
Effect of Paprika Xanthophyll Supplementation on Cognitive Improvement in a Multitasking Exercise: A Pilot Study for Middle-Aged and Older Adults


Abstract
:1. Introduction
2. Materials and Methods
2.1. Purpose
2.2. Study Design
2.2.1. Participants
2.2.2. Experimental Design
- Supplement; A commercial supplement (“OXYDRAIVE”; Glico Nutrition Co., Ltd., Osaka, Japan) containing PX extracted from natural red bell pepper was used in this study. Xanthophyll-containing gelatin capsules (each containing 9 mg of seven types of xanthophylls, including 5 mg of capsanthin and 0.5 mg/g of β-cryptoxanthin), were used in study 2. All participants took the capsules orally every morning with meals for four weeks. PX contains seven xanthophylls (capsanthin, cucurbitaxanthin A, β-cryptoxanthin, zeaxanthin, capsorubin, crypto-capsin, capsanthin, and 3,6-epoxide).
- Multitasking exercise; The multitasking exercise used in this study was “Co-kara exercise: CE, which was devised as a dementia-prevention exercise in S city, Osaka. CE consists of several kinds of basic movements (blocks), such as upper-limb exercises and foot-stomping exercises, which are combined in four beats of two repetitions each, with changes in rhythm and direction. The exercise time (CE) in study 1 was 15 min, while that in study 2 was 30 min.
2.3. Measurements
2.3.1. Measurements for Study 1
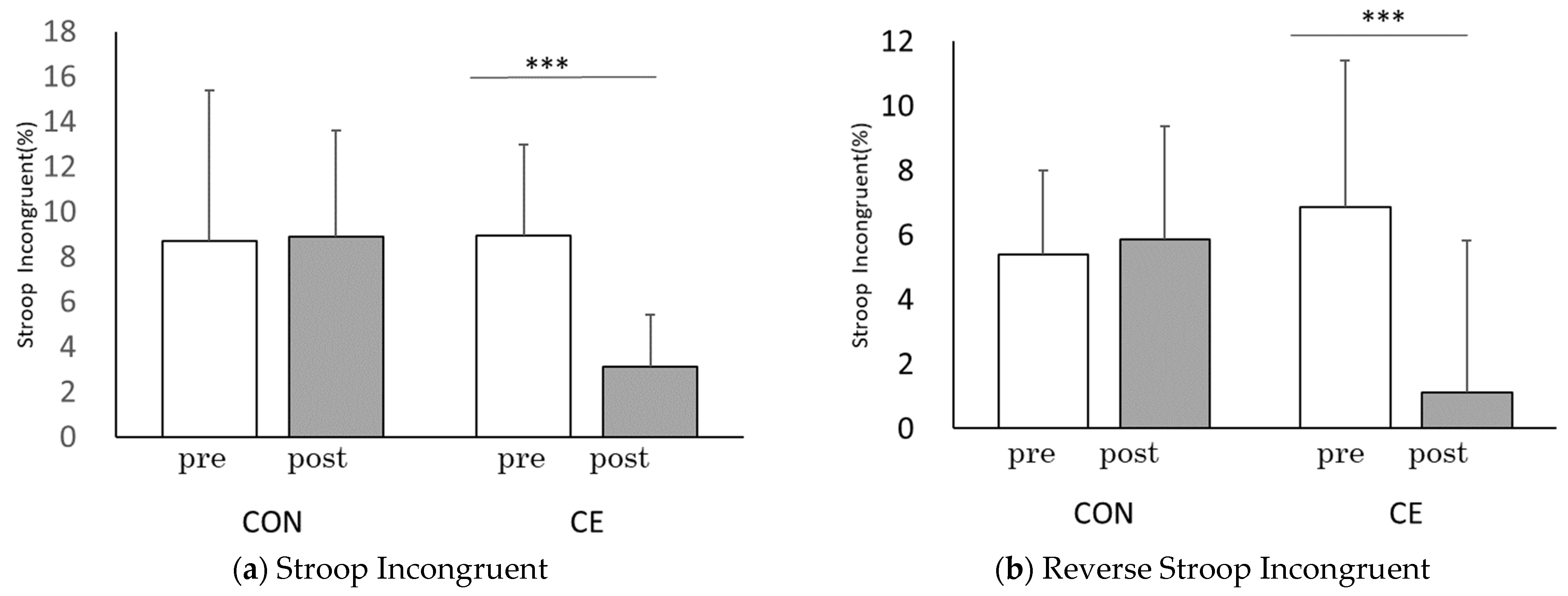
- Stroop Test; The New Stroop Test II [25], which can collectively measure two indices, ST interference and reverse ST interference, was used to assess cognitive function. This test involves the following two tasks: (1) identification of the color represented by a word and the color in which the letters are written and (2) identification of options showing inconsistency between the color of the letters and the meaning implied by the word (ST interference). The ability to handle this ST interference is calculated as the difference in performance between the incongruent and congruent tasks and is evaluated as an executive function. In study 1, we compared the ST interference rate with the reverse ST interference rate.
