
Clinical Experience of High Frequency and Low Frequency TENS in Treatment of Diabetic Neuropathic Pain in Russia

 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
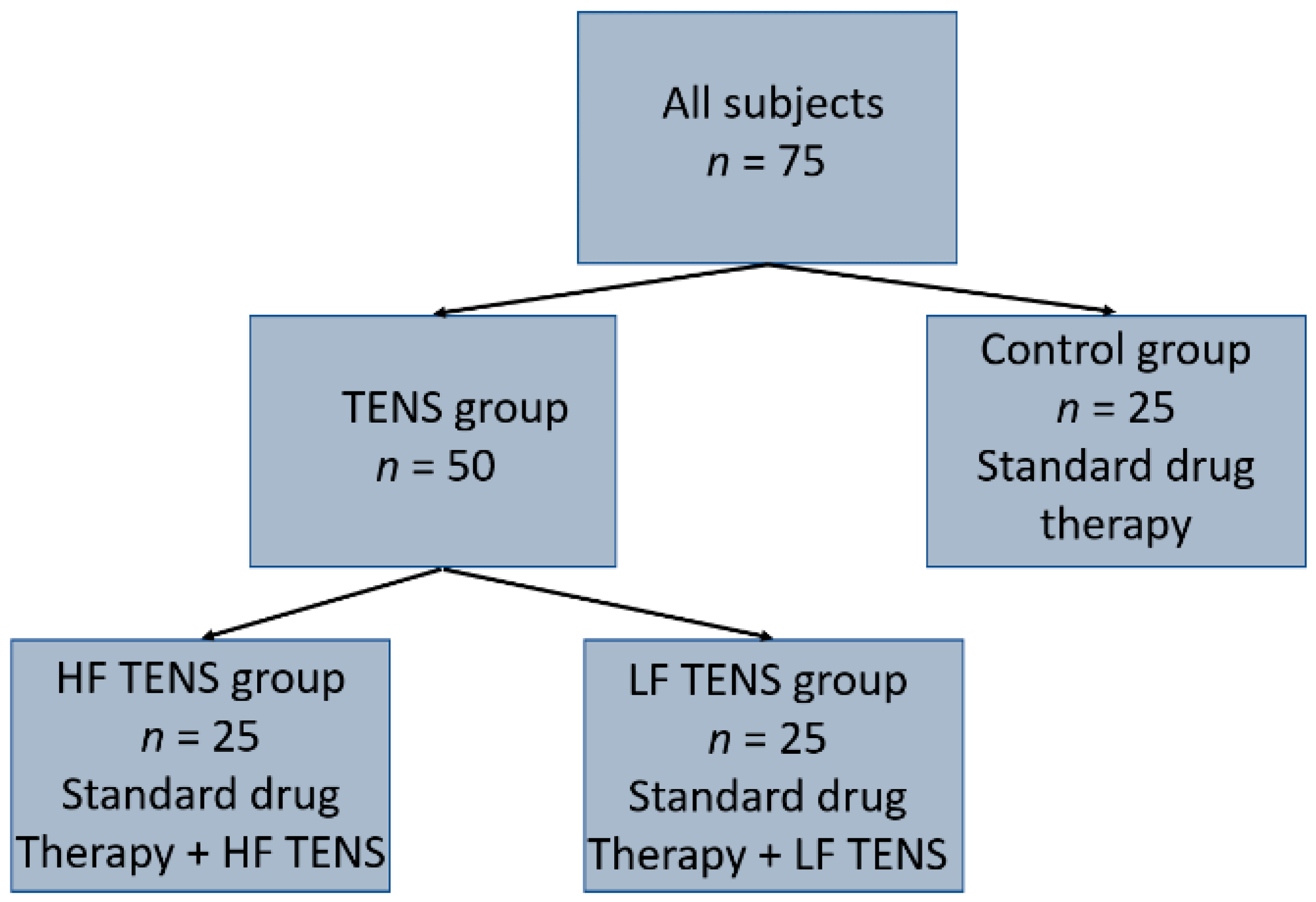
2.1. Participants
- Age—from 21 to 60 years old, including first period middle-aged (males 22–35 years, females 21–35 years) and second period middle-aged (males 36–60 years, females 36–55 years);
- Medically stable type 2 diabetes mellitus (the diagnosis was made by an endocrinologist or internist);
- Serum level HbA1c in two separate tests is lower than 7.0%;
- Distal axonal neuropathy of lower extremity vitrificated by electromyography (EMG);
- History of neuropathic pain for over 6 months;
- Neuropathic pain intensity is 5 scores or more on the visual analogue scale (VAS) and 4 scores or more on the Douleur Neuropathique 4 Questions (DN4).
