



A Comprehensive Appraisal of Meta-Analyses of Exercise-Based Stroke Rehabilitation with Trial Sequential Analysis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Identification and Screening of Studies
2.2. Data Extraction
2.3. Data Analysis
2.3.1. Statistical Methods
2.3.2. Outcome Definitions
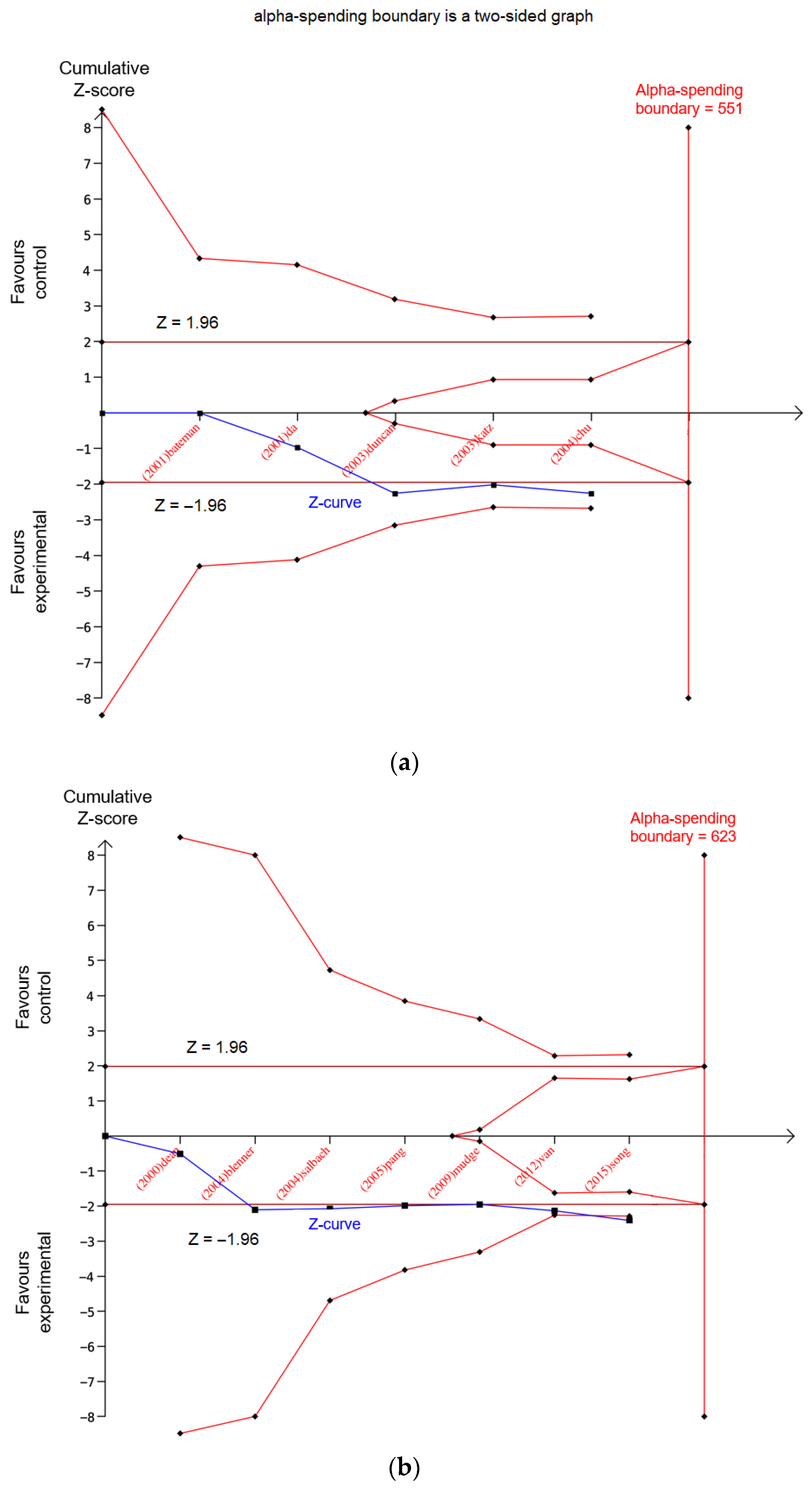
- Potentially spurious evidence of effects: Analyses whose last point of the Z-curve is outside the conventional boundary (i.e., significant in the original meta-analysis) but inside of the monitoring boundary present potentially spurious evidence, indicating that further trials or larger samples are required. (Figure 3a).
- Firm evidence of effects: Analyses whose Z-curves cross the monitoring boundary but do not reach the RIS present firm evidence of intervention effects (Figure 3b).
- Absence of evidence: Analyses whose Z-curves do not reach the RIS and remain inside the conventional boundary present an absence of evidence. This indicates that, although the result was deemed insignificant, increasing the sample size may lead to a different result (Figure 3c).
- Lack of effect: Analyses whose Z-curves reach the RIS but do not cross the conventional boundary are considered to most likely have no significant effect (Figure 3d).
