
Profiles of Burnout, Job Demands and Personal Resources among Emergency Call-Takers and Dispatchers



Abstract
1. Introduction
- Differentiation of burnout profiles in the ECDs group, using four dimensions of burnout from the LBQ questionnaire, and describing the profiles of workers who are at risk of occupational burnout;
- Determining the relationships connecting given profiles with some jobs demands, such as the number of shifts per month and working hours per week, and personal resources, such as the way of assessing the situation, the level of self-efficacy, the level of education and having an active hobby.
- The application of a person-oriented approach provides information allowing for the determination of the risk of occupational burnout in ECDs;
- Burnout profiles can highlight the differences in job demands and employees’ personal resources, which coexist with symptoms of burnout.
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.3. Other Factors and Data Analysis
3. Results
3.1. Group Characteristics according to Applied Variables
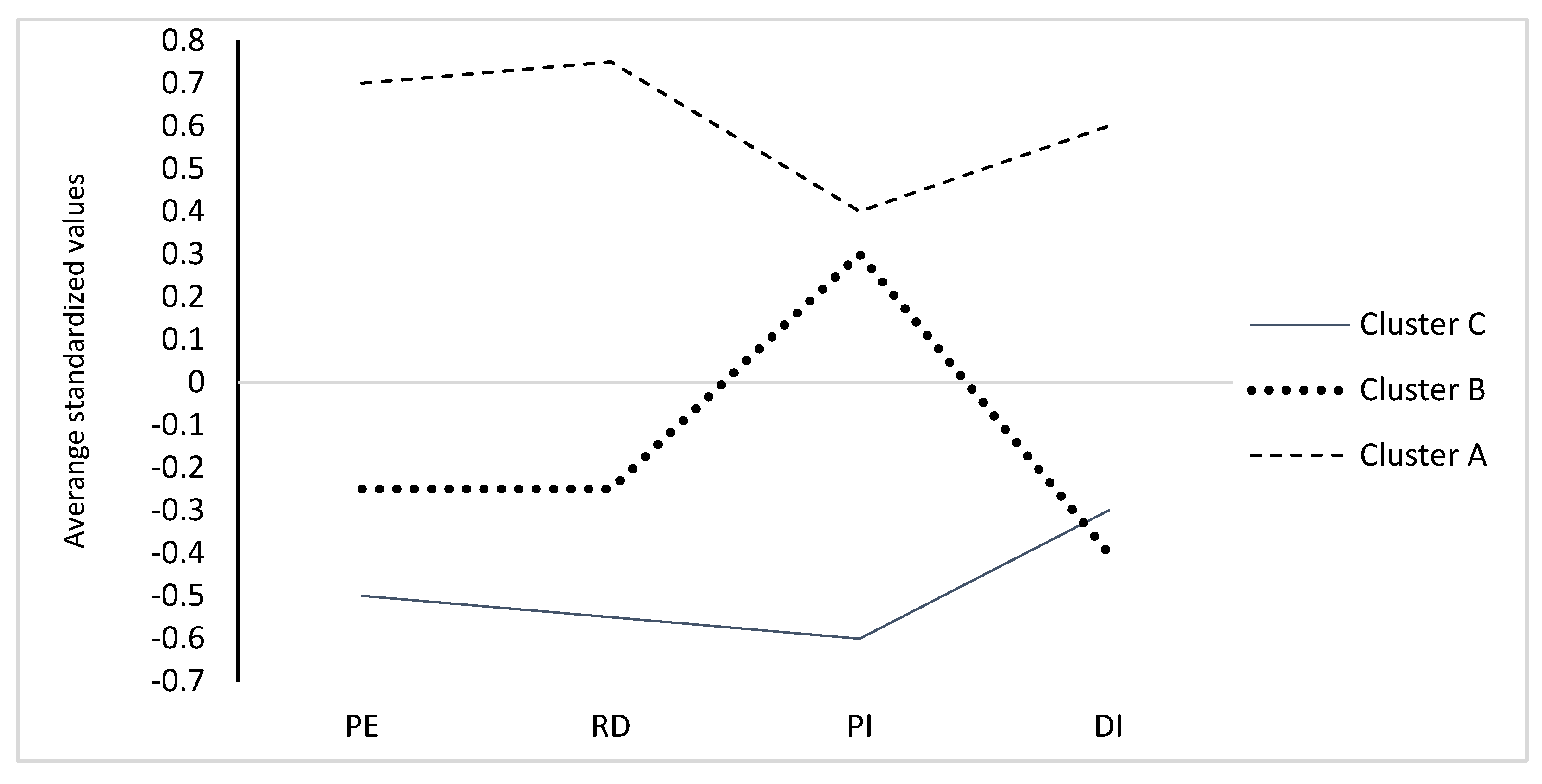
3.2. Profiles of Burnout
3.3. Diversification of Profiles due to Sociodemographic Variables, Working Conditions and Personal Resources
4. Discussion
4.1. Introduction
4.2. Burnout, Perceived Stress and Self-Efficacy among Emergency Call-Takers and Dispatchers
4.3. Profiles of Burnout among Emergency Call-Takers and Dispatchers
4.4. Profiles of Burnout, Organizational Demands and Personal Factors
4.5. Profiles Which Are at Risk of Occupational Burnout
5. Organizational Indications
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Burn-Out an “Occupational Phenomenon”: International Classification of Diseases. Burn-Out an “Occupational Phenomenon”: International Classification of Diseases (who.int). 2019. Available online: https://www.who.int/news/item/28-05-2019-burn-out-an-occupational-phenomenon-international-classification-of-diseases (accessed on 6 October 2021).
- Mäkikangas, A.; Hyvönen, K.; Feldt, T. The energy and identification continua of burnout and work engagement: Developmental profiles over eight years. Burn. Res. 2017, 5, 44–54. [Google Scholar] [CrossRef]
- Golembiewski, R.T. A note on Leitner’s study: Highlighting two models of burnout. Group Organinization Stud. 1986, 14, 5–13. [Google Scholar] [CrossRef]
