
Impact of Actual Use Behavior of Healthcare Wearable Devices on Quality of Life: A Cross-Sectional Survey of People with Dementia and Their Caregivers in Ghana

 , , ,
, , ,  and
and
Abstract
1. Introduction
- (i).
- Assess the impact of the actual use of healthcare wearable devices on the quality of life (QoL) of PWDs, using the extended UTAUT model and SF-36 quality of life instruments.
- (ii).
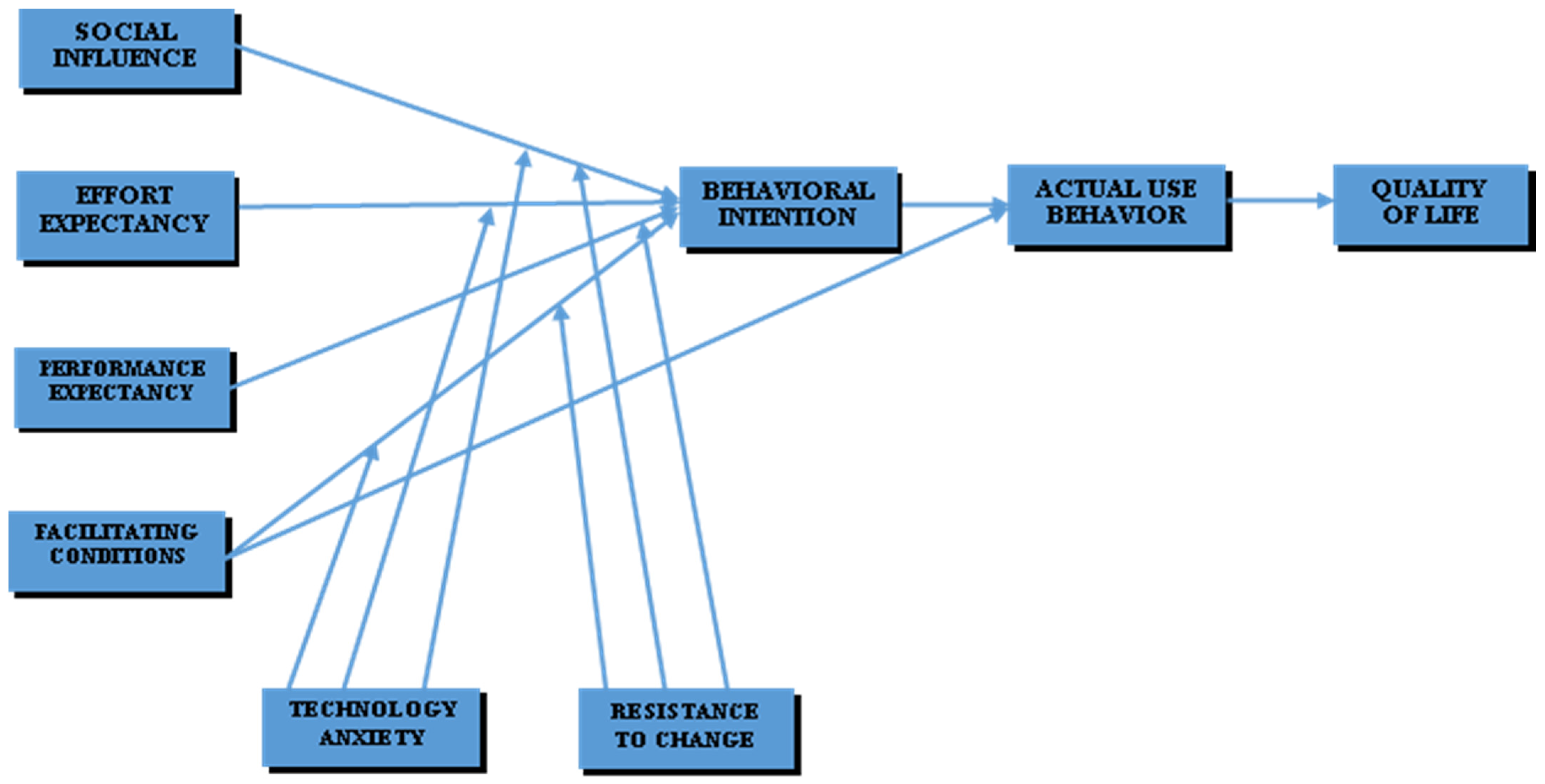
- Provide an overview of the determinants of actual use behaviors among PWDs by assessing the influence of factors, such as behavioral intention, effort expectancy, social influence, facilitating conditions, resistance to change, and technology anxiety, on the actual use behavior of healthcare wearable devices among PWDs.
2. Theoretical Basis and Conceptual Framework
2.1. Extended UTAUT Model
2.1.1. Performance Expectancy (PE)
2.1.2. Effort Expectancy (EE)
2.1.3. Social Influence (SI)
2.1.4. Facilitating Conditions (FC)
2.1.5. Behavioral Intention (BI)
2.1.6. Technology Anxiety (TA) and Resistance to Change (RC)
2.1.7. SF-36
2.1.8. Moderating Effect
2.1.9. Conceptual Framework
3. Methodology
3.1. Research and Questionnaire Design, and Data Collection
3.2. 36-Item Short-Form Survey (SF-36) Coding and Scoring
3.3. Quality Control Measures and Handling Biases
3.4. Data Analysis
4. Results
4.1. Descriptive Statistics
4.2. Evaluation of Measurement Model
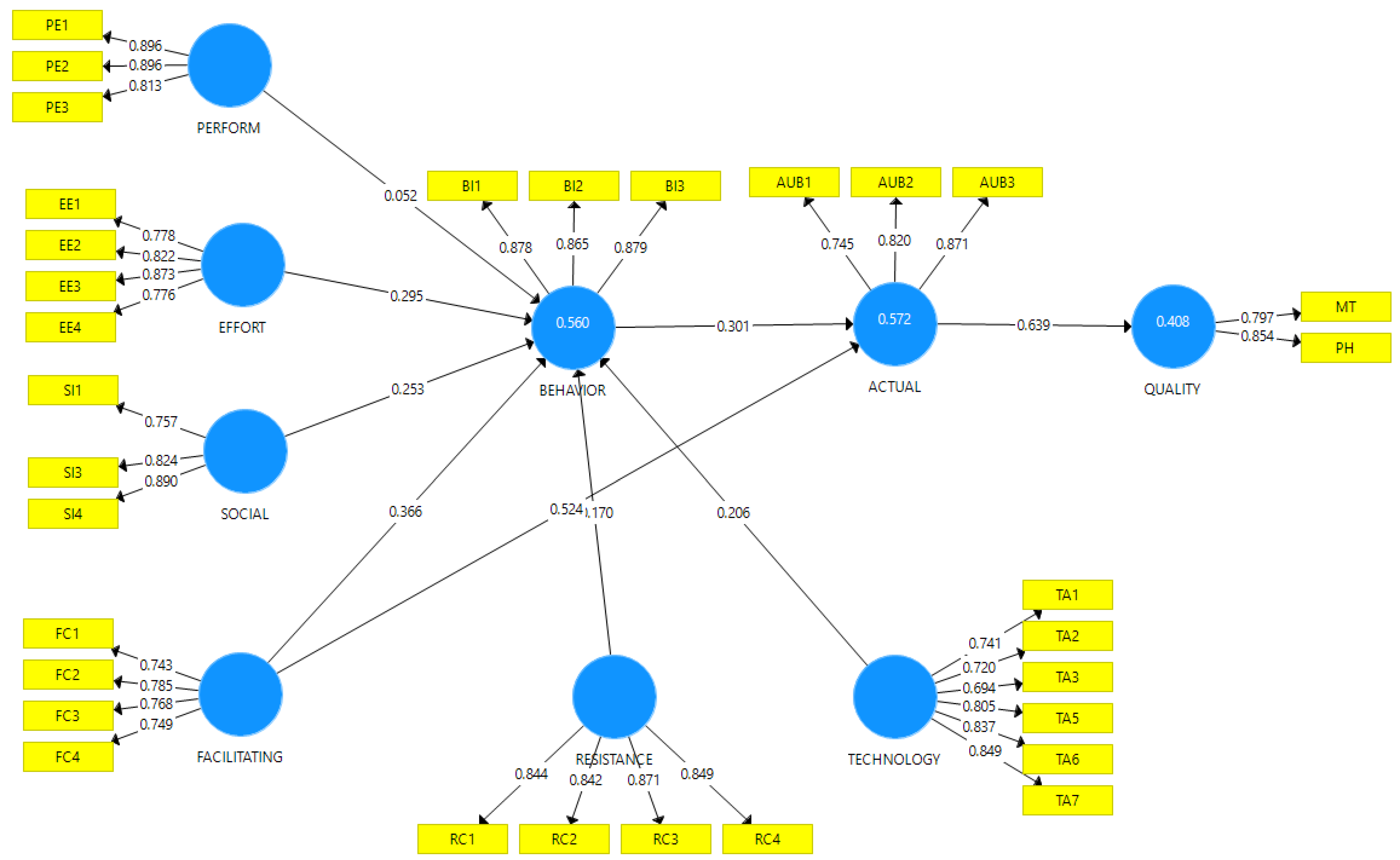
4.3. Evaluation of Structural Model
Hypotheses Testing
4.4. Evaluating the Mediating Role of BI on FC and AUB
4.5. Evaluating Moderatiing Effects of TA and RC on BI
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Constructs | Items | Descriptions | Literature Sources |
|---|---|---|---|
| Behavioral Intention | BI1 | I/patient intend(s) to use healthcare wearable devices in the near future | [2,101,102] |
| BI2 | I/patient intend(s) intend to use healthcare wearable devices at every opportunity in the future | ||
| BI3 | I/patient plan(s) to increase his/her/my use of healthcare wearable devices in the future | ||
| Effort Expectancy | EE1 | Learning how to use healthcare wearable devices will be easy for me/patient | [2,13,103] |
| EE2 | I/patient find(s) healthcare wearable devices easy to use | ||
| EE3 | It is easy for me/patient to become skillful at using healthcare wearable devices | ||
| EE4 | My/patient’s interaction with healthcare wearable devices is clear and understandable | ||
| Facilitating Conditions | FC1 | I/patient have/has the necessary resources to use healthcare wearable devices | [2,103] |
| FC2 | I/patient have/has the knowledge necessary to use healthcare wearable devices | ||
| FC3 | I/patient know my/his/her medical practitioners have the necessary knowledge to help me/him/her use healthcare wearable devices | ||
| FC4 | Healthcare wearable devices are compatible with other technologies the I/patient use(s) | ||
| Performance Expectancy | PE1 | I/patient find(s) the healthcare wearable device useful in my/his/her live | [2,13,39,104] |
| PE2 | Using healthcare wearable device will help me/patient accomplish things more quickly | ||
| PE3 | Using healthcare wearable device will improve my/patient’s quality of daily healthcare | ||
| Resistance to Change | RC1 | I/patient don’t want healthcare wearable devices to interfere with the way I/he/she deal(s) with relevant health problems | [2,13,48,103] |
| RC2 | I/patient don’t/doesn’t want healthcare wearable devices to change the way I/she/he lived my/his/her life before | ||
| RC3 | I/patient don’t/doesn’t want healthcare wearable devices to change the way I/he/she interact (s) with other people | ||
| RC4 | I/patient don’t/doesn’t want healthcare wearable devices to change the way my/his/her medical practitioners handle(s) my/his/her health issues | ||
| Social Influence | SI1 | People who are important to me/patient think that I/he/she should use healthcare wearable devices | [13,103,104] |
| SI2 | People who influence me/patient think I/she/he should use healthcare wearable devices | ||
| SI3 | People whose opinions are valuable to me/patient would prefer that I/he/she use(s) healthcare wearable devices | ||
| SI4 | Medical Practitioners think using healthcare wearable devices will enhance my/patient’s quality of life | ||
| Technology Anxiety | TA1 | Wearing healthcare wearable devices would make me/patient nervous | [2,12] |
| TA2 | Using healthcare wearable devices make me/patient worried | ||
| TA3 | Using healthcare wearable devices may make me/patient to be confuse | ||
| TA4 | Using healthcare wearable devices make me/patient feel uncomfortable | ||
| TA5 | Using healthcare wearable devices may cause me/patient to perceive increase in the chances of me/him/her losing my/his/her cognitive abilities completely | ||
| TA6 | Using healthcare wearable devices make me/patient feel less human | ||
| TA7 | Using healthcare wearable devices make me/patient feel unsafe due to security issues such as hacking | ||
| Actual Use Behavior | UB1 | Using healthcare wearable devices seem to be a pleasant experience for me/patient | [2,105] |
| UB2 | I/patient use(s) healthcare wearable devices currently | ||
| UB3 | I/patient intend(s) to spend time on the use of healthcare wearable devices |
| Physical Functioning | Yes, Limited a Lot | Yes, Limited a Little | Not Limited at All | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| f | % | f | % | f | % | ||||||||||
| Healthcare wearable devices limit (patient/me) in doing vigorous activities | 11 | 3.4 | 43 | 13.4 | 266 | 83.1 | |||||||||
