1. Introduction
Falls are indicators of feebleness, immovability, and severe chronic injury in elderly people. Fall risks reduce normal tasks by producing injury and movement limitations. Most injuries in the elderly are caused by falls that can produce hip fractures and forearm injuries [
1,
2,
3].
The prediction of fall risks must consider the range of ages and fitness status within the elderly patients and report the variety of reasons for falls. Fall risk factors are listed in controlled studies, which agree to the detection of patients at risk. Older people with several health deficiencies are at the highest risk [
4,
5,
6].
A fall is defined as an unintentional occasion that leads the patient to rest on a ground level. Falls are designated in three stages, as follows [
7]:
An introducing event that relocates the patient’s center of mass away from its base of support which can be caused by environmental hazards or unstable joint weakness.
The second stage of a fall is the inability of the patient to sustain an upright posture to perceive this movement in time to evade a fall due to loss of sensory function.
The third stage is the effect of the patient’s body on solid surfaces, which yields to the conduction of forces to the patients’ organs. The prospective for damage is a function of the magnitude and direction of the fall forces.
Research is moving towards automation, deep learning (DL), and artificial intelligence. Dynamic monitoring networks speed up the stream of health-related risk information [
1,
2,
3]. These developments convey convenience to high-risk situations and reveal concealed dangers to hospitalized elderly patients. Thus, protecting people’s lives from violation or violence incidents is a life-risking challenge and is a needed research track for monitoring research. There are numerous health-related risks to personal lives and hospitals everywhere. In [
2], the authors studied three metallic materials, and their applications in metal-on-metal bearing for hip implants in terms of contact pressure. The authors employed finite element simulation for predicting contact pressure under normal walking conditions. Recently, both the health-related risk techniques and the count of monitoring health-related risks have grown radically. This carries random risks to the safety and stable process of many premises such as hospitals and hospices. Thus, effective tools to identify various monitoring risks and to combat these risks are immediately required. An automated monitoring system (ASS) can identify health-related risk incidences and prevent them.
Many researchers have utilized deep learning models for the monotonous prediction of unusual monitoring movements for hospitalized elderly patients [
1]. Many monitoring systems employ deep learning models, especially in the image recognition paradigm [
2,
3], and motion analysis [
3,
4,
5]. Machine learning techniques usually have high prediction performance, such as DNN recurrent neural network (RNN) and Catboost [
6]. However, the prediction accuracy has room for improvement. Deep learning techniques are performed by using neurons to extract hidden monitoring features. However, techniques such as deep learning [
5,
6,
7,
8,
9] take a long time to train the system. Thus, a single deep learning technique will not encounter the real-time requirements of the monitoring systems in the new generation.
There are several hybrid monitoring prediction models that unite several deep learning techniques such as support vector deeps (SVM) and C-means [
10,
11,
12,
13], SVM based on naive Bayes, LDBoost [
11,
12], and support vector deep with recurrent C-means clustering [
3]. Also, there are mixtures of several deep learning techniques such as Vinaya-kumar and its equivalents [
12,
13,
14]. The authors in [
15] utilized RNN and SVM models to extract spatial and temporal features. The authors in [
16] presented a recurrent DNN system to detect the semantic features of monitoring settings. Other unions of deep learning techniques and neural techniques. For instance, the authors in [
17] presented a deep learning model with a hidden belief technique to extract features and RNN for classification. The authors in [
18] utilized a stacked encoder-decoder model for feature selection and then utilized random forests for classification. The authors in [
19] presented a deep learning fusion classification model.