- Leiter, M.P.; Maslach, C. Latent burnout profiles: A new approach to understanding the burnout experience. Burn. Res. 2016, 3, 89–100. [Google Scholar] [CrossRef]
- Berjot, S.; Altintas, E.; Grebot, E.; Lasage, F.-X. Burnout risk profiles among French psychologist. Burn. Res. 2017, 7, 10–20. [Google Scholar] [CrossRef]
- Mäkikangas, A.; Kinnunen, U. The person-oriented approach to burnout: A systematic review. Burn. Res. 2016, 3, 11–23. [Google Scholar] [CrossRef]
- Bakker, A.; Demerouti, E. Job demands-resources theory: Taking stock and looking forward. J. Occup. Health Psychol. 2017, 22, 273–285. [Google Scholar] [CrossRef] [PubMed]
- Xanthopoulou, D.; Bakker, A.B.; Dollard, M.F.; Demerouti, E.; Schaufeli, W.B.; Taris, T.W.; Schreurs, P.J.G. When do job demands particularly predict burnout? The moderating role of job resources. J. Manag. Psychol. 2007, 22, 766–785. [Google Scholar] [CrossRef]
- Xanthopoulou, D.; Bakker, A.B.; Demerouti, E.; Schaufeli, W.B. The role of personal resources in the job demands-resources model. Int. J. Stress Manag. 2007, 14, 121–141. [Google Scholar] [CrossRef]
- Folkman, S. Stress, Health, and Coping: An Overview. In The Oxford Handbook of Stress, Health, and Coping; Folkman, S., Ed.; Oxford University Press: Oxford, MS, USA, 2011; pp. 3–11. [Google Scholar]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Shakespeare-Finch, J.; Rees, A.; Armstrong, D. Social support, self-efficacy, trauma, and well-being in emergency medical dispatchers. Soc. Indic. Res. 2015, 123, 549–565. [Google Scholar] [CrossRef]
- Bandura, A. Social cognitive theory goes global. Psychologist 2009, 22, 504–506. [Google Scholar]
- Wood, R.E.; Locke, E.A. The relation of self-efficacy and grade goals to academic performance. Educ. Psychol. Meas. 1987, 47, 1013–1024. [Google Scholar] [CrossRef]
- Bandura, A. Cultivate self-efficacy for personal and organizational effectiveness. In Handbook of Principles of Organizational Behavior, 2nd ed.; Locke, E.A., Ed.; John Wiley & Sons, Ltd.: Chichester, UK, 2009; pp. 179–200. [Google Scholar]
- Shoji, K.; Cieslak, R.; Smoktunowicz, E.; Rogala, A.; Benight, C.C.; Luszczynska, A. Associations between job burnout and selfefficacy: A meta-analysis. Anxiety Stress Coping 2015, 29, 367–386. [Google Scholar] [CrossRef] [PubMed]
- Xanthopoulou, D.; Bakker, A.B.; Fischbach, A. Work engagement among employees facing emotional demands: The role of personal resources. J. Pers. Psychol. 2013, 12, 74–84. [Google Scholar] [CrossRef]
