
Artificial Intelligence Advances in the World of Cardiovascular Imaging



Abstract
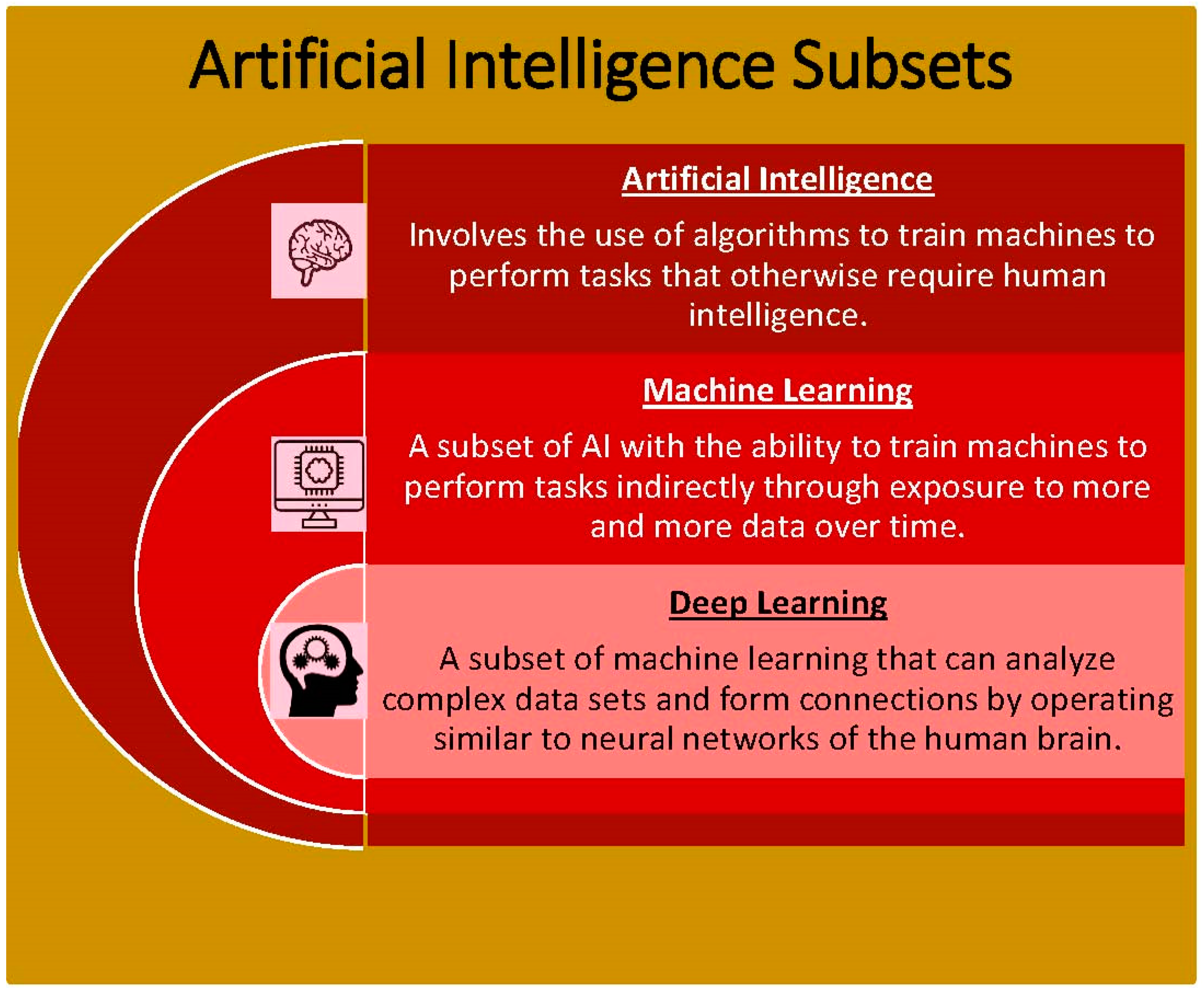
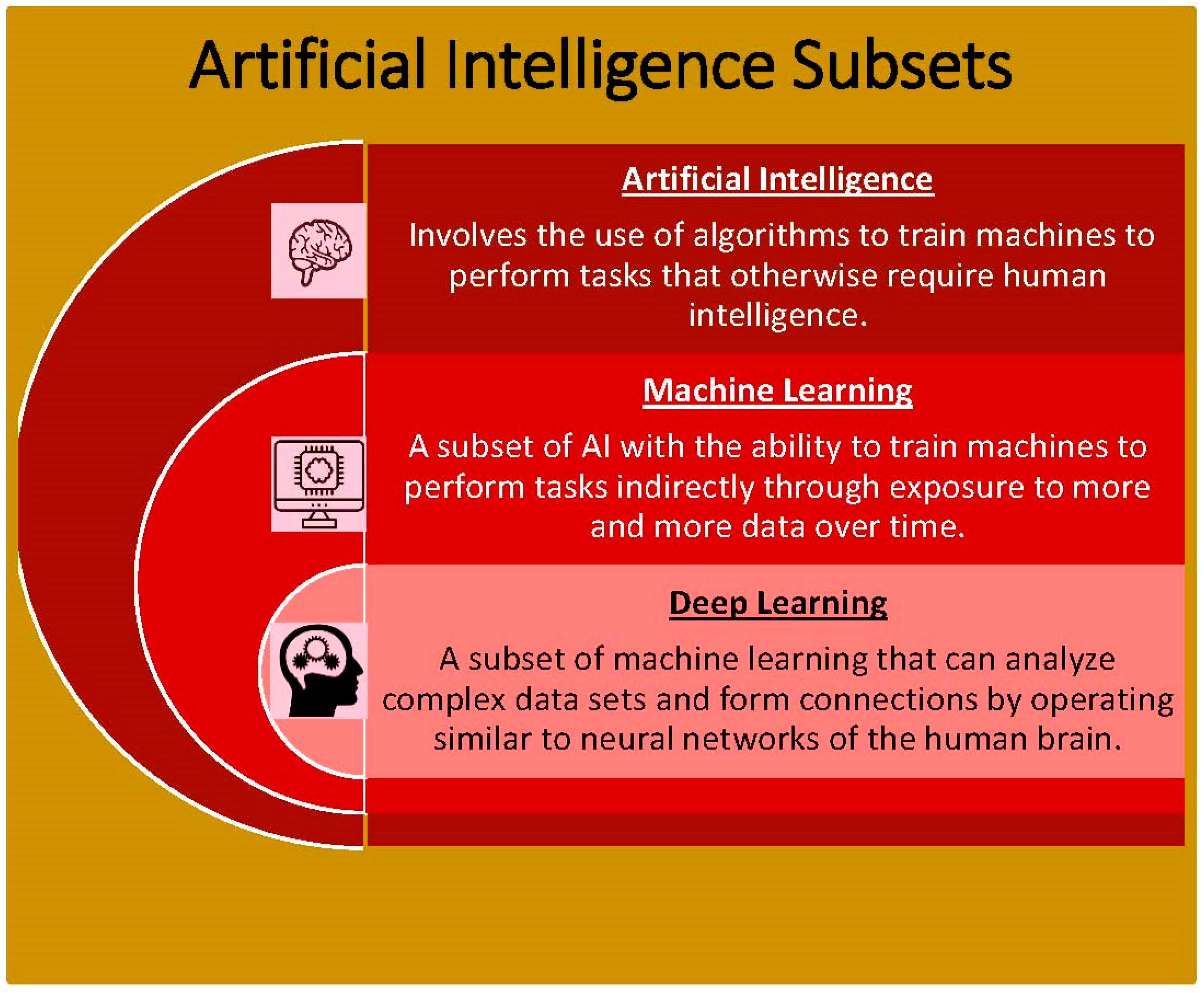
:1. Introduction
2. AI: General Medical Applications
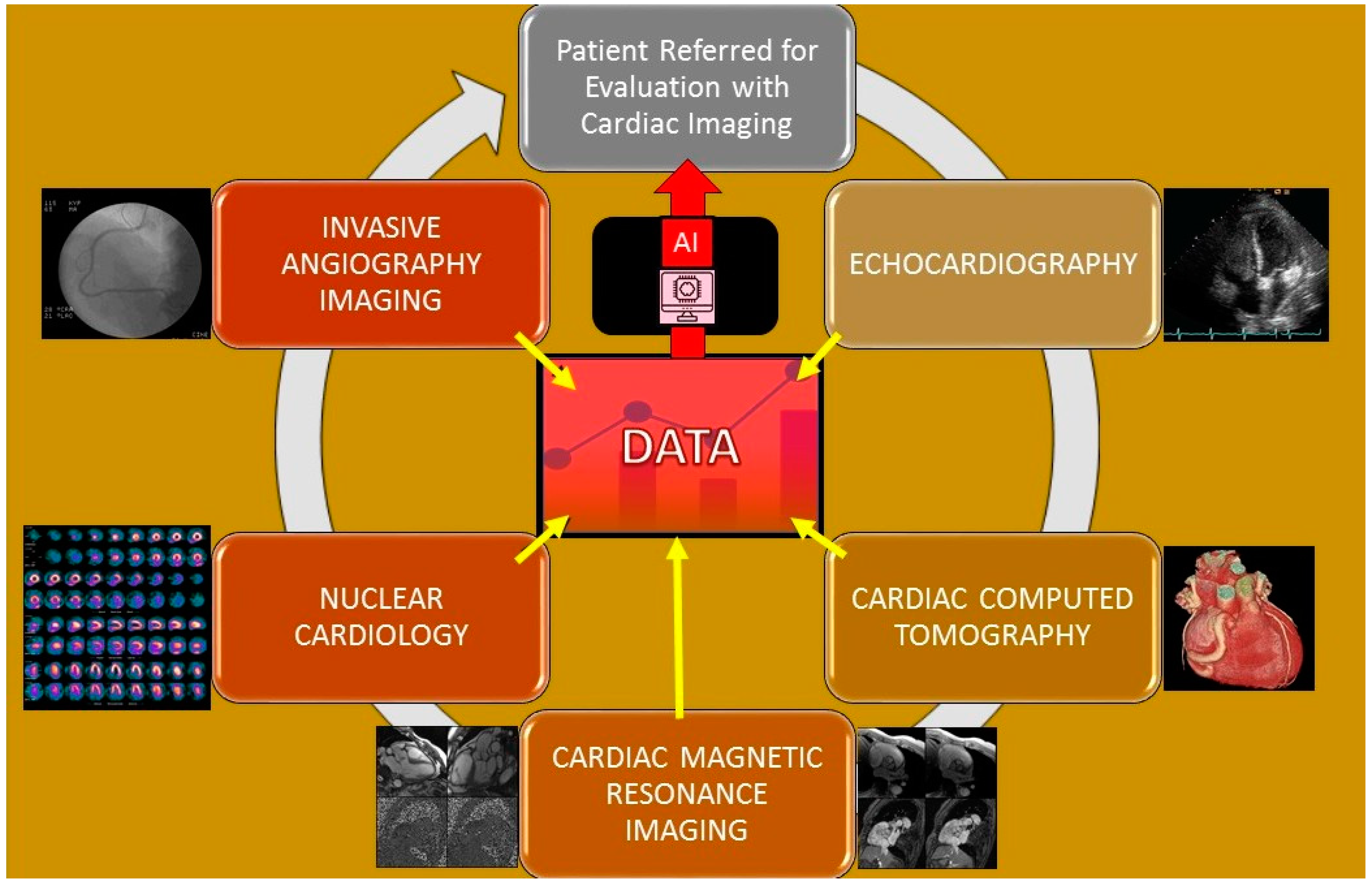
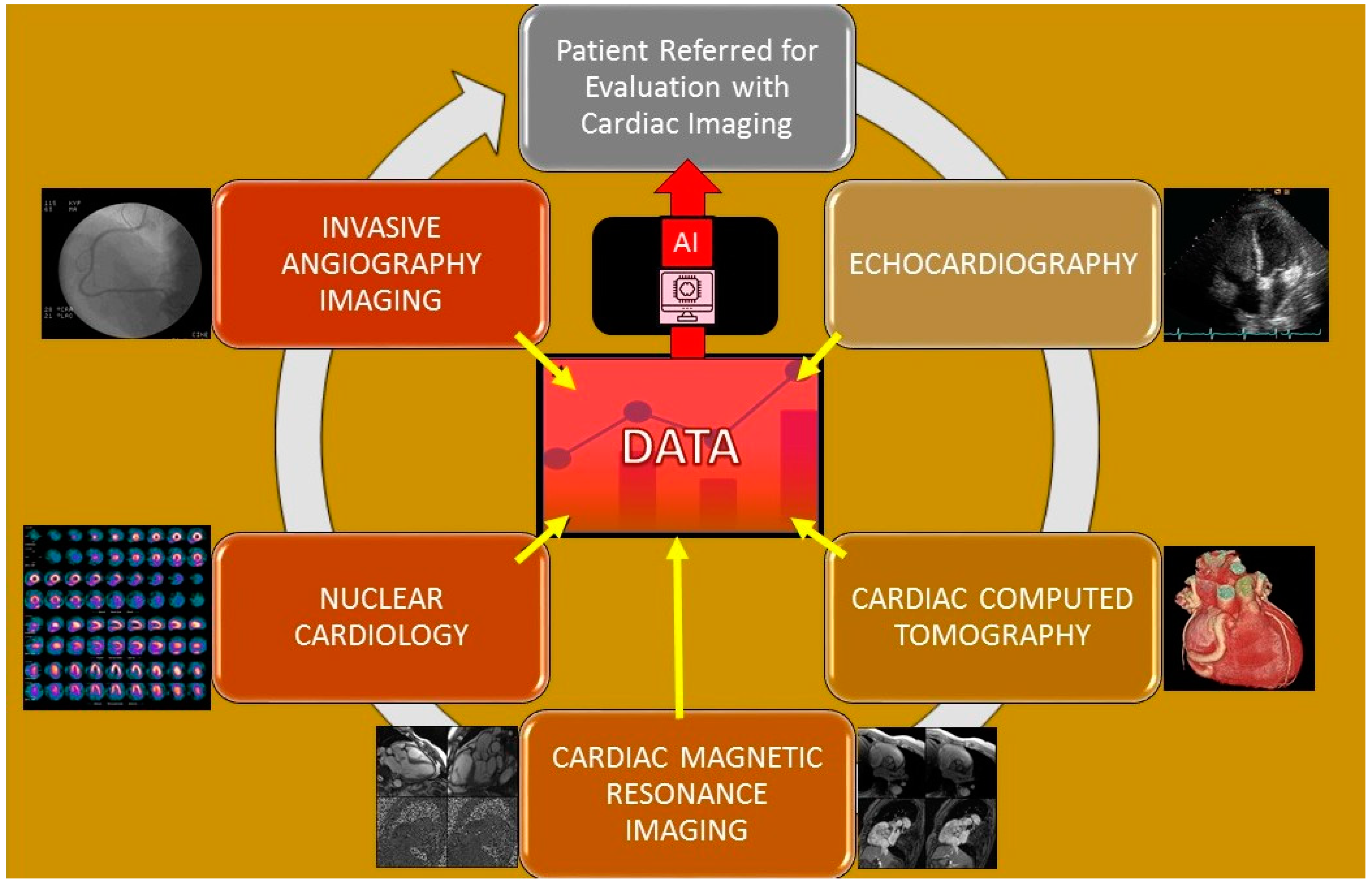
3. AI: Cardiology Imaging Applications
3.1. Echocardiography
3.2. Cardiac Computed Tomography
3.3. Cardiac Magnetic Resonance Imaging
3.4. Nuclear Cardiology
3.5. Angiography Imaging
3.6. Intravascular Imaging
3.7. Software Programs in Clinical Practice That Employ AI
4. Limitations of Artificial Intelligence
5. Future Applications of Artificial Intelligence
6. Conclusions
Funding
Conflicts of Interest
References
- Itchhaporia, D. Artificial intelligence in cardiology. Trends Cardiovasc. Med. 2020, 32, 34–41. [Google Scholar] [CrossRef]
- Zhang, X.-D. Machine learning. In A Matrix Algebra Approach to Artificial Intelligence; Springer: Singapore, 2020; pp. 223–440. [Google Scholar]
- Supervised vs. Unsupervised Learning—Javatpoint. www.javatpoint.com. (n.d.) Available online: https://www.javatpoint.com/difference-between-supervised-and-unsupervised-learning (accessed on 28 October 2021).
