
Effectiveness of Shock-Absorbing Insole for High-Heeled Shoes on Gait: Randomized Controlled Trials

Abstract
:1. Introduction
2. Materials and Methods
- Healthy adult women;
- Persons who consented to the purpose and the method of this research, which were explained to them beforehand;
- Persons who had not suffered from a musculoskeletal injury to the lower extremities within the past year;
- Persons who did not have an orthopedic disability or pain in the lower Extremities;
- Persons whose buttocks, knees, and ankle joint range of motion (ROM) were in the normal range;
- Persons who satisfied height in the range of 155–175 cm and WHO Standard Normal BMI Index of 18.5–24.9.
2.1. Sample Size
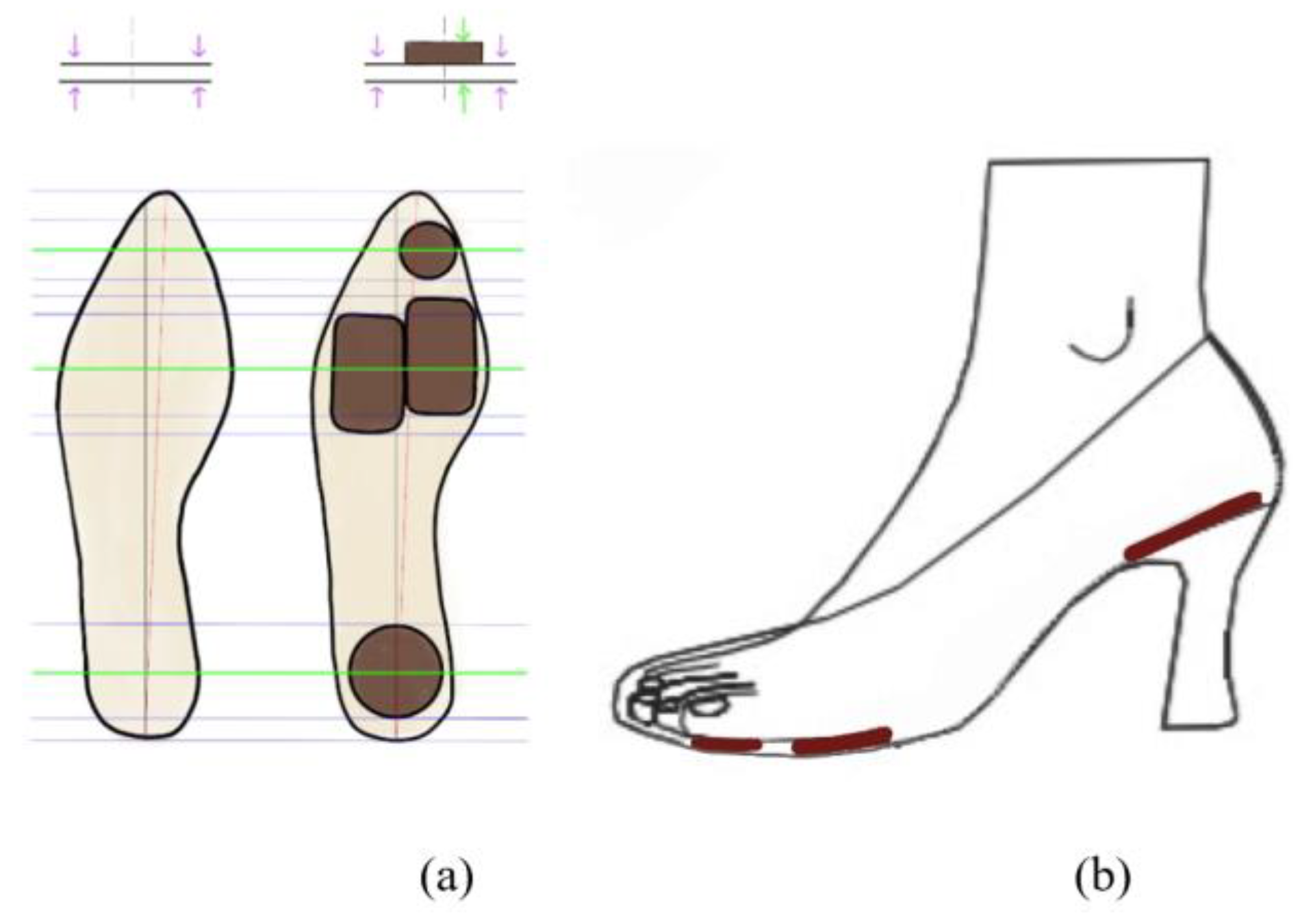
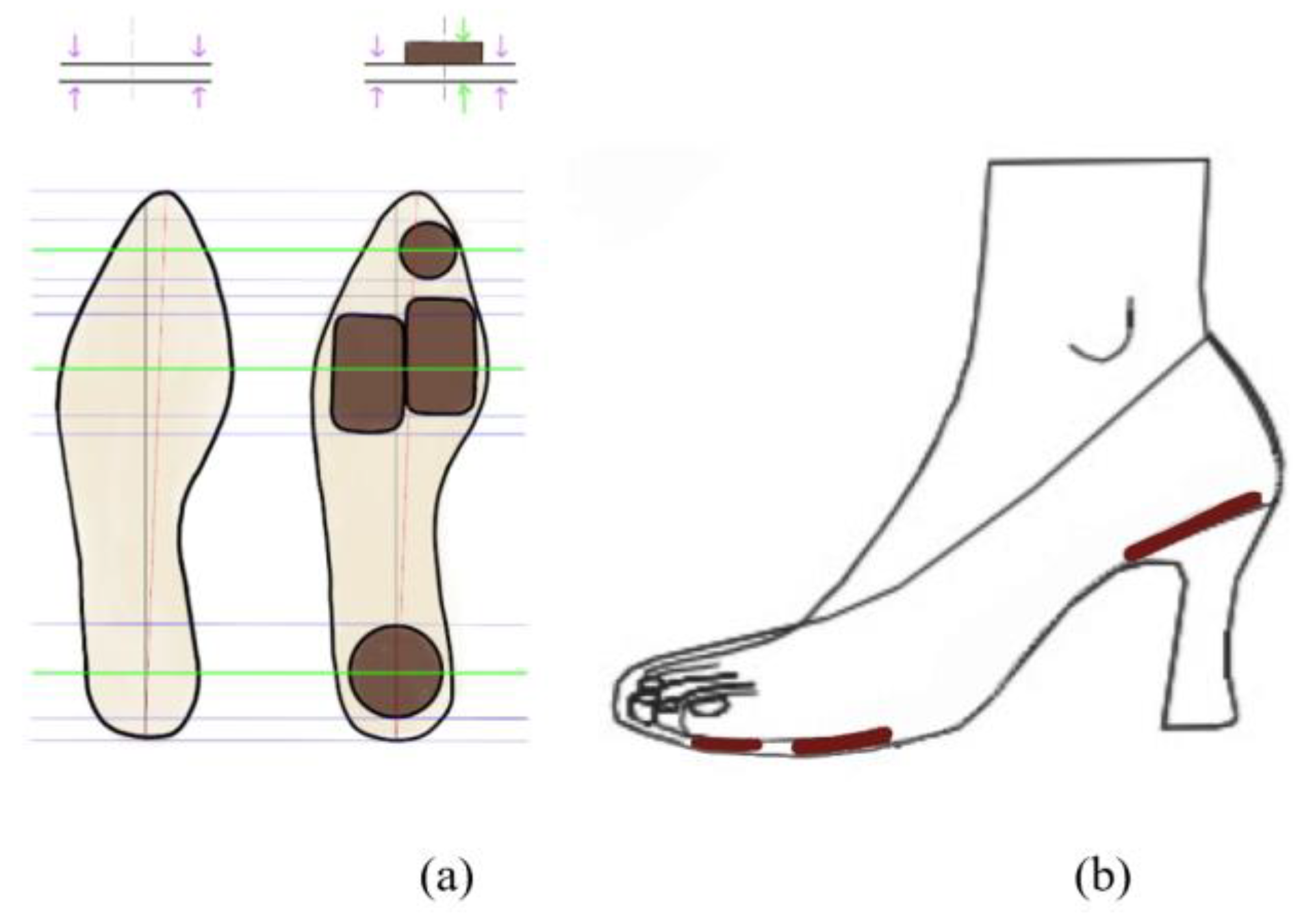
2.2. The Information Regarding the Shock-Absorbing Insole for Use with HH Shoes
2.3. Study Design
2.4. Experimental Procedure
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, M.; Jiang, C.; Fekete, G.; Teo, E.; Gu, Y. Health view to decrease negative effect of high heels wearing: A systemic review. Appl. Bionics Biomech. 2021, 2021, 1–10. [Google Scholar] [CrossRef]
- Moon, G.S. The effect for the different height of high-heeled shoes on the lower extremity joint during the level running. Korean J. Sport Sci. 2014, 23, 1311–1324. [Google Scholar]
- Fox, A.S. Change-of-direction biomechanics: Is what’s best for anterior cruciate ligament injury prevention also best for performance? Sports Med. 2018, 48, 1799–1807. [Google Scholar] [CrossRef]
- LaPlaca, D.A.; Seedman, J. The importance of the foot and ankle in athletic performance. Strength Cond. J. 2021, 43, 67–79. [Google Scholar] [CrossRef]
- Mishra, E.; Jena, S.; Bhoi, C.; Arunachalam, T.; Panda, S.K. Effect of high heel gait on hip and knee-ankle-foot rollover characteristics while walking over inclined surfaces—a pilot study. Foot 2019, 40, 8–13. [Google Scholar] [CrossRef]