| Healthcare wearable devices limit (patient/me) in doing moderate activities. | 97 | 30.3 | 223 | 69.7 | |||||||||||
| Healthcare wearable devices limit (patient/me) in lifting or carrying groceries | 77 | 24.1 | 243 | 75.9 | |||||||||||
| Healthcare wearable devices limit (patient/me) in climbing several flights of stairs | 1 | 0.3 | 60 | 18.8 | 259 | 80.9 | |||||||||
| Healthcare wearable devices limit (patient/me) in climbing one flight of stairs | 2 | 0.6 | 82 | 25.6 | 236 | 73.8 | |||||||||
| Healthcare wearable devices limit (patient/me) in bending, kneeling, or stooping | 1 | 0.3 | 54 | 16.9 | 265 | 82.8 | |||||||||
| Healthcare wearable devices limit (patient/me) in walking more than a mile | 4 | 1.3 | 67 | 20.9 | 249 | 77.8 | |||||||||
| Healthcare wearable devices limit (patient/me) in walking several hundred yards | 62 | 19.4 | 258 | 80.6 | |||||||||||
| Healthcare wearable devices limit (patient/me) in walking one hundred yards | 1 | 0.3 | 62 | 19.4 | 257 | 80.3 | |||||||||
| Healthcare wearable devices limit (patient/me) in bathing or dressing him/herself | 4 | 1.3 | 72 | 22.5 | 244 | 76.3 | |||||||||
| Role-Physical | Yes | No | |||||||||||||
| f | % | f | % | ||||||||||||
| Healthcare wearable devices help (patient/me) in cutting down the amount of time (patient/I) spent on work or other activities | 61 | 19.1 | 259 | 80.9 | |||||||||||
| Healthcare wearable devices make (patient/me) accomplish less than (patient/I) would like | 47 | 14.7 | 273 | 85.3 | |||||||||||
| Healthcare wearable devices make (patient/me) limited in his/her/my kind of work or other activities | 62 | 19.4 | 258 | 80.6 | |||||||||||
| Healthcare wearable devices make (patient/me) have difficulties performing work or other activities (e.g., it took extra effort) | 45 | 14.1 | 275 | 85.9 | |||||||||||
| Bodily Pain | None | Very mild | Mild | ||||||||||||
| f | % | f | % | f | % | ||||||||||
| How much bodily pain have you (patient) had during the past 4 weeks while using healthcare wearable devices? | 194 | 60.6 | 97 | 30.3 | 29 | 9.1 | |||||||||
| Not at all | Not at all | A little bit | |||||||||||||
| f | % | f | % | f | % | ||||||||||
| During the past 4 weeks, how much did pain interfere with your normal work since using healthcare wearable devices? | 284 | 88.8 | 20 | 6.3 | 16 | 5.0 | |||||||||
| General Health | Definitely True | Mostly True | Don’t Know | Mostly False | Definitely False | ||||||||||
| f | % | f | % | f | % | f | % | f | % | ||||||
| With healthcare wearable devices, it seem (patient/I) get sick a little easier than other people | 12 | 3.8 | 14 | 4.4 | 268 | 83.8 | 26 | 8.1 | |||||||
| With healthcare wearable devices, (patient/I) am(is) as healthy as anybody (patient/I) know | 201 | 62.8 | 70 | 21.9 | 49 | 15.3 | |||||||||
| With Healthcare wearable devices, (patient/I) expect(s) (patient’s/my) health to get worse | 11 | 3.4 | 45 | 14.1 | 19 | 5.9 | 238 | 74.4 | 7 | 2.2 | |||||
| With Healthcare wearable devices (patient’s/my) health is excellent | 268 | 83.8 | 8 | 2.5 | 44 | 13.8 | |||||||||
| Excellent | Very Good | Good | Fair | Poor | |||||||||||
| f | % | f | % | f | % | f | % | f | % | ||||||
| With the help of healthcare wearable devices, (patient/I) will say (his/her/my) health is: | 125 | 39.1 | 167 | 52.2 | 24 | 7.5 | 4 | 1.3 | |||||||
| Vitality | All of the time | None of the time | |||||||||||||
| f | % | f | % | ||||||||||||
| With healthcare wearable devices, (patient’s/I) feel full of life | 259 | 80.9 | 61 | 19.1 | |||||||||||
| With healthcare wearable devices, (patient’s/I) have a lot of energy | 273 | 85.3 | 47 | 14.7 | |||||||||||
| With healthcare wearable devices, (patient’s/I) feel worn out | 62 | 19.4 | 258 | 80.6 | |||||||||||
| With healthcare wearable devices, (patient’s/I) feel tired | 45 | 14.1 | 275 | 85.9 | |||||||||||
| Role-Emotional | Yes | No | |||||||||||||
| f | % | f | % | ||||||||||||
| Using healthcare wearable devices has made me (patient) cut down the amount of time spent on work or other activities | 293 | 91.6 | 27 | 8.4 | |||||||||||
| Using healthcare wearable devices has made (patient/me) accomplished less than (patient/I) would have liked | 26 | 8.1 | 294 | 91.9 | |||||||||||
| Using healthcare wearable devices made (patient/me) do work or other activities less carefully than usual | 29 | 9.1 | 291 | 90.9 | |||||||||||
| Mental Health | All of the time | Some of the time | A little of the time | None of the time | |||||||||||
| f | % | f | % | f | % | f | % | ||||||||
| Using healthcare wearable devices has made (patient/me) to be a very nervous person | 4 | 1.3 | 22 | 6.9 | 95 | 29.7 | 199 | 62.2 | |||||||
| Using healthcare wearable devices has made (patient/me) feel so down in the dumps that nothing could cheer (him/her/me) up | 2 | 0.6 | 23 | 7.2 | 129 | 40.3 | 166 | 51.9 | |||||||
| Using healthcare wearable devices has made (patient/me) felt calm and peaceful | 133 | 41.6 | 148 | 46.3 | 38 | 11.9 | 1 | 0.3 | |||||||
| Using healthcare wearable devices has made (patient/me) felt downhearted and depressed | 3 | 0.9 | 21 | 6.6 | 145 | 45.3 | 151 | 47.2 | |||||||
| Using healthcare wearable devices has made (patient/me) to be happy | 132 | 42.2 | 158 | 49.4 | 26 | 8.1 | 1 | 0.3 | |||||||
| Reported Health Transition | Much better now than one year ago | Somewhat better now than one year ago | About the same as one year ago | Somewhat worse now than one year ago | Much worse now than one year ago | ||||||||||
