
Safety of Chuna Manipulation Therapy in 289,953 Patients with Musculoskeletal Disorders: A Retrospective Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Data Collection
2.2. Nursing Situation Reports and Routine Vigilance by Medical and Nursing Staff
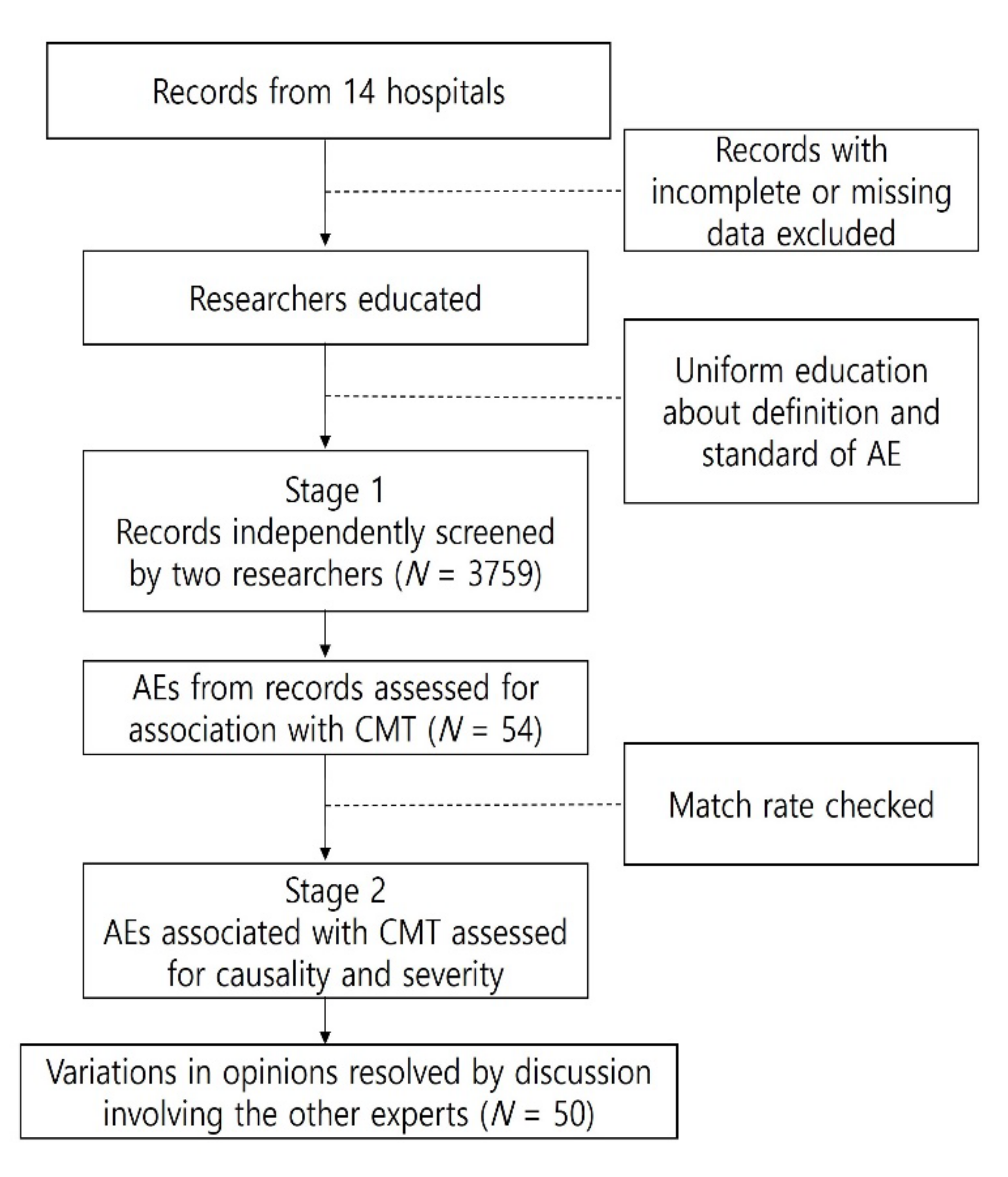
2.3. Screening for AEs
2.4. Analysis of AEs
2.5. Patient and Public Involvement
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Inter-Rater Agreement and Reliability Analysis
3.3. Types and Frequency of AEs
3.3.1. Worsening of Musculoskeletal Pain
3.3.2. Rib Fractures
3.3.3. Falls during Treatment
3.3.4. Vertigo, Chest Pain, and Unpleasant Sensation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Korea Society of Chuna Menual Medicine for Spine & Nerve. Chuna Manual Medicine; Korea Sosciety of Chuna Menual Medicine: Seoul, Korea, 2019; Volume 1. [Google Scholar]
- Kim, M.-Y.; Ha, I.-H.; Lee, J.-H.; Kim, J.-H.; Jung, B. Usage Report of Chuna Manual Therapy in Patients Visiting Korean Medical Institutions -Using Electronic Medical Records(EMR) of 21 Korean Medicine Hospitals and Clinics. J. Korean Med. 2019, 40, 86–98. [Google Scholar] [CrossRef] [Green Version]
- Hurwitz, E.L. Epidemiology: Spinal manipulation utilization. J. Electromyogr. Kinesiol. 2012, 22, 648–654. [Google Scholar] [CrossRef] [PubMed]
- Adams, J.; Peng, W.; Cramer, H.; Sundberg, T.; Moore, C.; Amorin-Woods, L.; Sibbritt, D.; Lauche, R. The Prevalence, Patterns, and Predictors of Chiropractic Use Among US Adults Results From the 2012 National Health Interview Survey. Spine 2017, 42, 1810–1816. [Google Scholar] [CrossRef] [PubMed]
- Chou, R.; Qaseem, A.; Snow, V.; Casey, D.; Cross, J.T., Jr.; Shekelle, P. Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society. Ann. Intern. Med. 2007, 147, 478–491. [Google Scholar] [CrossRef]