Distributed intelligent learning techniques and deep techniques are presented by many researchers [
19,
20,
21,
22]. Such systems train high-dimensionality input rapidly and effectively so they can be utilized to train the enormous size of data in the training phase of the two phase prediction monitoring systems. Multi-risk prediction phase of monitoring systems, deep neural techniques can extract hidden features and extract unpreceded health-related risks with high performance. An investigation of monitoring prediction is proposed in [
19]. The authors in [
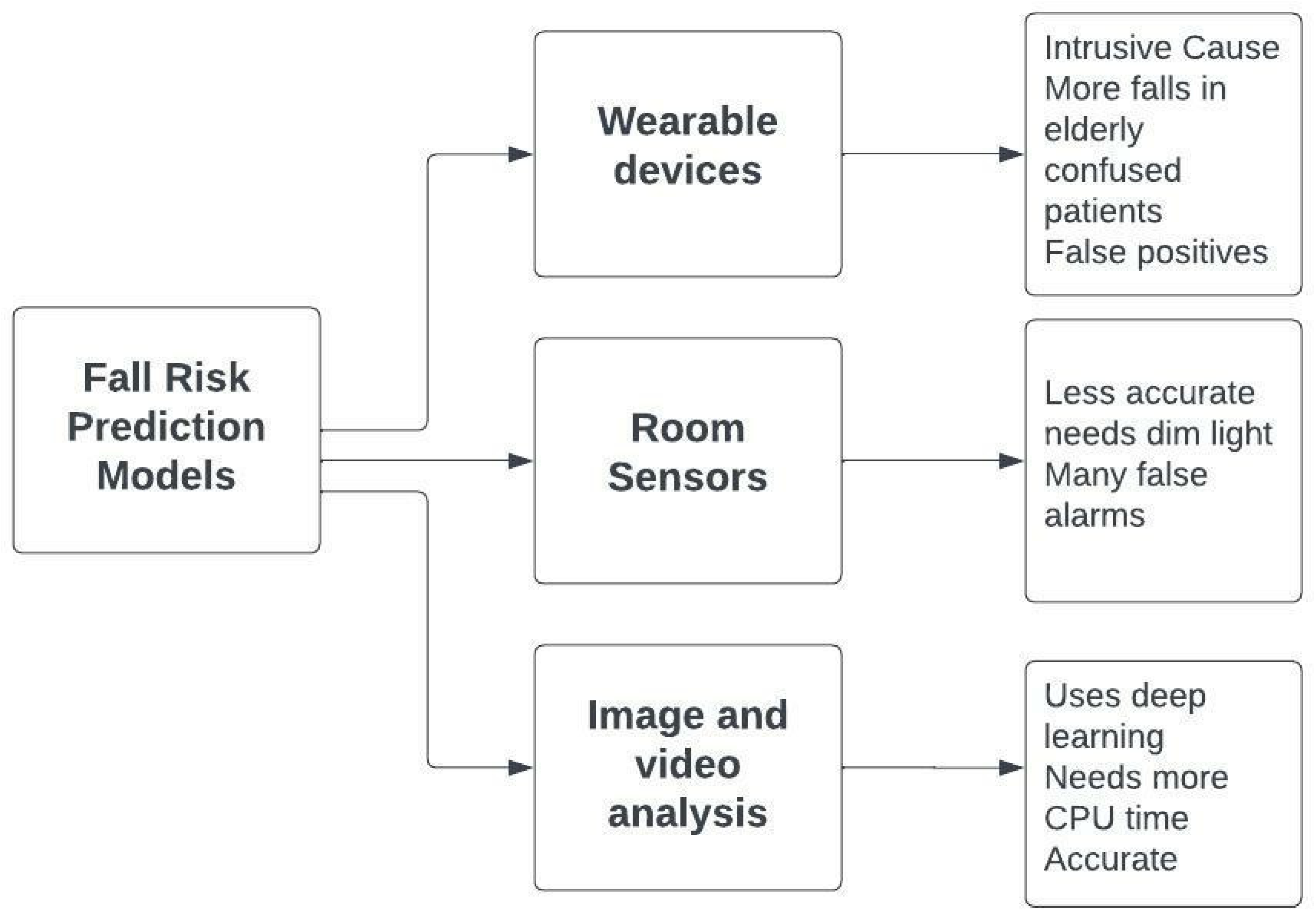
19] presented a flow model which performed the first phase by using Snowflake Python as the deep learning framework and the RNN architecture. The complexity is enlarged if the data is altered on several hardware models. Such methods predict only safe and risky incidences without further classifying risky incidences. These hybrid models are doing well on previously defined datasets, but with new health-related risk types, more development is necessary. Guaranteeing the real-time requirements of monitoring prediction without degrading the performance is an imperative problem that has to be deliberated for next-era monitoring systems. Based on previous research, this paper proposes an improvement for an automated health monitoring system such that various risky incidences can be classified in real-time, thus constructing a more reliable system. Different fall risk prediction models are depicted in
Figure 1.
