
Clinical Comparison of Diode Laser Assisted “v-Shape Frenectomy” and Conventional Surgical Method as Treatment of Ankyloglossia

 ,
,  , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
- -
- Subjects had to be aged between 8 and 12 years old, in good general health conditions and with no hematic problems;
- -
- Subjects could not be under orthodontic treatment;
- -
- Subjects could not present genetic or congenital pathologies;
- -
- Subjects who need to take drugs were excluded;
- -
- Subjects presenting viral diseases were excluded;
- -
- The parents of the subjects had to sign an Informed Consent in order for the subject to join the study.
2.2. Preoperative Measurements and Treatment
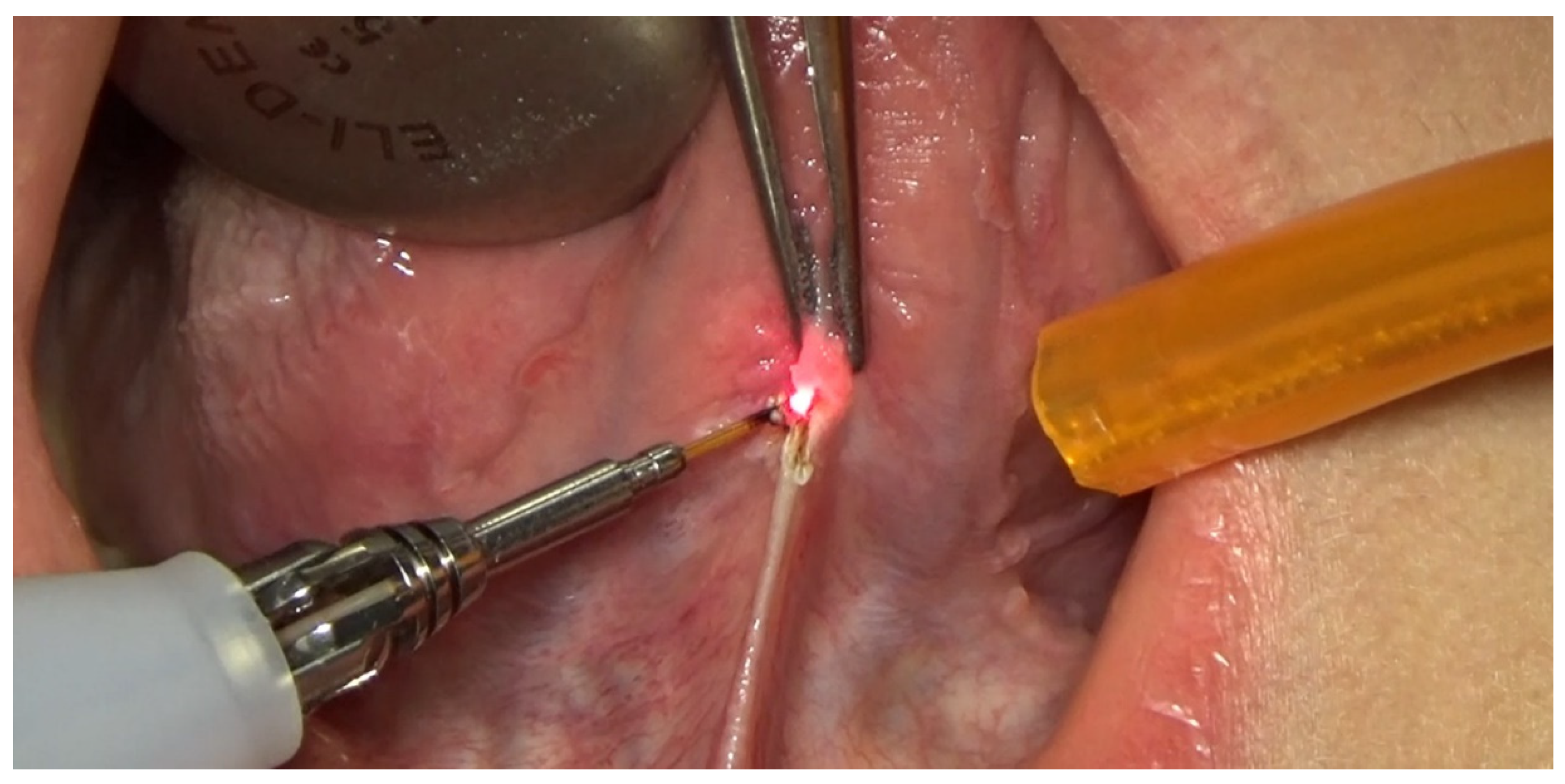
2.3. Operative Protocol for Group A
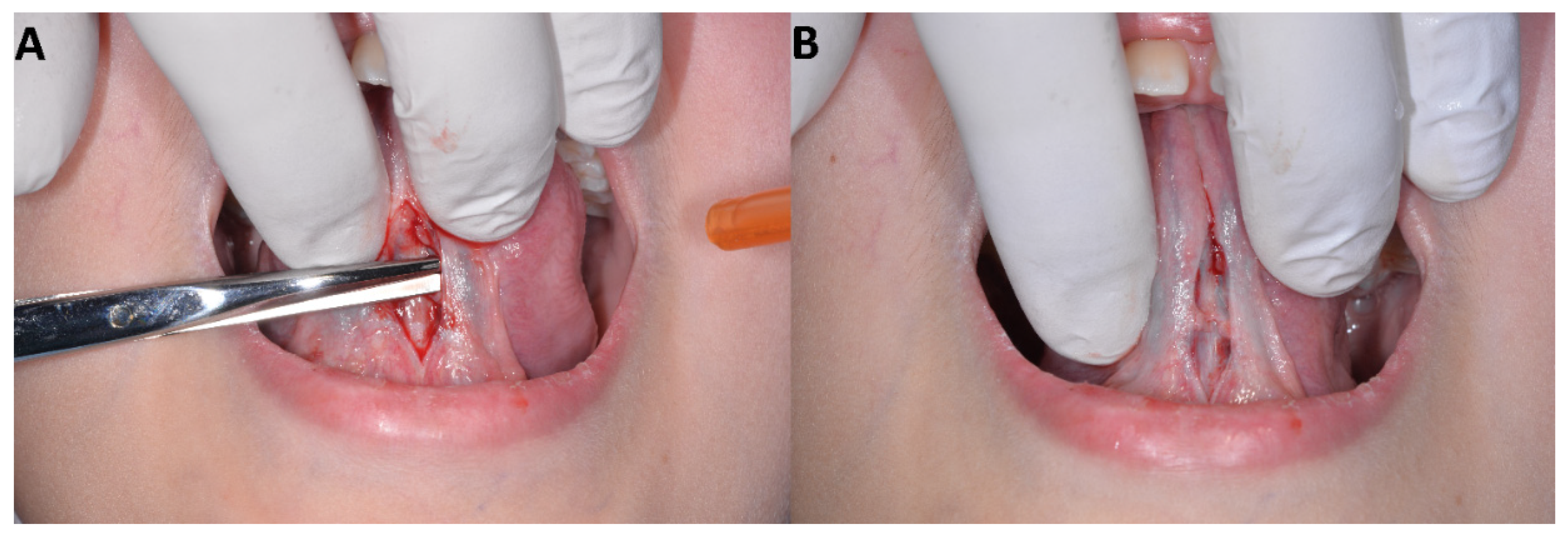
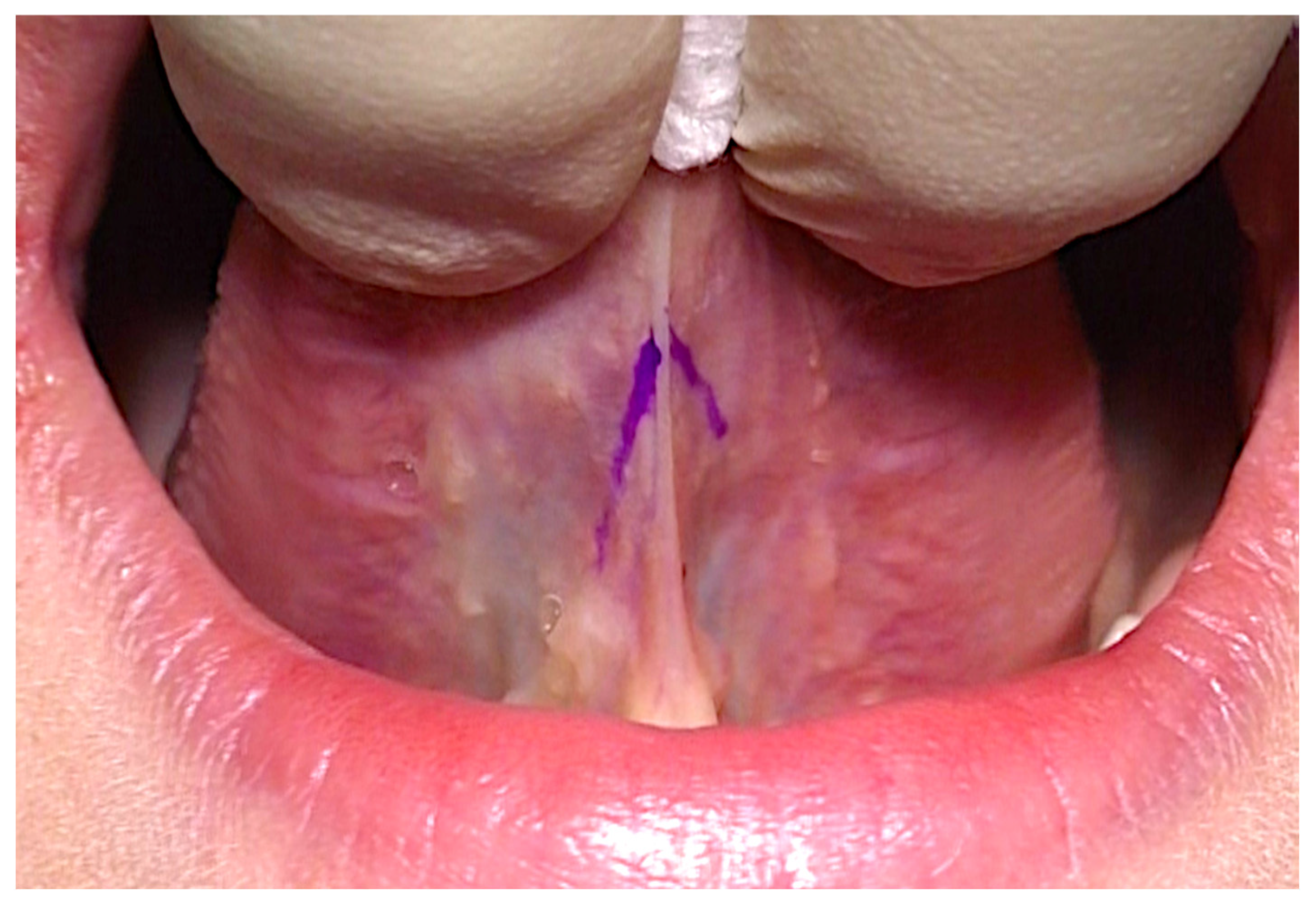
2.4. Operative Protocol for Group B
2.5. Statistical Analysis
3. Results
4. Discussion
5. Limits of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chiapasco, M. Illustrated Manual of Oral Surgery; Elsevier-Masson: Milano, Italy, 2002. [Google Scholar]
- Wallace, A.F. Tongue tie. Lancet 1963, 2, 377–378. [Google Scholar] [CrossRef]
- Walsh, J.; McKenna Benoit, M. Ankyloglossia and other oral ties. Otoryngol Clin North Am. 2019, 52, 795–811. [Google Scholar] [CrossRef]
- Jackson, R. Improving breastfeeding outcomes: The impact of tongue-tie. Community Pract. 2012, 85, 42–44. [Google Scholar]
- Wallace, H.; Clarke, S. Tngue tie division in infants with breast feeding difficulties. Int. J. Pediatr. Otorhinolaryngol. 2006, 70, 1257–1261. [Google Scholar] [CrossRef] [PubMed]
- Buryk, M.; Bloom, D.; Shope, T. Efficacy of neonatal release of ankyloglossia: A randomied trial. Pediatrics 2011, 128, 280–288. [Google Scholar] [CrossRef] [Green Version]
- Suter, V.G.; Bornstein, M.M. Ankyloglossia: Facts and myths in diagnosis and treatment. J. Periodontol. 2009, 80, 1204–1219. [Google Scholar] [CrossRef] [PubMed]
- Lalakea, M.L.; Messner, A.H. Ankyloglossia: Does it matter? Pediatr. Clin. N. Am. 2003, 50, 381–397. [Google Scholar] [CrossRef]