- Verified intervention effects: Analyses whose Z-curves cross the monitoring boundary and also reach the RIS are considered to have a ‘verified’ intervention effect, indicating that the intervention effects are indeed statistically significant (Figure 3e).
3. Results
3.1. Eligible Meta-Analyses
3.2. Characteristics of Meta-Analyses
3.3. Meta-Analyses with Potentially Spurious Evidence
3.4. Meta-Analyses with Firm Evidence of Effects
3.5. Meta-Analyses with the Absence of Evidence
3.6. Meta-Analyses with a Lack of Effect
3.7. Meta-Analyses with Verified Intervention Effects
3.8. Sensitivity Analyses of the TSA
4. Discussion
4.1. Discrepancies in the Results of Three Types of Exercise Interventions
4.2. Consistency in the Results of Theory-Based Exercise
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Searching Strategy
Appendix A.1. CINAHL (to May 2022)
Appendix A.2. PubMed (to May 2022)
Appendix A.3. Medline (to May 2022)
Appendix A.4. Embase (to May 2022)
Appendix A.5. Scopus (to May 2022)
Appendix A.6. Cochrane (to May 2022)
References
- Field, A.P.; Gillett, R. How to do a meta-analysis. Br. J. Math. Stat. Psychol. 2010, 63, 665–694. [Google Scholar] [CrossRef] [PubMed]
- Hedges, L.V. Meta-analysis. J. Educ. Stat. 1992, 17, 279–296. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Phillips, A.N. Meta-analysis: Principles and procedures. BMJ 1997, 315, 1533–1537. [Google Scholar] [CrossRef] [Green Version]
- Schulz, K.F.; Chalmers, I.; Hayes, R.J.; Altman, D.G. Empirical evidence of bias: Dimensions of methodological quality associated with estimates of treatment effects in controlled trials. JAMA 1995, 273, 408–412. [Google Scholar] [CrossRef]
- Berkey, C.S.; Mosteller, F.; Lau, J.; Antman, E.M. Uncertainty of the time of first significance in random effects cumulative meta-analysis. Control. Clin. Trials 1996, 17, 357–371. [Google Scholar] [CrossRef]
- Hughes, M.D.; Pocock, S.J. Stopping rules and estimation problems in clinical trials. Stat. Med. 1988, 7, 1231–1242. [Google Scholar] [CrossRef]
- Armitage, P. Sequential analysis in therapeutic trials. Annu. Rev. Med. 1969, 20, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Pocock, S.J. Group sequential methods in the design and analysis of clinical trials. Biometrika 1977, 64, 191–199. [Google Scholar] [CrossRef]
- Lan, K.G.; Hu, M.; Cappelleri, J.C. Applying the law of iterated logarithm to cumulative meta-analysis of a continuous endpoint. Stat. Sin. 2003, 13, 1135–1145. [Google Scholar]
- Wetterslev, J.; Jakobsen, J.C.; Gluud, C. Trial sequential analysis in systematic reviews with meta-analysis. BMC Med. Res. Methodol. 2017, 17, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brok, J.; Thorlund, K.; Gluud, C.; Wetterslev, J. Trial sequential analysis reveals insufficient information size and potentially false positive results in many meta-analyses. J. Clin. Epidemiol. 2008, 61, 763–769. [Google Scholar] [CrossRef] [PubMed]
- Kang, H. Trial sequential analysis: Novel approach for meta-analysis. Anesth. Pain Med. 2021, 16, 138–150. [Google Scholar] [CrossRef]
- Castellini, G.; Bruschettini, M.; Gianola, S.; Gluud, C.; Moja, L. Assessing imprecision in Cochrane systematic reviews: A comparison of GRADE and Trial Sequential Analysis. Syst. Rev. 2018, 7, 110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wetterslev, J.; Thorlund, K.; Brok, J.; Gluud, C. Trial sequential analysis may establish when firm evidence is reached in cumulative meta-analysis. J. Clin. Epidemiol. 2008, 61, 64–75. [Google Scholar] [CrossRef]
- Kwakkel, G.; Lannin, N.A.; Borschmann, K.; English, C.; Ali, M.; Churilov, L.; Saposnik, G.; Winstein, C.; Van Wegen, E.E.; Wolf, S.L.; et al. Standardized measurement of sensorimotor recovery in stroke trials: Consensus-based core recommendations from the stroke recovery and rehabilitation roundtable. Neurorehabilit. Neural Repair 2017, 31, 784–792. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.-Y.; Park, B.-S.; Kim, J. Effects of high frequency repetitive transcranial magnetic stimulation with physical healthy exercise in stroke. Toxicol. Environ. Health Sci. 2015, 7, 160–170. [Google Scholar] [CrossRef]
