (n = 394) n (%) | Overall (n = 788) n (%) | |
|---|---|---|---|
| Gender, male | 166 (42.1) | 190 (48.2) | 356 (45.2) |
| Age, years | |||
| 18–29 | 96 (24.4) | 93 (23.6) | 189 (24.0) |
| 30–39 | 105 (26.6) | 95 (24.1) | 200 (25.4) |
| 40–49 | 114 (28.9) | 121 (30.7) | 235 (29.8) |
| 50–59 | 60 (15.2) | 64 (16.2) | 124 (15.7) |
| 60–64 | 19 (4.8) | 21 (5.3) | 40 (5.1) |
| BMI, kg/m2 | |||
| <18.5 | 40 (10.2) | 53 (13.5) | 93 (11.8) |
| 18.5–25.0 | 275 (69.8) | 261 (66.2) | 536 (68.0) |
| ≥25.0 | 79 (20.1) | 80 (20.3) | 159 (20.2) |
| Weight management goal | |||
| Want to gain weight | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Want to maintain weight | 112 (28.4) | 131 (33.2) | 243 (30.8) |
| Want to lose weight | 282 (71.6) | 263 (66.8) | 545 (69.2) |
| Don’t want to answer | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Highest education level | |||
| Less than high school | 7 (1.8) | 7 (1.8) | 14 (1.8) |
| High school graduate | 85 (21.6) | 96 (24.4) | 181 (23.0) |
| Some college | 84 (21.3) | 77 (19.5) | 161 (20.4) |
| College graduate | 189 (48.0) | 186 (47.2) | 375 (47.6) |
| Graduate school | 26 (6.6) | 24 (6.1) | 50 (6.3) |
| Household income | |||
| Less than 2 million yen a | 41 (10.4) | 48 (12.2) | 89 (11.3) |
| 2–6 million yen | 202 (51.3) | 176 (44.7) | 378 (48.0) |
| More than 6 million yen | 151 (38.3) | 170 (43.1) | 321 (40.7) |
| Participants with dietary treatments | |||
| 15 (3.8) | 20 (5.1) | 35 (4.4) | |
| Number of ads previously seen | |||
| 0 | 117 (29.7) | ||
| 1 | 82 (20.8) | ||
| 2 | 88 (22.3) | ||
| 3 (all) | 107 (27.2) |
| Intervention (n = 394) | Control (n = 394) | p-Value | Effect Size (d) | |||||
|---|---|---|---|---|---|---|---|---|
| Before | After | Change (After–Before) | Before | After | Change (After–Before) | |||
| FF-CHBs | 2.20 a (0.77) b | 2.36 (0.85) | 0.16 (0.11–0.22) c | 2.22 (0.73) | 2.12 (0.74) | −0.10 (−0.14–−0.06) c | <0.001 d | 0.528 |
| Intention to take functional foods | 2.87 a (1.15) b | 3.08 (1.22) | 0.21 (0.12–0.30) c | 2.94 (1.18) | 3.00 (1.20) | 0.06 (−0.02–0.14) c | 0.018 d | 0.169 |
| Intervention (n = 394) | Control (n = 394) | p-Value | Effect Size (η2) | |
|---|---|---|---|---|
| FF-CHBs | 2.37 a (2.32–2.42) b | 2.11 (2.06–2.16) | <0.001 | 0.026 |
| Intention to take functional foods | 3.11 a (3.03–3.19) b | 2.98 (2.89–3.06) | 0.026 | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iye, R.; Okuhara, T.; Okada, H.; Goto, E.; Furukawa, E.; Kiuchi, T. The Effect of Exposure to “Exemption” Video Advertisements for Functional Foods: A Randomized Control Study in Japan. Healthcare 2022, 10, 345. https://doi.org/10.3390/healthcare10020345
Iye R, Okuhara T, Okada H, Goto E, Furukawa E, Kiuchi T. The Effect of Exposure to “Exemption” Video Advertisements for Functional Foods: A Randomized Control Study in Japan. Healthcare. 2022; 10(2):345. https://doi.org/10.3390/healthcare10020345
Chicago/Turabian StyleIye, Reina, Tsuyoshi Okuhara, Hiroko Okada, Eiko Goto, Emi Furukawa, and Takahiro Kiuchi. 2022. "The Effect of Exposure to “Exemption” Video Advertisements for Functional Foods: A Randomized Control Study in Japan" Healthcare 10, no. 2: 345. https://doi.org/10.3390/healthcare10020345
APA StyleIye, R., Okuhara, T., Okada, H., Goto, E., Furukawa, E., & Kiuchi, T. (2022). The Effect of Exposure to “Exemption” Video Advertisements for Functional Foods: A Randomized Control Study in Japan. Healthcare, 10(2), 345. https://doi.org/10.3390/healthcare10020345