- Azzolino, D.; Passarelli, P.C.; De Angelis, P.; Piccirillo, G.B.; D’Addona, A.; Cesari, M. Poor Oral Health as a Determinant of Malnutrition and Sarcopenia. Nutrients 2019, 11, 2898. [Google Scholar] [CrossRef] [Green Version]
- Olivi, G.; Signore, A.; Olivi, M.; Genovese, M.D. Lingual frenectomy: Functional evaluation and new therapeutical approach. Eur. J. Paediatr. Dent. 2012, 13, 101–106. [Google Scholar]
- Ostapiuk, B. Tongue mobility in ankyloglossia with regard to articulation. Ann. Acad. Med. Atetin. 2006, 52 (Suppl. 3), 37–47. [Google Scholar]
- Messner, A.H.; Lalakea, M.L. The effect ankyloglossia on speech in children. Otolaryngol. Head Neck Surg. 2002, 127, 539–545. [Google Scholar] [CrossRef]
- Lalakea, M.L.; Messner, A.H. Ankyloglossia: The adolescent and adult perspective. Otolaryngol. Head Neck Surg. 2003, 128, 746–752. [Google Scholar] [CrossRef]
- Webb, A.N.; Hao, W.; Hong, P. The effect of tongue-tie division on breastfeeding and speech articulation: A systematic review. Int. J. Pediatr. Otorhinolaryngol. 2013, 77, 635–646. [Google Scholar] [CrossRef]
- Northcutt, M.E. The lingual frenulum. J. Clin. Orthod. 2009, 43, 557–565. [Google Scholar] [PubMed]
- Yoon, A.J.; Zaghi, S.; Ha, S.; Law, C.S.; Guilleminault, C.; Liu, S.Y. Ankyloglossia as a risk factor for maxillary hypo-l’asia and soft palate elongation: A functional-morphological study. Orthod. Craniofacial Res. 2017, 20, 237–244. [Google Scholar] [CrossRef]
- Sforza, E.; Bacon, W.; Weiss, T.; Thibault, A.; Petiau, C.; Krieger, J. Upper airway collapsibility and cephalometric variables in patients with obstructive sleep apnea. Am. J. Respir. Crit. Care Med. 2000, 161, 347–352. [Google Scholar] [CrossRef]
- Ficarra, G. Manuale di Patologia e Medicina Orale; McGraw-Hill: Milano, Italy, 2006. [Google Scholar]
- Kupietky, A.; Boter, E. Ankyloglossia in the infant and young child: Clinical suggestions for diagnosis and management. Pediatr. Dent. 2005, 27, 40–46. [Google Scholar]
- Messner, A.H.; Lalakea, M.L.; Aby, J.; Macmahon, J.; Bair, E. Ankyloglossia: Incidence and associated feeding difficulties. Arch. Otholaryngol. Head Neck Surg. 2002, 126, 36–39. [Google Scholar] [CrossRef] [Green Version]