- National Institute for Health and Clinical Excellence. Low Back Pain: Early Management of Persistent Non-Specific Low Back Pain; National Institute for Health and Clinical Excellence: London, UK, 2009. [Google Scholar]
- Assendelft, W.J.; Morton, S.C.; Yu, E.I.; Suttorp, M.J.; Shekelle, P.G. Spinal manipulative therapy for low back pain A meta-analysis of effectiveness relative to other therapies. Ann. Intern. Med. 2003, 138, 871–881. [Google Scholar] [CrossRef]
- Verhaeghe, N.; Schepers, J.; Van Dun, P.; Annemans, L. Osteopathic care for spinal complaints: A systematic literature review. PLoS ONE 2018, 13, e0206284. [Google Scholar] [CrossRef] [Green Version]
- Schneider, M.; Haas, M.; Glick, R.; Stevans, J.; Landsittel, D. Comparison of Spinal Manipulation Methods and Usual Medical Care for Acute and Subacute Low Back Pain. Spine 2015, 40, 209–217. [Google Scholar] [CrossRef] [Green Version]
- Swait, G.; Finch, R. What are the risks of manual treatment of the spine? A scoping review for clinicians. Chiropr. Man. Ther. 2017, 25, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Gouveia, L.O.; Castanho, P.; Ferreira, J.J. Safety of Chiropractic Interventions: A systematic review. Spine 2009, 34, E405–E413. [Google Scholar] [CrossRef]
- Wand, B.M.; Heine, P.J.; E O’Connell, N. Should we abandon cervical spine manipulation for mechanical neck pain? Yes. BMJ 2012, 344, e3679. [Google Scholar] [CrossRef] [Green Version]
- National Cancer Institute (NIH). Common Terminology Criteria for Adverse Events (CTCAE) v5.0. Available online: https://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm (accessed on 4 April 2021).