- Nguyen, L.Y.; Harris, K.D.; Morelli, K.M.; Tsai, L.C. Increased knee flexion and varus moments during gait with high-heeled shoes: A systematic review and meta-analysis. Gait Posture 2021, 85, 117–125. [Google Scholar] [CrossRef]
- Liau, Y.Y.; Kim, S.; Jin, S.; Ryu, K. The effect of wearing high-heels and carrying a backpack on trunk biomechanics. Int. J. Ind. Ergon. 2021, 86, 103229. [Google Scholar] [CrossRef]
- Gerych, D.; Tvrznik, A.; Prokesova, E.; Nemeckova, Z.; Jelen, K. Analysis of peak pressure, maximal force, and contact area changes during walking and running with conventional and shock-absorbing insoles in the combat boots of the czech army. J. Mech. Med. Biol. 2013, 13, 1350042. [Google Scholar] [CrossRef]
- Patwa, R.; Saha, N.; Sáha, P. Magnetic hydrogel based shoe insoles for prevention of diabetic foot. J Magn. Magn. Mater. 2020, 514, 167153. [Google Scholar] [CrossRef]
- Kim, B.G.; Lee, J.S.; Yang, J.O.; Lee, B.J. Analysis of the plantar pressure on the flat and slope walking by insole type. Korean J. Sport Sci. 2018, 28, 165–173. [Google Scholar]
- Charu, G.; Manoj, M.; Jaspreet, K.; Minaxi, S. A systematic review and meta-analysis on effect of spinal mobilization and manipulation on cardiovascular responses. Hong Kong Physiother J. 2020, 40, 75–87. [Google Scholar]
- Kwon, M.H.; Han, B.D.; Cho, S.J.; Cho, J.H. Analysis of body fat mass index for korean adults. Korean J. Fam. Med. 2021, 11, 81–85. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A.G. G* power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Párraga-Montilla, J.A.; Pozuelo-Carrascosa, D.P.; Carmona-Torres, J.M.; Laredo-Aguilera, J.A.; Cobo-Cuenca, A.I.; Latorre-Román, P.Á. Gait performance as an indicator of cognitive deficit in older people. Gait Perform. Indic. Cogn. Deficit Older People 2021, 18, 3428. [Google Scholar] [CrossRef] [PubMed]
- Cha, Y.J. Analysis of differences in the degree of biomechanical adaptation according to habituation to different heel heights. Sci. World J. 2020, 2020, 1–11. [Google Scholar] [CrossRef] [PubMed]