- Buscemi, N.; Hartling, L.; Vandermeer, B.; Tjosvold, L.; Klassen, T.P. Single data extraction generated more errors than double data extraction in systematic reviews. J. Clin. Epidemiol. 2006, 59, 697–703. [Google Scholar] [CrossRef]
- Thorlund, K.; Engstrøm, J.; Wetterslev, J.; Brok, J.; Imberger, G.; Gluud, C. User Manual for Trial Sequential Analysis (TSA); Copenhagen Trial Unit: Copenhagen, Denmark, 2017; pp. 1–119. [Google Scholar]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Demets, D.L.; Lan, K.G. Interim analysis: The alpha spending function approach. Stat. Med. 1994, 13, 1341–1352. [Google Scholar] [CrossRef]
- Saunders, D.H.; Sanderson, M.; Hayes, S.; Johnson, L.; Kramer, S.; Carter, D.D.; Jarvis, H.; Brazzelli, M.; Mead, G.E. Physical fitness training for stroke patients. Cochrane Database Syst. Rev. 2020, 2020, CD003316. [Google Scholar]
- Pang, M.Y.; Eng, J.J.; Dawson, A.S.; Gylfadóttir, S. The use of aerobic exercise training in improving aerobic capacity in individuals with stroke: A meta-analysis. Clin. Rehabil. 2006, 20, 97–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonini-Rocha, A.C.; de Andrade, A.L.S.; Moraes, A.M.; Gomide Matheus, L.B.; Diniz, L.R.; Martins, W.R. Effectiveness of Circuit-Based Exercises on Gait Speed, Balance, and Functional Mobility in People Affected by Stroke: A Meta-Analysis. PM&R 2018, 10, 398–409. [Google Scholar] [CrossRef]
- Pogrebnoy, D.; Dennett, A. Exercise programs delivered according to guidelines improve mobility in people with stroke: A systematic review and meta-analysis. Int. J. Stroke 2019, 14, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qin, L.; Wei, X.; Liu, L.; Zhu, H. Effectiveness of tai chi on movement, emotion and quality of life in patients with stroke: A meta-analysis. Chin. J. Tissue Eng. Res. 2016, 20, 297–303. [Google Scholar] [CrossRef]
- Balady, G.J.; Williams, M.A.; Ades, P.A.; Bittner, V.; Comoss, P.; Foody, J.M.; Franklin, B.; Sanderson, B.; Southard, D. Core components of cardiac rehabilitation/secondary prevention programs: 2007 update: A scientific statement from the american heart association exercise, cardiac rehabilitation, and prevention committee, the council on clinical cardiology; the councils on cardiovascular nursing, epidemiology and prevention, and nutrition, physical activity, and metabolism; and the american association of cardiovascular and pulmonary rehabilitation. Circulation 2007, 115, 2675–2682. [Google Scholar] [PubMed] [Green Version]
- Mehrholz, J.; Thomas, S.; Elsner, B. Treadmill training and body weight support for walking after stroke. Cochrane Database Syst. Rev. 2017, 2017, CD002840. [Google Scholar] [CrossRef]
- Van Peppen, R.P.; Kwakkel, G.; Wood-Dauphinee, S.; Hendriks, H.J.; Van der Wees, P.J.; Dekker, J. The impact of physical therapy on functional outcomes after stroke: What’s the evidence? Clin. Rehabil. 2004, 18, 833–862. [Google Scholar] [CrossRef]
- Outermans, J.C.; Van De Port, I.; Wittink, H.; Kwakkel, G. Associations between aerobic capacity and walking capacity after stroke: A meta-analysis. In Cerebrovascular Diseases; Karger: Basel, Switzerland, 2013; Volume 35, p. 210. [Google Scholar]
- Begde, A.; Caliskan, O.; Campbell, L. Systematic review and meta-analysis of randomised controlled trials of hybrid assistive limb-assisted gait training for improving post-stroke gait ability. Eur. Stroke J. 2021, 6, 468. [Google Scholar]
- Lin, Y.H.; Lien, Y.S.; Tsai, C.Y.; Hsu, A.L.; Yu, M.H.; Chang, Y.J.; Chuang, L.L.; Wong, A.M. Effect of dual-task training on gait speed in individuals with stroke-a systematic review and meta analysis. Cerebrovasc. Dis. 2017, 43, 81–82. [Google Scholar]
- Plummer, P.; Iyigün, G. Effects of Physical Exercise Interventions on Dual-Task Gait Speed Following Stroke: A Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2018, 99, 2548–2560. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Q.X.; Ge, L.; Wang, C.C.; Ma, Q.S.; Liao, Y.T.; Huang, P.P.; Wang, G.D.; Xie, Q.L.; Rask, M. Robot-assisted therapy for balance function rehabilitation after stroke: A systematic review and meta-analysis. Int. J. Nurs. Stud. 2019, 95, 7–18. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.-Y.; Cheng, Y.-H.; Lai, C.-H.; Lin, Y.-N. Clinical non-superiority of technology-assisted gait training with body weight support in patients with subacute stroke: A meta-analysis. Ann. Phys. Rehabil. Med. 2020, 63, 535–542. [Google Scholar] [CrossRef] [PubMed]
