1. Introduction
The burden of breast cancer is high with a colossal effect on lives, families and communities. The disease has been a leading cause of death among women globally. The World Health Organisation has estimated that 2.3 million women have been infected globally, and there is a 650,000 mortality rate [
1]. Though incidence in the African region was lower than in other continents except for Asia, its age-standardised mortality rate has been ranked the highest worldwide, with Nigeria having the highest mortality rate [
2].
Although studies on the degree of knowledge and awareness of breast cancer in the late 1980s and early 1990s found that most women are unaware of the condition, particularly its risk factors and treatment options [
3], recent studies have revealed a rise in breast cancer awareness behavioural practices, particularly among women in more industrialised cultures [
4]. The same cannot be accurate for women in developing nations, particularly those in Africa’s Sub-Saharan area, where behavioural practices towards breast cancer screening are still poor [
5].
For instance, studies have revealed that most Nigerian women in rural and urban regions have little or no understanding of the disease’s risk factors, symptoms and good behavioural practices [
6,
7]. Such a behavioural practice gap has been associated with health communication and literacy.
In the field of health communication, information sources are important for health promotion and education. Scholars say that information sources are important for raising public health awareness because they are the basis for health communication activities [
8,
9]. Personal and community health improvement attitudes and knowledge are positively influenced by information sources. Making well-informed decisions, therefore, requires effective health communication.
The importance of information acquisition in health behaviour promotion has been highlighted in studies on health communication [
5]. The fact that breast cancer is a non-infectious invasive disease has increased the demand for communication-based treatments since a poor understanding of the disease can have various negative consequences, such as the spread of fear and the rejection of behavioural interventions [
5,
7]. As a result, the spread of breast cancer screening information is crucial to breast self-examination. Previous screening research has found that various sources of health information have both affirmative and negative effects on screening habits [
10]. Ascertaining the most valuable sources of information for raising women’s desire to engage in breast self-examination is critical to the success of breast cancer screening and behavioural interventions.
Existing research, particularly for communication on health, has shown that communication elements may not directly impact the public [
11,
12]. However, much health behaviour management research has concentrated on the indirect pathways via which communication features influence public behaviour. Scholars have underlined the need to determine indirect paths through psychological difficulties. As a result, this research aims to explore how women’s acquisition of breast cancer information from various sources influences their health beliefs and behavioural practice intentions via psychological factors.
The health belief model is one of the most often used models for studying the factors of people’s intentions to adopt a behavioural practice [
6,
7]. It focuses on psychological aspects such as vulnerability, severity barriers, cues to action, benefits and self-efficacy. However, few researchers have examined the elements influencing one’s health attitudes. This study aimed to fill that gap by investigating women’s health communication and behaviour towards breast cancer screening in Lagos, Nigeria. The HBM was used as the theoretical foundation for this research to improve women’s health communication and behaviour towards breast cancer screening in Lagos, Nigeria. The choice of Lagos is predicated on a 2009–2016 report of Nigeria National System of Cancer Registries which ranks Lagos as the second state with the most prevalent cases of breast cancer among women in Nigeria. The analysis will be guided by the following formulated hypotheses:
H1. There is a significant relationship between information sources and women’s perceived susceptibility to breast cancer and adherence to breast self-examination.
H2. There is a significant relationship between information sources and women’s perceived severity of breast cancer and adoption of (breast cancer) breast self-examination.
H3. There is a significant relationship between information sources and the perceived barrier of women towards breast self-examination.
3. Results
The demographic profile of the respondents is depicted in
Table 1. The findings show that 52.5% of the total respondents were within the ages of 20 and 29 years, while 23.3% were within the age group of 30 and 39 years. Similarly, 14.8% were within the age bracket of 40 and 49 years, 7.3% were between the ages of 50 and 59 years, while 2.3% were 60 years and above. In addition, the respondents’ marital status was revealed. The result shows that 48.8% of the total respondents were single, 47.0% were married, 1.8% were divorced and 2.5% of the study population were widows. This indicates that women, whether single or married, comprise most of the population, accounting for 95.8% of the total.