- Epilepsy and uncontrolled seizure disorder;
- Severely cognitive disorders;
- Mental illness;
- Hereditary polyneuropathy;
- History of peroneal nerve injury in the fibular tunnel or tibial nerve in the tarsal tunnel;
- History of stroke, spinal cord injury, traumatic brain injury, multiple sclerosis;
- Edema of lower extremity;
- History of cardiac arrhythmias or hemodynamic instability;
- Cardiac pacemaker or other implanted electronic system;
- Botulinum toxin injections to any lower extremity muscle in the last 3 months;
- Evidence of deep venous thrombosis or other forms of venous thromboembolism;
- Rheumatoid arthritis, gout, psoriasis and arthrosis of the joints of the lower extremities;
- Vascular atherosclerosis of the lower extremities.
2.2. Characteristics of Standard Drug Therapy
2.3. Characteristics of Motor and Sensory Disorders
2.4. Characteristics of Neuropathic Pain Assessment Tools
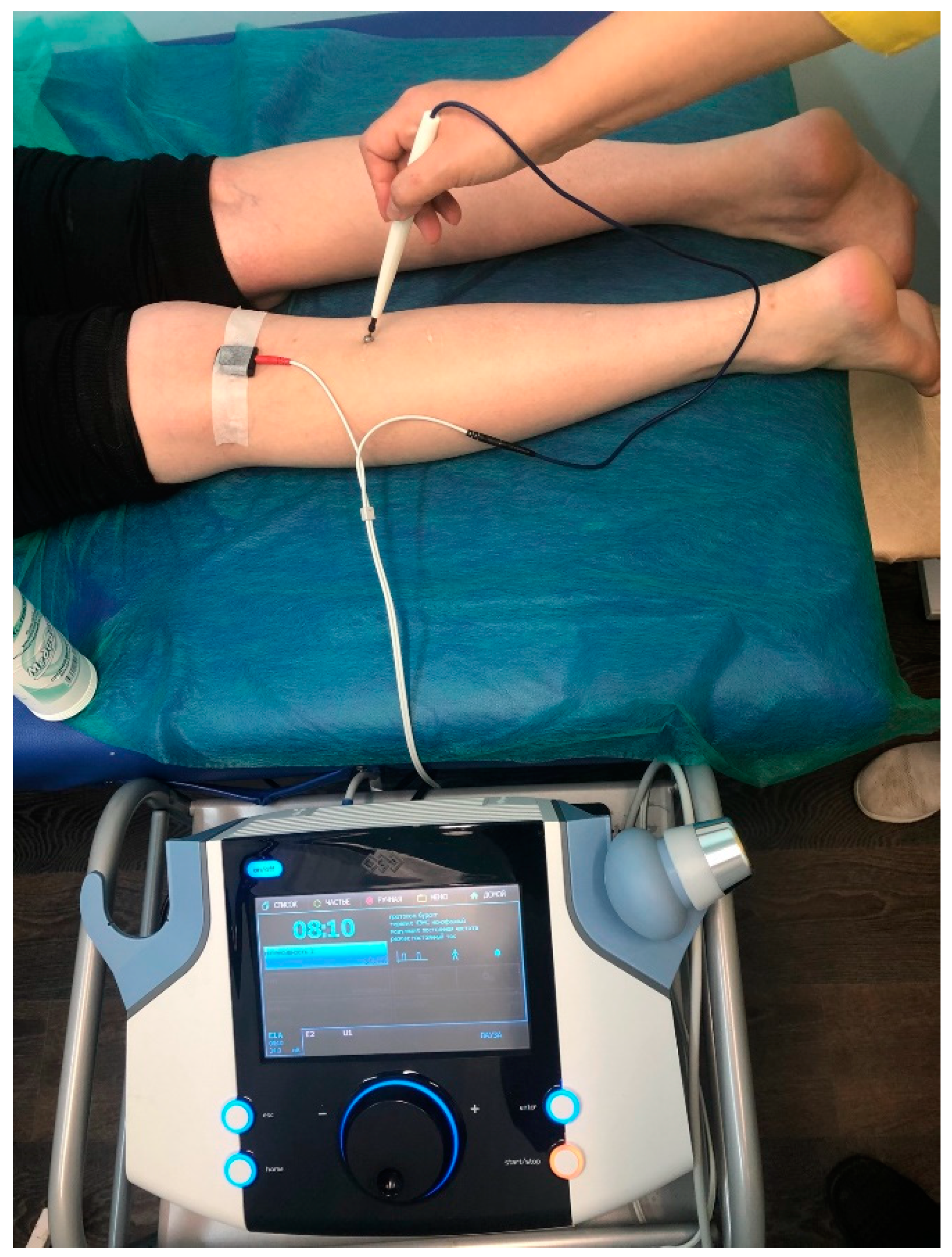
2.5. TENS Technique
2.6. Statistical Analysis
3. Results
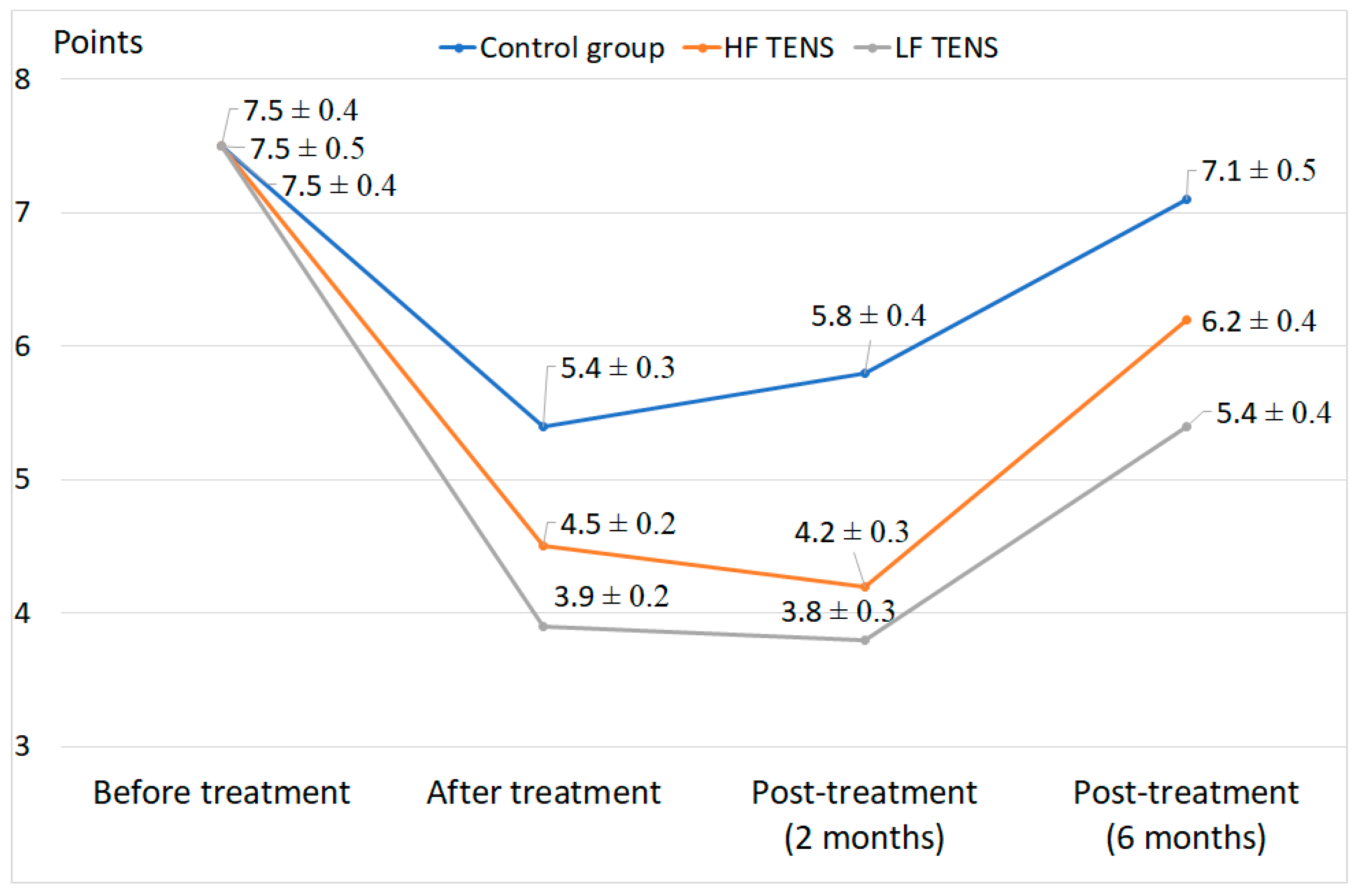
3.1. Pain Assessment Using VAS
3.2. Pain Assessment Using MPQ
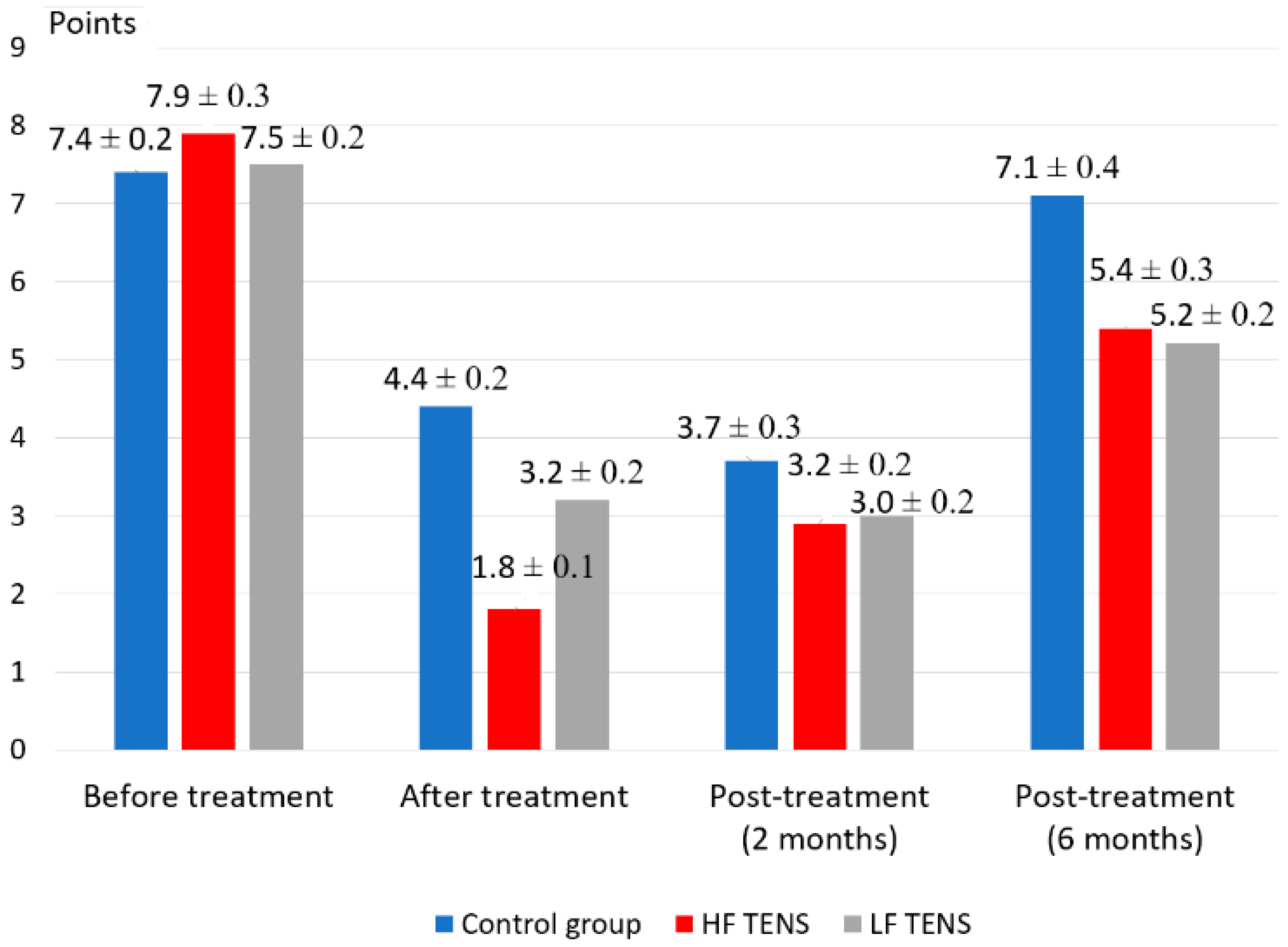
3.3. Pain Assessment Using DN4
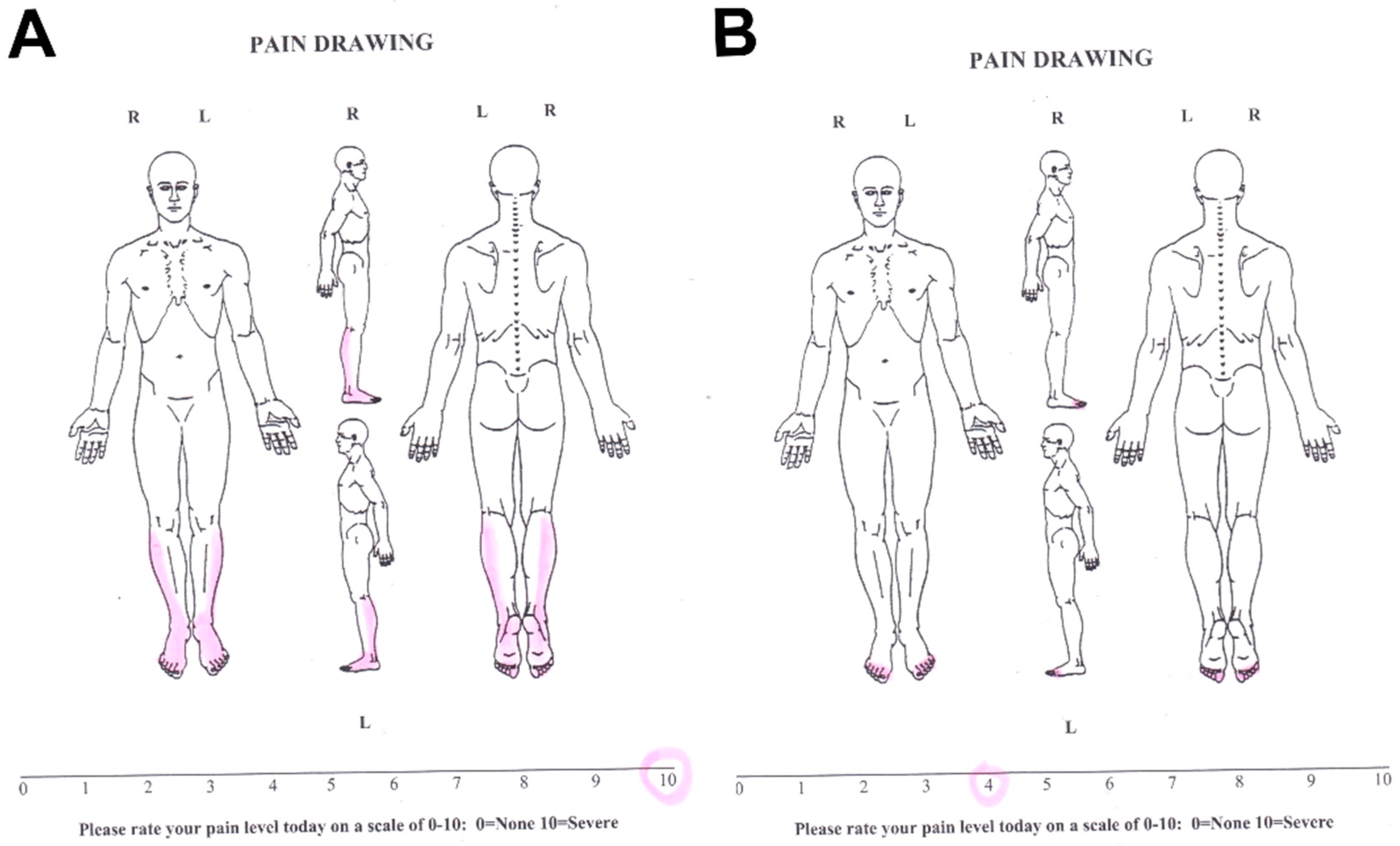
3.4. Pain Assessment Using Pain Drawing
4. Discussion
- Using direct TENS of peroneal and tibial nerves in treatment of neuropathic pain;
- A combination of HF TENS and LF TENS in treatment of patients with neuropathic pain;
- Complex application of VAS, MPQ, DN4 and Pain Drawing in neuropathic pain diagnosis in patients with diabetic neuropathies.
5. Limitations
- It was not possible to study the effectiveness of the combined use of HF TENS and LF TENS in the treatment of diabetic neuropathic pain and to compare these results with the use of separate methods of TENS;
- There was no comparative analysis of the effectiveness of HF TENS and LF TENS in the treatment of diabetic neuropathic pain between patients with type 1 diabetes mellitus and type 2 diabetes mellitus;