- IBM Cloud Education. What is Supervised Learning? IBM. Available online: https://www.ibm.com/cloud/learn/supervised-learning (accessed on 23 December 2021).
- IBM. Supervised vs. Unsupervised Learning: What’s the Difference? Available online: https://www.ibm.com/cloud/blog/supervised-vs-unsupervised-learning (accessed on 9 January 2021).
- Yu, A.C.; Eng, J. One Algorithm May Not Fit All: How Selection Bias Affects Machine Learning Performance. RadioGraphics 2020, 40, 1932–1937. [Google Scholar] [CrossRef]
- Buch, V.H.; Ahmed, I.; Maruthappu, M. Artificial intelligence in medicine: Current trends and future possibilities. Br. J. Gen. Pr. 2018, 68, 143–144. [Google Scholar] [CrossRef] [Green Version]
- Kabani, A.; El-Sakka, M.R. Object Detection and Localization Using Deep Convolutional Networks with Softmax Activation and Multi-class Log Loss. In Image Analysis and Recognition; Campilho, A., Karray, F., Eds.; Springer International Publishing: Cham, Switzerland, 2016; pp. 358–366. [Google Scholar]
- Arafati, A.; Hu, P.; Finn, J.P.; Rickers, C.; Cheng, A.L.; Jafarkhani, H.; Kheradvar, A. Artificial intelligence in pediatric and adult congenital cardiac MRI: An unmet clinical need. Cardiovasc. Diagn. Ther. 2019, 9, S310–S325. [Google Scholar] [CrossRef] [Green Version]
- Shah, S.J.; Katz, D.; Selvaraj, S.; Burke, M.A.; Yancy, C.W.; Gheorghiade, M.; Bonow, R.O.; Huang, C.-C.; Deo, R.C. Phenomapping for Novel Classification of Heart Failure with Preserved Ejection Fraction. Circulation 2015, 131, 269–279. [Google Scholar] [CrossRef] [Green Version]
- West, D.M. What is Artificial Intelligence? Brookings Institution. 2019. Available online: https://www.brookings.edu/research/what-is-artificial-intelligence/ (accessed on 28 October 2021).
- Lim, L.J.; Tison, G.H.; Delling, F.N. Artificial Intelligence in Cardiovascular Imaging. Methodist DeBakey Cardiovasc. J. 2020, 16, 138–145. [Google Scholar] [CrossRef]
- Hamet, P.; Tremblay, J. Artificial Intelligence in medicine. Metabolism 2017, 69, S36–S40. [Google Scholar] [CrossRef]
- Amisha, P.M.; Pathania, M.; Rathaur, V.K. Overview of artificial intelligence in medicine. J. Fam. Med. Prim. Care 2019, 8, 2328–2331. [Google Scholar] [CrossRef]
- Momentum Janitorial. Ai-Enabled Robotic Surgery: How Collaborative Robots are Assisting Surgeons. Far North Surgery. 18 October 2020. Available online: https://www.farnorthsurgery.com/blog/aienabled-robotic-surgery-how-collaborative-robots-are-assisting-surgeons (accessed on 23 December 2021).