- Griffith, D. Do tongue-ties affect breastfeeding? J. Hum. Lact. 2004, 20, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Khoo, A.K.; Dabbas, N.; Sudhakaran, N.; Ade-Ajayi, N.; Patel, S. Nipple pain at presentation predicts success of tongue-tie division for breastfeeding problems. Eur. J. Pediatr. Surg. 2009, 19, 370–373. [Google Scholar] [CrossRef]
- Kotlow, L.A. Ankylogllossia (tongue-tie): A diagnostic and treatment quandary. Quintessence Int. 1999, 30, 259–262. [Google Scholar]
- Nurchis, M.C.; Pascucci, D.; Lopez, M.A.; Moffa, A.; Passarelli, P.C.; Bressi, F.; Casale, M.; Damiani, G. Epidemiology of odontogenic sinusitis: An old, underestimated disease, even today. A narrative literature review. J. Biol. Regul. Homeost. Agents 2020, 34 (Suppl. 3), 195–200. [Google Scholar] [PubMed]
- Bollero, P.; Passarelli, P.C.; D’Addona, A.; Pasquantonio, G.; Mancini, M.; Condò, R.; Cerroni, L. Oral management of adult patients undergoing hematopoietic stem cell transplantation. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 876–887. [Google Scholar] [PubMed]
- Passarelli, P.C.; Pagnoni, S.; Piccirillo, G.B.; Desantis, V.; Benegiamo, M.; Liguori, A.; Papa, R.; Papi, P.; Pompa, G.; D’Addona, A. Reasons for Tooth Extractions and Related Risk Factors in Adult Patients: A Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 2575. [Google Scholar] [CrossRef] [PubMed]
- Passarelli, P.C.; Pasquantonio, G.; Manicone, P.F.; Cerroni, L.; Condo, R.; Mancini, M.; D’Addona, A. Orofacial signs and dental abnormalities in patients with Mulvihill-Smith syndrome: A literature review on this rare progeroid pathology. Medicine (Baltimore) 2018, 97, e0656. [Google Scholar] [CrossRef] [PubMed]
- Breinis, P.; Alves, F.G.; Alves, C.A.; Cintra, R.G.; Almeida, D.; Passarelli, P.C.; Domingues, C.; Gerbim, T.; Gasparetto, R.; de Abreu, L.C.; et al. The eleventh reported case of Mulvihill-Smith syndrome in the literature. BMC Neurol. 2014, 14, 4. [Google Scholar] [CrossRef] [Green Version]
- Gross, A.J.; Herrmann, T.R. History of lasers. World J. Urol. 2007, 25, 217–220. [Google Scholar] [CrossRef]