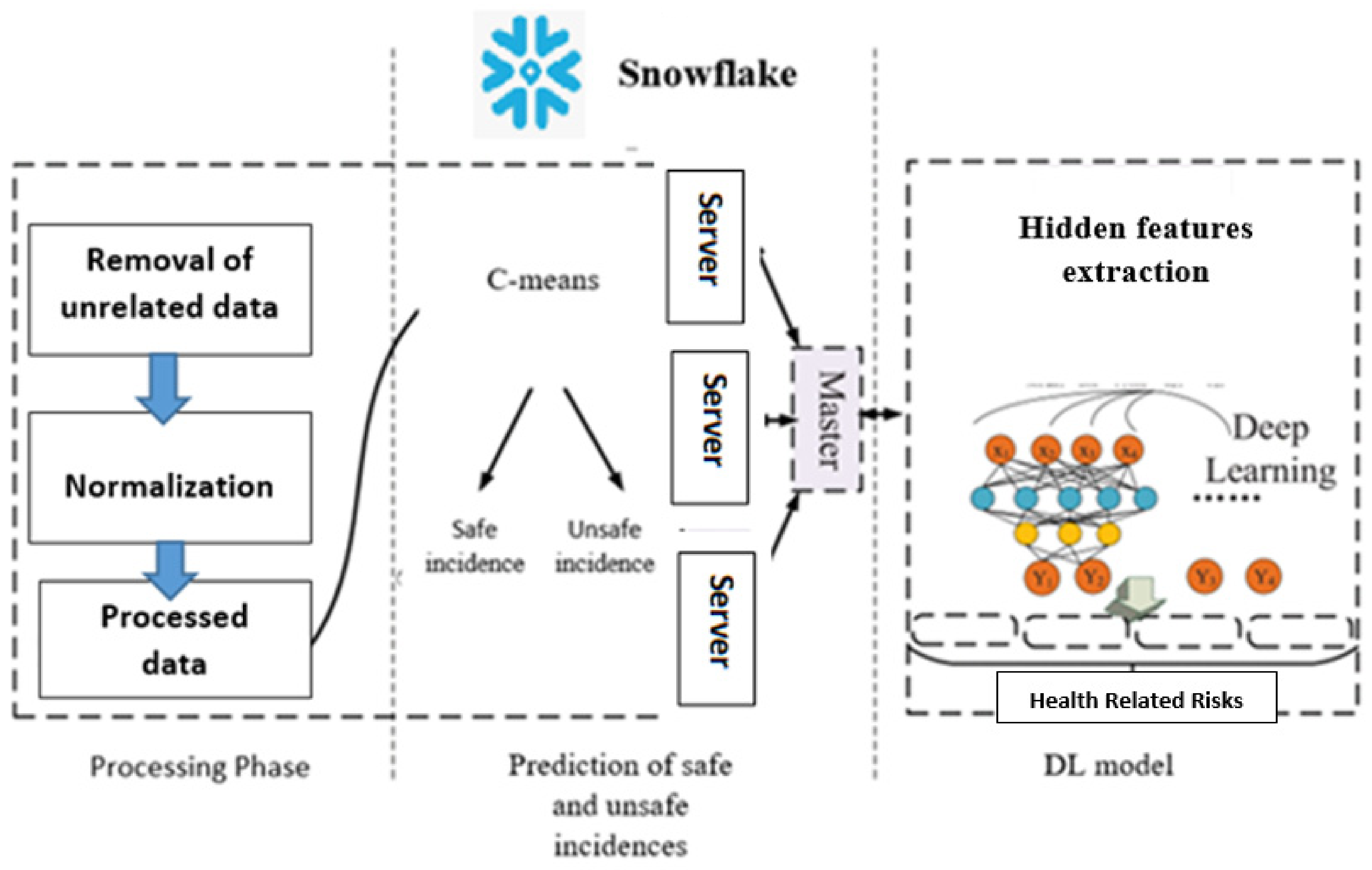
Therefore, in this paper, we introduce a monitoring intelligent prediction system. The proposed system incorporates a scalable clustering method using the Catboost binary classification. These techniques are executed on the Snowflake platform (
https://www.snowflake.com/en/) accessed on 23 June 2022, for real-time prediction of risk. Snowflake’s Data Cloud is powered by an advanced data platform provided as Software-as-a-Service (SaaS). Snowflake enables data storage, processing, and analytic solutions that are faster, easier to use, and far more flexible than traditional offerings [
22] We then employ a deep learning neural network to classify various monitoring alert types (fall, fall with broken bones, and falls that lead to death).