| f | % | f | % | f | % | f | % | f | % | ||||||
| How is your (patient’s) health now compared to 1 year ago since using healthcare wearable devices? | 14 | 4.4 | 136 | 42.5 | 126 | 39.4 | 30 | 9.4 | 14 | 4.4 | |||||
| Social Functioning | Not at all | Slightly | Moderately | ||||||||||||
| f | % | f | % | f | % | ||||||||||
| During the past 4 weeks since using healthcare wearable devices, to what extent has your (patient’s) physical health or emotional problems interfered with your normal social activities with family, friends, neighbors, or groups? | 194 | 60.6 | 97 | 30.3 | 29 | 9.1 | |||||||||
| Some of the time | A little of the time | None of the time | |||||||||||||
| f | % | f | % | f | % | ||||||||||
| During the past 4 weeks since using healthcare wearable devices, how much of the time has your physical health or emotional problems interfered with your social activities (like visiting with friends, relatives, etc.)? | 17 | 5.3 | 20 | 6.3 | 283 | 88.4 | |||||||||
| Correlation Matrix and Square Root of the AVE Assessed by Fornell–Larcker Criterion | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| AUB | BI | EE | FC | PE | QoL | RC | SI | TA | |
| AUB | 0.814 | ||||||||
| BI | 0.644 | 0.874 | |||||||
| EE | 0.543 | 0.647 | 0.813 | ||||||
| FC | 0.721 | 0.654 | 0.856 | 0.762 | |||||
| PE | 0.185 | 0.249 | 0.086 | 0.050 | 0.869 | ||||
| QoL | 0.639 | 0.813 | 0.640 | 0.802 | 0.195 | 0.826 | |||
| RC | 0.237 | 0.193 | 0.235 | 0.280 | 0.162 | 0.205 | 0.852 | ||
| SI | 0.121 | 0.385 | 0.144 | 0.117 | 0.577 | 0.242 | 0.056 | 0.825 | |
| TA | 0.219 | 0.251 | 0.182 | 0.246 | 0.168 | 0.263 | 0.819 | 0.125 | 0.777 |
| Heterotrait–Monotrait Ratio of correlation (HTMT) | |||||||||
| AUB | BI | EE | FC | PE | QoL | RC | SI | TA | |
| AUB | |||||||||
| BI | 0.802 | ||||||||
| EE | 0.673 | 0.764 | |||||||
| FC | 0.933 | 0.808 | 1.073 | ||||||
| PE | 0.241 | 0.279 | 0.137 | 0.127 | |||||
| QoL | 0.998 | 1.178 | 0.949 | 1.276 | 0.297 | ||||
| RC | 0.294 | 0.221 | 0.269 | 0.339 | 0.195 | 0.299 | |||
| SI | 0.177 | 0.456 | 0.183 | 0.172 | 0.703 | 0.336 | 0.096 | ||
| TA | 0.279 | 0.280 | 0.215 | 0.309 | 0.208 | 0.384 | 0.972 | 0.146 | |
| AUB | BI | EE | FC | PE | QoL | RC | SI | TA | |
| AUB1 | 0.745 | 0.418 | 0.381 | 0.499 | 0.254 | 0.430 | 0.213 | 0.098 | 0.153 |
| AUB2 | 0.820 | 0.543 | 0.450 | 0.607 | 0.130 | 0.549 | 0.191 | 0.151 | 0.190 |
| AUB3 | 0.871 | 0.593 | 0.486 | 0.642 | 0.094 | 0.568 | 0.184 | 0.052 | 0.188 |
| BI1 | 0.565 | 0.878 | 0.577 | 0.595 | 0.298 | 0.854 | 0.166 | 0.321 | 0.191 |
| BI2 | 0.559 | 0.865 | 0.605 | 0.581 | 0.225 | 0.618 | 0.214 | 0.331 | 0.276 |
| BI3 | 0.565 | 0.879 | 0.514 | 0.538 | 0.126 | 0.659 | 0.124 | 0.359 | 0.189 |
| EE1 | 0.382 | 0.477 | 0.778 | 0.576 | 0.003 | 0.491 | 0.106 | 0.044 | 0.118 |
| EE2 | 0.359 | 0.503 | 0.822 | 0.667 | 0.121 | 0.523 | 0.167 | 0.103 | 0.099 |
| EE3 | 0.407 | 0.505 | 0.873 | 0.768 | −0.029 | 0.501 | 0.229 | 0.093 | 0.164 |
| EE4 | 0.583 | 0.598 | 0.776 | 0.749 | 0.162 | 0.554 | 0.244 | 0.209 | 0.199 |
| FC1 | 0.487 | 0.435 | 0.475 | 0.743 | 0.003 | 0.797 | 0.175 | 0.061 | 0.247 |
| FC2 | 0.680 | 0.439 | 0.490 | 0.785 | −0.008 | 0.605 | 0.201 | −0.015 | 0.144 |
| FC3 | 0.407 | 0.505 | 0.873 | 0.768 | −0.029 | 0.501 | 0.229 | 0.093 | 0.164 |
| FC4 | 0.583 | 0.598 | 0.776 | 0.749 | 0.162 | 0.554 | 0.244 | 0.209 | 0.199 |
| MT | 0.487 | 0.435 | 0.475 | 0.743 | 0.003 | 0.797 | 0.175 | 0.061 | 0.247 |
| PE1 | 0.160 | 0.250 | 0.065 | 0.066 | 0.896 | 0.203 | 0.141 | 0.572 | 0.143 |
| PE2 | 0.186 | 0.233 | 0.096 | 0.027 | 0.896 | 0.166 | 0.123 | 0.489 | 0.137 |
| PE3 | 0.126 | 0.138 | 0.059 | 0.034 | 0.813 | 0.123 | 0.176 | 0.417 | 0.176 |
| PH | 0.565 | 0.878 | 0.577 | 0.595 | 0.298 | 0.854 | 0.166 | 0.321 | 0.191 |
| RC1 | 0.222 | 0.149 | 0.169 | 0.197 | 0.165 | 0.171 | 0.844 | 0.041 | 0.720 |
| RC2 | 0.163 | 0.160 | 0.209 | 0.218 | 0.125 | 0.153 | 0.842 | 0.059 | 0.694 |
| RC3 | 0.171 | 0.148 | 0.219 | 0.265 | 0.116 | 0.177 | 0.871 | 0.045 | 0.652 |
| RC4 | 0.243 | 0.192 | 0.200 | 0.268 | 0.143 | 0.194 | 0.849 | 0.045 | 0.717 |
| SI1 | 0.030 | 0.218 | 0.150 | 0.099 | 0.455 | 0.103 | 0.025 | 0.757 | 0.064 |
| SI3 | 0.162 | 0.304 | 0.108 | 0.130 | 0.505 | 0.198 | 0.144 | 0.824 | 0.187 |
| SI4 | 0.094 | 0.393 | 0.115 | 0.072 | 0.481 | 0.262 | −0.017 | 0.890 | 0.064 |
| TA1 | 0.216 | 0.178 | 0.129 | 0.274 | 0.104 | 0.302 | 0.546 | 0.102 | 0.741 |
| TA2 | 0.222 | 0.149 | 0.169 | 0.197 | 0.165 | 0.171 | 0.844 | 0.041 | 0.720 |
| TA3 | 0.163 | 0.160 | 0.209 | 0.218 | 0.125 | 0.153 | 0.842 | 0.059 | 0.694 |
| TA5 | 0.156 | 0.146 | 0.097 | 0.129 | 0.144 | 0.157 | 0.604 | 0.061 | 0.805 |
| TA6 | 0.114 | 0.233 | 0.153 | 0.194 | 0.145 | 0.229 | 0.565 | 0.147 | 0.837 |
| TA7 | 0.178 | 0.256 | 0.114 | 0.153 | 0.118 | 0.200 | 0.561 | 0.130 | 0.849 |
| AUB | BI | EE | FC | PE | QoL | RC | SI | TA | |
| AUB | 1.000 | ||||||||
| BI | 1.747 | ||||||||
| EE | 3.814 | ||||||||
| FC | 1.747 | 3.892 | |||||||
| PE | 1.548 | ||||||||
| QoL | |||||||||
| RC | 3.187 | ||||||||
| SI | 1.555 | ||||||||
| TA | 3.127 |
References
- World Health Organization. Dementia—Fact Sheet; World Health Organization: Geneva, Switzerland, 2021; Available online: https://www.who.int/en/news-room/fact-sheets/detail/dementia (accessed on 20 October 2019).
- Dai, B.; Larnyo, E.; Tetteh, E.A.; Aboagye, A.K.; Musah, A.-A.I. Factors Affecting Caregivers’ Acceptance of the Use of Wearable Devices by Patients with Dementia: An Extension of the Unified Theory of Acceptance and Use of Technology Model. Am. J. Alzheimer’s Dis. Other Dement. 2020, 35, 1533317519883493. [Google Scholar] [CrossRef] [PubMed]