- Lopez, M.A.; Passarelli, P.C.; Marra, M.; Lopez, A.; D’Angelo, A.; Moffa, A.; Martinez, S.; Casale, M.; D’Addona, A. Photodynamic therapy (PDT) in non-surgical treatment of periodontitis. J. Biol. Regul. Homeost. Agents 2020, 34 (Suppl. 3), 67–78. [Google Scholar]
- Lopez, M.A.; Passarelli, P.C.; Marra, M.; Lopez, A.; Moffa, A.; Casale, M.; D’Addona, A. Antimicrobial efficacy of photodynamic therapy (PDT) in periodontitis and peri-implantitis: A systematic review. J. Biol. Regul. Homeost. Agents 2020, 34 (Suppl. 3), 59–65. [Google Scholar] [PubMed]
- Maggioni, M.; Attanasio, T.; Scarpelli, F. Il Laser in Odontoiatria; Piccin-Nuova Libraria: Padova, Italy, 2009. [Google Scholar]
- Deppe, H.; Horch, H. Laser applications in oral surgery and implant dentistry. Lasers Med. Sci. 2007, 22, 217–221. [Google Scholar] [CrossRef]
- Morit, A.; Beer, F.; Goharkhay, K.; Schoop, U.; Strassl, M.; Verheyen, P. Oral Laser Application; Quintessen Verlags-GmbH: Berlin, Germany, 2006. [Google Scholar]
- De Santis, D.; Zanotti, G.; Zanotti, M.; Bondì, V.; Gelpi, F. Laser Assisted Frenulectomy: New Fashion or New Operative Method? Minerva Stomatol: Verona, Italy, 2011; pp. 1–8. [Google Scholar]
- Marini, L.; Rojas, M.A.; Sahrmann, P.; Aghazada, R.; Pilloni, A. Early Wound Healing Score: A system to evaluate the early healing of periodontal soft tissue wounds. J. Periodontal Implant Sci. 2018, 48, 274–283. [Google Scholar] [CrossRef]
- Gabriele, S.; Gaudy, J.F.; Savini, D. Aspetti anatomici e chirurgici della frenulectomia linguale. Ital. Oral Surg. 2008, 3, 7–14. [Google Scholar]
- Fiorotti, R.C.; Bertolini, M.M.; Nicola, J.H.; Nicola, E.M. Early lingual frenectomy assisted by CO2 laser helps prevention and treatment of functional alterations caused by ankyloglossia. Int. J. Orofac. Myol. 2004, 30, 64–71. [Google Scholar] [CrossRef]
- McKenzie, A.L. Lasers in Surgery and Medicine. Phys. Med. Biol. 1984, 29, 619–641. [Google Scholar] [CrossRef]
- Eming, S.A.; Martin, P.; Tomic-Canic, M. Wound repair and regeneration: Mechanisms, signaling, and translation. Sci. Transl. Med. 2014, 265, 3–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gebauer, D.; Constantinescu, M.A. Effect of surgical laser on collagen-rich tissue. Handchir. Mikrochir. Plast. Chir. 2000, 32, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Yu, W.; Naim, J.O.; Lanzafame, R.J. The effect of photoirradiation on the secretion of TGF-β PDGF and bFGF from fibroblasts in vitro. Lasers Surg. Med. 1994, 6, 8. [Google Scholar]