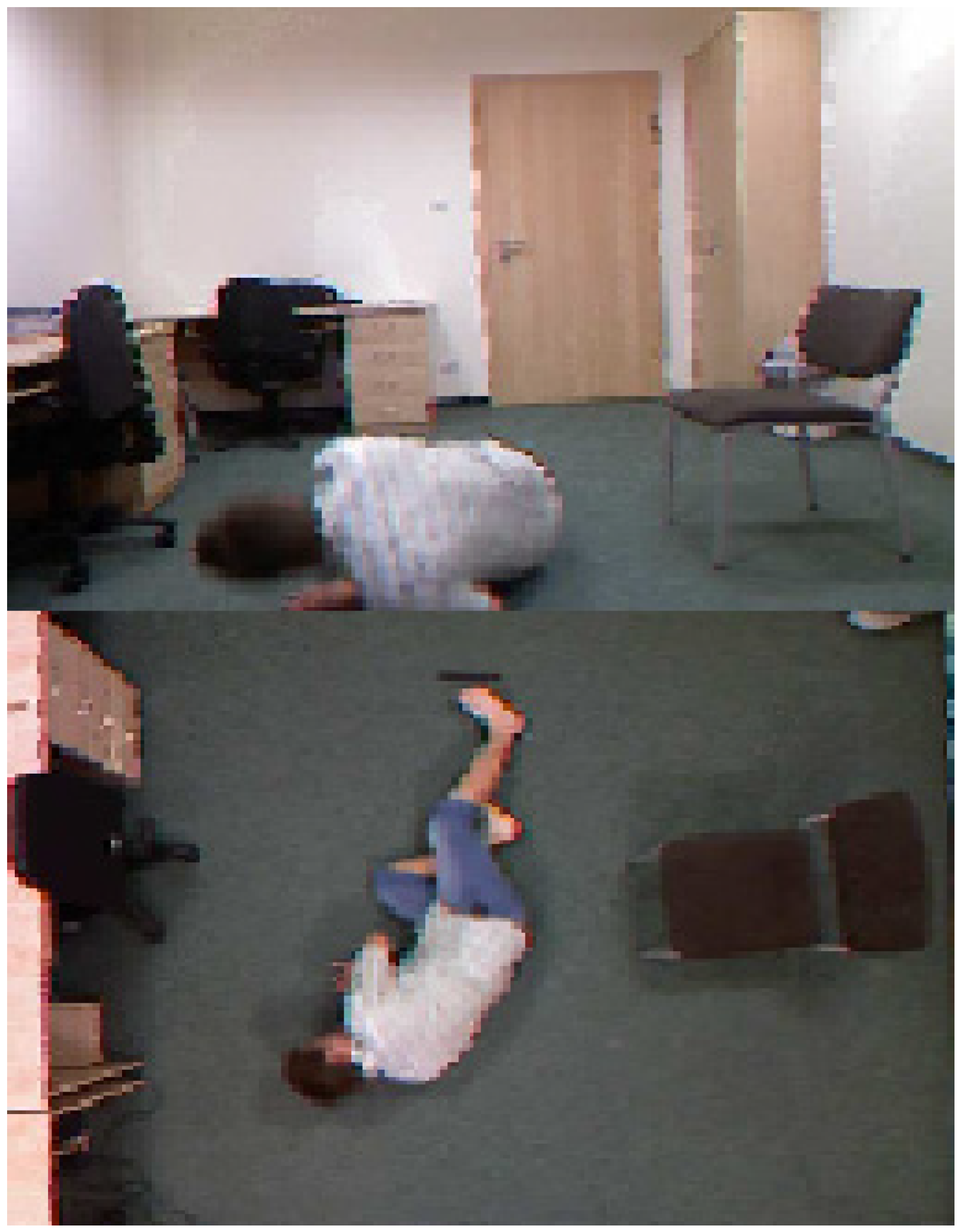
This paper proposes a multi-stage monitoring prediction model using a distributed method that can be utilized for a considerably sized dataset. The proposed model utilizes intelligent techniques to extract hidden features to prevent an overfitting problem. A comparison of the performance of the true positive rate on the SERV-112 and SV-S2017 datasets depicts a higher true positive rate for health-related risk incidences and a higher true positive rate for multi-risk prediction. Both datasets are composed of an image sequence of 120 frames for each incident.