- International. AsD. ADI—Dementia Statistics. Alzheimer’s Disease International. Available online: www.alzint.org/about/dementia-facts-figures/dementia-statistics/ (accessed on 6 January 2020).
- Larnyo, E.; Dai, B.; Akey-Torku, B.; Nutakor, J.A.; Tetteh, E.A.; Larnyo, A.; Mensah, N.M.D. Evaluating Ghanaian Family Carers’ Perceptions on the Use of Healthcare Wearable Devices by Dementia Patients. Int. J. Sci. Res. Sci. Eng. Technol. 2020, 7, 612–627. [Google Scholar] [CrossRef]
- World Health Organization. Dementia: A Global Public Health Challenge. 2015. Available online: http://www.who.int/topics/dementia/en/ (accessed on 20 October 2019).
- Banerjee, S. Good news on dementia prevalence—We can make a difference. Lancet 2013, 382, 1384–1386. [Google Scholar] [CrossRef]
- Wu, W.; Haick, H. Materials and Wearable Devices for Autonomous Monitoring of Physiological Markers. Adv. Mater. 2018, 30, e1705024. [Google Scholar] [CrossRef] [PubMed]
- Ogundaini, O.O.; de la Harpe, R.; McLean, N. Integration of mHealth Information and Communication Technologies into the Clinical Settings of Hospitals in Sub-Saharan Africa: Qualitative Study. Adv. Digit. Health Open Sci. 2021, 9, e26358. [Google Scholar] [CrossRef]
- Bastoni, S.; Wrede, C.; da Silva, M.C.; Sanderman, R.; Gaggioli, A.; Braakman-Jansen, A.; van Gemert-Pijnen, L. Factors Influencing Implementation of eHealth Technologies to Support Informal Dementia Care: Umbrella Review. Adv. Digit. Health Open Sci. 2021, 4, e30841. [Google Scholar] [CrossRef]
- Wei, J.; Boger, J. Sleep Detection for Younger Adults, Healthy Older Adults, and Older Adults Living with Dementia Using Wrist Temperature and Actigraphy: Prototype Testing and Case Study Analysis. Adv. Digit. Health Open Sci. 2021, 9, e26462. [Google Scholar] [CrossRef]
- Theile, G.; Klaas, V.; Tröster, G.; Guckenberger, M. mHealth Technologies for Palliative Care Patients at the Interface of In-Patient to Outpatient Care: Protocol of Feasibility Study Aiming to Early Predict Deterioration of Patient’s Health Status. Adv. Digit. Health Open Sci. 2017, 6, e142. [Google Scholar] [CrossRef]
- Yang, P.; Bi, G.; Qi, J.; Wang, X.; Yang, Y.; Xu, L. Multimodal wearable intelligence for dementia care in healthcare 4.0: A survey. Inf. Syst. Front. 2021, 1–18. [Google Scholar] [CrossRef]
- Hoque, R.; Sorwar, G. Understanding factors influencing the adoption of mHealth by the elderly: An extension of the UTAUT model. Int. J. Med. Inform. 2017, 101, 75–84. [Google Scholar] [CrossRef]
- Collins, T.; Aldred, S.; Woolley, S.; Rai, S. Addressing the deployment challenges of health monitoring devices for a dementia study. In Proceedings of the 5th EAI International Conference on Wireless Mobile Communication and Healthcare-“Transforming Healthcare through Innovations in Mobile and Wireless Technologies”, London, UK, 14–16 October 2015; European Alliance for Innovation (EAI): Ghent, Belgium, 2015. [Google Scholar] [CrossRef]
- AlMahadin, G.; Lotfi, A.; Zysk, E.; Siena, F.L.; Carthy, M.M.; Breedon, P. Parkinson’s disease: Current assessment methods and wearable devices for evaluation of movement disorder motor symptoms—A patient and healthcare professional perspective. BMC Neurol. 2020, 20, 419. [Google Scholar] [CrossRef]
- Stavropoulos, T.G.; Lazarou, I.; Diaz, A.; Gove, D.; Georges, J.; Manyakov, N.V.; Pich, E.M.; Hinds, C.; Tsolaki, M.; Nikolopoulos, S.; et al. Wearable devices for assessing function in alzheimer’s disease: A european public involvement activity about the features and preferences of patients and caregivers. Front. Aging Neurosci. 2021, 13, 643135. [Google Scholar] [CrossRef] [PubMed]
- Megges, H.; Freiesleben, S.D.; Rösch, C.; Knoll, N.; Wessel, L.; Peters, O. User experience and clinical effectiveness with two wearable global positioning system devices in home dementia care. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2018, 4, 636–644. [Google Scholar] [CrossRef] [PubMed]
- Cote, A.C.; Phelps, R.J.; Kabiri, N.S.; Bhangu, J.S.; Thomas, K.K. Evaluation of wearable technology in dementia: A systematic review and meta-analysis. Front. Med. 2021, 7, 501104. [Google Scholar] [CrossRef] [PubMed]
- Dutta, K.K.; Sharma, S.; Sasidharan, A.; Mukundan, C.S. Sleep monitoring wearables: Present to future. In Wearable/Personal Monitoring Devices Present to Future; Gargiulo, G.D., Naik, G.R., Eds.; Springer: Singapore, 2022; pp. 133–152. [Google Scholar] [CrossRef]
- Ray, P.P.; Dash, D.; De, D. A systematic review and implementation of IOT-based pervasive sensor-enabled tracking system for dementia patients. J. Med. Syst. 2019, 43, 287. [Google Scholar] [CrossRef] [PubMed]
- Ehleringer, H.E.; Kim, S.J. The wearable lullaby: Improving sleep quality of caregivers of dementia patients. In Proceedings of the CHI ’13 Extended Abstracts on Human Factors in Computing Systems, Paris, France, 27 April–2 May 2013; Association for Computing Machinery: Paris, France, 2013; pp. 409–414. [Google Scholar] [CrossRef]
- Andersson, P.; Mattsson, L.-G. Service innovations enabled by the “internet of things”. IMP J. 2015, 9, 85–106. [Google Scholar] [CrossRef]
- Atzori, L.; Iera, A.; Morabito, G. The internet of things: A survey. Comput. Netw. 2010, 54, 2787–2805. [Google Scholar] [CrossRef]
- WHOQOL. WHOQOL: Measuring Quality of Life. Division of Mental Health and Prevention of Substance Abuse. 2012. Available online: https://www.who.int/tools/whoqol (accessed on 20 October 2019).