- Weibel, L.; Gabrion, I.; Aussedat, M.; Kreutz, G. Work-related stress in an emergency medical dispatch center. Ann. Emerg. Med. 2003, 41, 500–506. [Google Scholar] [CrossRef]
- Adams, K.; Shakespeare-Finch, J.; Armstrong, D. An interpretative phenomenological analysis of stress and well-being in emergency medical dispatchers. J. Loss Trauma 2015, 20, 430–448. [Google Scholar] [CrossRef]
- Bedini, S.; Braun, F.; Weibel, L.; Aussedat, M.; Pereira, B.; Dutheil, F. Stress and salivary cortisol in emergency medical dispatchers: A randomized shifts control trial. PLoS ONE 2017, 12, e0177094. [Google Scholar] [CrossRef]
- Sprigg, C.A.; Armitage, C.J.; Hollis, K. Verbal abuse in the National Health Service: Impressions of the prevalence, perceived reasons for and relationships with staff psychological well-being. Emerg. Med. J. 2007, 24, 281–282. [Google Scholar] [CrossRef][Green Version]
- Smith, E.; Holmes, L.; Burkle, F. Exploring the physical and mental health challenges associated with emergency service call-taking and dispatching: A review of the literature. PDM 2019, 34, 1–6. [Google Scholar] [CrossRef]
- Golding, S.; Horsfield, C.; Annette, D.; Egan, B.; Jones, M.; Raleigh, M.; Schofield, P.; Sguires, A.; Start, K.; Quinn, T.; et al. Exploring the psychological health of emergency dispatch centre operatives: A systematic review and narrative synthesis. PeerJ 2017, 5, 1–29.e3735. [Google Scholar] [CrossRef]
- Amoafo, E.; Hanbali, N.; Patel, A.; Singh, P. What are the significant factors associated with burnout in doctors? Occup. Med. 2015, 65, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Makara-Studzińska, M.; Wajda, Z.; Lizińczyk, S. Years of service, self-efficacy, stress and burnout among polish firefighters. Int. J. Environ. 2020, 33, 283–297. [Google Scholar] [CrossRef] [PubMed]
- Lin, R.T.; Lin, Y.T.; Hsia, Y.F.; Kuo, C.C. Long working hours and burnout in health care workers: Non-linear dose-response relationship and the effect mediated by sleeping hours-A cross-sectional study. J. Occup. Health 2021, 63, e12228. [Google Scholar] [CrossRef] [PubMed]
- Meischke, H.; Painter, I.; Lilly, M.; Beaton, R.; Revere, D.; Calhoun, R.; Seeley, K.D.; Carslay, Y.; Moe, C.; Baseman, J. An exploration of sources, symptoms and buffers of occupational stress in 9-1-1 emergency call centers. Ann. Emerg. Dispatch Response 2015, 3, 28–35. [Google Scholar]