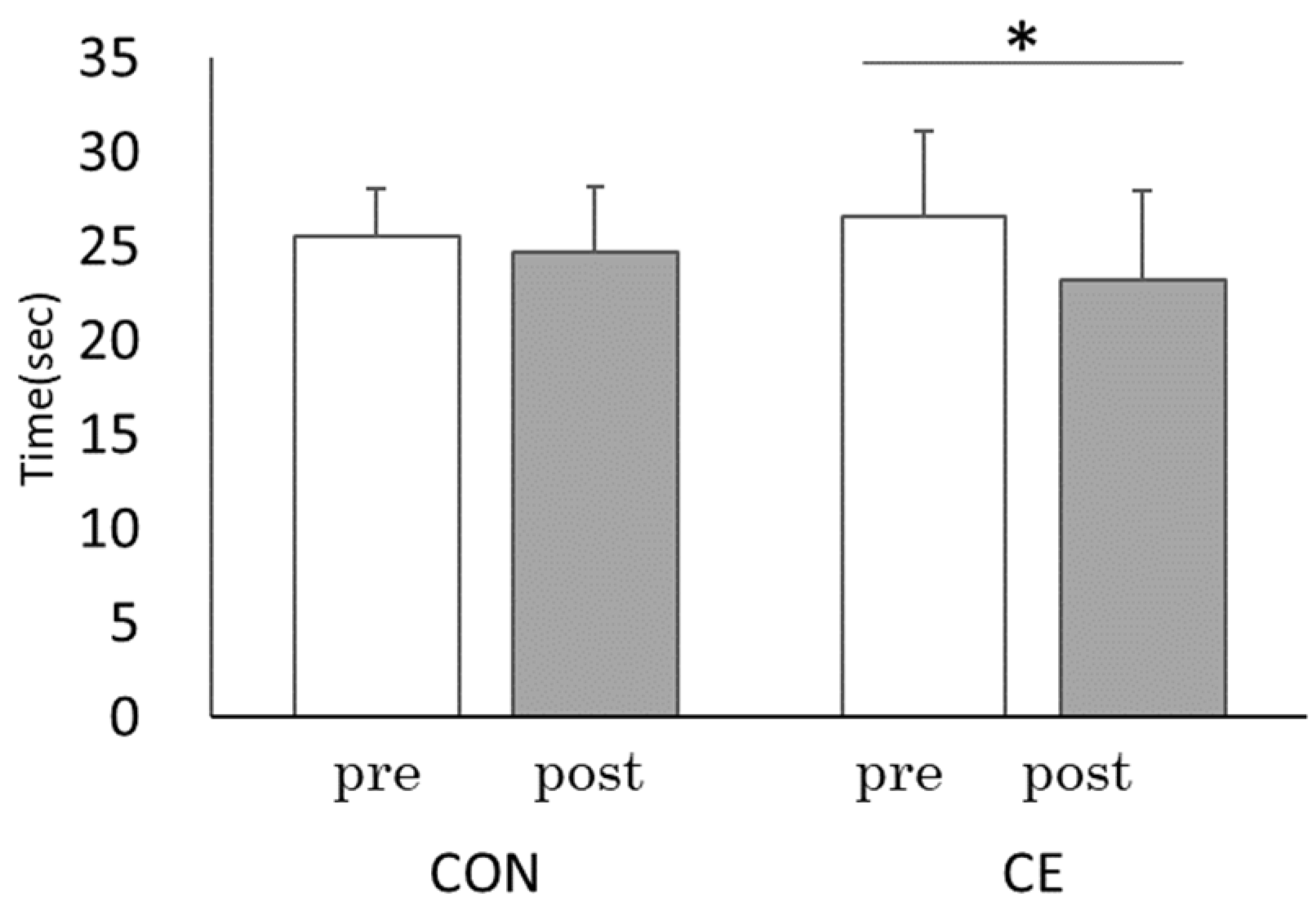
- Trail-making test; The TMT was used to assess cognitive function [26]. The TMT consists of the following two parts: Part A (TMT-A) consists of numbers only, in the order of “1–25,” while Part B (TMT-B) in the Japanese version consists of numbers and Hiragana in Japanese, in the order of “1-A-2-I-3-U....”. The time to complete each part of the TMT was recorded, and raw time scores were used as the dependent variables. The TMT is a well-established neuropsychological assessment method that can comprehensively evaluate attention, working memory, spatial exploration, and processing speed. In particular, the TMT-B can be used to characterize attentional conversion ability and executive function. The TMT-B has been used in many studies [27,28,29]. In study 1, only the TMT-B was used; practice sessions were conducted to avoid the influence of learning effects in the TMT.