- Prevention CfDCa. Measuring Healthy Days: Population Assessment of the Health-Related Quality of Life; Centers for Disease Control and Prevention: Atlanta, Georgia, 2000.
- Gandek, B.; Sinclair, S.J.; Kosinski, M.; Ware, J.E., Jr. Psychometric evaluation of the SF-36 health survey in Medicare managed care. Health care financing review. Summer 2004, 25, 5–25. [Google Scholar]
- McHorney, C.A. Health status assessment methods for adults: Past accomplishments and future challenges. Annu. Rev. Public Health 1999, 20, 309–335. [Google Scholar] [CrossRef]
- Estoque, R.C.; Togawa, T.; Ooba, M.; Gomi, K.; Nakamura, S.; Hijioka, Y.; Kameyama, Y. A review of quality of life (QOL) assessments and indicators: Towards a “QOL-Climate” assessment framework. AMBIO 2019, 48, 619–638. [Google Scholar] [CrossRef]
- Moller, V. A place in the sun of life in South Africa. J. Soc. Indic. S. Afr. 1992, 9, 101–108. [Google Scholar]
- Moller, V. Quality of Life in South Africa: Measurement and Analysis; ERIC: Bristol, UK, 1987; ISBN 0796905037.
- Liu, D.; Maimaitijiang, R.; Gu, J.; Zhong, S.; Zhou, M.; Wu, Z.; Luo, A.; Lu, C.; Hao, Y. Using the Unified Theory of Acceptance and Use of Technology (UTAUT) to Investigate the Intention to Use Physical Activity Apps: Cross-Sectional Survey. JMIR Mhealth Uhealth 2019, 7, e13127. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Miguel Cruz, A.; Rios Rincon, A.; Buttar, V.; Ranson, Q.; Goertzen, D. What factors determine therapists’ acceptance of new technologies for rehabilitation—A study using the Unified Theory of Acceptance and Use of Technology (UTAUT). Disabil. Rehabil. 2015, 37, 447–455. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-P.; Anol, B. Learning Online Social Support: An Investigation of Network Information Technology Based on UTAUT. Cyber Psychol. Behav. 2008, 11, 268–272. [Google Scholar] [CrossRef] [PubMed]
- Sykes, T.A.; Venkatesh, V.; Gosain, S. Model of Acceptance with Peer Support: A Social Network Perspective to Understand Employees’ System Use. MIS Q. 2009, 33, 371–393. [Google Scholar] [CrossRef]
- Wang, Y.-S.; Wu, M.-C.; Wang, H.-Y. Investigating the determinants and age and gender differences in the acceptance of mobile learning. Br. J. Educ. Technol. 2009, 40, 92–118. [Google Scholar] [CrossRef]
- Chao, C.-M. Factors Determining the Behavioral Intention to Use Mobile Learning: An Application and Extension of the UTAUT Model. Front. Psychol. 2019, 10, 1652. [Google Scholar] [CrossRef]
- Wang, H.-Y.; Wang, S.-H. User acceptance of mobile internet based on the Unified Theory of Acceptance and Use of Technology: Investigating the determinants and gender differences. Soc. Behav. Personal. Int. J. 2010, 38, 415–426. [Google Scholar] [CrossRef]
- Hewitt, C.; Politis, I.; Amanatidis, T.; Sarkar, A. Assessing public perception of self-driving cars: The autonomous vehicle acceptance model. In Proceedings of the 24th International Conference on Intelligent User Interfaces, Marina del Ray, CA, USA, 17–20 March 2019; Association for Computing Machinery: New York, NY, USA, 2019; pp. 518–527. [Google Scholar]
- Venkatesh, V.; Morris, M.G.; Davis, G.B.; Davis, F.D. User acceptance of information technology: Toward a unified view. MIS Q. 2003, 425–478. [Google Scholar] [CrossRef]
- Boontarig, W.; Chutimaskul, W.; Chongsuphajaisiddhi, V.; Papasratorn, B. (Eds.) Factors influencing the Thai elderly intention to use smartphone for e-Health services. In Proceedings of the 2012 IEEE Symposium on Humanities, Science and Engineering Research, Kuala Lumpur, Malaysia, 24–27 June 2012; IEEE: Piscataway, NJ, USA, 2012. [Google Scholar]
- Sun, Y.; Wang, N.; Guo, X.; Peng, Z. Understanding the acceptance of mobile health services: A comparison and integration of alternative models. J. Electron. Commer. Res. 2013, 14, 183. [Google Scholar]
- Kraut, R.E.; Rice, R.E.; Cool, C.; Fish, R.S. Varieties of social influence: The role of utility and norms in the success of a new communication medium. Organ. Sci. 1998, 9, 437–453. [Google Scholar] [CrossRef]
- Rice, R.E.; Grant, A.E.; Schmitz, J.; Torobin, J. Individual and network influences on the adoption and perceived outcomes of electronic messaging. Soc. Netw. 1990, 12, 27–55. [Google Scholar] [CrossRef]
- Yuan, Y.; Fulk, J.; Shumate, M.; Monge, P.R.; Bryant, J.A.; Matsaganis, M. Individual Participation in Organizational Information Commons. Hum. Commun. Res. 2005, 31, 212–240. [Google Scholar] [CrossRef]
- LeRouge, C.M.; Hah, H.; Deckard, G.J.; Jiang, H. Designing for the Co-Use of Consumer Health Technology in Self-Management of Adolescent Overweight and Obesity: Mixed Methods Qualitative Study. JMIR Mhealth Uhealth 2020, 8, e18391. [Google Scholar] [CrossRef] [PubMed]
- Jewer, J. Patients’ intention to use online postings of ED wait times: A modified UTAUT model. Int. J. Med. Inform. 2018, 112, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Sheppard, B.H.; Hartwick, J.; Warshaw, P.R. The theory of reasoned action: A meta-analysis of past research with recommendations for modifications and future research. J. Consum. Res. 1988, 15, 325–343. [Google Scholar] [CrossRef]
- Venkatesh, V.; Davis, F.D. A theoretical extension of the technology acceptance model: Four longitudinal field studies. Manag. Sci. 2000, 46, 186–204. [Google Scholar] [CrossRef]
- Wang, H.; Liang, L.; Du, C.; Wu, Y. Implementation of Online Hospitals and Factors Influencing the Adoption of Mobile Medical Services in China: Cross-Sectional Survey Study. JMIR Mhealth Uhealth 2021, 9, e25960. [Google Scholar] [CrossRef]
- Han, S.; Mustonen, P.; Seppanen, M.; Kallio, M. Physicians’ behavior intentions regarding the use of mobile technology: An exploratory study. In Proceedings of the PACIS 2004 Proceedings, Shanghai, China, 8–11 July 2004; p. 49. [Google Scholar]
- Deng, Z.; Mo, X.; Liu, S. Comparison of the middle-aged and older users’ adoption of mobile health services in China. Int. J. Med. Inform. 2014, 83, 210–224. [Google Scholar] [CrossRef]
- Meuter, M.L.; Ostrom, A.L.; Bitner, M.J.; Roundtree, R. The influence of technology anxiety on consumer use and experiences with self-service technologies. J. Bus. Res. 2003, 56, 899–906. [Google Scholar] [CrossRef]