Similarly, the researchers examined the educational status of the 400 respondents, discovering that only 3.8% had no formal education, 3.3% were students, 21.0% of the study population were secondary school graduates and 72.1% were tertiary institution graduates. The bulk of the respondents, however, had finished tertiary education. This suggests that most of the respondents were educated, and their information may be trusted.
In addition, 30.5% of the 400 total respondents were students, 12.3% were artisan/handwork, 24.8% were businesswomen and the remaining 32.5% were employed. Most respondents were employed. Meanwhile, 286 respondents, representing 71.5%, identified themselves as Christians, whereas 101 respondents, representing 25.3%, identified themselves as Muslims. Traditional accounted for 2.5% of the respondents, while other religions accounted for 30.8%. Most of the respondents were Christian, accounting for 71.5% of the study population.
H1. There is a significant relationship between information sources and women’s perceived susceptibility to breast cancer and adherence to breast self-examination.
Hypothesis one tested the relationship between information sources and women’s perceived susceptibility to breast cancer and adherence to breast self-examination. Path coefficients, t-statistics, R-square values and
p-values were used to interpret the results. The path coefficient, as shown in
Figure 1, determines the degree and strength of the correlation between the observed variables. The R-square, on the other hand, determined the amount of variance in the women’s perceived susceptibility to breast cancer and adherence to breast self-examination, as indicated by the information sources. As shown in
Table 2, the
p-value denotes the degree of probability that must be less than 0.05 to be considered significant, whereas the t-statistics denote the measured differences in standard error units.
Figure 1 shows the PLS algorithm model of information sources and women’s perceived susceptibility to breast cancer with the loading values of each item of measurement for both information sources (television, radio, newspaper, friends/family, Internet, and health workers) and women’s perceived susceptibility to breast cancer.
Figure 1 also depicts the PLS Bootstrapping Model with β and P-coefficients of the value of both variables. The
p-value determines the amount of probability.
Table 2 shows the factor loadings of all the measurement items for information sources and perceived susceptibility to breast cancer. Composite reliability, average variance extracted (AVE) computation and Cronbach Alpha were used to assess the instrument’s validity and reliability. Meanwhile, the factor loading, composite reliability, AVE and Cronbach Alpha criteria were met. Convergent and discriminant validity were also considered in the study when determining construct validity. Convergent validity is evidence of a link between information sources and perceived susceptibility to breast cancer.
The discriminant validity of information sources and perceived susceptibility to breast cancer is depicted in
Table 3. The heterotrait–monotrait (HTMT) ratio of correlations method was used to assess the discriminant validity. The analysis results show that all the values are less than the HTMT 0.85 critical value. These things considered, the average heterotrait–heteromethod correlation is lower than the average monotrait–heteromethod correlation. As a result, the discriminant validity is established. Similarly, the common method bias was tested via VIF, as depicted in
Table 2. The results obtained were within the recommended threshold of 3.3.
Table 4 shows the model fit for information sources and perceived susceptibility to breast cancer. All the model fit indicators were found to be acceptable. The standardised residual average between the observed matrix and the hypothesised covariance matrices is represented by SRMR. The result of SRMR is less than the 0.08 threshold point; therefore, the SRMR value of 0.071 is considered reliable, indicating a good fit.
To determine the PLS-SEM predictive relevance of the measurement constructs and the data points of indicators, the Q
2 values were used. The Q
2 value is 0.390, which is larger than zero. This suggests that the PLS path model has predictive relevance for the constructs. The F-square was used to determine the effect size in the same vein. The F-square is 2.117, as indicated in
Table 5. This implies that the sample effect is considered large.
Table 5 depicts the smart partial least squared statistical results of hypothesis one, which focused on the relationship between information sources and perceived susceptibility to breast cancer. Generally, the findings show that information sources have a significant effect on perceived susceptibility to breast self-examination at (β = 0.803, R
2 = 0.644, t-statistics = 12.763 > 1.96,
p-value =0.000 < 0.05). The Path coefficient of 0.803 implied a high degree of relationship between information sources and perceived susceptibility to breast cancer. The R
2 value of 0.644 indicates that information sources can explain a 64.4% variance in women’s perceived susceptibility to breast cancer.