- Moucheboeuf, G.; Griffier, R.; Gasq, D.; Glize, B.; Bouyer, L.; Dehail, P.; Cassoudesalle, H. Effects of robotic gait training after stroke: A meta-analysis. Ann. Phys. Rehabil. Med. 2020, 63, 518–534. [Google Scholar] [CrossRef]
- Jeon, B.-J.; Kim, W.-H.; Park, E.-Y. Effect of task-oriented training for people with stroke: A meta-analysis focused on repetitive or circuit training. Top. Stroke Rehabil. 2015, 22, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Youkhana, S.; Dean, C.M.; Wolff, M.; Sherrington, C.; Tiedemann, A. Yoga-based exercise improves balance and mobility in people aged 60 and over: A systematic review and meta-analysis. Age Ageing 2016, 45, 21–29. [Google Scholar] [CrossRef] [Green Version]
- Ge, L.; Zheng, Q.-X.; Liao, Y.-T.; Tan, J.-Y.; Xie, Q.-L.; Rask, M. Effects of traditional Chinese exercises on the rehabilitation of limb function among stroke patients: A systematic review and meta-analysis. Complement. Ther. Clin. Pract. 2017, 29, 35–47. [Google Scholar] [CrossRef]
- Wu, S.; Chen, J.; Wang, S.; Jiang, M.; Wang, X.; Wen, Y. Effect of Tai Chi Exercise on Balance Function of Stroke Patients: A Meta-Analysis. Med. Sci. Monit. Basic Res. 2018, 24, 210–215. [Google Scholar] [CrossRef]
- Zou, L.; Wang, C.; Chen, X.; Wang, H. Baduanjin exercise for stroke rehabilitation: A systematic review with meta-analysis of randomized controlled trials. Int. J. Environ. Res. Public Health 2018, 15, 600. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Stone, A.J. Combined Aerobic and Resistance Training for Cardiorespiratory Fitness, Muscle Strength, and Walking Capacity after Stroke: A Systematic Review and Meta-Analysis. J. Stroke Cerebrovasc. Dis. 2020, 29, 104498. [Google Scholar] [CrossRef] [Green Version]
- Ada, L.; Dorsch, S.; Canning, C.G. Strengthening interventions increase strength and improve activity after stroke: A systematic review. Aust. J. Physiother. 2006, 52, 241–248. [Google Scholar] [CrossRef] [Green Version]
- Veldema, J.; Jansen, P. Resistance training in stroke rehabilitation: Systematic review and meta-analysis. Clin. Rehabil. 2020, 34, 1173–1197. [Google Scholar] [CrossRef] [PubMed]
- Regan, E.W.; Handlery, R.; Beets, M.W.; Fritz, S.L. Are Aerobic Programs Similar in Design to Cardiac Rehabilitation Beneficial for Survivors of Stroke? A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2019, 8, e012761. [Google Scholar] [CrossRef] [PubMed]
- Anan, W. Is Robot-Assisted Gait Training More Effective on Improving Gait Velocity and Balance in Poststroke Patients Compared to Conventional Overground Gait Training? A Meta-Analysis. Ph.D. Thesis, California State University, Fresno, CA, USA, 2017. [Google Scholar]
- Mehrholz, J.; Pohl, M.; Kugler, J.; Elsner, B. The Improvement of Walking Ability Following Stroke: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials. Dtsch. Aerzteblatt Int. 2018, 115, 639–645. [Google Scholar] [CrossRef]
- Calabrò, R.S.; Sorrentino, G.; Cassio, A.; Mazzoli, D.; Andrenelli, E.; Bizzarini, E.; Campanini, I.; Carmignano, S.M.; Cerulli, S.; Chisari, C.; et al. robotic-assisted gait rehabilitation following stroke: A systematic review of current guidelines and practical clinical recommendations. Eur. J. Phys. Rehabil. Med. 2021, 57, 460–471. [Google Scholar] [CrossRef] [PubMed]
- Ghai, S.; Ghai, I.; Effenberg, A.O. Effects of dual tasks and dual-task training on postural stability: A systematic review and meta-analysis. Clin. Interv. Aging 2017, 12, 557–577. [Google Scholar] [CrossRef] [Green Version]
- Luo, X.C.; Zhou, J.; Zhang, Y.G.; Liu, Y.Y.; Li, J.J.; Zheng, Z.; Tong, F.; Feng, F. Effects of Tai Chi Yunshou on upper limb function and balance in stroke survivors: A protocol for systematic review and meta analysis. Medicine 2020, 99, e21040. [Google Scholar] [CrossRef] [PubMed]