- Guo, X.; Sun, Y.; Wang, N.; Peng, Z.; Yan, Z. The dark side of elderly acceptance of preventive mobile health services in China. Electron. Mark. 2013, 23, 49–61. [Google Scholar] [CrossRef]
- Smither, J.A.-A.; Braun, C.C. Technology and older adults: Factors affecting the adoption of automatic teller machines. J. Gen. Psychol. 1994, 121, 381–389. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36): I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Folstein, F.M.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Ware, J.; Snow, K.; Kosinski, M.; Gandek, B. SF-36 Health Survey. Manual and Interpretation Guide; The Health Institute, New England Medical Center: Boston, MA, USA, 1993; p. 136. [Google Scholar]
- Collins, J.J.; Buncher, R.C.; Halperin, W. Managing the quality and conduct of epidemiologic studies. J. Occup. Environ. Med. 1991, 33, 1213–1215. [Google Scholar]
- Kroke, A.; Bergmann, M.M.; Lotze, G.; Jeckel, A.; Klipstein-Grobusch, K.; Boeing, H. Measures of quality control in the German component of the epic study. Ann. Nutr. Metab. 1999, 43, 216–224. [Google Scholar] [CrossRef]
- Babbie, E. The Basics of Social Research; Wadsworth/Thomson Learning: Belmont, CA, USA, 2002. [Google Scholar]
- Birky, W. Mating Patterns and Social Structure in a Wild Group of Formosan Macaques. Ph.D. Thesis, Department of Anthropology, Rutgers University, New Brunswick, NJ, USA, 2002. [Google Scholar]
- Prasanna, R.; Huggins, T.J. Factors affecting the acceptance of information systems supporting emergency operations centres. Comput. Hum. Behav. 2016, 57, 168–181. [Google Scholar] [CrossRef]
- Reinartz, W.; Haenlein, M.; Henseler, J. An empirical comparison of the efficacy of covariance-based and variance-based SEM. Int. J. Res. Mark. 2009, 26, 332–344. [Google Scholar] [CrossRef]
- Hair, J.J.F.; Sarstedt, M.; Matthews, L.M.; Ringle, C.M. Identifying and treating unobserved heterogeneity with FIMIX-PLS: Part I—method. Eur. Bus. Rev. 2016, 28, 63–76. [Google Scholar] [CrossRef]
- Hair, J.F.; Ringle, C.M.; Sarstedt, M. Partial least squares structural equation modeling: Rigorous applications, better results, and higher acceptance. Long-Range Plan. 2013, 46, 1–12. [Google Scholar] [CrossRef]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E.; Tatham, R.L. Multivariate Data Analysis; Prentice Hall: Upper Saddle River, NJ, USA, 1998. [Google Scholar]
- Fornell, C.; Larcker, D.F. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Hair, J.F., Jr.; Hult, G.T.M.; Ringle, C.; Sarstedt, M. A primer on Partial Least Squares Structural Equation Modeling (PLS-SEM), 1st ed.; Sage Publications: Thousand Oaks, CA, USA, 2014; ISBN 1483377431. [Google Scholar]
- Chin, W.; Newsted, P. Structural Equation Modeling Analysis with Small Samples Using Partial Least Square. In Statistical Strategies for Small Sample Research; Sage Publications: Thousand Oaks, CA, USA, 1999. [Google Scholar]
- Cho, H.-C.; Abe, S. Is two-tailed testing for directional research hypotheses tests legitimate? J. Bus. Res. 2013, 66, 1261–1266. [Google Scholar] [CrossRef]
- Hair Jr, J.F.; Sarstedt, M.; Ringle, C.M.; Gudergan, S.P. Advanced Issues in Partial Least Squares Structural Equation Modeling; Sage Publications: Thousand Oaks, CA, USA, 2017; ISBN 1483377385. [Google Scholar]
- Zhao, X.; Lynch, J.G., Jr.; Chen, Q. Reconsidering Baron, and Kenny: Myths and truths about mediation analysis. J. Consum. Res. 2010, 37, 197–206. [Google Scholar] [CrossRef]
- Alm, N.; Astell, A.; Ellis, M.; Dye, R.; Gowans, G.; Campbell, J. A cognitive prosthesis and communication support for people with dementia. Neuropsychol. Rehabil. 2004, 14, 117–134. [Google Scholar] [CrossRef]
- Hamada, T.; Kuwahara, N.; Morimoto, K.; Yasuda, K.; Akira, U.; Abe, S. (Eds.) Preliminary Study on Remote Assistance for People with Dementia at Home by Using Multi-media Contents. Universal Access in Human-Computer Interaction Addressing Diversity; Springer: Berlin/Heidelberg, Germany, 2009. [Google Scholar]
- Gibson, G.; Dickinson, C.; Brittain, K.; Robinson, L. The everyday use of assistive technology by people with dementia and their family carers: A qualitative study. BMC Geriatr. 2015, 15, 89. [Google Scholar] [CrossRef] [PubMed]
- Olsson, A.; Engström, M.; Skovdahl, K.; Lampic, C. My, your and our needs for safety and security: Relatives’ reflections on using information and communication technology in dementia care. Scand. J. Caring Sci. 2012, 26, 104–112. [Google Scholar] [CrossRef]
- Price, C. Evaluation of an activity monitoring system for people with dementia. J. Assist. Technol. 2007, 1, 11–17. [Google Scholar] [CrossRef]
- Wang, R.H.; Sudhama, A.; Begum, M.; Huq, R.; Mihailidis, A. Robots to assist daily activities: Views of older adults with Alzheimer’s disease and their caregivers. Int. Psychogeriatr. 2017, 29, 67–79. [Google Scholar] [CrossRef]
- Riikonen, M.; Paavilainen, E.; Salo, H. Factors supporting the use of technology in the daily life of home-living people with dementia. Technol. Disabil. 2013, 25, 233–243. [Google Scholar] [CrossRef]
- Alvseike, H.; Brønnick, K. Feasibility of the iPad as a hub for smart house technology in the elderly; effects of cognition, self-efficacy, and technology experience. J. Multidiscip. Healthc. 2012, 5, 299. [Google Scholar] [CrossRef]
- Czaja, S.J.; Charness, N.; Fisk, A.D.; Hertzog, C.; Nair, S.N.; Rogers, W.A.; Sharit, J. Factors predicting the use of technology: Findings from the center for research and education on aging and technology enhancement (CREATE). Psychol. Aging 2006, 21, 333. [Google Scholar] [CrossRef] [PubMed]
- Melenhorst, A.-S.; Rogers, W.A.; Bouwhuis, D.G. Older adults’ motivated choice for technological innovation: Evidence for benefit-driven selectivity. Psychol. Aging 2006, 21, 190. [Google Scholar] [CrossRef] [PubMed]
- Van den Heuvel, E.; Jowitt, F.; McIntyre, A. Awareness, requirements and barriers to use of Assistive Technology designed to enable independence of people suffering from Dementia (ATD). Technol. Disabil. 2012, 24, 139–148. [Google Scholar] [CrossRef]