- Soderstrom, M.; Jeding, K.; Ekstedt, M.; Perski, A.; Akerstedt, T. Insufficient sleep predicts clinical burnout. J. Occup. Health Psychol. 2012, 17, 175–183. [Google Scholar] [CrossRef]
- Byron, K. A meta-analytic review of work-family conflict and its antecedents. J. Vocat. Behav. 2005, 67, 169–198. [Google Scholar] [CrossRef]
- Marchand, A.; Blanc, M.; Beauregard, N. Do age and gender contribute to workers’ burnout symptoms? J. Occup. Med. 2018, 66, 405–411. [Google Scholar] [CrossRef]
- Jaworowska, A. Massimo Santinello Link Burnout Questionnaire. Polska Normalizacja; Laboratory of Psychological Tests of the Polish Psychological Society: Warszawa, Poland, 2014. [Google Scholar]
- Besse, C.S.; Bonsack, C.; Gilles, I.; Golay, P. Work-related burnout among personnel at a university hospital: Identifying quantitative and qualitative differences using latent class analysis. J. Ment. Health 2021, 30, 388–399. [Google Scholar] [CrossRef]
- McAleavy, T.; Choi, B.; Arlikatti, S. Faceless heroes: A content analysis of determinants for the recruitment, career development & retention of Emergency Medical Dispatchers in the United States of America. Int. J. Disast. Risk. Reduct. 2021, 61, 1–8. [Google Scholar] [CrossRef]
- Makara-Studzińska, M.; Załuski, M.; Adamczyk, K. Burnout and perceived stress of Polish emergency call takers and dispatchers. Int. J. Environ. 2021, 18, 10206. [Google Scholar] [CrossRef]
- Makara-Studzińska, M.; Załuski, M.; Adamczyk, K. Polish Emergency Dispatchers during a COVID-19 pandemic—Burnout syndrome, perceived stress, and self-efficacy. Effects of multidimensional path analysis. Front. Psychol. 2021, 12, 729772. [Google Scholar] [CrossRef] [PubMed]
- Juczyński, Z.; Ogińska-Bulik, N. Skala Odczuwanego Stresu—PSS-10. In Narzędzia Pomiaru Stresu i Radzenia Sobie ze Stresem; Laboratory of Psychological Tests of the Polish Psychological Society: Warszawa, Poland, 2009; pp. 11–22. [Google Scholar]
- Juczyński, Z. Skala uogólnionej własnej skuteczności—GSES. In Narzędzia Pomiaru w Promocji i Psychologii Zdrowia; Juczyński, Z., Ed.; Laboratory of Psychological Tests of the Polish Psychological Society: Warszawa, Poland, 2001; pp. 89–94. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.R-project.org/ (accessed on 6 May 2021).