- Shen, C.; Liu, F.; Yao, L.; Li, Z.; Qiu, L.; Fang, S. Effects of MOTOmed movement therapy on the mobility and activities of daily living of stroke patients with hemiplegia: A systematic review and meta-analysis. Clin. Rehabil. 2018, 32, 1569–1580. [Google Scholar] [CrossRef]
- Nedergård, H.; Arumugam, A.; Sandlund, M.; Bråndal, A.; Häger, C.K. Effect of robotic-assisted gait training on objective biomechanical measures of gait in persons post-stroke: A systematic review and meta-analysis. J. NeuroEng. Rehabil. 2021, 18, 64. [Google Scholar] [CrossRef] [PubMed]
- Tedla, J.S.; Dixit, S.; Gular, K.; Abohashrh, M. Robotic-Assisted Gait Training Effect on Function and Gait Speed in Subacute and Chronic Stroke Population: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Eur. Neurol. 2019, 81, 103–111. [Google Scholar] [CrossRef]
- Kendall, B.J.; Gothe, N.P. Effect of aerobic exercise interventions on mobility among stroke patients a systematic review. Am. J. Phys. Med. Rehabil. 2015, 95, 214–224. [Google Scholar] [CrossRef]
- Luo, L.; Zhu, S.; Shi, L.; Wang, P.; Li, M.; Yuan, S. High Intensity Exercise for Walking Competency in Individuals with Stroke: A Systematic Review and Meta-Analysis. J. Stroke Cerebrovasc. Dis. 2019, 28, 104414. [Google Scholar] [CrossRef] [PubMed]
- Wevers, L.; Van De Port, I.; Vermue, M.; Mead, G.; Kwakkel, G. Effects of task-oriented circuit class training on walking competency after stroke: A systematic review. Physiotherapy 2011, 97, eS1623–eS1624. [Google Scholar] [CrossRef] [Green Version]
- Silva, S.; Borges, L.R.; Santiago, L.; Lucena, L.; Lindquist, A.R.; Ribeiro, T. Motor imagery for gait rehabilitation after stroke. Cochrane Database Syst. Rev. 2020, 2020, CD013019. [Google Scholar] [CrossRef]
- French, B.; Thomas, L.; Leathley, M.; Sutton, C.; McAdam, J.; Forster, A.; Langhorne, P.; Price, C.; Walker, A.; Watkins, C. Does repetitive task training improve functional activity after stroke? A Cochrane systematic review and meta-analysis. J. Rehabil. Med. 2010, 42, 9–14. [Google Scholar] [CrossRef]
- Shu, Y.; Bi, M.M.; Zhou, T.T.; Liu, L.; Zhang, C. Effect of dual-task training on gait and balance in stroke patients: A updated meta-analysis. Am. J. Phys. Med. Rehabil. 2022. [Google Scholar] [CrossRef]
- Zhang, X.; Xu, F.; Shi, H.; Liu, R.; Wan, X. Effects of dual-task training on gait and balance in stroke patients: A meta-analysis. Clin. Rehabil. 2022, 36, 02692155221097033. [Google Scholar] [CrossRef] [PubMed]
- Schröder, J.; Truijen, S.; Van Criekinge, T.; Saeys, W. Feasibility and effectiveness of repetitive gait training early after stroke: A systematic review and meta-analysis. J. Rehabil. Med. 2019, 51, 78–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Q.; Yang, H.; Zhou, Q.; Pan, H. Effects of cognitive motor dual-task training on stroke patients: A RCT-based meta-analysis. J. Clin. Neurosci. 2021, 92, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Van De Port, I.G.L.; Wood-Dauphinee, S.; Lindeman, E.; Kwakkel, G. Effects of exercise training programs on walking competency after stroke: A systematic review. Am. J. Phys. Med. Rehabil. 2007, 86, 935–951. [Google Scholar] [CrossRef]
- Da Campo, L.; Hauck, M.; Marcolino, M.A.Z.; Pinheiro, D.; Plentz, R.D.M.; Cechetti, F. Effects of aerobic exercise using cycle ergometry on balance and functional capacity in post-stroke patients: A systematic review and meta-analysis of randomised clinical trials. Disabil. Rehabil. 2021, 43, 1558–1564. [Google Scholar] [CrossRef] [PubMed]
- Wist, S.; Clivaz, J.; Sattelmayer, M. Muscle strengthening for hemiparesis after stroke: A meta-analysis. Ann. Phys. Rehabil. Med. 2016, 59, 114–124. [Google Scholar] [CrossRef] [PubMed]
- Mehta, S.; Pereira, S.; Viana, R.; Mays, R.; McIntyre, A.; Janzen, S.; Teasell, R.W. Resistance training for gait speed and total distance walked during the chronic stage of stroke: A meta-analysis. Top. Stroke Rehabil. 2012, 19, 471–478. [Google Scholar] [CrossRef] [Green Version]
- Gelaw, A.Y.; Janakiraman, B.; Teshome, A.; Ravichandran, H. Effectiveness of treadmill assisted gait training in stroke survivors: A systematic review and meta-analysis. Glob. Epidemiol. 2019, 1, 100012. [Google Scholar] [CrossRef]