- We could not investigate the effectiveness of TENS methods in the treatment of patients with myelinopathy type of peripheral nerve disorders, and we could not compare these results with the results of treatment of patients with an axonal disorder;
- We could not study the effectiveness of TENS compared with the use of sham stimulation in the control group.
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Al Zamil, M.K. Results of a comparative analysis between transcutaneous electroneurostimulation and acupuncture in the treatment of 548 patients with diabetic distal polyneuropathy of the lower extremities. Clin. Neurol. 2019, 4, 9–17. [Google Scholar]
- Gürgen, S.G.; Sayın, O.; Cetin, F.; Tuç Yücel, A. Transcutaneous electrical nerve stimulation (TENS) accelerates cutaneous wound healing and inhibits proinflammatory cytokines. Inflammation 2014, 37, 775–784. [Google Scholar] [CrossRef] [PubMed]
- Vieira, P.J.; Ribeiro, J.P.; Cipriano, G., Jr.; Umpierre, D.; Cahalin, L.P.; Moraes, R.S.; Chiappa, G.R. Effect of transcutaneous electrical nerve stimulation on muscle metaboreflex in healthy young and older subjects. Eur. J. Appl. Physiol. 2012, 112, 1327–1334. [Google Scholar] [CrossRef] [PubMed]
- Haan, N.; Song, B. Therapeutic application of electric fields in the injured nervous system. Adv. Wound Care 2014, 3, 56–165. [Google Scholar] [CrossRef] [Green Version]
- Kutlu, A.K.; Ceçen, D.; Gürgen, S.G.; Sayın, O.; Cetin, F. A Comparison Study of Growth Factor Expression following Treatment with Transcutaneous Electrical Nerve Stimulation, Saline Solution, Povidone-Iodine, and Lavender Oil in Wounds Healing. Evid Based Complement. Alternat. Med. 2013, 2013, 361832. [Google Scholar] [CrossRef]
- Luo, B.; Huang, J.; Lu, L.; Hu, X.; Luo, Z.; Li, M. Electrically induced brain derived neurotrophic factor release from Schwann cells. J. Neurosci. Res. 2014, 92, 893–903. [Google Scholar] [CrossRef]
- Forciniti, L.; Ybarra, J.; Zaman, M.; Schmidt, C. Schwann cell response on polypyrrole substrates upon electrical stimulation. Acta Biomater. 2014, 10, 2423–2433. [Google Scholar] [CrossRef]