- De Santis, D.; Gerosa, R.; Graziani, P.F.; Zanotti, G.; Rossini, N.; Castellani, R.; Bissolotti, G.; Chiarini, L.; Nocini, P.F.; Bertossi, D. Lingual frenectomy: A comparison between the conventional surgical and laser procedure. Minerva Stomatol. 2013, 62 (Suppl. 1), 45–53. [Google Scholar]
- Yadav, R.K.; Verma, U.P.; Sajjanhar, I.; Tiwari, R. Frenectomy with conventional scalpel and Nd:YAG laser technique: A comparative evaluation. J. Indian Soc. Periodontolol. 2019, 23, 48–52. [Google Scholar] [CrossRef]
- Sarmadi, R.; Gabre, P.; Thor, A. Evaluation of upper labial frenectomy: A randomized, controlled, comparative study of conventional scalpel technique and Er:YAG laser technique. Clin. Exp. Dent. Res. 2021, 7, 522–530. [Google Scholar] [CrossRef]
- Mazzoni, A.; Navarro, R.S.; Fernandes, K.P.S.; Horliana, A.C.R.T.; Mesquita-Ferrari, R.A.; Motta, P.B.; Silva, T.; Gomes, A.; Martimbianco, A.L.C.; Sobral, A.P.T.; et al. Evaluation of the effects of high-level laser and electrocautery in lingual frenectomy surgeries in infants: Protocol for a blinded randomised controlled clinical trial. BMJ Open 2021, 11, e050733. [Google Scholar] [CrossRef] [PubMed]
- Shang, J.; Han, M.; Sun, J.; Xu, D.; Qu, W. Comparative Study on the Treatment of Ankyloglossia by Using Er:YAG Laser or Traditional Scalpel. J. Craniofacial Surg. 2021, 32, 792–795. [Google Scholar] [CrossRef]
- Brignardello-Petersen, R. Use of lasers seems to result in a small decrease in postoperative complications after labial frenectomy compared with scalpels. J. Am. Dent. Assoc. 2020, 151, 42. [Google Scholar] [CrossRef] [PubMed]
- Protasio, A.C.R.; Galvao, E.L.; Falci, S.G.M. Laser Techniques or Scalpel Incision for Labial Frenectomy: A Meta-analysis. J. Maxillofac. Oral Surg. 2019, 18, 490–499. [Google Scholar] [CrossRef] [PubMed]
- Nammour, S. Laser-Assisted Tongue-Tie Frenectomy for Orthodontic Purpose: To Suture or Not to Suture? Photobiomodulation Photomed. Laser Surg. 2019, 37, 381–382. [Google Scholar] [CrossRef]