- van Melick, N.; Meddeler, B.M.; Hoogeboom, T.J.; Nijhuis-van der Sanden, M.W.G.; van Cingel, R.E.H. How to determine leg dominance: The agreement between self-reported and observed performance in healthy adults. PLoS ONE 2017, 12, e0189876. [Google Scholar] [CrossRef] [PubMed]
- Melai, T.; Ijzerman, T.H.; Schaper, N.C.; de Lange, T.L.H.; Willems, P.J.B.; Meijer, K.; Lieverse, A.G.; Savelberg, H.H.C.M. Calculation of plantar pressure time integral, an alternative approach. Gait Posture 2011, 34, 379–383. [Google Scholar] [CrossRef] [PubMed]
- Price, C.; Parker, D.; Nester, C. Validity and repeatability of three in-shoe pressure measurement systems. Validity Repeatability Three-Shoe Press. Meas. Syst. 2016, 46, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Elsais, W.M.; Preece, S.J.; Jones, R.K.; Herrington, L. Between-day repeatability of lower limb emg measurement during running and walking. J. Electromyogr. Kinesiol. 2020, 55, 102473. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.; Jeong, D.; Choi, H. The effects of squat exercises with vertical whole-body vibration on the center of pressure and trunk muscle activity in patients with low back pain. J Int. Acad. Phys. Ther. Res. 2020, 11, 2253–2260. [Google Scholar] [CrossRef]
- Dubois, A.; Bresciani, J.-P. Validation of an ambient system for the measurement of gait parameters. J. Biomech. 2018, 69, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, A.; Singh, D.K.A.; Shahar, S. ‘Timed up and go’ test: Age, gender and cognitive impairment stratified normative values of older adults. PLoS ONE 2017, 12, e0185641. [Google Scholar]
- Aboutorabi, A.; Bahramizadeh, M.; Arazpour, M.; Fadayevatan, R.; Farahmand, F.; Curran, S.; Hutchins, S.W. A systematic review of the effect of foot orthoses and shoe characteristics on balance in healthy older subjects. Prosthet. Orthot. Int. 2016, 40, 170–181. [Google Scholar] [CrossRef] [PubMed]
- Losa Iglesias, M.E.; Becerro de Bengoa Vallejo, R.; Palacios Peña, D. Impact of soft and hard insole density on postural stability in older adults. Geriatr. Nurs. 2012, 33, 264–271. [Google Scholar] [CrossRef]