- World Health Organization. The Use of the WHO-UMC System for Standardized Case Causality Assessment; World Health Organization: Uppsala, Sweden, 2013. [Google Scholar]
- Pohlman, K.A.; O’Beirne, M.; Thiel, H.; Cassidy, J.; Mior, S.; Hurwitz, E.L.; Westaway, M.; Ishaque, S.; Yager, J.; Vohra, S. Development and validation of providers’ and patients’ measurement instruments to evaluate adverse events after spinal manipulation therapy. Eur. J. Integr. Med. 2014, 6, 451–466. [Google Scholar] [CrossRef]
- International Council for Harmonisation. Good Clinical Practice; ICH-GCP (E6), GLOSSARY 1.2 Adverse Event (AE). Available online: http://ichgcp.net/1-glossary (accessed on 16 January 2021).
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- European Commission Enterprise; Industry Directorate-General. A Guideline on Summary of Product Characteristics. Available online: http://ec.europa.eu/health/files/eudralex/vol-2/c/smpc_guideline_rev2_en.pdf.2009 (accessed on 4 May 2021).
- Rubinstein, S.M.; De Zoete, A.; Van Middelkoop, M.; Assendelft, W.J.J.; de Boer, M.; van Tulder, M. Benefits and harms of spinal manipulative therapy for the treatment of chronic low back pain: Systematic review and meta-analysis of randomised controlled trials. BMJ 2019, 364, l689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutting, N.; Kerry, R.; Coppieters, M.W.; Scholten-Peeters, G.G. Considerations to improve the safety of cervical spine manual therapy. Musculoskelet. Sci. Pr. 2018, 33, 41–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carnes, D.; Mars, T.S.; Mullinger, B.; Froud, R.; Underwood, M. Adverse events and manual therapy: A systematic review. Man. Ther. 2010, 15, 355–363. [Google Scholar] [CrossRef]
- Rozmovits, L.; Mior, S.; Boon, H. Exploring approaches to patient safety: The case of spinal manipulation therapy. BMC Complement. Altern. Med. 2016, 16, 164. [Google Scholar] [CrossRef] [Green Version]
- Oliphant, D. Safety of Spinal Manipulation in the Treatment of Lumbar Disk Herniations: A Systematic Review and Risk Assessment. J. Manip. Physiol. Ther. 2004, 27, 197–210. [Google Scholar] [CrossRef]
- Kim, K.-T.; Lee, D.-H.; Cho, D.-C.; Sung, J.-K.; Kim, Y.-B. Preoperative Risk Factors for Recurrent Lumbar Disk Herniation in L5–S1. J. Spinal Disord. Tech. 2015, 28, E571–E577. [Google Scholar] [CrossRef]
- Kranenburg, H.; Schmitt, M.; Puentedura, E.; Luijckx, G.; van der Schans, C. Adverse events associated with the use of cervical spine manipulation or mobilization and patient characteristics: A systematic review. Musculoskelet. Sci. Pr. 2017, 28, 32–38. [Google Scholar] [CrossRef]
- Riggs, B.L.; Khosla, S.; Melton, L.J., III. Sex Steroids and the Construction and Conservation of the Adult Skeleton. Endocr. Rev. 2002, 23, 279–302. [Google Scholar] [CrossRef]
- Wuermser, L.-A.; Achenbach, S.J.; Amin, S.; Khosla, S.; Melton, L.J. What Accounts for Rib Fractures in Older Adults? J. Osteoporos. 2011, 2011, 457591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suk, S.-I. Orthopaedics; Choesin-uihagsa: Seoul, Korea, 2013; p. 1699. [Google Scholar]