- Weller, B.E.; Bowen, N.K.; Faubert, S.J. Latent class analysis: A guide to best practice. J. Black Psychol. 2020, 46, 287–311. [Google Scholar] [CrossRef]
- Everitt, B.S.; Landau, S.; Leese, M. Cluster Analysis, 4th ed.; Arnold: London, UK, 2001; pp. 62–64. [Google Scholar]
- James., G.; Witten, D.; Hastie, T.; Tibshirani, R. An Introduction to Statistical Learning. With Application in R; Springer: New York, NY, USA, 2013; pp. 386–390. [Google Scholar]
- Kaufman, L.; Rousseeuw, P.J. Clustering by means of Medoids. In Statistical Data Analysis Based in the L1–Norm and Related Methods; Dodge, Y., Ed.; Elsevier: Amsterdam, The Netherlands, 1987; pp. 405–416. [Google Scholar]
- Pihur, V.; Datta, S.; Datta, S. Weighted rank aggregation of cluster validation measures: A Monte Carlo ross-entropy approach. Bioinformatics 2007, 23, 1607–1615. [Google Scholar] [CrossRef] [PubMed]
- Hilaire Schneider, C.; Saint-Cast, A.; Michelland, L.; de Stefano, C.; Radou, L.; Chouied, T.; Savary, D.; Gueye, P.; Jehel, L.; Lapostolle, F. Répercussions psychologiques de la prise en charge des appels d’urgence sur les assistants de régulation médicale (ARM) d’un SAMU–Centre 15 [Psychological effects of emergency calls management on medical dispatcher assistants in a SAMU-Center 15]. Encephale 2021, 47, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Boland, L.L.; Kinzy, T.G.; Myers, R.N.; Fernstrom, K.M.; Kamrud, J.W.; Mink, P.J.; Stevens, A.C. Burnout and exposure to critical incidents in a cohort of emergency medical services workers from Minnesota. West J. Emerg. Med. 2018, 19, 987–995. [Google Scholar] [CrossRef]
- Lesage, F.-X.; Berjot, S.; Deschamps, F. Psychometric properties of the French versions of the perceived stress scale. Int. J. Occup. Med. Environ. Health 2012, 25, 178–184. [Google Scholar] [CrossRef]
- Turner, A.D.; James, B.D.; Capuano, A.W.; Aggarwal, N.T.; Barnes, L.L. Perceived stress and cognitive decline in different cognitive domains in a cohort of older African Americans. Am. J. Geriatr. Psychiatry 2017, 25, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Makara-Studzińska, M.; Załuski, M.; Jagielski, P.; Wójcik-Małek, D.; Szelepajło, M. An exploration of perceived stress, burnout syndrome, and self-efficacy in a group of Polish air traffic controllers and maritime navigators: Similarities and differences. Int. J. Environ. 2021, 18, 53. [Google Scholar] [CrossRef] [PubMed]
- Bakker, A.B.; Demerouti, E.; De Boer, E.; Schaufeli, W. Job demands and job resources as predictors of absence duration and frequency. J. Vocat. Behav. 2003, 62, 341–356. [Google Scholar] [CrossRef]
- Ayala, E.; Carnero, A.M. Determinants of burnout in acute and critical care military nursing personnel: A cross-sectional study from Peru. PLoS ONE 2013, 8, e54408. [Google Scholar] [CrossRef]
- Maslach, C.; Leitner, M.P. Understanding the burnout experience: Recent research and its implications for psychiatry. World Psychiatry 2016, 15, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Ribas, V.R.; de Almeida, C.Â.V.; Martins, H.A.L.; Alves, C.F.D.O.; Alves, M.J.P.C.; Carneiro, S.M.D.O.; Ribas, V.R.; de Vasconcelos, C.A.C.; Sougey, E.B.; de Castro, R.M. Brazilian air traffic controllers exhibit excessive sleepiness. Dement. Neuropsychol. 2011, 5, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Roberti, J.W.; Harrington, L.N.; Storch, E.A. Further psychometric support for the 10-item version of the perceived stress scale. JCC 2006, 9, 135–147. [Google Scholar] [CrossRef]