- Hong, W.H.; Lee, Y.H.; Lin, Y.H.; Tang, S.F.T.; Chen, H.C. Effect of shoe heel height and total-contact insert on muscle loading and foot stability while walking. Foot Ankle Int. 2013, 34, 273–281. [Google Scholar] [CrossRef]
- Nagano, H.; Begg, R.K. Shoe-insole technology for injury prevention in walking. Sensors 2018, 18, 1468. [Google Scholar] [CrossRef]
- Bonanno, D.R.; Landorf, K.B.; Munteanu, S.E.; Murley, G.S.; Menz, H.B. Effectiveness of foot orthoses and shock-absorbing insoles for the prevention of injury: A systematic review and meta-analysis. Br. J. Sports Med. 2017, 51, 86–96. [Google Scholar] [CrossRef]
- Yoo, K.T. The effect of the insole height on lower limb joint angle and muscle activity at landing when the maximal ground reaction force of male in their 20s. J Converg. Inf. Technol. 2020, 10, 132–139. [Google Scholar]
- Hapsari, V.D.; Xiong, S. Effects of high heeled shoes wearing experience and heel height on human standing balance and functional mobility. Ergonomics 2016, 59, 249–264. [Google Scholar] [CrossRef]
- Kim, Y.; Joo, J.; Jung, J. Effects of custom-made 3D printed insoles on the trajectories of center of pressure of flat foot gait. In Proceedings of the KSPE 2017 Spring Conference, Je-Ju do, Korea, 17 May 2017. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Equipment Model (Company) | Variables | Unit | |
|---|---|---|---|
| In-Shoe Pressure Measuring System | Pedar-X System (Novel Gmbh, Germany) | Peak pressure (PP) Contact area (CA) Force time integral (FTI) | kPa cm2 Ns/cm2 |
| Comfort Visual Analog Scale (Comfort VAS) | - | comfort levels | score |
| Surface EMG | Noraxon EMG (Noraxon USA Inc., Scottsdale, AZ, USA) | Root Mean Square (RMS) Reference voluntary contraction (RVC) | uV % |
| Kinematics (Joint Angles) Motion Analysis | OptiTrack (Natural Point, OR, USA) | Degree | ° |
| Timed up and go test (TUG) | - | functional mobility | sec |
| Experimental Group (n= 26) | Control Group (n = 26) | p | ||
|---|---|---|---|---|
| Age (years) | 25.38 ± 8.27 | 25.31 ± 7.01 | 0.973 a | |