- Chou, H.K.; Yan, S.H.; Lin, I.C.; Tsai, M.T.; Chen, C.C.; Woung, L.C. A pilot study of the telecare medical support system as an intervention in dementia care: The views and experiences of primary caregivers. J. Nurs. Res. 2012, 20, 169–180. [Google Scholar] [CrossRef]
- Cristancho-Lacroix, V.; Moulin, F.; Wrobel, J.; Batrancourt, B.; Plichart, M.; De Rotrou, J.; Cantegreil-Kallen, I.; Rigaud, A.S. A web-based program for informal caregivers of persons with alzheimer’s disease: An iterative user-centered design. JMIR Res. Protoc. 2014, 3, e46. [Google Scholar] [CrossRef]
- Lundberg, S. The results from a two-year case study of an information and communication technology support system for family caregivers. Disabil. Rehabil. Assist. Technol. 2014, 9, 353–358. [Google Scholar] [CrossRef]
- O’Neill, S.A.; Mason, S.; Parente, G.; Donnelly, M.P.; Nugent, C.D.; McClean, S.; Scotney, B.; Craig, D. Video Reminders as Cognitive Prosthetics for People with Dementia. Ageing Int. 2011, 36, 267–282. [Google Scholar] [CrossRef]
- Schroeter, C.; Mueller, S.; Volkhardt, M.; Einhorn, E.; Huijnen, C.; van den Heuvel, H.; van Berlo, A.; Bley, A.; Gross, H.-M. Realization and user evaluation of a companion robot for people with mild cognitive impairments. In Proceedings of the 2013 IEEE International Conference on Robotics and Automation, Karlsruhe, Germany, 6–10 May 2013. [Google Scholar] [CrossRef]
- Orpwood, R.; Gibbs, C.; Adlam, T.; Faulkner, R.; Meegahawatte, D. The design of smart homes for people with dementia—user-interface aspects. Univers. Access Inf. Soc. 2005, 4, 156–164. [Google Scholar] [CrossRef]
- Cahill, S.; Begley, E.; Faulkner, J.P.; Hagen, I. “It gives me a sense of independence” findings from Ireland on the use and usefulness of assistive technology for people with dementia. Technol. Disabil. 2007, 19, 133–142. [Google Scholar] [CrossRef]
- Boyd, A.; Synnott, J.; Nugent, C.; Elliott, D.; Kelly, J. Community-based trials of mobile solutions for the detection and management of cognitive decline. Healthc. Technol. Lett. 2017, 4, 93–96. [Google Scholar] [CrossRef]
- Robinson, L.; Brittain, K.; Lindsay, S.; Jackson, D.; Olivier, P. Keeping in touch everyday (kite) project: Developing assistive technologies with people with dementia and their carers to promote independence. Int. Psychogeriatr. 2009, 21, 494–502. [Google Scholar] [CrossRef] [PubMed]
- Williams, K.; Pennathur, P.; Bossen, A.; Gloeckner, A. Adapting telemonitoring technology use for older adults: A pilot study. Res. Gerontol. Nurs. 2016, 9, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Serafini, D.J.; Damianakis, T.; Marziali, E. Clinical practice standards and ethical issues applied to a virtual group intervention for spousal caregivers of people with alzheimer’s. Soc. Work. Health Care 2007, 44, 225–243. [Google Scholar] [CrossRef] [PubMed]
- Evans, N.; Harris, N.; Kuppuswamy, A. A smarter future: Technology to enhance an independent lifestyle for our future selves. Int. J. Ther. Rehabil. 2011, 18, 694–699. [Google Scholar] [CrossRef]
- Guisado-Fernández, E.G.; Mackey, L.M.; Blake, C.; Caulfield, B.M. Factors influencing the adoption of smart health technologies for people with dementia and their informal caregivers: Scoping review and design framework. JMIR Aging 2019, 2, e12192. [Google Scholar] [CrossRef]
- Carlsson, C., Carlsson, J., Hyvonen, K., Puhakainen, J., Walden, P., Eds.; Adoption of Mobile Devices/Services—Searching for Answers with the UTAUT. In Proceedings of the 39th Annual Hawaii International Conference on System Sciences (HICSS’06), Kauai, HI, USA, 4–7 January 2006. [Google Scholar]
- Tam, T.M.; Dosso, J.A.; Robillard, J.M. The impact of a global pandemic on people living with dementia and their care partners: Analysis of 417 lived experience reports. J. Alzheimers Dis. 2021, 80, 865–875. [Google Scholar] [CrossRef]
- Stara, V.; Vera, B.; Bolliger, D.; Paolini, S.; de Jong, M.; Felici, E.; Koenderink, S.; Rossi, L.; Von Doellen, V.; and di Rosa, M. Toward the integration of technology-based interventions in the care pathway for people with dementia: A cross-national study. Int. J. Environ. Res. Public Health 2021, 18, 10405. [Google Scholar] [CrossRef]
- Werner, P.; Stein-Shvachman, I.; Korczyn, A.D. Early onset dementia: Clinical and social aspects. Int. Psychogeriatr. 2009, 21, 631–636. [Google Scholar] [CrossRef]
- Bhattacherjee, A.; Hikmet, N. Reconceptualizing organizational support and its effect on information technology usage: Evidence from the health care sector. J. Comput. Inf. Syst. 2008, 48, 69–76. [Google Scholar] [CrossRef]
- Pan, S.; Jordan-Marsh, M. Internet use intention and adoption among Chinese older adults: From the expanded technology acceptance model perspective. Comput. Hum. Behav. 2010, 26, 1111–1119. [Google Scholar] [CrossRef]
- Venkatesh, V.; Thong, J.Y.; Xu, X. Consumer acceptance and use of information technology: Extending the unified theory of acceptance and use of technology. MIS Q. 2012, 36, 157–178. [Google Scholar] [CrossRef]
- Kijsanayotin, B.; Pannarunothai, S.; Speedie, S.M. Factors influencing health information technology adoption in Thailand’s community health centers: Applying the UTAUT model. Int. J. Med. Inform. 2009, 78, 404–416. [Google Scholar] [CrossRef] [PubMed]
- Xue, L.; Yen, C.C.; Chang, L.; Chan, H.C.; Tai, B.C.; Tan, S.B.; Duh, H.B.L.; Choolani, M. An exploratory study of aging women’s perception on access to health informatics via a mobile phone-based intervention. Int. J. Med. Inform. 2012, 81, 637–648. [Google Scholar] [CrossRef] [PubMed]


| Variable | Caregivers | PWDs | |
|---|---|---|---|
| Age (years) | |||
| 18 years | 4 (7%) | 0 (0%) | |
| 19 to 31 | 13 (22%) | 0 (0%) | |
| 32 to 44 | 19 (33%) | 0 (0%) | |
| 45 to 54 | 14 (24%) | 75 (28%) | |
| 55 to 64 | 6 (10%) | 120 (46%) | |
| 65 to 74 | 2 (3%) | 54 (21%) | |
| 75 and over | 0 (0%) | 13 (5%) | |
| Gender, n (%) | |||
| Female | 32 (55%) | 143 (55%) | |
| Male | 26 (45%) | 119 (45%) | |
| Marital Status | |||
| Single | 33 (57%) | 44 (17%) | |
| Married | 12 (21%) | 121 (46%) | |
| Widowed | 0 (0%) | 25 (10%) | |
| Widower | 0 (0%) | 23 (9%) | |
| Divorced | 13 (22%) | 49 (19%) | |
| Level of Education | |||
| No Formal Education | 3 (5%) | 19 (7%) | |