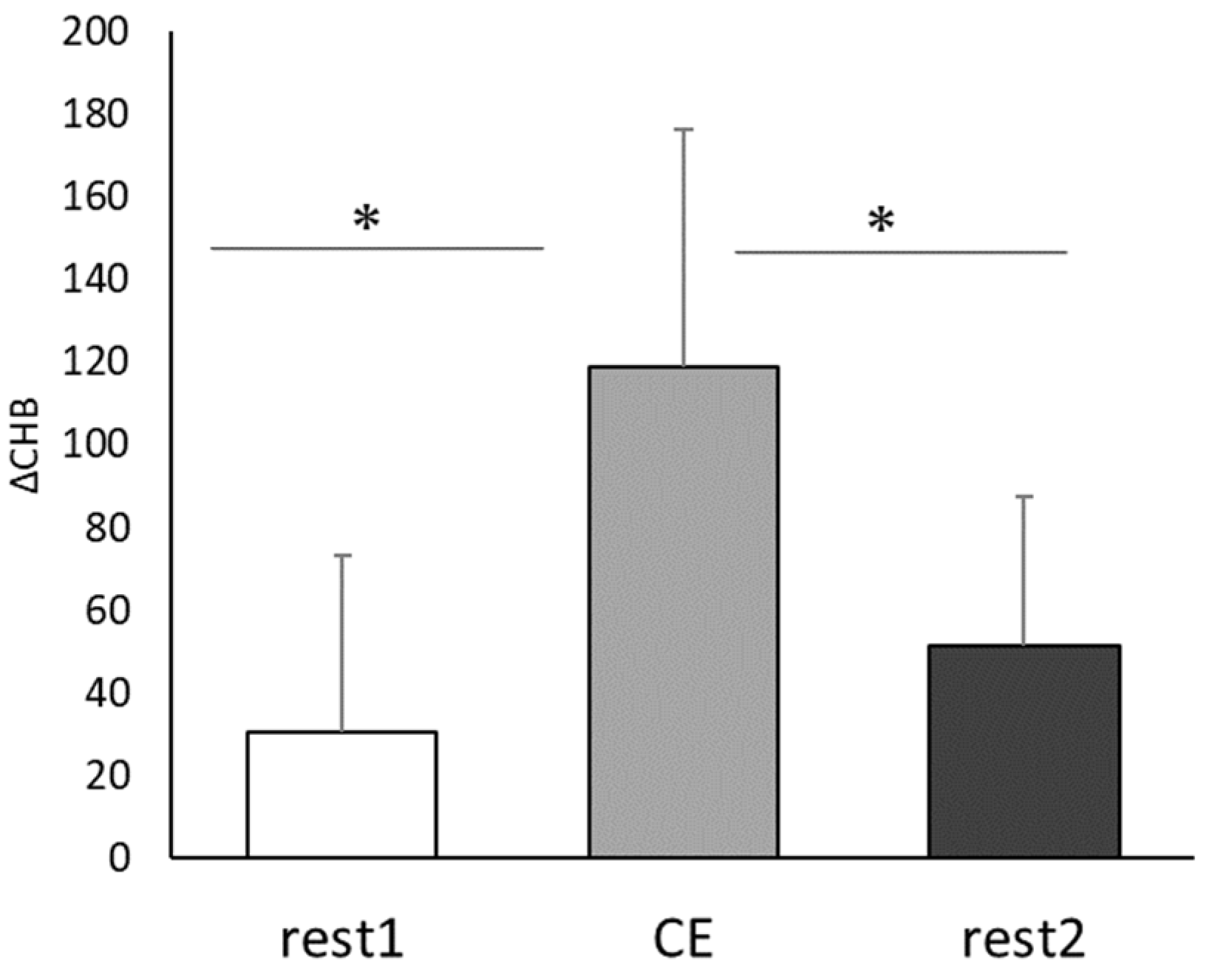
- Near-infrared Spectroscopy; Changes in oxygenated, deoxygenated, and total hemoglobin in blood in the frontal region of the brain during each trial were detected using the double channel of a near-infrared oxygenation monitor (NIRO-200; Hamamatsu Photonics KK, Hamamatsu, Japan). The NIRO probe was fixed to both sides of the forehead with double-sided tape and then firmly fixed with an elastic bandage to prevent it from floating. In this study, the mean value per minute of the change in total hemoglobin, which is the sum of the measurements of oxygenated and deoxygenated hemoglobin obtained from NIRO, was used as an index.
2.3.2. Measurements for Study 2
- TMT-A and TMT-B; Cognitive function tests (TMT-A, B) were conducted the following four times: before the first CE (before/pre), after CE (before/post), and before and after CE conducted four weeks later (four weeks/pre and four weeks/post, respectively). As in study 1, sufficient practice sessions were conducted to avoid the influence of learning effects in TMT. The TMT procedure was conducted according to the Japanese version of the manual [27] as follows: the participants were administered the practice questions for part A; after they completely understood part A, they were asked to attempt the questions from the actual part A. After completing the questions from part A, they were administered the practice questions for part B, and after they had understood part B, they were asked to attempt the questions from the actual part B, which was the same version as part A. After the CE, another version of the TMT was conducted in the same order (part A followed by part B). In this assessment, the practice questions were not administered. After four weeks of PX supplementation, the entire TMT procedure, including the order of the tests and the use of practice questions only for the pre-CE assessments, was repeated with two additional versions of the TMT.
- Standard questionnaire survey; The questionnaire consisted of 16 items (Table 2), and it evaluated medical history and smoking habits, exercise habits, and dietary habits among the items listed in the specific health checkup specified in the standards for the implementation of specific health checkups and specific health guidance (2007, Ministry of Health, Labour and Welfare, Ordinance No. 157) [30]. Questionnaires were distributed at the first survey and collected four weeks later. Responses were based on a two-response model (yes/no).