- De Araujo, J.G.L.; Araujo, E.M.D.S.; Rodrigues, F.C.N.; Paschoal, M.A.B.; Lago, A.D.N. High Power Laser and Photobiomodulation in Oral Surgery: Case Report. J. Lasers Med. Sci. 2019, 10, 75–78. [Google Scholar] [CrossRef]
- Khosraviani, F.; Ehsani, S.; Fathi, M.; Saberi-Demneh, A. Therapeutic effect of laser on pediatric oral soft tissue problems: A systematic literature review. Lasers Med. Sci. 2019, 34, 1735–1746. [Google Scholar] [CrossRef] [PubMed]
- Viet, D.H.; Ngoc, V.T.N.; Anh, L.Q.; Le Hoang Son, D.T.C.; Phung Thi Thu Ha, T.C. Reduced Need of Infiltration Anesthesia Accompanied With Other Positive Outcomes in Diode Laser Application for Frenectomy in Children. J. Lasers Med. Sci. 2019, 10, 92–96. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Description | Points |
|---|---|---|
| CSR | Merged incision margins | 6 |
| Incision margins in contact | 3 | |
| Visible distance between incision margins | 0 | |
| CSH | Absence of fibrin on the incision margins | 2 |
| Presence of fibrin on the incision margins | 1 | |
| Bleeding at the incision margins | 0 | |
| CSI | Absence of redness along the incision length | 2 |
| Redness involving <50% of the incision length | 1 | |
| Redness involving >50% of the incision length and/or pronounced swelling | 0 | |
| Maximum total score: 10 | ||
| Patient | Age | Sex | Kotlow’s Class | Length of the Operation (Minutes) | CSR | CSH | CSI | EHS |
|---|---|---|---|---|---|---|---|---|
| 1 | 8 | F | III | 38 | 6 | 2 | 2 | 10 |
| 2 | 9 | F | IV | 36 | 6 | 2 | 1 | 9 |
| 3 | 9 | F | III | 41 | 6 | 1 | 2 | 9 |
| 4 | 10 | M | IV | 45 | 3 | 1 | 1 | 5 |
| 5 | 10 | M | III | 47 | 3 | 0 | 1 | 4 |
| 6 | 9 | M | III | 48 | 6 | 2 | 1 | 9 |
| 7 | 11 | F | IV | 36 | 0 | 0 | 0 | 0 |
| 8 | 11 | M | IV | 38 | 6 | 1 | 1 | 8 |
| 9 | 8 | F | III | 34 | 3 | 1 | 0 | 4 |
| 10 | 10 | F | III | 39 | 6 | 2 | 2 | 10 |
| 11 | 9 | M | IV | 37 | 6 | 1 | 2 | 9 |
| 12 | 10 | F | III | 39 | 3 | 2 | 1 | 6 |
| 13 | 9 | F | IV | 47 | 3 | 1 | 2 | 6 |
| 14 | 10 | F | IV | 44 | 6 | 2 | 1 | 9 |
| 15 | 11 | M | III | 49 | 0 | 0 | 0 | 0 |
| 16 | 12 | M | III | 52 | 0 | 0 | 0 | 0 |