Specifically, out of the six information sources considered in this study, it was discovered that the Internet has the most predictive value at the standardised coefficient value of 0.465, followed closely by health workers in the prediction of perceived susceptibility to breast cancer. However, television, radio, newspaper and friends/family do not contribute significantly to the model.
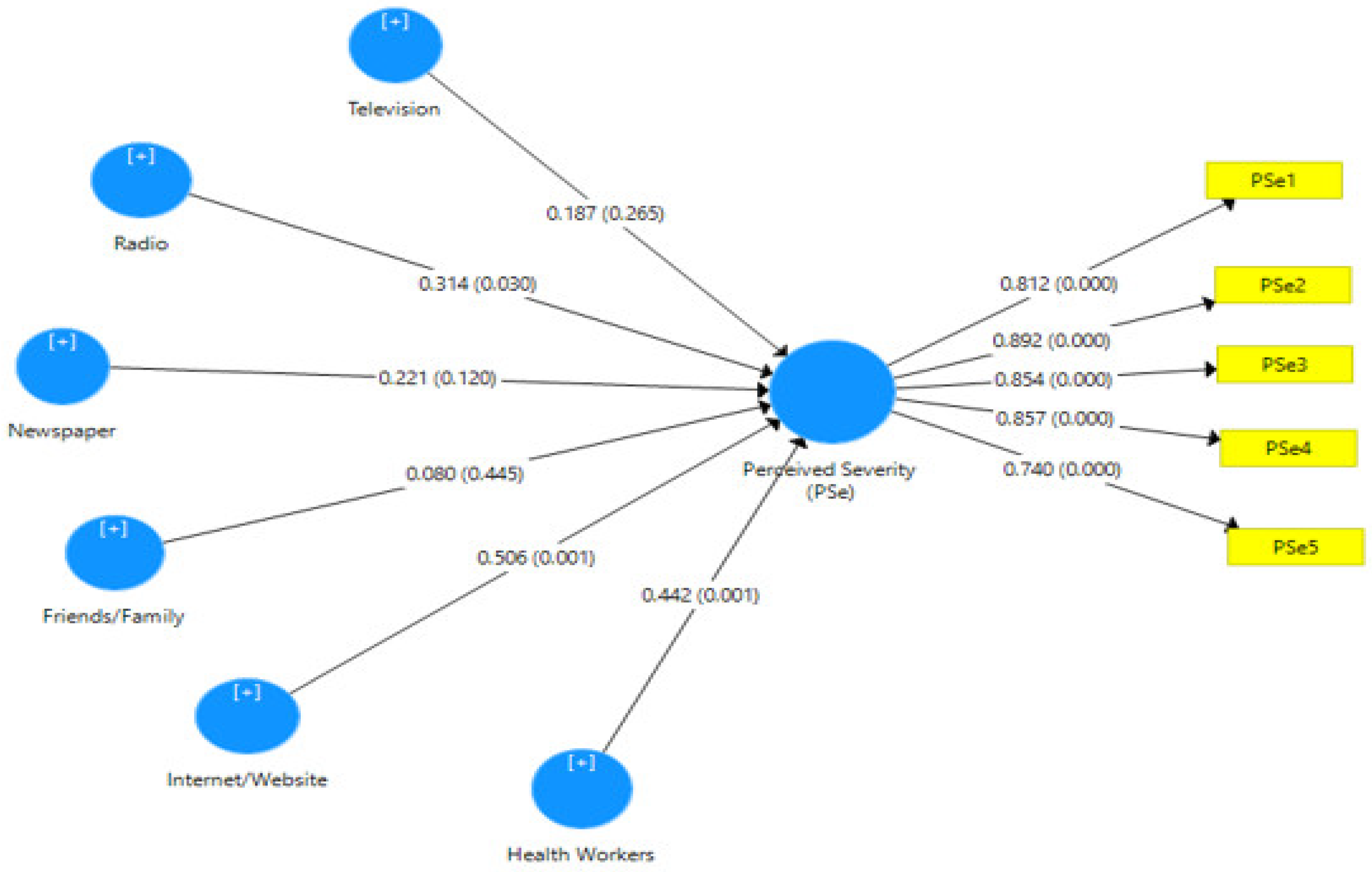
H2. There is a significant relationship between information sources and women’s perceived severity of breast cancer and adoption of (breast cancer) breast self-examination.