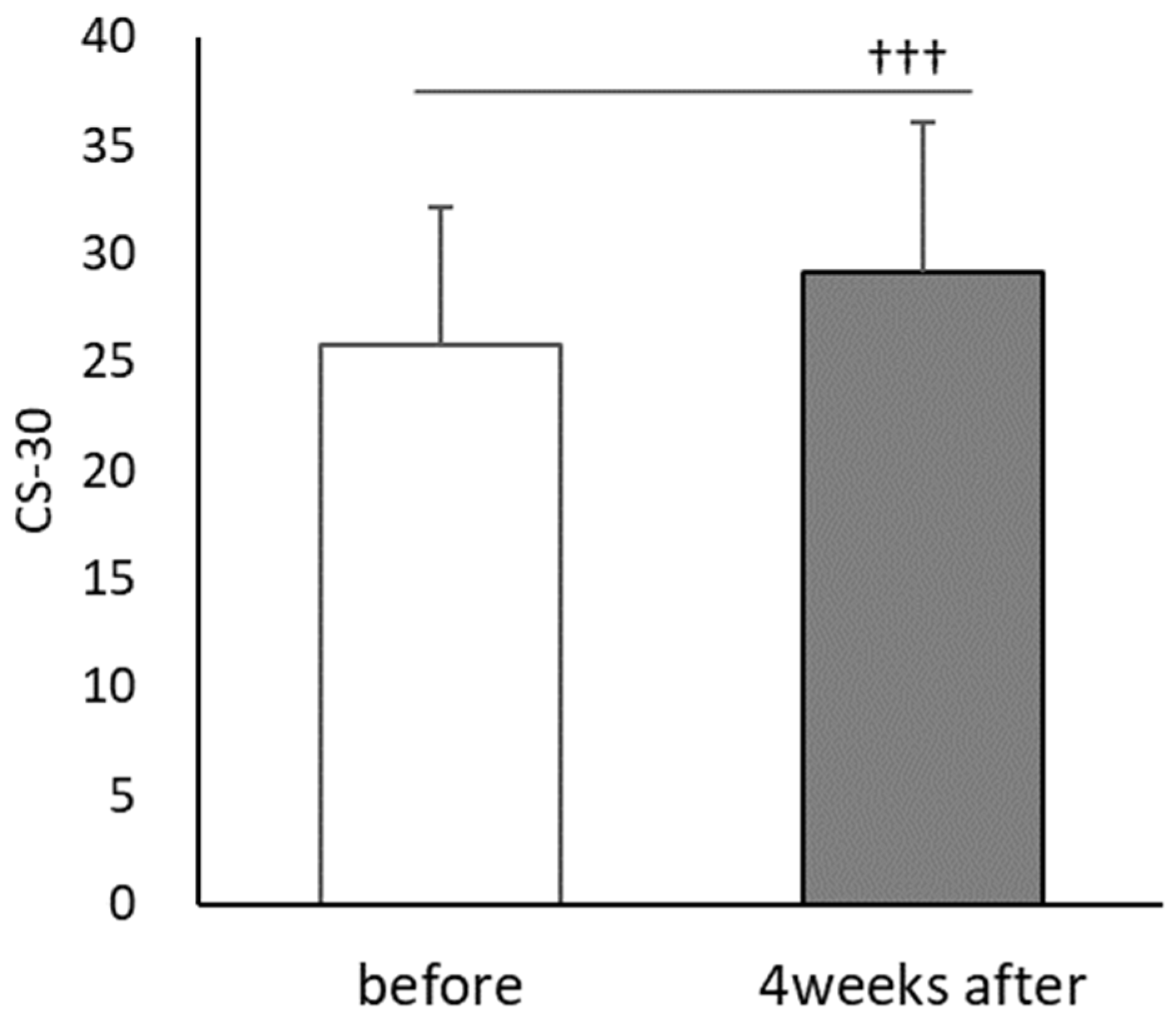
- CS-30; The CS-30 was determined as an index of lower limb muscle strength and exercise tolerance. The CS-30 has been shown to indicate exercise tolerance in patients with chronic respiratory diseases, as well as an index of lower limb muscle strength, and can be used to estimate the amount of physical activity by the number of steps commensurate with the exercise tolerance [31]. CS-30 evaluations were performed before and once after four weeks of PX supplementation.
- Heart rate; Heart rate measurement data were obtained using a wearable activity monitor equipped with an optical heart rate sensor (Huawei BAND 4: Huawei Technologies Japan K.K., Tokyo, Japan). The heart rate during the experiment, at rest, after CS-30 evaluation, during CE, and after CE was measured using the wearable activity monitor.