- Study Identifies Human Errors Associated with Surgical Errors. Baylor College of Medicine. Available online: https://www.bcm.edu/news/human-errors-adverse-surgical-events (accessed on 28 October 2021).
- Gottdiener, J.S.; Bednarz, J.; Devereux, R.; Gardin, J.; Klein, A.; Manning, W.J.; Morehead, A.; Kitzman, D.; Oh, J.; Quinones, M.; et al. American Society of Echocardiography recommendations for use of echocardiography in clinical trials. J. Am. Soc. Echocardiogr. 2004, 17, 1086–1119. [Google Scholar] [CrossRef]
- Rajih, E.; Tholomier, C.; Cormier, B.; Samouëlian, V.; Warkus, T.; Liberman, M.; Widmer, H.; Lattouf, J.-B.; Alenizi, A.M.; Meskawi, M.; et al. Error reporting from the da Vinci surgical system in robotic surgery: A Canadian multispecialty experience at a single academic centre. Can. Urol. Assoc. J. 2017, 11, E197–E202. [Google Scholar] [CrossRef] [Green Version]
- Seetharam, K.; Brito, D.; Farjo, P.D.; Sengupta, P.P. The Role of Artificial Intelligence in Cardiovascular Imaging: State of the Art Review. Front. Cardiovasc. Med. 2020, 7, 618849. [Google Scholar] [CrossRef]
- Arsanjani, R.; Xu, Y.; Dey, D.; Fish, M.; Dorbala, S.; Hayes, S.; Berman, D.; Germano, G.; Slomka, P. Improved Accuracy of Myocardial Perfusion SPECT for the Detection of Coronary Artery Disease Using a Support Vector Machine Algorithm. J. Nucl. Med. 2013, 54, 549–555. [Google Scholar] [CrossRef] [Green Version]
- Seetharam, K.; Shresthra, S.; Mills, J.D.; Sengupta, P.P. Artificial Intelligence in Nuclear Cardiology: Adding Value to Prognostication. Curr. Cardiovasc. Imaging Rep. 2019, 12, 14. [Google Scholar] [CrossRef]
- Zhang, J.; Gajjala, S.; Agrawal, P.; Tison, G.H.; Hallock, L.A.; Beussink-Nelson, L.; Lassen, M.H.; Fan, E.; Aras, M.A.; Jordan, C.; et al. Fully Automated Echocardiogram Interpretation in Clinical Practice. Circulation 2018, 138, 1623–1635. [Google Scholar] [CrossRef]
- Alsharqi, M.; Woodward, W.; Mumith, A.; Markham, D.; Upton, R.; Leeson, P. Artificial intelligence and echocardiography. Echo Res. Pract. 2018, 5, R115–R125. [Google Scholar] [CrossRef] [Green Version]
- Narula, S.; Shameer, K.; Omar, A.M.S.; Dudley, J.T.; Sengupta, P.P. Machine-Learning Algorithms to Automate Morphological and Functional Assessments in 2D Echocardiography. J. Am. Coll. Cardiol. 2016, 68, 2287–2295. [Google Scholar] [CrossRef]
- Seetharam, K.; Raina, S.; Sengupta, P.P. The Role of Artificial Intelligence in Echocardiography. Curr. Cardiol. Rep. 2020, 22, 99. [Google Scholar] [CrossRef] [PubMed]
- ACR RSNA. Cardiac CT for Calcium Scoring. Radiologyinfo.org 2020. Available online: https://www.radiologyinfo.org/en/info/ct_calscoring (accessed on 28 October 2021).