Hypothesis two tested the relationship between information sources and women’s perceived severity of breast cancer and adherence to breast self-examination. Path coefficients, t-statistics, R-square values and
p-values were used to interpret the results. As shown in
Figure 2, the path coefficient determines the degree and strength of the correlation between the observed variables. The R-square, on the other hand, determines the amount of variance in the women’s perceived severity of breast cancer and adoption of (breast cancer) breast self-examination, as indicated by the information sources. As shown in
Table 6, the
p-value denotes the degree of probability that must be less than 0.05 to be considered significant.
Figure 2 shows the PLS algorithm model of information sources and women’s perceived severity of breast cancer with the loading values of each item of measurement for both information sources (television, radio, newspaper, friends/family, Internet and health workers) and women’s perceived severity to breast cancer.
Figure 2 also depicts the PLS Bootstrapping Model with β and P-coefficients of the value of both variables. The
p-value determines the amount of probability.
Table 6 shows the factor loadings of all the measurement items for the perceived severity of breast cancer. Composite reliability, average variance extracted (AVE) computation and Cronbach Alpha were used to assess the instrument’s validity and reliability. Meanwhile, the factor loading, composite reliability, AVE and Cronbach Alpha criteria were met. Convergent and discriminant validity were also taken into account in the study when determining construct validity. Convergent validity is evidence of a link between information sources and the perceived severity of breast cancer examination.
The discriminant validity of information sources and perceived severity of breast cancer examination is depicted in
Table 7. The heterotrait–monotrait (HTMT) ratio of correlations method was used to assess the discriminant validity. The analysis results show that all the values are less than the HTMT 0.85 critical value. These things considered, the average heterotrait–heteromethod correlation is lower than the average monotrait–heteromethod correlation. As a result, the discriminant validity is established. Similarly, the common method bias was tested via VIF, as depicted in
Table 6. The results obtained were within the recommended threshold of 3.3. This can be concluded that the model is free from common method bias.
Table 8 displays the model fit for information sources and the perceived severity of breast cancer. All the model fit indicators were found to be acceptable. The standardised residual average between the observed matrix and the hypothesised covariance matrices is represented by SRMR. The result of SRMR is less than the 0.08 threshold point; therefore, the SRMR value of 0.069 is considered reliable, indicating a good fit.
To determine the PLS-SEM predictive relevance of the constructs of measurement and the data points of indicators, the Q
2 values were used. The Q
2 value is 0.329, which is larger than zero. This suggests that the PLS path model has predictive relevance for the constructs. In the same vein, the F-square was used to determine the effect size. The F-square is 2.210, as indicated in
Table 9. This implies that the sample effect is considered large.
Table 9 depicts the smart partial least squared statistical results of hypothesis two, which focused on the relationship between information sources and the perceived severity of breast cancer. Generally, the findings show that information sources have a significant effect on perceived susceptibility to breast cancer at (β = 0.743, R
2 = 0.553, t-statistics = 2.662 > 1.96,
p-value = 0.000 < 0.05). The path coefficient of 0.743 implies a high degree of relationship between information sources and the perceived severity of breast cancer. The R
2 value of 0.553 indicates that information sources can explain a 55.5% variance in women’s perceived severity of breast cancer.
Specifically, out of the six information sources considered in this study, it was discovered that the Internet has the most predictive value at the standardised coefficient value of 0.506, followed closely by health workers and radio information sources at 0.422 and 0.316, respectively, in the prediction of perceived severity to breast cancer. However, television, newspapers and friends/family do not contribute significantly to the model.
H3. There is a significant relationship between information sources and the perceived barrier of women towards breast self-examination.