| Weight (kg) | 57.70 ± 7.49 | 56.49 ± 8.24 | 0.598 a | |
| Height (m) | 162.62 ± 4.59 | 162.27 ± 6.26 | 0.793 a | |
| BMI (kg/m2) | 21.75 ± 1.99 | 21.38 ± 2.26 | 0.578 a | |
| Shoe size | 240.00 ± 5.10 | 239.42 ± 6.53 | 0.743 a | |
| IPAQ | Low | 11 (42.31) c | 6 (23.08) | 0.574 b |
| Moderate | 10 (38.46) | 11 (42.31) | ||
| High | 5 (19.23) | 9 (34.62) | ||
| TUG | 8.13 ± 0.98 | 9.13 ± 1.22 | 0.004 ** a |
| Experimental Group (n = 26) | Control Group (n = 26) | p–Value | ES | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | 95% CI | Mean | SD | 95% CI | ||||
| Hallux | PP (kPa) | 110.27 | 18.05 | 106.20–114.34 | 114.67 | 44.17 | 104.71–124.63 | 0.393 | 0.613 |
| CA (cm2) | 8.99 | 17.08 | 5.14–12.84 | 6.26 | 1.29 | 5.97–6.55 | 0.164 | 0.099 | |
| FTI (Ns/cm2) | 184.75 | 53.85 | 172.61–196.90 | 209.16 | 58.56 | 195.96–222.36 | 0.005 ** | 0.503 | |
| Toes | PP (kPa) | 41.38 | 14.66 | 38.08–44.69 | 50.34 | 12.86 | 47.44–53.24 | 0.000 *** | 0.457 |
| CA (cm2) | 5.60 | 5.35 | 4.40–6.81 | 5.87 | 1.55 | 5.52–6.22 | 0.678 | 0.197 | |
| FTI (Ns/cm2) | 76.07 | 35.46 | 68.07–84.06 | 121.42 | 38.15 | 122.82–130.02 | 0.000 *** | 0.311 | |
| Medial forefoot | PP (kPa) | 109.40 | 17.40 | 105.48–113.32 | 109.86 | 75.59 | 92.82–126.90 | 0.960 | 0.715 |
| CA (cm2) | 13.97 | 18.44 | 9.81–18.12 | 9.21 | 2.91 | 8.55–9.86 | 0.028 * | 0.216 | |
| FTI (Ns/cm2) | 441.60 | 105.91 | 417.72–465.48 | 363.85 | 97.14 | 341.95–385.75 | 0.000 *** | 0.492 | |
| Lateral forefoot | PP (kPa) | 75.94 | 13.27 | 72.95–78.93 | 59.07 | 43.09 | 49.35–68.78 | 0.002 * | 0.346 |
| CA (cm2) | 12.23 | 13.24 | 9.24–15.21 | 8.85 | 2.85 | 8.21–9.49 | 0.031 * | 0.344 | |
| FTI (Ns/cm2) | 274.12 | 70.63 | 258.20–290.05 | 196.99 | 75.47 | 179.97–214.01 | 0.000 *** | 0.430 | |
| Midfoot | PP (kPa) | 12.20 | 6.37 | 10.76–13.63 | 15.79 | 8.03 | 13.98–17.60 | 0.002 ** | 0.354 |
| CA (cm2) | 3.20 | 2.42 | 2.66–3.75 | 4.38 | 2.52 | 3.82–4.95 | 0.004 ** | 0.331 | |
| FTI (Ns/cm2) | 24.96 | 20.40 | 20.36–29.56 | 45.49 | 26.28 | 39.57–5.42 | 0.000 *** | 0.297 | |