| Primary School | 4 (7%) | 56 (21%) | |
| Less Than JHS | 1 (2%) | 2 (1%) | |
| Junior High School (JHS) | 7 (12%) | 82 (31%) | |
| Less Than SHS | 15 (26%) | 15 (6%) | |
| Senior High School (SHS) | 3 (5%) | 37 (14%) | |
| Nursing Diploma | 5 (9%) | 17 (6%) | |
| Teacher College Diploma | 7 (12%) | 16 (6%) | |
| Higher National Diploma (HND) | 1 (2%) | 7 (3%) | |
| Bachelor’s Degree | 12 (21%) | 11 (4%) | |
| Region of Residence | |||
| Greater Accra | 25 (43%) | 112 (43%) | |
| Eastern | 14 (24%) | 34 (26%) | |
| Ashanti | 19 (33%) | 68 (32%) | |
| Years of Illness or Caregiving | |||
| Less than 1 year | 10 (17%) | 23 (9%) | |
| 1 to 2 years | 19 (33%) | 52 (20%) | |
| 3 to 4 years | 8 (14%) | 109 (42%) | |
| 5 to 6 years | 11 (19%) | 55 (21%) | |
| 7 to 8 years | 6 (10%) | 11 (4%) | |
| 9 to 10 years | 3 (5%) | 11 (4%) | |
| Over 20 years | 1 (2%) | 1 (0%) | |
| MMSE Score | Frequency | Percentage | |
| Mild | 14 | 4% | |
| Moderate | 248 | 78% | |
| Severe | 58 | 18% |
| Scale | Cronbach Alpha | Cronbach Alpha Based on Standardized Items | n of Items | Mean | SD |
|---|---|---|---|---|---|
| Physical Functioning | 0.82 | 0.82 | 10 | 886.875 | 134.022 |
| Role Physical | 0.70 | 0.70 | 4 | 332.81 | 108.067 |
| Bodily Pain | 0.70 | 0.70 | 2 | 187.063 | 20.128 |
| General Health | 0.63 | 0.64 | 5 | 382.578 | 77.171 |
| Vitality | 0.70 | 0.70 | 4 | 332.813 | 108.068 |
| Social Functioning | 0.70 | 0.70 | 2 | 186.938 | 20.172 |
| Role Emotion | 0.60 | 0.60 | 3 | 274.375 | 62.595 |
| Mental Health | 0.70 | 0.68 | 5 | 304.156 | 61.489 |
| Constructs | Notation | Convergent Validity | Internal Consistency Reliability | ||
|---|---|---|---|---|---|
| Outer Loading | AVE | α | CR | ||
| Behavioral Intention | BI1 | 0.878 | 0.764 | 0.85 | 0.91 |
| BI2 | 0.865 | ||||
| BI3 | 0.879 | ||||
| Effort Expectancy | EE1 | 0.778 | 0.661 | 0.83 | 0.89 |
| EE2 | 0.822 | ||||
| EE3 | 0.873 | ||||
| EE4 | 0.776 | ||||
| Facilitating Conditions | FC1 | 0.743 | 0.580 | 0.76 | 0.85 |
| FC2 | 0.785 | ||||
| FC3 | 0.768 | ||||
| FC4 | 0.749 | ||||
| Performance Expectancy | PE1 | 0.896 | 0.756 | 0.84 | 0.90 |
| PE2 | 0.896 | ||||
| PE3 | 0.813 | ||||
| Resistance to Change | RC1 | 0.844 | 0.725 | 0.87 | 0.91 |
| RC2 | 0.842 | ||||
| RC3 | 0.871 | ||||
| RC4 | 0.849 | ||||
| Social Influence | SI1 | 0.757 | 0.681 | 0.77 | 0.87 |
| SI3 | 0.824 | ||||
| SI4 | 0.890 | ||||
| Technology Anxiety | TA1 | 0.741 | 0.603 | 0.87 | 0.90 |
| TA2 | 0.720 | ||||
| TA3 | 0.694 | ||||
| TA5 | 0.805 | ||||
| TA6 | 0.837 | ||||
| TA7 | 0.849 | ||||
| Actual Use Behavior | AUB1 | 0.745 | 0.62 | 0.75 | 0.85 |
| AUB2 | 0.820 | ||||
| AUB3 | 0.871 | ||||
| Quality of Life | PH | 0.854 | 0.682 | 0.54 | 0.81 |
| MT | 0.797 | ||||
| Hypothesis | Path | β | t-Statistics | p-Value | Hypothesis Supported or Not | |
|---|---|---|---|---|---|---|
| H1 | PE a→ BI b | 0.052 | 1.145 | 0.25 | Not Supported | |
| H2 | EE c→ BI | 0.295 | 4.410 | <0.001 | Supported | |
| H3 | SI d→ BI | 0.253 | 4.929 | <0.001 | Supported | |
| H4 | FC e→ BI | 0.366 | 5.383 | <0.001 | Supported | |
| H5 | FC→AUB f | 0.524 | 10.351 | <0.001 | Supported | |
| H6a | BI→AUB | 0.301 | 5.666 | <0.001 | Supported | |
| H7 | RC h→BI | −0.170 | 2.366 | 0.01 | Supported | |
| H8 | TA i→ BI | 0.206 | 2.912 | <0.001 | Supported | |
| H9 | AUB→QoL g | 0.639 | 17.448 | <0.001 | Supported | |
| Result of the Coefficients of Determination (R2) | ||||||
| CONSTRUCTS | R Square | R Square Adjusted | Remarks | |||
| AUB | 0.572 | 0.569 | Moderate | |||
| BI | 0.560 | 0.551 | Moderate | |||
| QoL | 0.408 | 0.406 | Moderate | |||
| Result of Blindfolding and Predictive Relevance (Q2) and Effect Size (q2) | ||||||
| CONSTRUCTS | Q2 | CONSTRUCTS | q2 | |||
| AUB | 0.370 | AUB→QoL | 0.157 | |||
| BI | 0.407 | BI→AUB | 0.062 | |||
| QoL | 0.271 | |||||
| Indirect Effects | ||||||
|---|---|---|---|---|---|---|
| Original Sample (O) | Sample Mean (M) | Standard Deviation (STDEV) | t Statistics (|O/STDEV|) | p Value | Remark Significant? | |
| BI→AUB | ||||||
| FC→AUB | 0.110 | 0.110 | 0.032 | 3.442 | <0.001 | Yes |
| FC→BI | ||||||
| Direct Effects | ||||||
| BI→AUB | 0.301 | 0.299 | 0.053 | 5.666 | <0.001 | Yes |
| FC→AUB | 0.524 | 0.525 | 0.051 | 10.351 | <0.001 | Yes |
| FC→BI | 0.366 | 0.364 | 0.068 | 5.383 | <0.001 | Yes |
| Hypothesis | Path | β | t-Statistics | p Value | Remarks |
|---|---|---|---|---|---|
| H10a | RC × EE→BI | 0.239 | 1.349 | 0.18 | Not Supported |
| H10b | RC × SI→BI | −0.255 | 2.383 | 0.01 | Supported |
| H10c | RC × FC→BI | −0.214 | 1.310 | 0.19 | Not Supported |
| H11a | TA × EE→BI | −0.052 | 0.312 | 0.76 | Not Supported |
| H11b | TA × SI→BI | 0.093 | 0.950 | 0.34 | Not Supported |
| H11c | TA × FC→BI | 0.168 | 1.071 | 0.29 | Not Supported |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Larnyo, E.; Dai, B.; Larnyo, A.; Nutakor, J.A.; Ampon-Wireko, S.; Nkrumah, E.N.K.; Appiah, R. Impact of Actual Use Behavior of Healthcare Wearable Devices on Quality of Life: A Cross-Sectional Survey of People with Dementia and Their Caregivers in Ghana. Healthcare 2022, 10, 275. https://doi.org/10.3390/healthcare10020275
Larnyo E, Dai B, Larnyo A, Nutakor JA, Ampon-Wireko S, Nkrumah ENK, Appiah R. Impact of Actual Use Behavior of Healthcare Wearable Devices on Quality of Life: A Cross-Sectional Survey of People with Dementia and Their Caregivers in Ghana. Healthcare. 2022; 10(2):275. https://doi.org/10.3390/healthcare10020275
Chicago/Turabian StyleLarnyo, Ebenezer, Baozhen Dai, Abigail Larnyo, Jonathan Aseye Nutakor, Sabina Ampon-Wireko, Edmund Nana Kwame Nkrumah, and Ruth Appiah. 2022. "Impact of Actual Use Behavior of Healthcare Wearable Devices on Quality of Life: A Cross-Sectional Survey of People with Dementia and Their Caregivers in Ghana" Healthcare 10, no. 2: 275. https://doi.org/10.3390/healthcare10020275
APA StyleLarnyo, E., Dai, B., Larnyo, A., Nutakor, J. A., Ampon-Wireko, S., Nkrumah, E. N. K., & Appiah, R. (2022). Impact of Actual Use Behavior of Healthcare Wearable Devices on Quality of Life: A Cross-Sectional Survey of People with Dementia and Their Caregivers in Ghana. Healthcare, 10(2), 275. https://doi.org/10.3390/healthcare10020275