- Mehrholz, J.; Thomas, S.; Kugler, J.; Pohl, M.; Elsner, B. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst. Rev. 2020, 2020, CD006185. [Google Scholar] [CrossRef]
- Polese, J.C.; Ada, L.; Dean, C.M.; Nascimento, L.R.; Teixeira-Salmela, L.F. Treadmill training is effective for ambulatory adults with stroke: A systematic review. J. Physiother. 2013, 59, 73–80. [Google Scholar] [CrossRef] [Green Version]
- English, C.; Hillier, S.L.; Lynch, E.A. Circuit class therapy for improving mobility after stroke. Cochrane Database Syst. Rev. 2017, 2017, CD007513. [Google Scholar] [CrossRef]
- Lawrence, M.; Junior, F.T.C.; Matozinho, H.H.S.; Govan, L.; Booth, J.; Beecher, J. Yoga for stroke rehabilitation. Cochrane Database Syst. Rev. 2017, 2017, CD011483. [Google Scholar] [CrossRef] [Green Version]
- Anjos, J.M.; Neto, M.G.; dos Santos, F.S.; Almeida, K.D.O.; Bocchi, E.A.; Bitar, Y.D.S.L.; Duraes, A.R. The impact Of high-intensity interval training On functioning And health-related quality Of life In post-stroke patients: A systematic review with meta-analysis. Clin. Rehabil. 2022, 36, 726–739. [Google Scholar] [CrossRef] [PubMed]
- Ada, L.; Dean, C.; Vargas, J.; Ennis, S. Mechanically assisted walking with body weight support versus assisted overground walking in subacute non-ambulatory stroke: A systematic review. Physiotherapy 2011, 97, eS29. [Google Scholar]
- Bruni, M.F.; Melegari, C.; De Cola, M.C.; Bramanti, A.; Bramanti, P.; Calabrò, R.S. What does best evidence tell us about robotic gait rehabilitation in stroke patients: A systematic review and meta-analysis. J. Clin. Neurosci. 2018, 48, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, L.R.; Boening, A.; Galli, A.; Polese, J.C.; Ada, L. Treadmill walking improves walking speed and distance in ambulatory people after stroke and is not inferior to overground walking: A systematic review. J. Physiother. 2021, 67, 95–104. [Google Scholar] [CrossRef] [PubMed]
- French, B.; Thomas, L.H.; Coupe, J.; McMahon, N.E.; Connell, L.; Harrison, J.; Sutton, C.J.; Tishkovskaya, S.; Watkins, C.L. Repetitive task training for improving functional ability after stroke. Cochrane Database Syst. Rev. 2016, 2016, CD006073. [Google Scholar] [CrossRef] [Green Version]
- Leng, Y.; Zhang, M.; Li, Y. Effects of Pilates exercise on balance, walking and lower limbs motor function in stroke patients: A meta-analysis. Med. Data Min. 2019, 2, 110–117. [Google Scholar]
- Staples, A. Should Robotic Assisted Gait Training Be the New Standard of Care for Balance Treatment in Chronic Stroke? A Meta-Analysis. Ph.D. Thesis, California State University, Fresno, CA, USA, 2017. [Google Scholar]
- Chen, B.-L.; Guo, J.-B.; Liu, M.-S.; Li, X.; Zou, J.; Chen, X.; Zhang, L.-L.; Yue, Y.-S.; Wang, X.-Q. Effect of Traditional Chinese Exercise on Gait and Balance for Stroke: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0135932. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, Y.; Cui, C.; Liu, Y.; Lei, M.; Liu, T.; Meng, L.; Jin, C. The effect of Tai Chi exercise on motor function and sleep quality in patients with stroke: A meta-analysis. Int. J. Nurs. Sci. 2017, 4, 314–321. [Google Scholar] [CrossRef]
- Lyu, D.; Lyu, X.; Zhang, Y.; Ren, Y.; Yang, F.; Zhou, L.; Zou, Y.; Li, Z. Tai Chi for stroke rehabilitation: A systematic review and meta-analysis of randomized controlled trials. Front. Physiol. 2018, 9, 983. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.; Wu, X.; Liu, Z.; Wang, J.; Wang, K.; Yin, J.; Wang, X. The Influences of Tai Chi on Balance Function and Exercise Capacity among Stroke Patients: A Meta-Analysis. Evid.-Based Complement. Altern. Med. 2021, 2021, 6636847. [Google Scholar] [CrossRef] [PubMed]
- McGill, K.; Sackley, C.M.; Godwin, J.; McGarry, J.; Brady, M.C. A systematic review of the efficiency of recruitment to stroke rehabilitation randomised controlled trials. Trials 2020, 21, 68. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Situation | Description | Gait Speed | Balance Outcome |
|---|---|---|---|