The organization of this paper is depicted as follows.
Section 2 outlines the materials and methods of the proposed research. The experimental settings and the classification results are elucidated in
Section 3. Conclusions from the proposed research are perceived in
Section 4.
3. Results and Discussion
The deep learning model is depicted in
Table 4. We generated a Snowflake framework and ran Snowflake processes; this is also an essential experimental setting for the final phase. The nodes are configured with a TMS 34010, Intel, New York, NY, USA, graphic processor (
https://www.ti.com/lit/pdf/spvu015 accessed on 23 June 2022), which utilizes Tensor as the prime platform of Keras. This permits us to decrease the training time of the DNN system. After the binary prediction by the DNN model on the Snowflake framework, the safe and unsafe incidences are directly computed by the distributed model to the master side. In the final phase, the monitoring prediction data saved on the master side can be utilized for prediction straight away as depicted in
Table 4.
3.1. Evaluation
Evaluation methods for prediction results of unsafe incidences are used. Precision and true positive rate and true negative rate are mostly measured. The ratio of incidences in the test subset diverges, and the classification outcomes may be inclined to incidences with higher occurrence data. Thus, the precision is not enough. The classification outcomes produced by the monitoring system can be partitioned into several groups.
The accuracy is the percentage of correctly classified incidences to the total incidences count. Accuracy is employed for all safe incidences and unsafe incidences in the test dataset. The true positive rate is the percentage of incidences defined as health-related risks, which are properly classified as health-related risks in the datasets for all items defined as health-related risks as depicted in the equations below.
where, true positive (
TP) is defined as the correctly classified health-related risk incidences, and
TN denotes the properly classifies safe incidences.
FP depicts the mistakenly classified positive incidences and a false negative is defined as the incorrectly classified negative incidences.
3.2. Binary Prediction Experiments
The prediction by the deep DNN prediction system, the results are depicted in
Table 5 and
Table 6. The prediction rate in SERV-112 is 91.80%, and the prediction results in the SV-S2017 are 99.67%, specifying health-related risk incidences can be predicted accurately. The false positive rate of health-related risk incidences is very little. This indicates that the accuracy of the prediction system is high. Prediction accuracy and the positive ratio for the SERV-112 set can encounter further prediction of health-related risk incidences in the final phase.
3.3. The Experimental Results of the Multi-Risk Health Related Incidences Prediction
The multi-risk health-related incidences prediction employs several deep learning frameworks: DNN, long short-term memory, and DNN + long short-term memory. The factors of the training system affect the prediction experimental ratios. After several epochs, the deep layers of the DNN system are made equal to 2056, the FC size is made equal to 6, and the pooling layers are made equal to 4. The factors for the long short-term memory system are set to 520. The parameter of the DNN + long short-term memory system is computed using the previous systems. The preliminary learning rate is equal to 0.02.
The precision rate of the loss rate of the training systems of eight convolutions is depicted. The three deep learning systems can accomplish high accuracy and low loss rates. It is observed that the count of epochs needed to predict only health-related risk incidences is 100 epochs, which is considerably low compared to the 500 epochs needed by the model in [
27] to predict safe incidences and the five types of health-related risk incidences. The early splitting of safe incidences avoids pointless training time for the multi-risk unsafe prediction phase based on the training deep learning CNN techniques [
28,
29,
30]. Therefore, the learning curve can be considerably abridged [
31].
In [
32,
33] the study assessed Tresca stress in CoCrMo-onCoCrMo hip implants using patient body mass index. The authors presented a 2D computational model to attain this objective.
Results depicted in
Figure 7 show the correlation between the real ratio of risk incidence in elderly patients from a physician’s judgment from patients’ charts, and the ratio of the risk incidence detected from the proposed system.