| Heel | PP (kPa) | 76.12 | 22.06 | 71.14–81.09 | 86.57 | 49.19 | 75.48–97.66 | 0.106 | 0.511 |
| CA (cm2) | 15.98 | 16.69 | 12.21–19.74 | 14.86 | 5.54 | 13.61–16.10 | 0.575 | 0.219 | |
| FTI (Ns/cm2) | 355.34 | 136.30 | 324.61–386.07 | 518.70 | 192.91 | 475.21–562.20 | 0.000 *** | 0.478 | |
| Variables | Overall Comfort of EG | Overall Comfort of CG | ||
|---|---|---|---|---|
| r | p | r | p | |
| Hallux | 0.045 | 0.829 | 0.382 | 0.054 |
| Toes | 0.337 | 0.093 | −0.174 | 0.395 |
| Medial forefoot | −0.082 | 0.691 | 0.385 | 0.052 |
| Lateral forefoot | −0.131 | 0.525 | −0.224 | 0.272 |
| Midfoot | −0.096 | 0.64 | −0.293 | 0.146 |
| Heel | 0.555 ** | 0.003 | −0.049 | 0.813 |
| Type Event | Experimental Group | Control Group | p–Value | ES | |||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | 95% CI | Mean | SD | 95% CI | ||||
| Gait Cycle | VL | 35.89 | 11.67 | 33.09–38.69 | 42.49 | 17.27 | 38.34–46.64 | 0.015 * | 0.431 |
| TA | 341.53 | 106.48 | 315.95–367.11 | 280.79 | 107.56 | 254.95–306.63 | 0.000 *** | 0.472 | |
| BF | 458.69 | 172.93 | 417.15–500.24 | 496.54 | 158.51 | 458.46–534.62 | 0.179 | 0.367 | |
| GA | 712.65 | 282.33 | 787.86–883.81 | 835.83 | 199.70 | 644.82–780.47 | 0.002 ** | 0.631 | |
| Stances Period | VL | 37.42 | 11.48 | 34.66–40.18 | 40.39 | 13.29 | 37.20–43.58 | 0.153 | 0.450 |
| TA | 342.26 | 101.61 | 317.85–366.67 | 310.09 | 108.12 | 284.12–336.07 | 0.065 | 0.413 | |
| BF | 478.53 | 115.63 | 450.75–506.31 | 510.00 | 171.11 | 468.90–551.11 | 0.192 | 0.391 | |
| GA | 677.72 | 127.37 | 695.55–770.98 | 733.27 | 157.00 | 647.13–708.32 | 0.022 * | 0.378 | |
| Swing Period | VL | 28.53 | 11.53 | 25.76–31.30 | 43.11 | 14.06 | 39.73–46.49 | 0.000 *** | 0.473 |
| TA | 357.20 | 108.65 | 331.10–383.30 | 357.16 | 119.27 | 328.51–385.81 | 0.998 | 0.618 | |
| BF | 442.88 | 155.39 | 405.55–480.21 | 435.91 | 151.00 | 399.64–472.19 | 0.783 | 0.552 | |
| GA | 703.02 | 166.75 | 662.96–743.07 | 699.37 | 131.49 | 667.78–730.96 | 0.891 | 0.328 | |
| %RVC | VL | 3.00 | 2.02 | 2.53–3.49 | 3.76 | 1.05 | 3.51–4.01 | 0.008 ** | 0.052 |