| Potentially spurious evidence of effects | Cross CB but not MB, and fail to reach RIS | 17.9% (n = 5) | 16.7% (n = 3) |
| Firm evidence of effects | Cross CB and MB, but fail to reach RIS | 7.1% (n = 2) | 5.6% (n = 1) |
| Absence of evidence | Do not cross CB or MB, and fail to reach RIS | 42.9% (n = 12) | 33.3% (n = 6) |
| Lack of effect | Do not cross CB or MB, but reach RIS | 0% | 0% |
| Verified intervention effects | Cross CB and MB, and reach RIS | 32.1% (n = 9) | 44.4% (n = 8) |
| Group | Review | Interventions | Outcome Measure | No. of Trials (Patients) | Required Information Size | Z-Score (MB) | Additional Information Size Needed |
|---|---|---|---|---|---|---|---|
| 1 | M. Y. Pang et al., 2006 [22] | aerobic exercise | gait speed | 5 (346) | 551 | −2.28 (−2.29) | 205 |
| 1 | B. J. Kendall et al., 2015 [53] | aerobic exercise | 6MWT | 8 (423) | 804 | −2.03 (−2.89) | 381 |
| 1 | L. Luo et al., 2019 [54] | high-intensity exercise | gait speed | 11 (345) | 604 | −2.02 (−2.82) | 259 |
| 3 | L. Wevers et al., 2011 [55] | circuit class training | gait speed | 4 (214) | 335 | −2.35 (−2.59) | 121 |
| 3 | S. Silva et al., 2020 [56] | task-oriented exercise | gait speed | 6 (191) | 346 | −2.01 (−2.84) | 155 |
| Group | Review | Interventions | Outcome Measure | No of Trials (Patients) | Required Information Size | Z-Score (MB) | Additional Information Size Needed |
|---|---|---|---|---|---|---|---|
| 3 | B. French et al., 2010 [57] | repetitive task training | balance (BBS) | 9 (504) | 925 | −2.05 (−2.89) | 421 |
| 3 | Y. Shu et al., 2022 [58] | dual-task training | balance (BBS) | 7 (219) | 438 | −1.98 (−3.01) | 219 |
| 3 | X. Zhang et al., 2022 [59] | dual-task training | balance (BBS) | 6 (194) | 369 | −2.03 (−2.9) | 175 |
| Group | Review | Interventions | Outcome Measure | No. of Trials (Patients) | Required Information Size | Z-Score (MB) | Additional Information Size Needed |
|---|---|---|---|---|---|---|---|
| 3 | J. Schröder et al., 2019 [60] | repetitive gait training | gait speed | 8 (572) | 762 | −2.39 (−2.39) | 190 |
| 3 | A. C. Bonini-Rocha et al., 2018 [23] | circuit-based exercises (CBEs) | change in gait speed | 7 (516) | 623 | −2.43 (−2.29) | 107 |
| Group | Review | Interventions | Outcome Measure | No. of Trials (Patients) | Required Information Size | Z-Score (MB) | Additional Information Size Needed |
|---|---|---|---|---|---|---|---|
| 3 | Q. Zhou et al., 2021 [61] | cognitive motor dual-task training | change in balance (BBS) | 5 (110) | 132 | −2.56 (−2.23) | 22 |
| Group | Review | Interventions | Outcome Measure | No of Trials (Patients) | Required Information Size | Z-Score (MB) | Additional Information Size Needed |
|---|---|---|---|---|---|---|---|
| 1 | I. G. L. Van De Port et al., 2007 [62] | cardiorespiratory fitness training | gait speed | 2 (102) | 262 | −1.74 (−3.44) | 160 |
| 1 | D. Pogrebnoy et al., 2019 [24] | exercise programmes (aerobic + resistance) | gait speed | 5 (248) | 728 | −1.66 (−3.7) | 480 |
| 1 | L. Da Campo et al., 2021 [63] | aerobic exercise (cycle ergometry) | 6MWT | 3 (188) | 1992 | 0.87 (−8.0) | 1804 |
| 1 | S. Wist et al., 2016 [64] | muscle strengthening | 6MWT | 6 (265) | 1808 | −1.07 (−8.0) | 1543 |
| 1 | S. Mehta et al., 2012 [65] | resistance training | 6MWT | 8 (331) | 748 | −1.86 (−3.2) | 417 |
| 2 | J. Mehrholz et al., 2017 [27] | machine-assist (dependent at baseline) | 6MWT | 5 (639) | 6016 | 0.91 (8.0) | 5377 |
| 2 | A. Y. Gelaw et al., 2019 [66] | treadmill assisted gait training | gait speed | 8 (695) | 7790 | 0.81 (−8.0) | 7095 |
| 2 | J. Mehrholz et al., 2020 [67] | machine-assist | 6MWT | 24 (1136) | 8346 | −0.99 (−8.0) | 7300 |
| 3 | J. C. Polese et al., 2013 [68] | treadmill | 6MWT | 6 (287) | 936 | −1.55 (−3.89) | 649 |
| 3 | C. English et al., 2017 [69] | circuit class therapy | gait speed | 2 (437) | 2567 | −1.17 (−5.36) | 2130 |
| 3 | X. Zhang et al., 2022 [59] | dual-task training | gait speed | 8 (225) | 1328 | −1.15 (−8.0) | 1103 |
| Group | Review | Interventions | Outcome Measure | No of Trials (Patients) | Required Information Size | Z-Score (MB) | Additional Information Size Needed |
|---|---|---|---|---|---|---|---|