The Bland-Altman plot of the real ratio of the risk incidence in elderly patients from a medical personal prognosis in comparison to the calculated ratio of risk incidence of the proposed system is depicted in
Figure 8.
The true positive rates of health-related risk incidences used for the three used models are depicted in
Table 5 and
Table 6. In the SERV-112 dataset, the monitoring prediction method predicted by the DNN is comparatively balanced. The True positive rate in the DNN system with four hidden layers is above 80%, and the health-related risk incidences have a moderate recall rate. Compared with the system presented, long short-term memory is considerably enhanced in the proposed research, with a true positive rate as high as 92.8%. The other groups of health-related risk incidences have a reasonably balanced true positive rate (namely; fall, fall with broken bones, and fall that leads to death).
Table 7 shows that other common health-related risk types have the highest true positive rate in the presented methods in the SV-S2017 dataset, except for falls that lead to death risk. In precise, the True positive rate of Fall, Fall with broken bones accomplish up to 98.7%. This means that fall and fall with broken bones can be classified with high precision, as depicted in
Table 7 and
Table 8.
The computational load is challenging due to the fact that these systems were realized on various platforms. Thus, the computational load can be depicted by simulation models. The final phase of the system is grounded on the statistic that testing datasets are partitioned into unsafe related risk incidences and safe incidences from the second phase. The incidences predicted as unsafe-related risks from the second phase were gathered on the server. The DNN prediction system of the final phase is predicted from the server, and testing will be converted frequently on various platforms. Snowflakes’ distributed hardware finalizes the data of the training input in the final phase and will save training time in this phase. The prediction system utilizes Azure Machine, which utilizes the speedup technique for faster training, so the computational load of the final phase can be enhanced.
Figure 9 depicts the correctly classified versus incorrectly-classified instances.
Table 9 and
Table 10 depict the comparison of the prediction time in seconds.
3.4. Comparison and Discussion
Comparison between the proposed model (DNN + LS) model and other fall prediction models is displayed in
Table 11.
Computational CPU Time
In deep learning neural networks, training time is one of the metrics for defining the model performance. In addition, classification CPU time is very crucial, especially for real time applications. The fall monitoring system is one of the real time applications where classification has to be done in real time from video captured by the camera. In the following table we display the CPU time comparisons for both training time and classification time.
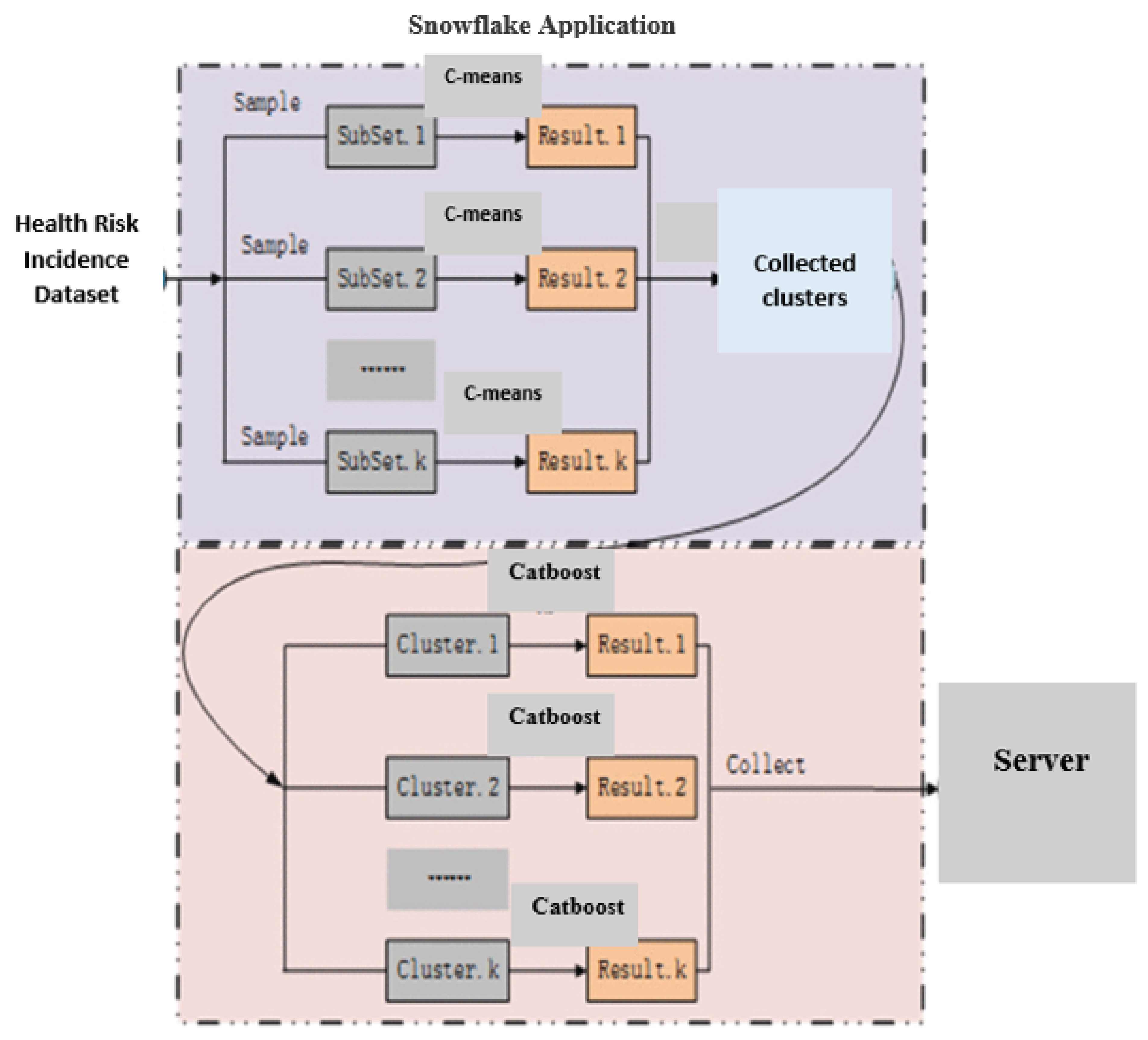