- Al-Majed, A.A.; Neumann, C.M.; Brushart, T.M.; Gordon, T. Brief electrical stimulation promotes the speed and accuracy of motor axonal regeneration. J. Neurosci. 2000, 20, 2602–2608. [Google Scholar] [CrossRef]
- Asensio-Pinilla, E.; Udina, E.; Jaramillo, J.; Navarro, X. Electrical stimulation combined with exercise increase axonal regeneration after peripheral nerve injury. Exp. Neurol. 2009, 219, 258–265. [Google Scholar] [CrossRef]
- Al Zamil, M.; Kulikova, N.; Bezrukova, O.; Volkova, I.; Stahurlova, V. Effectiveness of transcutaneous electrical neurostimulation for treatment of diabetic distal polyneuropathy. Eur. J. Neurol. 2019, 26, 552–744. [Google Scholar]
- Al Zamil, M.K.; Kulikova, N.G.; Minenko, I.A.; Vasil’va, E.S. Direct transcutaneous electroneurostimulation in the treatment of pathologies of the peripheral nervous system. Physiotherapist 2020, 3, 57–69. [Google Scholar] [CrossRef]
- Eberstein, A.; Eberstein, S. Electrical stimulation of denervated muscle: Is it worth, while? Med. Sci. Sports Exerc. 1996, 28, 1463–1469. [Google Scholar] [CrossRef] [PubMed]
- Gibson, W.; Benedict, M.; Wand, B.M.; Meads, C.; Catley, M.J.; O’Connell, N.E. Transcutaneous electrical nerve stimulation (TENS) for chronic pain—An overview of Cochrane Reviews. Cochrane Database Syst. Rev. 2019, 4, CD011890. [Google Scholar] [CrossRef] [PubMed]
- Nabi, B.N.; Saberi, A.; Eghbali, B.B.; Hosseininezhad, M.; Gelareh Biazar, G. Efficacy and Safety of TENS and Duloxetine in Patients with Painful Diabetic Neuropathy: A Single Blind Randomized Clinical Trial. J. Adv. Med. Biomed. Res. 2021, 29, 286–292. [Google Scholar] [CrossRef]
- Petrova, M.M.; Shnayder, N.A.; Kirichkova, G.A. Diabetic neuropathy: Definition, epidemiology. Sib. Med. Rev. 2008, 6, 97–102. [Google Scholar]
- Didangelos, T.; Doupis, J.; Veves, A. Painful diabetic neuropathy: Clinical aspects. Handb. Clin. Neurol. 2014, 126, 53–61. [Google Scholar] [CrossRef] [Green Version]
- Tesfaye, S.; Boulton, A.J.; Dickenson, A.H. Mechanisms and management of diabetic painful distal symmetrical polyneuropathy. Diabetes Care 2013, 36, 2456–2465. [Google Scholar] [CrossRef] [Green Version]