2.4. Statistical Analysis
2.5. Ethics
3. Result
3.1. Results of Study 1
3.2. Results of Study 2
3.2.1. Attributes of the Participants
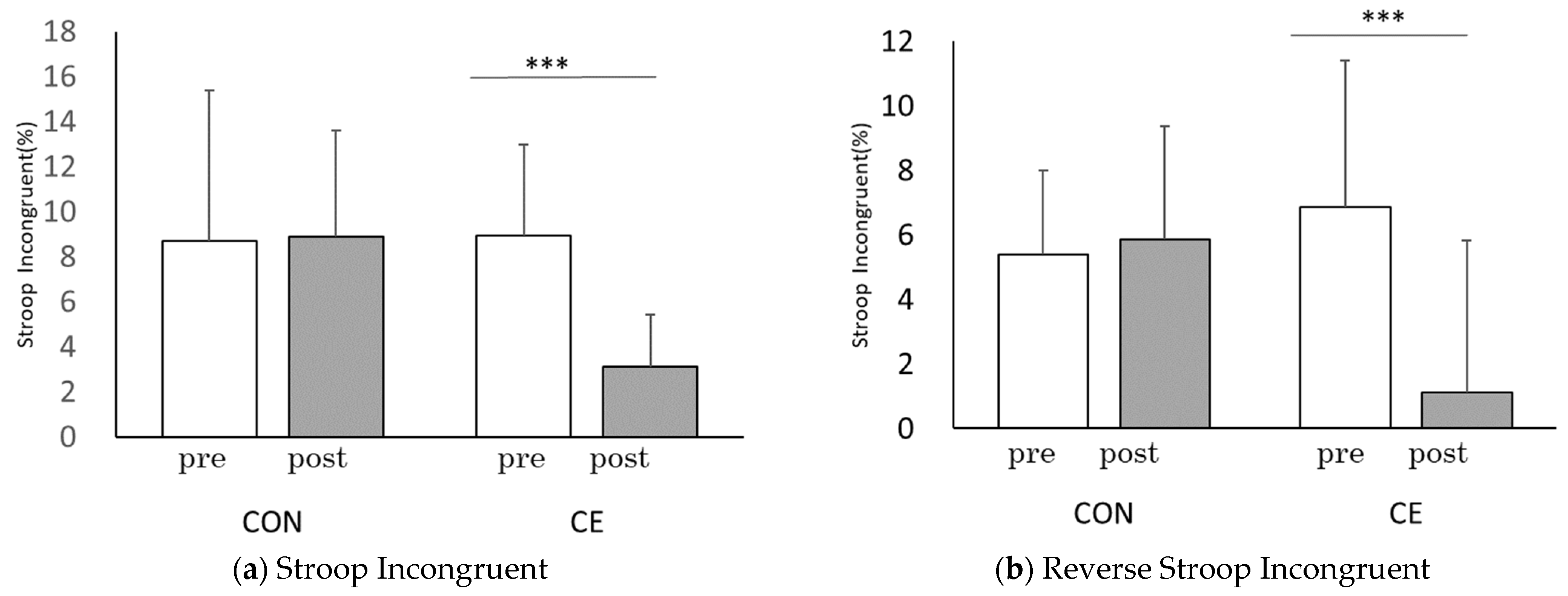
3.2.2. Cognitive Task
3.2.3. CS-30 and Heart Rate
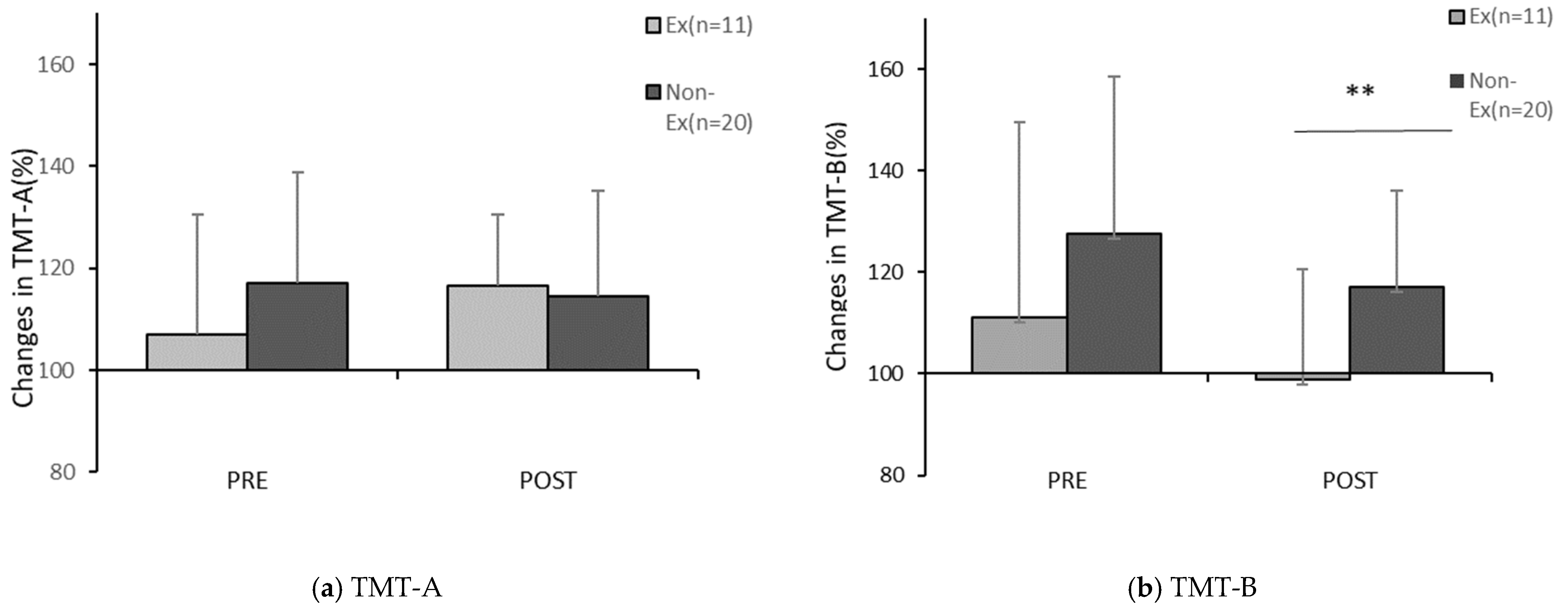
3.2.4. Changes in the TMT Score before and after PX Supplementation
4. Discussion
4.1. Synergistic Effects of Multitasking Exercise and PX
4.2. Effect of PX Supplementation
4.3. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Weinstein, A.M.; Voss, M.W.; Prakash, R.S.; Chaddock, L.; Szabo, A.; White, S.M.; Wojcicki, T.R.; Mailey, E.; McAuley, E.; Kramer, A.F.; et al. The association between aerobic fitness and executive function is mediated by prefrontal cortex volume. Brain Behav. Immun. 2012, 26, 811–819. [Google Scholar] [CrossRef] [Green Version]
- Cheng, S.T. Cognitive Reserve and the Prevention of Dementia: The Role of Physical and Cognitive Activities. Curr. Psychiatry Rep. 2016, 18, 85. [Google Scholar] [CrossRef] [Green Version]
- Yanagisawa, H.; Dan, I.; Tsuzuki, D.; Kato, M.; Okamoto, M.; Kyutoku, Y.; Soya, H. Acute moderate exercise elicits increased dorsolateral prefrontal activation and improves cognitive performance with Stroop test. Neuroimage 2010, 50, 1702–1710. [Google Scholar] [CrossRef] [PubMed]
- Hyodo, K.; Dan, I.; Suwabe, K.; Kyutoku, Y.; Yamada, Y.; Akahori, M.; Byun, K.; Kato, M.; Soya, H. Acute moderate exercise enhances compensatory brain activation in older adults. Neurobiol. Aging 2012, 33, 2621–2632. [Google Scholar] [CrossRef]
- Byun, K.; Hyodo, K.; Suwabe, K.; Ochi, G.; Sakairi, Y.; Kato, M.; Dan, I.; Soya, H. Positive effect of acute mild exercise on executive function via arousal-related prefrontal activations: An fNIRS study. Neuroimage 2014, 98, 336–345. [Google Scholar] [CrossRef]
- Satoh, M. The Effectiveness and Its Mechanism of Physical Exercise to Dementia. Jpn. J. Rehabil. Med. 2018, 55, 658–663. [Google Scholar] [CrossRef]
- Satoh, M.; Ogawa, J.; Tokita, T.; Nakaguchi, N.; Nakao, K.; Kida, H.; Tomimoto, H. The effects of physical exercise with music on cognitive function of elderly people: Mihama-Kiho project. PLoS ONE 2014, 9, e95230. [Google Scholar] [CrossRef]
- Suzuki, T.; Shimada, H.; Makizako, H.; Doi, T.; Yoshida, D.; Tsutsumimoto, K.; Anan, Y.; Uemura, K.; Lee, S.; Park, H. Effects of multicomponent exercise on cognitive function in older adults with amnestic mild cognitive impairment: A randomized controlled trial. BMC Neurol. 2012, 12, 128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chroboczek, M.; Kostrzewa, M.; Micielska, K.; Grzywacz, T.; Laskowski, R. Effect of Acute Normobaric Hypoxia Exposure on Executive Functions among Young Physically Active Males. J. Clin. Med. 2021, 10, 1560. [Google Scholar] [CrossRef]
- Goodall, S.; Gonzalez-Alonso, J.; Ali, L.; Ross, E.Z.; Romer, L.M. Supraspinal fatigue after normoxic and hypoxic exercise in humans. J. Physiol. 2012, 590, 2767–2782. [Google Scholar] [CrossRef] [Green Version]
- Tsukamoto, H.; Hashimoto, T.; Hirasawa, A.; Hasegawa, H.; Ogoh, S. Effect of hyperventilation-induced decrease in cerebral blood flow on cognitive function in healthy students. Jpn. J. Physiol. Anthropol. 2014, 19, 225–232. (In Japanese) [Google Scholar] [CrossRef]
- Ochi, G.; Yamada, Y.; Hyodo, K.; Suwabe, K.; Fukuie, T.; Byun, K.; Dan, I.; Soya, H. Neural basis for reduced executive performance with hypoxic exercise. Neuroimage 2018, 171, 75–83. [Google Scholar] [CrossRef]