As we can see from
Table 12, the proposed model maintains an average time that is lower than the other models in training time. This is due to two factors: The first factor is the Snowflake’s distributed hardware where the system is designed and implemented to be distributed system. The second factor is the application of the C-Means from the beginning to cluster the fall incidence from the No-Fall incidences before the deep learning training phase. The same two factors contribute significantly to less classification time for alarms to notify health personnel about a future fall incident, as depicted in
Table 13.
4. Conclusions
This article presented a cascading monitoring prediction technique based on distributed C-means, Catboost, and deep learning. We presented a methodology to solve monitoring systems problems that are computationally time-consuming and that have low prediction accuracy. The distributed methodology is utilized to accomplish the time-efficient processing of the monitoring prediction dataset. The unsafe related risk incidences and safe incidences were alienated by incorporating the distributed C-means and the Catboost technique. The isolated unsafe related risk incidences are fed to deep learning systems that extract hidden features of multi-risk incidences. The final phase performs the prediction of various related risk incidences promptly. The prediction system presented in this paper is evaluated using the SERV-112 and SV-S2017 datasets. The experimental results depict that the presented method can efficiently recognize the prediction of health-related risk incidences. The performance of safe incidences and the other three types of unsafe related risk incidences is 87.24% in the SERV-112 dataset, while the accuracy of unsafe incidences is 98.9% in the SV-S2017 dataset. We also compared the proposed model (DNN + LS) with the separate deep learning monitoring prediction systems (DNN and LS)), and the system presented in this paper achieved a higher true positive rate for most risk incidences irrespective of the incidence number of these related risk incidences, which determined that more elderly related risks could be precisely predicted. The proposed model maintains average time that is lower than the other models in training time. This is due to two factors. The first factor is the Snowflakes’ distributed hardware where the proposed system is designed and implemented to the distributed system. The second factor is the application of the C-Means from the beginning to cluster the fall incidence from the No-Fall incidences before the deep learning training phase. The same two factors contribute significantly to less classification time for alarms to notify health personnel about a future fall incident.
The limitation of this study is the lack of posture information in the learning stage, as it might help in the classification process, but it might take require more classification CPU time.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}