- Davoudi, M.; Rezaei, P.; Rajaeiramsheh, F.; Ahmadi, S.; Taheri, A.A. Predicting the quality of life based on pain dimensions and psychiatric symptoms in patients with Painful diabetic neuropathy: A cross-sectional prevalence study in Iranian patients. Health Qual Life Outcomes 2021, 19, 49. [Google Scholar] [CrossRef]
- Melikoglu, M.A.; Celik, A. Does Neuropathic Pain Affect the Quality of Sleep? Eurasian J. Med. 2017, 49, 40–43. [Google Scholar] [CrossRef]
- Minenko, I.A.; Al-Zamil, M.K. Dynamics of the quality of life of patients with diabetic neuropathic pain syndrome against the background of the complex application of transcutaneous electrical nerve stimulation and acupuncture. Sib. Sci. Med. J. 2017, 37, 62–67. [Google Scholar]
- Singh-Franco, D.; Jacobs, R.J. Patient perspectives on peripheral neuropathic pain experience within the community. Diabetes Metab. Syndr. Clin. Res. Rev. 2017, 11, S243–S246. [Google Scholar] [CrossRef]
- Teixeira, M.J. Challenges in the treatment of neuropathic pain. Drugs Today 2009, 45, 1–5. [Google Scholar]
- Moisset, X.; Bouhassira, D.; Couturier, J.A.; Alchaar, H.; Conradi, S.; Delmotte, M.H.; Lanteri-Minet, M.; Lefaucheur, J.P.; Mick, G.; Piano, V.; et al. Pharmacological and non-pharmacological treatments for neuropathic pain: Systematic review and French recommendations. Rev. Neurol. 2020, 176, 325–352. [Google Scholar] [CrossRef]
- Tesfaye, S.; Vileikyte, L.; Rayman, G.; Sindrup, S.H.; Perkins, B.A.; Baconja, M.; Vinik, A.I.; Boulton, A.J.M. Painful diabetic peripheral neuropathy: Consensus recommendations on diagnosis, assessmentand management. Diabetes Metab Res. Rev. 2011, 27, 629–638. [Google Scholar] [CrossRef]
- Shahanawaz, S.D. Effect of high TENS on neuropathic pain in diabetic neuropathy patients. Int. J. Physiother. Res. 2014, 2, 604–607. [Google Scholar]
- Upton, G.A.; Tinley, P.; Al-Aubaidy, H.; Crawford, R. The influence of transcutaneous electrical nerve stimulation parameters on the level of pain perceived by participants with painful diabetic neuropathy: A crossover study. Diabetes Metab Syndr. 2017, 11, 113–118. [Google Scholar] [CrossRef]