Hypothesis three tested the relationship between information sources and the perceived barrier of women towards breast self-examination. Path coefficients, t-statistics, R-square values and
p-values were used to interpret the results. The path coefficient, as shown in
Figure 3, determines the degree and strength of the correlation between the observed variables. The R-square, on the other hand, determines the amount of variance in the perceived barrier of women towards breast self-examination, as indicated by the information sources. As shown in
Table 10, the
p-value denotes the degree of probability that must be less than 0.05 to be considered significant.
Figure 3 shows the PLS algorithm model of information sources and perceived barriers of women towards breast self-examination with the loading values of each item of measurement for both information sources (television, radio, newspaper, friends/family, Internet and health workers) and perceived barrier of women towards breast self-examination.
Figure 3 also depicts the PLS Bootstrapping Model with β and P-coefficients of the value of both variables. The
p-value determines the amount of probability.
Table 10 displays the factor loadings of all the measurement items for the perceived barrier of women towards breast self-examination. Composite reliability, average variance extracted (AVE) computation and Cronbach Alpha were used to assess the instrument’s validity and reliability. Meanwhile, the factor loading, composite reliability, AVE and Cronbach Alpha criteria were met. Convergent and discriminant validity were also taken into account in the study when determining construct validity. Convergent validity is evidence of a link between information sources and the perceived barrier of women towards breast self-examination.
The discriminant validity of information sources and perceived barrier of women towards breast self-examination is depicted in
Table 11. The heterotrait–monotrait (HTMT) ratio of correlations method was used to assess the discriminant validity. The results of the analysis show that all the values are less than the HTMT 0.85 critical value. These things considered, the average heterotrait–heteromethod correlation is lower than the average monotrait–heteromethod correlation. As a result, the discriminant validity is established. Similarly, the common method bias was tested via VIF, as depicted in
Table 10. The results obtained were within the recommended threshold of 3.3. This can be concluded that the model is free from common method bias.
Table 12 displays the model fit for information sources and the perceived barrier of women towards breast self-examination. All the model fit indicators were found to be acceptable. The standardised residual average between the observed matrix and the hypothesised covariance matrices is represented by SRMR. The result of SRMR is less than the 0.08 threshold point; therefore, the SRMR value of 0.079 is considered reliable, indicating a good fit.
Additionally, to determine the PLS-SEM predictive relevance of the constructs of measurement and the data points of indicators, the Q
2 values were used. The Q
2 value is 0.497, which is larger than zero. This suggests that the PLS path model has predictive relevance for the constructs. In the same vein, the F-square was used to determine the effect size. The F-square is 3.110, as indicated in
Table 13. This implies that the sample effect is considered large.
Table 13 depicts the smart partial least squared statistical results of hypothesis three, which focused on the relationship between information sources and the perceived barrier of women towards breast self-examination. Generally, the findings show that information sources have a significant effect on perceived susceptibility to breast cancer at (β = 0.764, R
2 = 0.583, t-statistics = 11.523 > 1.96,
p-value = 0.000 < 0.05). The path coefficient of 0.764 implies a high degree of relationship between information sources and the perceived barrier of women towards breast self-examination. The R
2 value of 0.583 indicates that information sources can explain a 58.3% variance in the perceived barrier of women towards breast self-examination.
Specifically, out of the six information sources considered in this study, it was discovered that friends and family have the most predictive value at the standardised coefficient value of 0.739, followed closely by Internet and health workers’ information sources at 0.296 and 0.266, respectively, in the prediction of the perceived barrier of women towards breast self-examination. However, television, newspapers and radio do not contribute significantly to the model.
4. Discussion
Although previous studies concerning perceived susceptibility of breast self-examination globally and in Nigeria have majorly centered on a health context, ignoring the role played by the information sources by Abhang and Lopez [
26], few others have examined information sources in relationship to women’s perceived susceptibility to breast cancer.