- Stevinson, C.; Ernst, E. Risks associated with spinal manipulation. Am. J. Med. 2002, 112, 566–571. [Google Scholar] [CrossRef]
- Eric, L.; Hurwitz, D.; Morgenstern, H.; Vassilaki, M.; Chiang, L.-M. Frequency and Clinical Predictors of Adverse Reactions to Chiropractic Care in the UCLA Neck Pain Study. Spine 2005, 30, 1477–1484. [Google Scholar]
- Nielsen, S.M.; Tarp, S.; Christensen, R.; Bliddal, H.; Klokker, L.; Henriksen, M. The risk associated with spinal manipulation: An overview of reviews. Syst. Rev. 2017, 6, 64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karel, Y.H.; Verkerk, K.; Endenburg, S.; Metselaar, S.; Verhagen, A.P. Effect of routine diagnostic imaging for patients with musculoskeletal disorders: A meta-analysis. Eur. J. Intern. Med. 2015, 26, 585–595. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Total | Inpatient * | Outpatient |
|---|---|---|---|
| Patients, n | 289,953 | 47,965 | 241,988 |
| CMT sessions, n | 2,682,258 | 807,103 | 1,875,155 |
| Demographics | |||
| Sex | |||
| Female | 145,955 (50.3) | 24,531 (51.1) | 121,424 (50.2) |
| Male | 143,998 (49.7) | 23,434 (48.9) | 120,564 (49.8) |
| Age, years | |||
| Mean ± SD | 40.6 ± 13.8 | 42.3 ± 14.1 | 40.22 ± 13.74 |
| 0–9 | 825 (0.3) | 70 (0.1) | 755 (0.3) |
| 10–19 | 8829 (3.0) | 885 (1.8) | 7944 (3.3) |
| 20–29 | 55,624 (19.2) | 8968 (18.7) | 46,656 (19.3) |
| 30–39 | 91,350 (31.5) | 13,275 (27.7) | 78,075 (32.3) |
| 40–49 | 56,908 (19.6) | 9389 (19.6) | 47,519 (19.6) |
| 50–59 | 45,164 (15.6) | 9047 (18.9) | 36,117 (14.9) |
| 60–69 | 22,790 (7.9) | 4760 (9.9) | 18,030 (7.5) |
| 70–79 | 7455 (2.6) | 1342 (2.8) | 6113 (2.5) |
| ≥80 | 1008 (0.3) | 229 (0.5) | 779 (0.3) |
| District | |||
| Seoul | 157,686 (54.4) | 14,271 (29.8) | 143,415 (59.3) |
| Gyeonggi-do Province | 68,696 (23.7) | 10,658 (22.2) | 58,038 (24.0) |
| Chungcheong-do Province | 41,722 (14.4) | 13,759 (28.7) | 27,963 (11.6) |
| Gyeongsang-do Province | 11,585 (4.0) | 6486 (13.5) | 5099 (2.1) |
| Jeolla-do Province | 10,264 (3.5) | 2791 (5.8) | 7473 (3.1) |
| Treatment | |||
| Admissions, n | - | 1.1 ± 0.5 | - |
| Duration of admission, days | - | 15.0 ± 19.5 | - |
| Outpatient visits | 7.4 ± 11.4 | 5.3 ± 11.7 † | 7.8 ± 11.3 |
| CMT sessions per patient, n | 9.3 ± 13.5 | 16.8 ± 19.6 | 7.8 ± 11.3 |
| Total (n = 2,184,722) | n (%) | |
|---|---|---|
| S134 | Sprain and strain of cervical spine | 415,270 (19.0) |
| S335 | Sprain and strain of lumbar spine | 393,292 (18.0) |
| M511 | Lumbar and other intervertebral disc disorder with radiculopathy | 260,068 (11.9) |
| M519 | Intervertebral disc disorder, unspecified | 137,949 (6.3) |
| M518 | Other specified intervertebral disc disorder | 112,307 (5.1) |
| M545 | Low back pain | 108,010 (4.9) |
| M501 | Cervical disc disorder with radiculopathy | 80,600 (3.7) |
| M542 | Cervicalgia | 72,236 (3.3) |
| M480 | Spinal stenosis | 68,988 (3.2) |
| M509 | Cervical disc disorder, unspecified | 53,349 (2.4) |
| Inpatient (n = 53,862) † | ||
| S134 | Sprain and strain of cervical spine | 14,468 (26.9) |
| S335 | Sprain and strain of lumbar spine | 12,446 (23.1) |
| M511 | Lumbar and other intervertebral disc disorder with radiculopathy | 7834 (14.5) |
| M501 | Cervical disc disorder with radiculopathy | 2870 (5.3) |