| 1 | L. Da Campo et al., 2021 [63] | aerobic exercise (cycle ergometry) | change in balance (BBS) | 3 (195) | 513 | −1.78 (−3.48) | 318 |
| 2 | A. Y. Gelaw et al., 2019 [66] | treadmill assisted gait training | balance (BBS) | 2 (456) | 8913 | 0.64 (−8.0) | 8497 |
| 3 | L. Wevers et al., 2011 [55] | circuit class training | balance (BBS) | 2 (154) | 1788 | 0.82 (−8.0) | 1634 |
| 3 | C. English et al., 2017 [69] | task-oriented exercise | balance (BBS) | 4 (171) | 801 | −1.3 (−4.75) | 630 |
| 3 | A. C. Bonini-Rocha et al., 2018 [23] | circuit-based exercises | change in balance (BBS) | 3 (174) | 2689 | 0.71 (−8.0) | 2515 |
| 4 | M. Lawrence et al., 2017 [70] | theory-based exercise | balance (BBS) | 2 (69) | 358 | 1.23 (5.01) | 289 |
| Group | Review | Interventions | Outcome Measure | No. of Trials (Patients) | Required Information Size | Z-Score (MB) | Additional Information Size Needed |
|---|---|---|---|---|---|---|---|
| 1 | D. H. Saunders et al., 2020 [21] | aerobic exercise | 6MWT | 7 (225) | 216 | −2.86 (−1.96) | N/A |
| 1 | J. M. Anjos et al., 2022 [71] | high-intensity interval training | change in gait speed | 4 (100) | 72 | −2.87 (−1.96) | N/A |
| 2 | L. Ada et al., 2011 [72] | machine-assist | gait speed | 4 (258) | 117 | −4.2 (−1.96) | N/A |
| 2 | J. Mehrholz et al., 2017 [27] | machine-assist (independent at baseline) | 6MWT | 10 (423) | 423 | −2.81 (−1.96) | N/A |
| 2 | M. F. Bruni et al., 2018 [73] | end-effector device | gait speed | 7 (469) | 441 | −2.79 (−1.96) | N/A |
| 2 | L. R. Nascimento et al., 2021 [74] | treadmill assist walking | gait speed | 6 (266) | 88 | −4.78 (−1.96) | N/A |
| 3 | B. French et al., 2016 [75] | repetitive task training | gait speed | 12 (685) | 606 | −2.93 (−1.96) | N/A |
| 3 | Q. Zhou et al., 2021 [61] | cognitive motor dual-task training | change in gait speed | 5 (119) | 107 | −3.02 (−1.96) | N/A |
| 4 | Y. Leng et al., 2019 [76] | Pilates exercise | gait speed | 2 (80) | 65 | −3.13 (−1.96) | N/A |
| Group | Review | Interventions | Outcome Measure | No. of Trials (Patients) | Required Information Size | Z-Score (MB) | Additional Information Size Needed |
|---|---|---|---|---|---|---|---|
| 1 | J. M. Anjos et al., 2022 [71] | high-intensity interval training | change in balance (BBS) | 2 (64) | 60 | −2.93 (−1.96) | N/A |
| 2 | A. Staples et al., 2017 [77] | robotic-assisted gait training | balance (BBS) | 4 (108) | 69 | −3.51 (−1.96) | N/A |
| 4 | B.-L. Chen et al., 2015 [78] | traditional Chinese exercise | balance (BBS) | 6 (529) | 379 | −3.61 (−1.96) | N/A |
| 4 | L. Qin et al., 2016 [25] | tai chi exercise | balance (BBS) | 9 (558) | 243 | −4.65 (−1.96) | N/A |
| 4 | Y. Li et al., 2017 [79] | tai chi exercise | balance (BBS) | 9 (670) | 152 | −6.42 (−1.96) | N/A |
| 4 | D. Lyu et al., 2018 [80] | tai chi exercise | balance (BBS) | 7 (328) | 248 | −3.23 (−1.96) | N/A |
| 4 | Y. Leng et al., 2019 [76] | Pilates exercise | balance (BBS) | 3 (142) | 89 | −3.59 (−1.96) | N/A |
| 4 | X. Zheng et al., 2021 [81] | tai chi exercise | balance (BBS) | 5 (376) | 196 | −3.53 (−1.96) | N/A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, J.-Q.; Sun, Y.-W.; So, W.-S.; Sidarta, A.; Kwong, P.W.-H. A Comprehensive Appraisal of Meta-Analyses of Exercise-Based Stroke Rehabilitation with Trial Sequential Analysis. Healthcare 2022, 10, 1984. https://doi.org/10.3390/healthcare10101984
Li J-Q, Sun Y-W, So W-S, Sidarta A, Kwong PW-H. A Comprehensive Appraisal of Meta-Analyses of Exercise-Based Stroke Rehabilitation with Trial Sequential Analysis. Healthcare. 2022; 10(10):1984. https://doi.org/10.3390/healthcare10101984
Chicago/Turabian StyleLi, Jia-Qi, Yu-Wei Sun, Wing-Sam So, Ananda Sidarta, and Patrick Wai-Hang Kwong. 2022. "A Comprehensive Appraisal of Meta-Analyses of Exercise-Based Stroke Rehabilitation with Trial Sequential Analysis" Healthcare 10, no. 10: 1984. https://doi.org/10.3390/healthcare10101984
APA StyleLi, J.-Q., Sun, Y.-W., So, W.-S., Sidarta, A., & Kwong, P. W.-H. (2022). A Comprehensive Appraisal of Meta-Analyses of Exercise-Based Stroke Rehabilitation with Trial Sequential Analysis. Healthcare, 10(10), 1984. https://doi.org/10.3390/healthcare10101984