- Ajmani, R.S.; Metter, E.J.; Jaykumar, R.; Ingram, D.K.; Spangler, E.L.; Abugo, O.O.; Rifkind, J.M. Hemodynamic changes during aging associated with cerebral blood flow and impaired cognitive function. Neurobiol. Aging 2000, 21, 257–269. [Google Scholar] [CrossRef]
- Ogoh, S. Relationship between cognitive function and regulation of cerebral blood flow. J Physiol Sci 2017, 67, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Catchlove, S.J.; Macpherson, H.; Hughes, M.E.; Chen, Y.; Parrish, T.B.; Pipingas, A. An investigation of cerebral oxygen utilization, blood flow and cognition in healthy aging. PLoS ONE 2018, 13, e0197055. [Google Scholar] [CrossRef]
- Nakagawa, K.; Kiko, T.; Hatade, K.; Asai, A.; Kimura, F.; Sookwong, P.; Tsuduki, T.; Arai, H.; Miyazawa, T. Development of a high-performance liquid chromatography-based assay for carotenoids in human red blood cells: Application to clinical studies. Anal. Biochem. 2008, 381, 129–134. [Google Scholar] [CrossRef]
- Nakagawa, K.; Kiko, T.; Hatade, K.; Sookwong, P.; Arai, H.; Miyazawa, T. Antioxidant effect of lutein towards phospholipid hydroperoxidation in human erythrocytes. Br. J. Nutr. 2009, 102, 1280–1284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishino, A.; Sugimoto, K.; Sambe, H.; Ichihara, T.; Takaha, T.; Kuriki, T. Effects of Dietary Paprika Xanthophylls on Ultraviolet Light-Induced Skin Damage: A Double-Blind Placebo-Controlled Study. J. Oleo Sci. 2018, 67, 863–869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakagawa, K.; Kiko, T.; Miyazawa, T.; Carpentero Burdeos, G.; Kimura, F.; Satoh, A.; Miyazawa, T. Antioxidant effect of astaxanthin on phospholipid peroxidation in human erythrocytes. Br. J. Nutr. 2011, 105, 1563–1571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyazawa, T.; Nakagawa, K.; Takekoshi, H.; Higuchi, O.; Kato, S.; Kondo, M.; Kimura, F.; Miyazawa, T. Ingestion of Chlorella Reduced the Oxidation of Erythrocyte Membrane Lipids in Senior Japanese Subjects. J. Oleo Sci. 2013, 62, 873–881. [Google Scholar] [CrossRef] [Green Version]
- Ichihara, T.; Nishino, A.; Takaha, T.; Kuriki, T.; Nihei, H.; Yasui, H.; Maoka, T.; Kawamoto, K. Effect of paprika xanthophyll supplementation on oxygen uptake in athletes: A randomized, double-blind, placebo-controlled study. J. Phys. Fit. Sports Med. 2018, 7, 247–252. [Google Scholar] [CrossRef]
- Yamada, M.; Matsuda, T.; Ichihara, T.; Sakamaki-Sunaga, M.M. Effects of Orally Ingested Paprika Xanthophylls on Respiratory Metabolism during Endurance Exercise: Study Protocol for an Interventional Randomised Controlled Trial. Health Sci. J. 2020, 14, 1–5. [Google Scholar] [CrossRef]
- Maeda, H.; Nishino, A.; Maoka, T. Biological Activities of Paprika Carotenoids, Capsanthin and Capsorubin. Adv Exp Med Biol 2021, 1261, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Imazu, H.; Anzai, T.; Denpo, K.; Nagayoshi, M.; Tagai, M.; Hanaie, K.; Takeda, Y.; Wadazumi, T. “Sakai Kokkara Taiso” no Torikumi to Kouka: Taiso no Fukyu niyoru Socialcapital no jousei wo mezashite. Hokenshi J. 2016, 72, 672–677. (In Japanese) [Google Scholar]
- Hakoda, Y.; Megumi, W. The Stroop/Reverse-Stroop TestsII; Toyo Physical: Fukuoka, Japan, 2017. (In Japanese) [Google Scholar]
- Zakzanis, K.K.; Mraz, R.; Graham, S.J. An fMRI study of the Trail Making Test. Neuropsychologia 2005, 43, 1878–1886. [Google Scholar] [CrossRef]