| M518 | Other specified intervertebral disc disorder | 2281 (4.2) |
| M480 | Spinal stenosis | 1663 (3.1) |
| S836 | Sprain and strain of other and unspecified part of knee | 1293 (2.4) |
| M545 | Low back pain | 1169 (2.2) |
| M519 | Intervertebral disc disorder, unspecified | 746 (1.4) |
| M255 | Joint pain | 589 (1.1) |
| Outpatient (n = 2,130,860) ‡ | ||
| S134 | Sprain and strain of cervical spine | 400,802 (18.8) |
| S335 | Sprain and strain of lumbar spine | 380,846 (17.9) |
| M511 | Lumbar and other intervertebral disc disorder with radiculopathy | 252,234 (11.8) |
| M519 | Intervertebral disc disorder, unspecified | 137,203 (6.4) |
| M518 | Other specified intervertebral disc disorder | 110,026 (5.2) |
| M545 | Low back pain | 106,841 (5.0) |
| M501 | Cervical disc disorder with radiculopathy | 77,730 (3.6) |
| M542 | Cervicalgia | 71,788 (3.4) |
| M480 | Spinal stenosis | 67,325 (3.2) |
| M509 | Cervical disc disorder, unspecified | 52,968 (2.5) |
| Case | Total | Severity § | |||||
|---|---|---|---|---|---|---|---|
| n | Incidence 1 * (95% CI) | Incidence 2 † (95% CI) | Frequency | Mild | Moderate | Severe | |
| Classification ‡ | |||||||
| Increased musculoskeletal pain or discomfort | 29 | 0.09 (0.06–0.12) | 1.08 (0.73–1.52) | Very rare | 9 | 19 | 1 |
| Rib fracture | 11 | 0.03 (0.02–0.06) | 0.41 (0.21–0.70) | Very rare | 0 | 11 | 0 |
| Falls | 6 | 0.02 (0.01–0.04) | 0.22 (0.09–0.45) | Very rare | 6 | 0 | 0 |
| Dizziness | 1 | 0.003 (0.000–0.013) | 0.04 (0.00–0.16) | Very rare | 0 | 1 | 0 |
| Chest pain without rib fracture | 2 | 0.01 (0.00–0.02) | 0.07 (0.01–0.23) | Very rare | 1 | 1 | 0 |
| Mild discomfort | 1 | 0.003 (0.000–0.013) | 0.04 (0.00–0.16) | Very rare | 1 | 0 | 0 |
| Total | 50 | 0.15 (0.11–0.19) | 1.86 (1.39–2.43) | Very rare | 17 | 32 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.; Kim, G.-B.; Kim, H.-j.; Park, J.; Lee, J.-W.; Jeong, W.-j.; Kim, H.-G.; Kim, M.-Y.; Park, K.-S.; Lee, J.; et al. Safety of Chuna Manipulation Therapy in 289,953 Patients with Musculoskeletal Disorders: A Retrospective Study. Healthcare 2022, 10, 294. https://doi.org/10.3390/healthcare10020294
Kim S, Kim G-B, Kim H-j, Park J, Lee J-W, Jeong W-j, Kim H-G, Kim M-Y, Park K-S, Lee J, et al. Safety of Chuna Manipulation Therapy in 289,953 Patients with Musculoskeletal Disorders: A Retrospective Study. Healthcare. 2022; 10(2):294. https://doi.org/10.3390/healthcare10020294
Chicago/Turabian StyleKim, Suna, Gook-Beom Kim, Hyo-jun Kim, Joon Park, Ji-Won Lee, Wu-jin Jeong, Hye-Gyeong Kim, Min-Young Kim, Kyoung-Sun Park, Jinho Lee, and et al. 2022. "Safety of Chuna Manipulation Therapy in 289,953 Patients with Musculoskeletal Disorders: A Retrospective Study" Healthcare 10, no. 2: 294. https://doi.org/10.3390/healthcare10020294
APA StyleKim, S., Kim, G.-B., Kim, H.-j., Park, J., Lee, J.-W., Jeong, W.-j., Kim, H.-G., Kim, M.-Y., Park, K.-S., Lee, J., Lee, J.-H., Shin, J.-S., Shin, B.-C., & Ha, I.-H. (2022). Safety of Chuna Manipulation Therapy in 289,953 Patients with Musculoskeletal Disorders: A Retrospective Study. Healthcare, 10(2), 294. https://doi.org/10.3390/healthcare10020294