| 17 | 9 | F | IV | 39 | 3 | 1 | 0 | 4 |
| 18 | 9 | M | III | 37 | 3 | 1 | 2 | 6 |
| 19 | 12 | M | IV | 46 | 6 | 2 | 2 | 10 |
| 20 | 8 | F | III | 29 | 3 | 2 | 2 | 7 |
| 21 | 9 | M | III | 37 | 6 | 2 | 2 | 10 |
| 22 | 12 | F | IV | 41 | 3 | 1 | 1 | 5 |
| 23 | 8 | F | III | 33 | 3 | 2 | 1 | 6 |
| 24 | 10 | M | IV | 43 | 3 | 2 | 2 | 7 |
| 25 | 9 | M | III | 46 | 6 | 1 | 2 | 9 |
| 26 | 10 | M | III | 47 | 3 | 1 | 1 | 5 |
| 27 | 11 | F | IV | 41 | 6 | 2 | 2 | 10 |
| 28 | 8 | F | III | 40 | 6 | 2 | 2 | 10 |
| 29 | 12 | M | IV | 38 | 3 | 2 | 1 | 6 |
| Patient | Age | Sex | Kotlow’s Class | Length of the Operation (Minutes) | CSR | CSH | CSI | EHS |
|---|---|---|---|---|---|---|---|---|
| 1 | 9 | F | IV | 16 | 6 | 2 | 2 | 10 |
| 2 | 9 | F | III | 19 | 6 | 2 | 2 | 10 |
| 3 | 10 | M | III | 14 | 6 | 2 | 2 | 10 |
| 4 | 8 | M | IV | 19 | 6 | 2 | 2 | 10 |
| 5 | 12 | F | III | 18 | 6 | 2 | 2 | 10 |
| 6 | 12 | M | IV | 18 | 6 | 1 | 1 | 8 |
| 7 | 10 | F | III | 13 | 6 | 2 | 2 | 10 |
| 8 | 11 | F | III | 17 | 6 | 2 | 2 | 10 |
| 9 | 9 | F | IV | 16 | 6 | 2 | 2 | 10 |
| 10 | 9 | M | IV | 19 | 6 | 2 | 1 | 9 |
| 11 | 8 | M | III | 18 | 6 | 1 | 2 | 9 |
| 12 | 10 | F | IV | 22 | 6 | 2 | 2 | 10 |
| 13 | 9 | F | III | 18 | 6 | 2 | 2 | 10 |
| 14 | 11 | M | III | 17 | 6 | 2 | 2 | 10 |
| 15 | 11 | F | IV | 19 | 6 | 2 | 2 | 10 |
| 16 | 9 | M | IV | 23 | 6 | 2 | 2 | 10 |
| 17 | 8 | M | III | 21 | 6 | 1 | 2 | 9 |
| 18 | 9 | F | III | 13 | 6 | 2 | 2 | 10 |
| 19 | 10 | M | IV | 15 | 6 | 2 | 1 | 9 |
| 20 | 11 | M | III | 17 | 6 | 2 | 1 | 9 |
| 21 | 10 | F | IV | 21 | 6 | 2 | 2 | 10 |
| 22 | 12 | F | III | 17 | 6 | 2 | 2 | 10 |
| 23 | 12 | F | IV | 20 | 6 | 2 | 2 | 10 |
| 24 | 10 | M | III | 23 | 6 | 1 | 1 | 8 |
| 25 | 9 | M | IV | 18 | 6 | 2 | 2 | 10 |
| 26 | 9 | F | III | 15 | 6 | 2 | 2 | 10 |
| 27 | 10 | F | IV | 17 | 6 | 2 | 2 | 10 |
| 28 | 9 | M | III | 18 | 6 | 2 | 1 | 9 |
| 29 | 8 | M | III | 21 | 6 | 2 | 2 | 10 |
| 30 | 8 | M | IV | 14 | 6 | 1 | 1 | 8 |
| 31 | 12 | F | III | 17 | 6 | 2 | 2 | 10 |
| 32 | 11 | F | IV | 18 | 6 | 2 | 2 | 10 |
| Variable | Group A | Group B | p-Value |
|---|---|---|---|
| Gender (M/F) | 14/15 | 15/17 | 0.91 |
| Age (±SD) | 10 ± 1.28 | 9.8 ± 1.3 | 0.73 |