- Brain Function Test Iinkai. Japan Society for Higher Brain Dysfunction. Trail Making Test Japanese Edition (TMT-J); Shinkoh Igaku Shuppansha Co., Ltd: Tokyo, Japan, 2019. (In Japanese) [Google Scholar]
- Cangoz, B.; Karakoc, E.; Selekler, K. Trail Making Test: Normative data for Turkish elderly population by age, sex and education. J. Neurol. Sci. 2009, 283, 73–78. [Google Scholar] [CrossRef]
- Kose, Y.; Ikenaga, M.; Yamada, Y.; Morimura, K.; Takeda, N.; Ouma, S.; Tsuboi, Y.; Yamada, T.; Kimura, M.; Kiyonaga, A.; et al. Timed Up and Go test, atrophy of medial temporal areas and cognitive functions in community-dwelling older adults with normal cognition and mild cognitive impairment. Exp. Gerontol. 2016, 85, 81–87. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare, Seisakunituite. Available online: https://www.mhlw.go.jp/seisakunitsuite/bunya/kenkou_iryou/kenkou/seikatsu/dl/hoken-program2_02.pdf (accessed on 15 January 2020). (In Japanese).
- Iwai, K. The study on estimation of physical activity and evaluation of cardiac function in pulmonary rehabilitation. J. Jp. Soc. Resp. Care Rehab. 2020, 29, 186–190. (In Japanese) [Google Scholar] [CrossRef]
- Techayusukcharoen, R.; Iida, S.; Aoki, C. Observing brain function via functional near-infrared spectroscopy during cognitive program training (dual task) in young people. J. Phys. Ther. Sci. 2019, 31, 550–555. [Google Scholar] [CrossRef] [Green Version]
- Polidori, M.C.; Stahl, W.; Griffiths, H.R. Nutritional cognitive neuroscience of aging: Focus on carotenoids and cognitive frailty. Redox Biol. 2021, 44, 101996. [Google Scholar] [CrossRef]
- Zamroziewicz, M.K.; Barbey, A.K. Nutritional Cognitive Neuroscience: Innovations for Healthy Brain Aging. Front. Neurosci. 2016, 10, 240. [Google Scholar] [CrossRef] [Green Version]
- Johnson, E.J. A possible role for lutein and zeaxanthin in cognitive function in the elderly. Am. J. Clin. Nutr. 2012, 96, 1161S–1165S. [Google Scholar] [CrossRef] [Green Version]
- Davinelli, S.; Ali, S.; Solfrizzi, V.; Scapagnini, G.; Corbi, G. Carotenoids and Cognitive Outcomes: A Meta-Analysis of Randomized Intervention Trials. Antioxidants 2021, 10, 223. [Google Scholar] [CrossRef]
- Nishino, A.; Ichihara, T.; Takaha, T.; Kuriki, T.; Nihei, H.; Kawamoto, K.; Yasui, H.; Maoka, T. Accumulation of Paprika Carotenoids in Human Plasma and Erythrocytes. J. Oleo Sci. 2015, 64, 1135–1142. [Google Scholar] [CrossRef] [Green Version]
- Solerte, S.B.; Ceresini, G.; Ferrari, E.; Fioravanti, M. Hemorheological changes and overproduction of cytokines from immune cells in mild to moderate dementia of the Alzheimer’s type: Adverse effects on cerebromicrovascular system. Neurobiol. Aging 2000, 21, 271–281. [Google Scholar] [CrossRef]
- Di Francescomarino, S.; Sciartilli, A.; Di Valerio, V.; Di Baldassarre, A.; Gallina, S. The effect of physical exercise on endothelial function. Sports Med. 2009, 39, 797–812. [Google Scholar] [CrossRef] [PubMed]
- Shibuya-Tayoshi, S.; Sumitani, S.; Kikuchi, K.; Tanaka, T.; Tayoshi, S.; Ueno, S.; Ohmori, T. Activation of the prefrontal cortex during the Trail-Making Test detected with multichannel near-infrared spectroscopy. Psychiatry Clin. Neurosci. 2007, 61, 616–621. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | Sex | Age (Year) Mean; Age Range | Hight (cm) Mean ± SD | Weight (kg) Mean ± SD |
|---|---|---|---|---|
| 31 | All | 62.4; 51–74 | 160.0 ± 7.7 | 57.9 ± 11.8 |
| 6 | Male | 63.7; 52–73 | 170.0 ± 4.9 | 73.6 ± 9.8 |