| TA | 23.55 | 6.93 | 21.89–25.21 | 22.09 | 4.89 | 20.92–23.27 | 0.136 | 0.063 | |
| BF | 31.10 | 7.05 | 27.70–32.98 | 30.34 | 11.01 | 29.41–32.79 | 0.634 | 0.008 | |
| GA | 50.23 | 15.54 | 46.49,–53.96 | 55.91 | 15.73 | 52.13–59.68 | 0.038 * | 0.118 | |
| Experimental Group | Control Group | p−Value | ES | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | 95% CI | Mean | SD | 95% CI | ||||
| Hip | Flex−Ext | 3.28 | 6.43 | 1.83–4.73 | 0.42 | 2.54 | −0.15−0.99 | 0.000 *** | 0.253 |
| Abd−Add | −4.94 | 2.85 | −5.58–4.30 | −7.99 | 5.15 | −9.15–6.83 | 0.055 | 0.319 | |
| Int−Ext | −15.08 | 9.8 | −17.29–12.87 | −21.84 | 5.68 | −23.12–20.56 | 0.000 *** | 0.104 | |
| Knee | Flex−Ext | 9.53 | 4.16 | 8.59−10.47 | 8.4 | 4.23 | 7.44−9.35 | 0.000 *** | 0.017 |
| Abd−Add | 5.25 | 2.97 | 4.58−5.92 | 8.34 | 4.6 | 7.31−9.38 | 0.000 *** | 0.013 | |
| Int−Ext | −0.64 | 2.65 | −1.24–0.04 | −0.89 | 2.3 | −1.41–0.37 | 0.000 *** | 0.003 | |
| Ankle | Flex−Ext | 17.98 | 4.17 | 17.04−18.92 | 24.01 | 5.09 | 22.86−25.15 | 0.100 | 0.260 |
| Abd−Add | −6.22 | 3.76 | −7.07–5.37 | −4.61 | 6.26 | −6.02–3.20 | 0.000 *** | 0.198 | |
| Int−Ext | 14.44 | 9.97 | 12.19−16.68 | 22.15 | 5.18 | 20.99−23.32 | 0.486 | 0.158 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cha, Y.-J. Effectiveness of Shock-Absorbing Insole for High-Heeled Shoes on Gait: Randomized Controlled Trials. Healthcare 2022, 10, 1864. https://doi.org/10.3390/healthcare10101864
Cha Y-J. Effectiveness of Shock-Absorbing Insole for High-Heeled Shoes on Gait: Randomized Controlled Trials. Healthcare. 2022; 10(10):1864. https://doi.org/10.3390/healthcare10101864
Chicago/Turabian StyleCha, Yu-Jin. 2022. "Effectiveness of Shock-Absorbing Insole for High-Heeled Shoes on Gait: Randomized Controlled Trials" Healthcare 10, no. 10: 1864. https://doi.org/10.3390/healthcare10101864
APA StyleCha, Y.-J. (2022). Effectiveness of Shock-Absorbing Insole for High-Heeled Shoes on Gait: Randomized Controlled Trials. Healthcare, 10(10), 1864. https://doi.org/10.3390/healthcare10101864