- Melzack, R.; Wall, P.D. Acupuncture and transcutaneous electrical nerve stimulation. Postgrad Med. J. 1984, 60, 893–896. [Google Scholar] [CrossRef] [Green Version]
- Melzack, R.; Wall, P.D. Pain mechanisms: A new theory. Science 1965, 150, 971–979. [Google Scholar] [CrossRef]
- Sabino, G.S.; Santos, C.M.; Francischi, J.N.; Resende, M.A. Release of endogenous opioids following transcutaneous electric nerve stimulation in an experimental model of acute inflammatory pain. J. Pain 2008, 9, 157–163. [Google Scholar] [CrossRef]
- Gozani, S.N. Remote Analgesic Effects of Conventional Transcutaneous Electrical Nerve Stimulation: A Scientific and Clinical Review With A Focus On Chronic Pain. Pain Res. 2019, 12, 3185–3201. [Google Scholar] [CrossRef] [Green Version]
- Nabi, B.N.; Sedighinejad, A.; Haghighi, M.; Biazar, G.; Hashemi, M.; Haddadi, S.; Fathi, A. Comparison of transcutaneous electrical nerve stimulation and pulsed radiofrequency sympathectomy for treating painful diabetic neuropathy. Anesthesiol. Pain Med. 2015, 5, e29280. [Google Scholar] [CrossRef] [Green Version]
- Johnson, M. Transcutaneous Electrical Nerve Stimulation: Mechanisms, Clinical Application and Evidence. Rev. Pain 2007, 1, 7–11. [Google Scholar] [CrossRef]
- Kocyigit, F.; Akalin, E.; Gezer, N.S.; Orbay, O.; Kocyigit, A.; Ada, E. Functional magnetic resonance imaging of the effects of low-frequency transcutaneous electrical nerve stimulation on central pain modulation: A double-blind, placebo-controlled trial. Clin. J. Pain 2012, 28, 581–588. [Google Scholar] [CrossRef]
- Mokhtari, T.; Ren, Q.; Li, N.; Wang, F.; Bi, Y.; Hu, L. Transcutaneous Electrical Nerve Stimulation in Relieving Neuropathic Pain: Basic Mechanisms and Clinical applications. Curr. Pain Headache Rep. 2020, 24, 14. [Google Scholar] [CrossRef]
- Reis, F.; Guimarães, F.; Nogueira, L.C.; Meziat-Filho, N.; Sanchez, T.A.; Wideman, T. Association between pain drawing and psychological factors in musculoskeletal chronic pain: A systematic review. Physiother. Theory Pract. 2019, 35, 533–542. [Google Scholar] [CrossRef]