- Bakker, A.; Costa, P. Chronic job burnout and daily functioning: A theoretical analysis. Burn. Res. 2014, 1, 112–119. [Google Scholar] [CrossRef]
- Hakanen, J.; Demerouti, E.; Xanthopoulou, D. Job resources boost work engagement, particularly when job demands are high. J. Educ. Psychol. 2007, 99, 274. [Google Scholar] [CrossRef]
- Prati, G.; Pietrantoni, L.; Cicognani, E. Self-efficacy moderates the relationship between stress appraisal and quality of life among rescue workers. Anxiety Stress Coping 2010, 23, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Grau, R.; Salanova, M.; Peiró, J.M. Efectos moduladores de la autoeficacia en el estrés laboral [Modulating effects of self-efficacy in job stress]. Apunt. Psicol. 2012, 30, 311–321. [Google Scholar]
- Ventura, M.; Llorens Gumbau, S.; Salanova, M. Professional self-efficacy as a predictor of burnout and engagement: The role of challenge and hindrance demands. JPIA 2014, 149, 277–302. [Google Scholar] [CrossRef]
- Lorente, L.; Salanova, M.; Martínez, I.M.; Vera, M. How personal resources predict work engagement and self-rated performance among construction workers: A social cognitive perspective. Int. J. Psychol. 2014, 49, 200–207. [Google Scholar] [CrossRef]
- Van Wingerden, J.; Derks, D. Fostering employee well-being via a job crafting intervention. J. Vocat. Behav. 2017, 100, 164–174. [Google Scholar] [CrossRef]
- Schwarzer, R.; Hallum, S. Perceived teacher self-efficacy as a predictor of job stress and burnout: Mediation analyses. Appl. Psychol. 2008, 57, 152–171. [Google Scholar] [CrossRef]
- Konopaske, R.; Ivancevich, J.M.; Matteson, M.T. Organizational Behavior and Management, 11th ed.; McGraw-Hill Education: New York, NY, USA, 2017. [Google Scholar]
- Hamid, N. The relationship between socio-demographic variables, job stressors and hardiness among nurses in Iran. Afr. J. Nurs. Midwifery 2007, 9, 49–63. [Google Scholar]
- Martinussen, M.; Richardsen, A.M. Air traffic controller burnout: Survey responses regarding job demands, job resources, and health. Aviat. Space Environ. Med. 2006, 77, 422–428. [Google Scholar] [PubMed]
- Anczewska, M.; Świtaj, P.; Roszczyńska, J. Wypalenie zawodowe. Adv. Psychiatry Neurol. 2005, 14, 67. [Google Scholar]
- Maslach, C.; Schaufeli, W.; Leitner, M. Job Burn. Annu. Rev. Psychol. 2001, 52, 397–422. [Google Scholar] [CrossRef] [PubMed]
- Brody, L.R.; Hall, J.A. Płeć, emocje i ekspresja. In Psychologia Emocji, 1st ed.; Lewis, M.M., Haviland-Jones, J., Eds.; GWP: Gdańsk, Poland, 2005; pp. 431–445. [Google Scholar]
- Nolen-Hoeksema, S. Sex differences in unipolar depression: Evidence and theory. Psychol. Bull. 1987, 101, 259–282. [Google Scholar] [CrossRef]
- Farber, B. Treatment strategies for different types of teacher burnout. Psychother. Pract. 2000, 56, 675–689. [Google Scholar] [CrossRef]
- Salvagioni, D.A.J.; Melanda, F.N.; Mesas, A.E.; González, A.D.; Gabani, F.L.; Andrade, S.M. Physical, psychological and occupational consequences of job burnout: A systematic review of prospective studies. PLoS ONE 2017, 12, e0185781. [Google Scholar] [CrossRef]