| 25 | Female | 62.0; 51–74 | 158.0 ± 6.1 | 54.1 ± 8.65 |
| Questions | Changes in the TMT Score before and after PX Supplementation | |||||
|---|---|---|---|---|---|---|
| Number | Before | Four Weeks after | ||||
| No | Yes | TMT-A | TMT-B | TMT-A | TMT-B | |
| Are you currently taking a drug to lower blood pressure? | 21 | 10 | −0.351 | −0.214 | −0.184 | 0.176 |
| Are you currently taking a drug to lower blood glucose or insulin injections? | 30 | 1 | 0.084 | 0.150 | 0.121 | 0.105 |
| Are you currently taking a drug to lower cholesterol or neutral fat? | 26 | 5 | −0.318 | 0.144 | 0.195 | 0.036 |
| Have you ever been told by a doctor that you have a stroke (e.g., cerebral hemorrhage, cerebral infarction) or have you ever received treatment for a stroke? | 31 | 0 | - | - | - | - |
| Have you ever been told by a doctor that you have heart disease (e.g., angina, myocardial infarction) or have you ever received treatment for heart disease? | 30 | 1 | 0.104 | 0.073 | −0.204 | −0.001 |
| Have you ever been told by a doctor that you have chronic renal failure/renal insufficiency or have you ever received treatment for chronic renal failure (dialysis, etc.)? | 31 | 0 | - | - | - | - |
| Have you ever been told by a doctor that you have anemia? | 28 | 3 | 0.222 | 0.067 | 0.185 | 0.156 |
| Are you a current regular smoker? | 31 | 0 | - | - | - | - |
| Have you gained ≥10 kg since you were 20 years old? | 18 | 13 | 0.055 | 0.213 | −0.121 | −0.042 |
| Have you been exercising at least two days per week, at least 30 min each at an intensity that causes a slight sweat, for at least one year? | 20 | 11 | −0.202 | −0.333 | 0.106 | −0.455 * |
| Do you walk for at least 1 h every day or have equivalent physical activities in your daily life? | 19 | 12 | −0.088 | −0.013 | 0.128 | −0.108 |
| Do you walk faster than people of your age and sex? | 15 | 16 | 0.083 | −0.166 | 0.035 | 0.022 |
| Do you have an evening meal within 2 h before bedtime three days or more per week? | 23 | 8 | 0.332 | 0.325 | 0.087 | 0.216 |
| Do you have any snacks or sweet beverages other than breakfast, lunch, and dinner? | 15 | 13 | 0.298 | −0.273 | −0.114 | 0.088 |
| Do you skip breakfast three days or more per week? | 24 | 7 | 0.362 * | 0.220 | 0.125 | −0.323 |
| Do you feel refreshed after a night’s sleep? | 11 | 19 | 0.127 | −0.171 | 0.098 | −0.072 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shirai, A.; Wadazumi, T. Effect of Paprika Xanthophyll Supplementation on Cognitive Improvement in a Multitasking Exercise: A Pilot Study for Middle-Aged and Older Adults. Healthcare 2022, 10, 81. https://doi.org/10.3390/healthcare10010081
Shirai A, Wadazumi T. Effect of Paprika Xanthophyll Supplementation on Cognitive Improvement in a Multitasking Exercise: A Pilot Study for Middle-Aged and Older Adults. Healthcare. 2022; 10(1):81. https://doi.org/10.3390/healthcare10010081
Chicago/Turabian StyleShirai, Asako, and Tsuyoshi Wadazumi. 2022. "Effect of Paprika Xanthophyll Supplementation on Cognitive Improvement in a Multitasking Exercise: A Pilot Study for Middle-Aged and Older Adults" Healthcare 10, no. 1: 81. https://doi.org/10.3390/healthcare10010081
APA StyleShirai, A., & Wadazumi, T. (2022). Effect of Paprika Xanthophyll Supplementation on Cognitive Improvement in a Multitasking Exercise: A Pilot Study for Middle-Aged and Older Adults. Healthcare, 10(1), 81. https://doi.org/10.3390/healthcare10010081