- Warke, K.; Al-Smadi, J.; Baxter, D. Walsh, D.M. Lowe-Strong AS. Efficacy of transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain in a multiple sclerosis population: A randomized, placebo-controlled clinical trial. Clin. J. Pain 2006, 22, 812–819. [Google Scholar] [CrossRef]
- Jin, D.; Xu, Y.; Geng, D.; Yan, T. Effect of transcutaneous electrical nerve stimulation on symptomatic diabetic peripheral neuropathy: A meta-analysis of randomized controlled trials. Diabetes Res. Clin. Pract. 2010, 89, 10–15. [Google Scholar] [CrossRef]
- Sluka, K.A.; Bjordal, J.M.; Marchand, S.; Rakel, B.A. What makes transcutaneous electrical nerve stimulation work? Making sense of the mixed results in the clinical literature. Phys. Ther. 2013, 93, 1397–1402. [Google Scholar] [CrossRef]
- Sluka, K.A.; Deacon, M.; Stibal, A.; Strissel, S.; Terpstra, A. Spinal blockade of opioid receptors prevents the analgesia produced by TENS in arthritic rats. J. Pharmacol. Exp. Ther. 1999, 289, 840–846. [Google Scholar]
- Somers, D.; Clemente, F.R. Transcutaneous electrical nerve stimulation for the management of neuropathic pain: The effects of frequency and electrode position on prevention of allodynia in a rat model of complex regional pain syndrome type II. Phys. Ther. 2006, 86, 698–709. [Google Scholar] [CrossRef] [Green Version]
- Vance, C.G.; Dailey, D.L.; Rakel, B.A.; Sluka, K.A. Using TENS for pain control: The state of the evidence. Pain Manag. 2014, 4, 197–209. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Before Treatment (Mean ± S.E.M.) | After Treatment (Mean ± S.E.M.) | 2 Months Post-treatment (Mean ± S.E.M.) | 6 Months Post-treatment (Mean ± S.E.M.) |
|---|---|---|---|---|
| Sensory Dimensions | ||||
| Control group | 16.2 ± 0.41 | 11.4 ± 0.56 * | 10.4 ± 0.40 * | 14.7 ± 0.49 |
| HF TENS | 15.3 ± 0.42 | 6.10 ± 0.43 *# | 7.22 ± 0.43 *# | 10.3 ± 0.36 *# |
| LF TENS | 15.2 ± 0.43 | 9.42 ± 0.42 *# | 7.51 ± 0.42 *# | 11.1 ± 0.45 *# |
| Affective Dimensions | ||||
| Control group | 10.2 ± 0.39 | 6.4 ± 0.28 * | 7.2 ± 0.27 * | 9.82 ± 0.4 |