- Bakusic, J.; Schaufeli, W.; Claes, S.; Godderis, L. Stress, burnout and depression: A systematic review on DNA methylation mechanisms. J. Psychosom. Res. 2017, 92, 34–44. [Google Scholar] [CrossRef]


{kind=link}
| Parameter | M ± SD |
|---|---|
| Age | 34.43 ± 8.11 |
| Sex (women) % | 56.4 |
| Years of service | 4.46 ± 2.64 |
| Number of shifts per month | 14.60 ± 6.83 |
| Number of working hours per week | 43.33 ± 6.37 |
| PE | 20.86 ± 3.91 |
| RD | 20.09 ± 4.24 |
| PI | 22.95 ± 3.22 |
| DI | 18.48 ± 3.45 |
| PSS-10 | 15.92 ± 6.73 |
| GSES | 30.96 ± 4.90 |
| Parameter | Cluster | ||||||
|---|---|---|---|---|---|---|---|
| A (n = 189) | B (n = 182) | C (n = 182) | Kruskal–Wallis H Test | Dunn–Bonferroni Test | p | ||
| PE | M ± SD | 23.78 ± 2.98 | 19.88 ± 3.05 | 18.84 ± 3.77 | 178.79 | A > B > C | p < 0.015 |
| RD | M ± SD | 23.36 ± 3.35 | 19.04 ± 3.21 | 17.76 ± 3.9 | 186.46 | A > B > C | p < 0.015 |
| PI | M ± SD | 24.12 ±2.81 | 23.77 ± 2.87 | 20.94 ± 3.03 | 126.34 | A > B > C | p < 0.015 |
| DI | M ± SD | 20.6. 3 ± 2.86 | 17.17 ± 2.77 | 17.58 ± 3.5 | 205.70 | A > C > B | p < 0.015 |
| LBQINDEX | M ± SD | 91.883 ± 5.80 | 79.857 ± 5.96 | 75.120 ± 9.49 | 340.901 | A > B > C | p < 0.015 |
| Parameter | Cluster | p | |||||
|---|---|---|---|---|---|---|---|
| A | B | C | Kruskal–Wallis H Test | Dunn–Bonferroni Test | |||
| Years of service as ECD | M ± SD | 3.19 ± 2.4 | 5.66 ± 2.48 | 4.2 ± 2.58 | 73.51 | B > C > A | p < 0.015 |
| Age | M ± SD | 34.021 ± 8.75 | 34.937 ± 7.44 | 34.021 ± 8.75 | 3.095 | n.s. | |
| Sex % | Men | 40.21 | 35.16 | 55.49 | 16.59 | C > A > B | p < 0.015 |
| Women | 59.79 | 64.84 | 44.51 | B > A > C | |||
| Number of shifts per month | M ± SD | 14.27± 2.37 | 14.42 ± 1.88 | 14 ± 1.85 | 0.783 | n.s. | |
| Number of working hours per week | M ± SD | 42.27± 6.52 | 45.08± 5.81 | 42.49± 6.43 | 36.37 | B > C > A | p < 0.015 |
| PSS-10 | M ± SD | 15.6 ± 5.86 | 21.42 ± 4.92 | 10.76 ± 4.61 | 237.63 | B > A > C | p < 0.015 |
| Education % | Vocational | 0.53 | 0.00 | 0.00 | 5.99 | p = 0.7358 | |
| Secondary | 31.75 | 23.63 | 21.98 | A > B > C | |||
| Higher | 67.20 | 75.27 | 77.47 | C > B > A | |||
| No information | 0.53 | 1.10 | 0.55 | ||||
| Trained profession or only ECD profession | % | 30 | 34.8 | 32,4 | p = n.s. | ||
| GSES | M ± SD | 31.35 ± 4.66 | 28.54 ± 5.34 | 32.98 ± 3.47 | 89.56 | C > A > B | p < 0.015 |
| Hobby, yes | % | 93.6 | 84.92 | 95.1 | 18.28 | C > A > B | p < 0.015 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Załuski, M.; Makara-Studzińska, M. Profiles of Burnout, Job Demands and Personal Resources among Emergency Call-Takers and Dispatchers. Healthcare 2022, 10, 281. https://doi.org/10.3390/healthcare10020281
Załuski M, Makara-Studzińska M. Profiles of Burnout, Job Demands and Personal Resources among Emergency Call-Takers and Dispatchers. Healthcare. 2022; 10(2):281. https://doi.org/10.3390/healthcare10020281
Chicago/Turabian StyleZałuski, Maciej, and Marta Makara-Studzińska. 2022. "Profiles of Burnout, Job Demands and Personal Resources among Emergency Call-Takers and Dispatchers" Healthcare 10, no. 2: 281. https://doi.org/10.3390/healthcare10020281
APA StyleZałuski, M., & Makara-Studzińska, M. (2022). Profiles of Burnout, Job Demands and Personal Resources among Emergency Call-Takers and Dispatchers. Healthcare, 10(2), 281. https://doi.org/10.3390/healthcare10020281