| Kotlow’s class (III/IV) | 16/13 | 17/15 | 0.87 |
| Time of the operation (min) (±SD) | 41 ± 12 | 18 ± 5 | <0.001 |
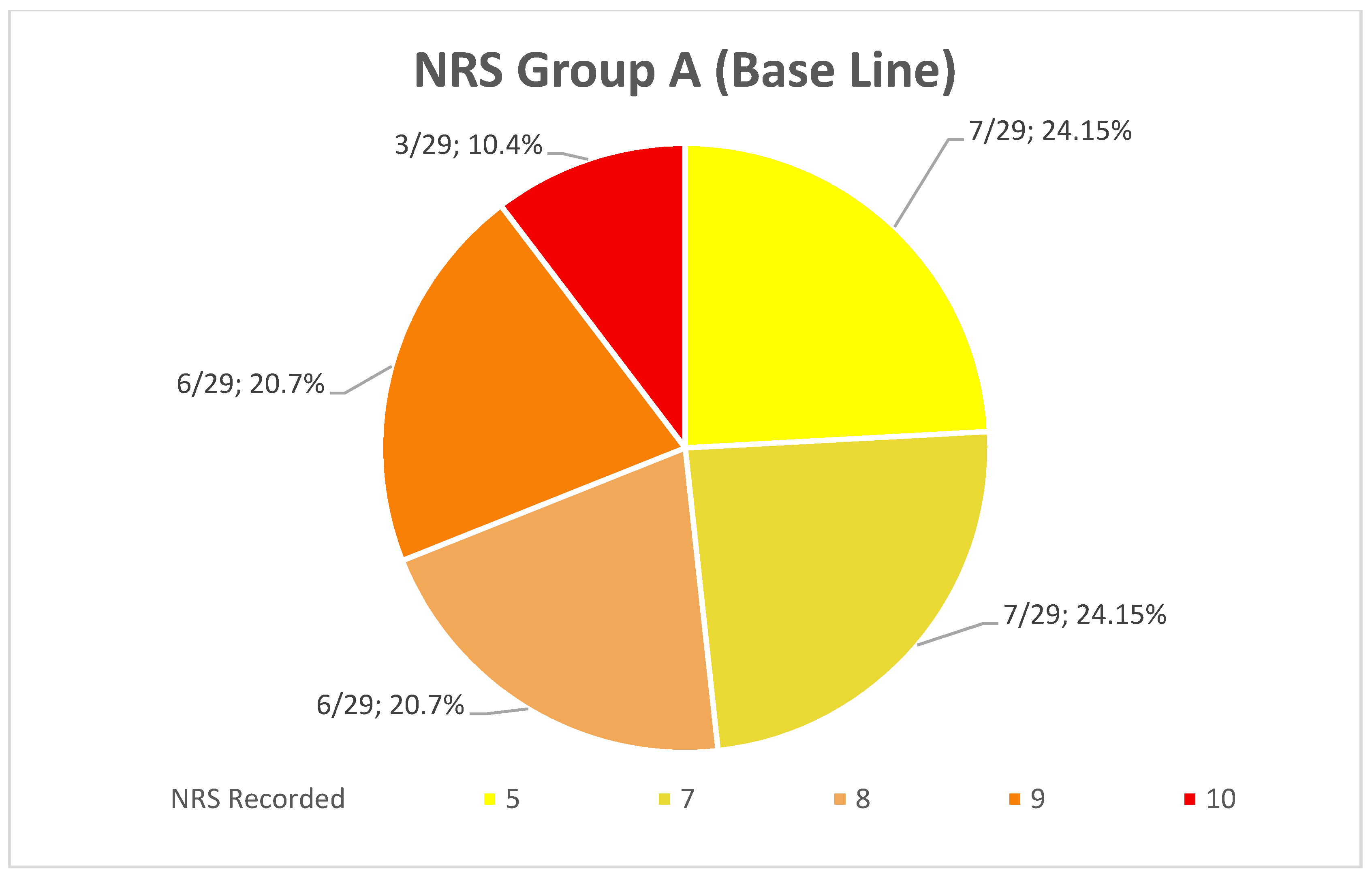
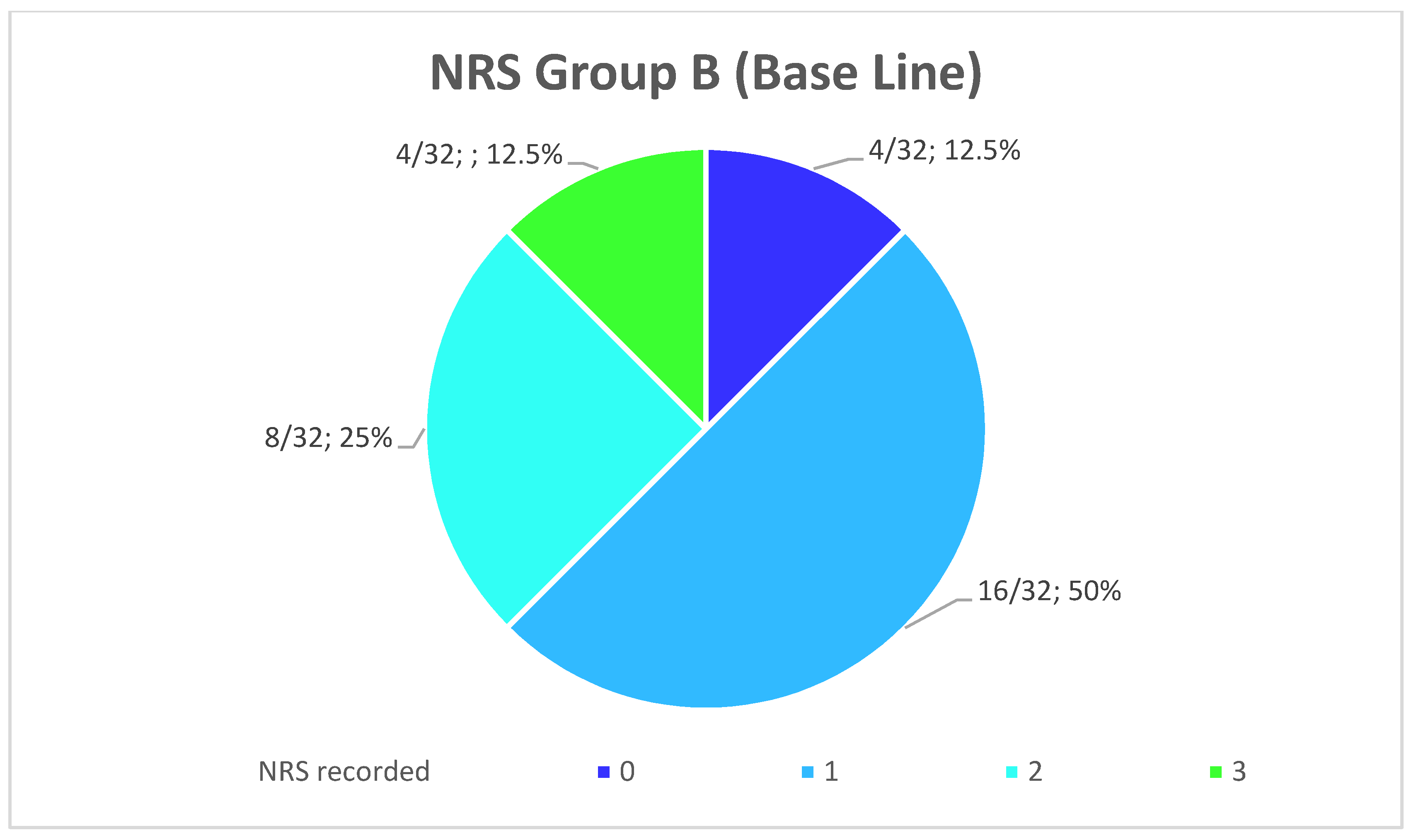
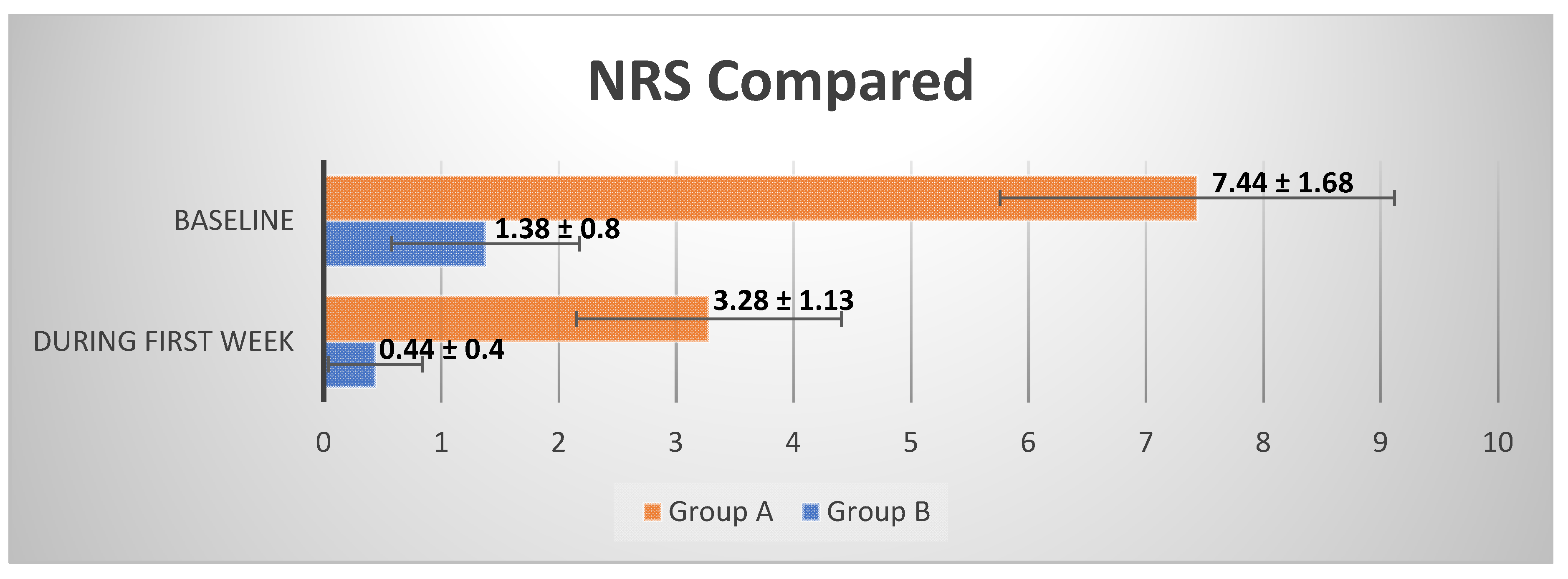
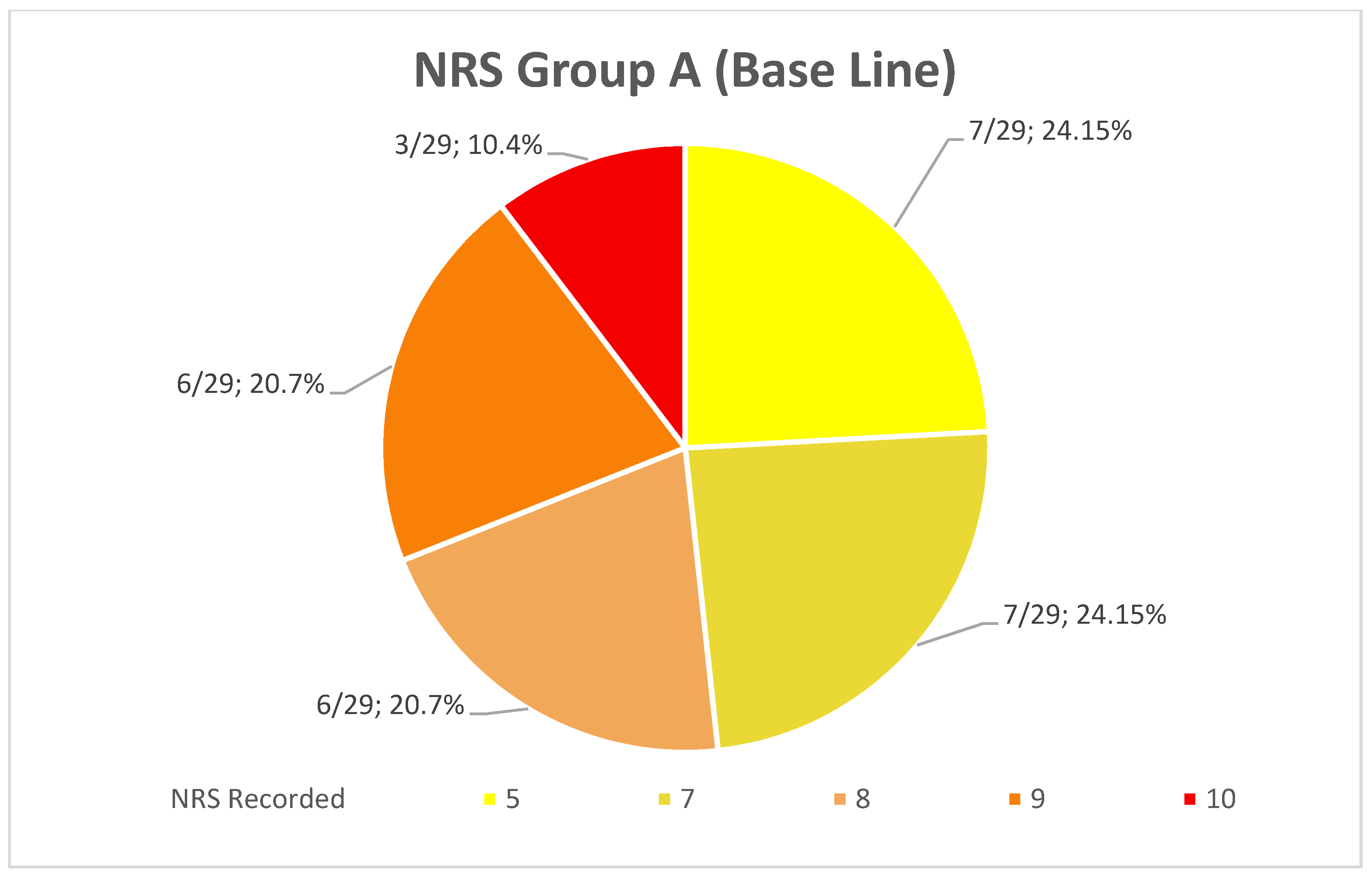
| NRS (Baseline) (±SD) | 7.44 ± 1.68 | 1.38 ± 0.8 | <0.001 |
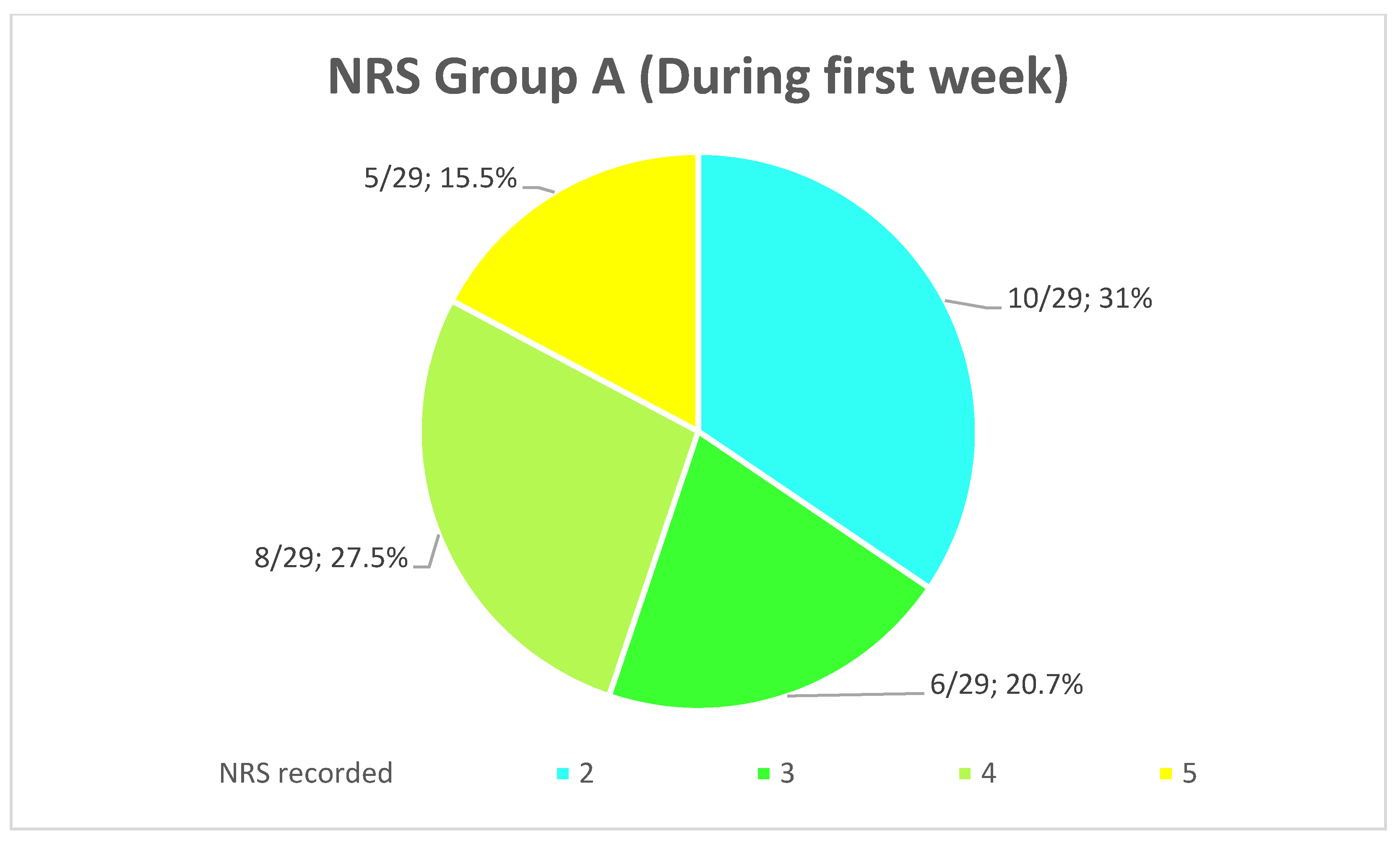
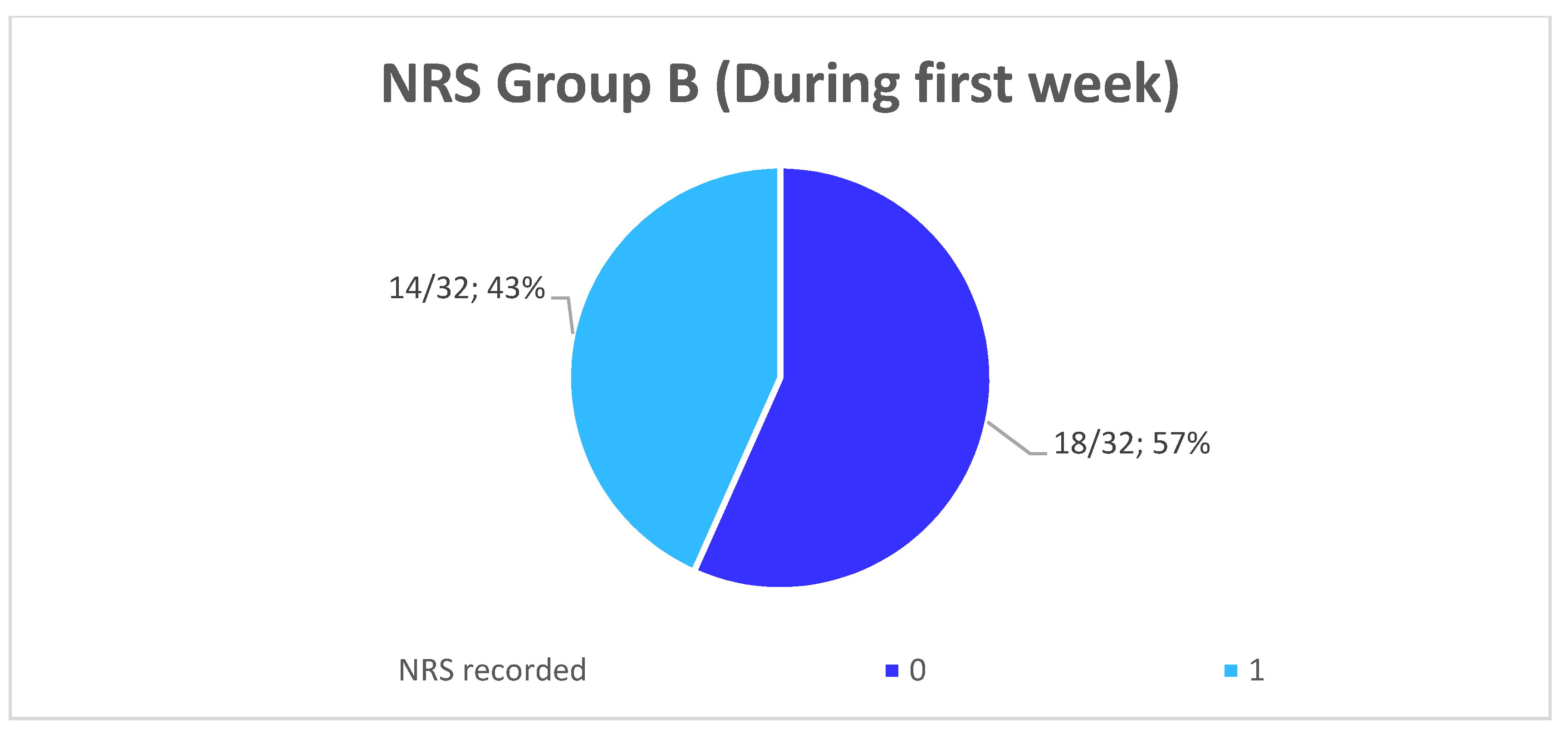
| NRS (First week) (±SD) | 3.28 ± 1.13 | 0.44 ± 0.4 | <0.001 |
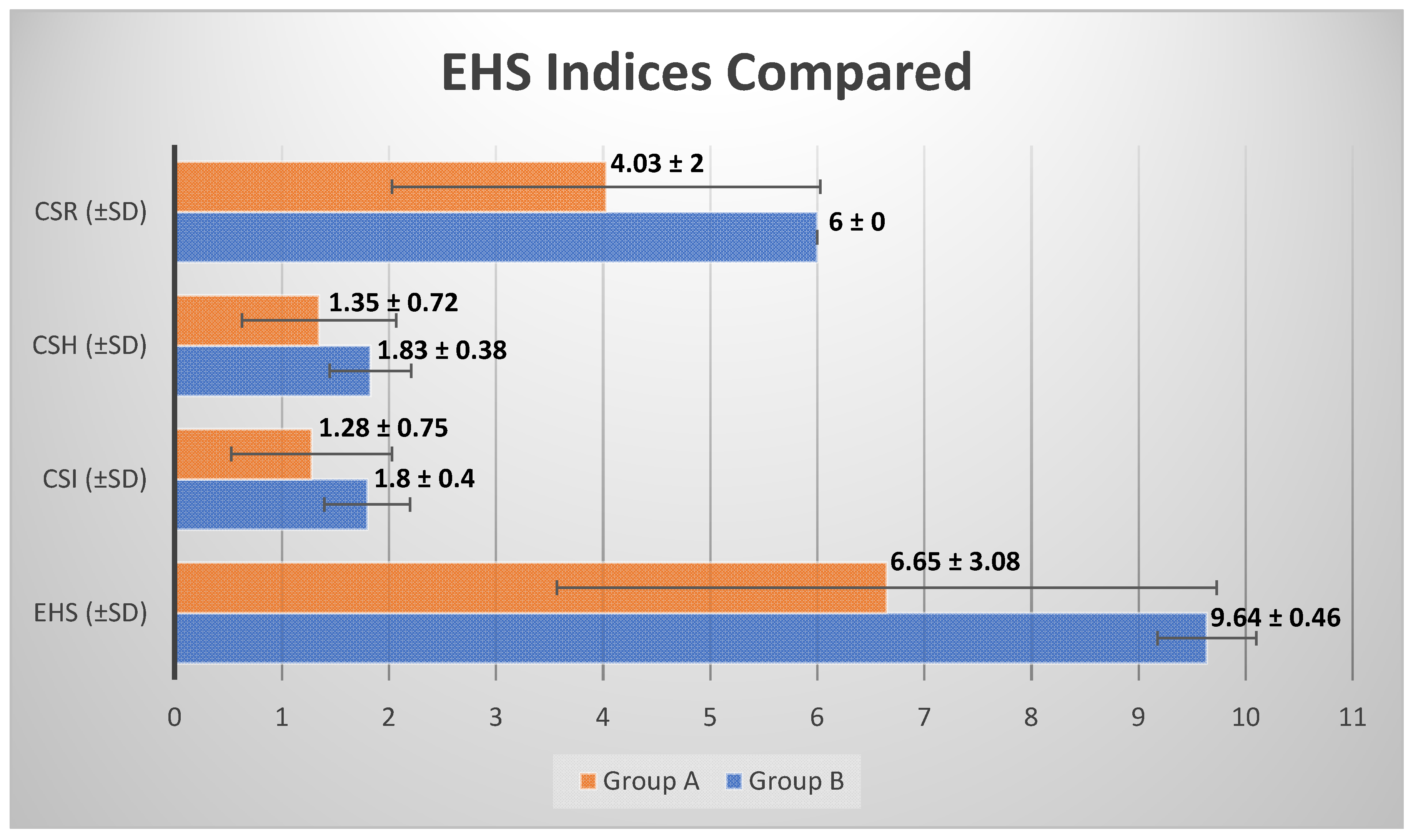
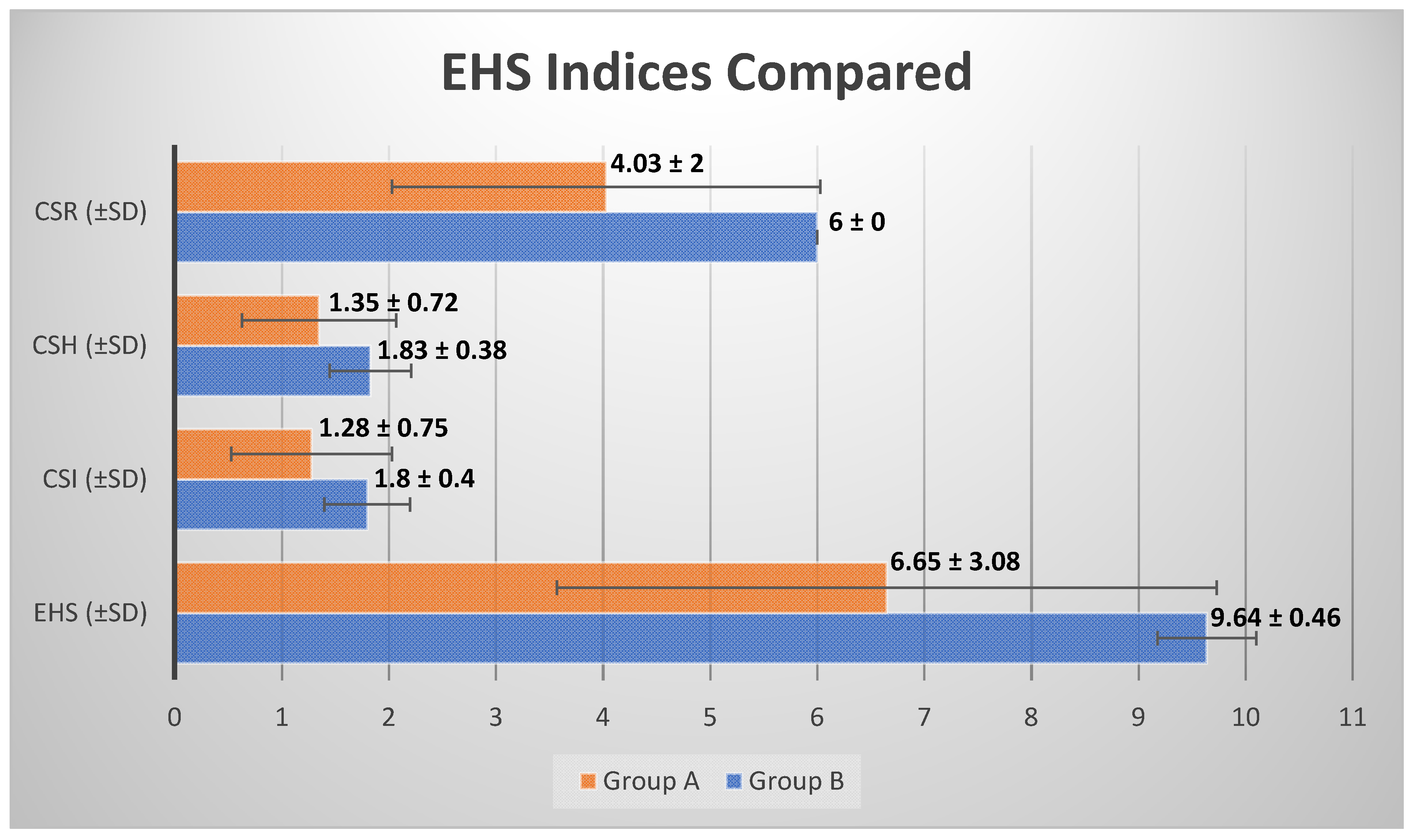
| CSR (±SD) | 4.03 ± 2 | 6 ± 0 | <0.001 |
| CSH (±SD) | 1.35 ± 0.72 | 1.83 ± 0.38 | 0.0018 |
| CSI (±SD) | 1.28 ± 0.75 | 1.8 ± 0.4 | 0.0014 |
| EHS (±SD) | 6.65 ± 3.08 | 9.64 ± 0.46 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tancredi, S.; De Angelis, P.; Marra, M.; Lopez, M.A.; Manicone, P.F.; Passarelli, P.C.; Romeo, A.; Grassi, R.; D'Addona, A. Clinical Comparison of Diode Laser Assisted “v-Shape Frenectomy” and Conventional Surgical Method as Treatment of Ankyloglossia. Healthcare 2022, 10, 89. https://doi.org/10.3390/healthcare10010089
Tancredi S, De Angelis P, Marra M, Lopez MA, Manicone PF, Passarelli PC, Romeo A, Grassi R, D'Addona A. Clinical Comparison of Diode Laser Assisted “v-Shape Frenectomy” and Conventional Surgical Method as Treatment of Ankyloglossia. Healthcare. 2022; 10(1):89. https://doi.org/10.3390/healthcare10010089
Chicago/Turabian StyleTancredi, Sileno, Paolo De Angelis, Mario Marra, Michele Antonio Lopez, Paolo Francesco Manicone, Pier Carmine Passarelli, Antonino Romeo, Roberta Grassi, and Antonio D'Addona. 2022. "Clinical Comparison of Diode Laser Assisted “v-Shape Frenectomy” and Conventional Surgical Method as Treatment of Ankyloglossia" Healthcare 10, no. 1: 89. https://doi.org/10.3390/healthcare10010089
APA StyleTancredi, S., De Angelis, P., Marra, M., Lopez, M. A., Manicone, P. F., Passarelli, P. C., Romeo, A., Grassi, R., & D'Addona, A. (2022). Clinical Comparison of Diode Laser Assisted “v-Shape Frenectomy” and Conventional Surgical Method as Treatment of Ankyloglossia. Healthcare, 10(1), 89. https://doi.org/10.3390/healthcare10010089