The test of hypothesis one focused on the possibility of information sources (television, radio, newspaper, family/friends, Internet and health workers) significantly affecting women’s perceived susceptibility to breast cancer and adherence to breast self-examination. The concepts of information sources and perceived susceptibility have long been a subject of research among scholars [
27,
28]. Out of all the information sources examined in this study, only the Internet/websites and health workers significantly influenced women’s perceived susceptibility to breast cancer. Additionally, the coefficient table, model fit, discriminant validity and construct validity and reliability indicated that information sources used to access woman’s perceived susceptibility towards adherence to BSE, which are: the Internet and health workers, all have a significant effect on how women believe in being diagnosed with breast cancer. This could be attributed to the need for these information sources by Lagos women to access a wide variety of information relating to adherence to breast self-examination. The Internet’s significance can be because of younger women relying more on the Internet for information sources, as they are Internet- and tech-savvy [
29]. In addition, there is an increased use of smartphones with Internet access capabilities of health information sources due to easy access and everyday use, which has resulted in a high degree of human beings’ believability [
30].
This result is similar to earlier research by Jackson et al. [
31]; Ayandipo et al. [
32] that identified health workers as the primary sources of health information among cancer patients. This conclusion also corroborates the findings of a systematic review and empirical research on information sources among cancer patients, which indicated that health professionals were the most often used source of information [
33,
34].
Since healthcare professionals play significant roles in the lives of women with breast cancer, it is not surprising that they were the primary source of information. However, some studies revealed that personal communication with some healthcare professionals revealed that breast cancer patients are primarily given verbal information because most have low literacy levels [
35,
36].
The perceived susceptibility is a significant determinant and foundation for attitudinal change [
37,
38]. In a study carried out by Masoumi [
39] to find out if perceived susceptibility mediates attitudinal change and behaviour, it was discovered that susceptibility is predicated on a significant perception of the risk of acquiring an illness or disease. Information sources on the Internet and from health workers invariably influence women’s susceptibility level and engender attitudinal change towards BSE.
Hypothesis two tested if there is a significant relationship between information sources and the perceived barrier of women towards breast self-examination. While many respondents reported hearing about breast cancer from traditional sources such as radio, television and newspapers, as well as interpersonal sources such as health professionals, friends and family, most respondents cited the family as their source.
Because it is human nature for people to confide in their closest circle about such delicate/sensitive material, family and friends could be viewed as having a significant impact on their attitudes. Since respondents believe that friends may provide various services, including material and emotional support, they are a good source of aid and a booster for women’s attitudes about learning more about the disease. However, Alberti et al. [
40] stress that health literacy may influence the effectiveness of family health communication. Inadequate health literacy could inevitably result in information distortion via this channel.
The Internet/websites, on the other hand, have had a significant impact on women’s views around breast cancer because it has increased their awareness, competence and participation in health decision making. Additionally, independent Internet inquiries can supplement and synergize often time-constrained doctor–patient interactions in the clinic [
41]. The Internet has been identified as a vital source of health information [
42]. Due to its similarities to traditional media in its ability to reach a broad audience, the Internet may economically and geographically reach a wide populace. Facebook, Instagram, Twitter, WhatsApp and Snapchat are typically employed for this purpose. According to Isa Ali Ibrahim, Nigeria’s Minister of Communication, 75% of Nigerians with Internet access use social media [
43].
These findings indicate that Internet users generally view cancer-related material as valuable and that the majority addressed Internet-derived information with their healthcare providers and thought that clinicians listened to such information. Nevertheless, some of these respondents exhibited skepticism regarding the dependability of Internet-based medical information. Not only did the Internet/website encourage respondents to seek health information quickly, but it also encouraged distrust in their thinking. Not to mention a sensitive aspect of people’s lives—their health—the trustworthiness and veracity of online information have frequently been questioned. This has altered their views towards examining the information they obtain on the Internet and cross-checking it with other sources, such as family/friends, health professionals, etc.
Even though interpersonal communication approaches to breast cancer communication take longer and can only reach a limited number of people compared to mainstream media, some of the respondents in this study have accessed enough information on breast self-examination through interpersonal communication channels. The study reveals that healthcare professionals are considered the source of knowledge among other interpersonal communication channels.



 ,
, 


{kind=link}
{kind=link}
{kind=link}