| HF TENS | 9.10 ± 0.35 | 5.0 ± 0.21 *# | 5.5 ± 0.11 *# | 6.9 ± 0.29 *# |
| LF TENS | 10.3 ± 0.36 | 3.28 ± 0.27 *# | 2.9 ± 0.17 *# | 4.5 ± 0.34 *# |
| Evaluative Dimensions | ||||
| Control group | 4.5 ± 0.11 | 3.4 ± 0.26 * | 3.3 ± 0.20 * | 4.3 ± 0.19 |
| HF TENS | 4.6 ± 0.12 | 1.5 ± 0.13 *# | 2.3 ± 0.13 *# | 2.8 ± 0.16 *# |
| LF TENS | 4.6 ± 0.11 | 1.7 ± 0.12 *# | 1.5 ± 0.12 *# | 2.7 ± 0.15 *# |
| Total Pain Rating Index | ||||
| Control group | 30.9 ± 0.37 | 21.2 ± 0.25 * | 20.9 ± 0.23 * | 28.8 ± 0.24 |
| HF TENS | 29.0 ± 0.39 | 12.6 ± 0.24 *# | 15 ± 0.22 *# | 20 ± 0.24 *# |
| LF TENS | 30.1 ± 0.37 | 14.4 ± 0.24 *# | 11.9 ± 0.17 *# | 18.3 ± 0.23 *# |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Zamil, M.; Minenko, I.A.; Kulikova, N.G.; Alade, M.; Petrova, M.M.; Pronina, E.A.; Romanova, I.V.; Narodova, E.A.; Nasyrova, R.F.; Shnayder, N.A. Clinical Experience of High Frequency and Low Frequency TENS in Treatment of Diabetic Neuropathic Pain in Russia. Healthcare 2022, 10, 250. https://doi.org/10.3390/healthcare10020250
Al-Zamil M, Minenko IA, Kulikova NG, Alade M, Petrova MM, Pronina EA, Romanova IV, Narodova EA, Nasyrova RF, Shnayder NA. Clinical Experience of High Frequency and Low Frequency TENS in Treatment of Diabetic Neuropathic Pain in Russia. Healthcare. 2022; 10(2):250. https://doi.org/10.3390/healthcare10020250
Chicago/Turabian StyleAl-Zamil, Mustafa, Inessa A. Minenko, Natalia G. Kulikova, Michael Alade, Marina M. Petrova, Elena A. Pronina, Irina V. Romanova, Ekaterina A. Narodova, Regina F. Nasyrova, and Natalia A. Shnayder. 2022. "Clinical Experience of High Frequency and Low Frequency TENS in Treatment of Diabetic Neuropathic Pain in Russia" Healthcare 10, no. 2: 250. https://doi.org/10.3390/healthcare10020250
APA StyleAl-Zamil, M., Minenko, I. A., Kulikova, N. G., Alade, M., Petrova, M. M., Pronina, E. A., Romanova, I. V., Narodova, E. A., Nasyrova, R. F., & Shnayder, N. A. (2022). Clinical Experience of High Frequency and Low Frequency TENS in Treatment of Diabetic Neuropathic Pain in Russia. Healthcare, 10(2), 250. https://doi.org/10.3390/healthcare10020250