- Al’Aref, S.J.; Maliakal, G.; Singh, G.; van Rosendael, A.R.; Ma, X.; Xu, Z.; Alawamlh, O.A.H.; Lee, B.; Pandey, M.; Achenbach, S.; et al. Machine learning of clinical variables and coronary artery calcium scoring for the prediction of obstructive coronary artery disease on coronary computed tomography angiography: Analysis from the CONFIRM registry. Eur. Hear. J. 2019, 41, 359–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, A.; Kolossváry, M.; Motwani, M.; Išgum, I.; Maurovich-Horvat, P.; Slomka, P.J.; Dey, D. Artificial intelligence in cardiovascular CT: Current status and future implications. J. Cardiovasc. Comput. Tomogr. 2021, 15, 462–469. [Google Scholar] [CrossRef]
- McCollough, C.; Leng, S. Use of artificial intelligence in computed tomography dose optimisation. Ann. ICRP 2020, 49, 113–125. [Google Scholar] [CrossRef]
- Immonen, E.; Wong, J.; Nieminen, M.; Kekkonen, L.; Roine, S.; Törnroos, S.; Lanca, L.; Guan, F.; Metsälä, E. The use of deep learning towards dose optimization in low-dose computed tomography: A scoping review. Radiography 2021, 28, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Seetharam, K.; Kagiyama, N.; Shrestha, S.; Sengupta, P.P. Clinical Inference From Cardiovascular Imaging: Paradigm Shift Towards Machine-Based Intelligent Platform. Curr. Treat. Options Cardiovasc. Med. 2020, 22, 8. [Google Scholar] [CrossRef]
- Kuehn, B.M. Cardiac Imaging on the Cusp of an Artificial Intelligence Revolution. Circulation 2020, 141, 1266–1267. [Google Scholar] [CrossRef] [PubMed]
- Dorado-Díaz, P.I.; Sampedro-Gómez, J.; Vicente-Palacios, V.; Sánchez, P.L. Applications of Artificial Intelligence in Cardiology. The Future is Already Here. Rev. Española Cardiol. 2019, 72, 1065–1075. [Google Scholar] [CrossRef]
- Mathur, P.; Srivastava, S.; Xu, X.; Mehta, J.L. Artificial Intelligence, Machine Learning, and Cardiovascular Disease. Clin. Med. Insights Cardiol. 2020, 14. [Google Scholar] [CrossRef]
- Zhang, N.; Yang, G.; Gao, Z.; Xu, C.; Zhang, Y.; Shi, R.; Keegan, J.; Xu, L.; Zhang, H.; Fan, Z.; et al. Deep learning for diagnosis of chronic myocardial infarction on nonen-hanced cardiac cine MRI. Radiology 2019, 291, 606–617. [Google Scholar] [CrossRef] [Green Version]
- El-Tallawi, K.C.; Aljizeeri, A.; Nabi, F.; Al-Mallah, M.H. Myocardial Perfusion Imaging Using Positron Emission Tomography. Methodist DeBakey Cardiovasc. J. 2020, 16, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.-H.; Betancur, J.; Sharir, T.; Einstein, A.J.; Bokhari, S.; Fish, M.B.; Ruddy, T.D.; Kaufmann, P.A.; Sinusas, A.J.; Miller, E.; et al. Machine learning predicts per-vessel early coronary revascularization after fast myocardial perfusion SPECT: Results from multicentre REFINE SPECT registry. Eur. Hear. J. Cardiovasc. Imaging 2019, 21, 549–559. [Google Scholar] [CrossRef]
- Knaapen, P. Computed Tomography to Replace Invasive Coronary Angiography? Circ. Cardiovasc. Imaging 2019, 12, e008710. [Google Scholar] [CrossRef] [Green Version]
- Siegersma, K.; Leiner, T.; Chew, D.; Appelman, Y.; Hofstra, L.; Verjans, J. Artificial intelligence in cardiovascular imaging: State of the art and implications for the imaging cardiologist. Neth. Hear. J. 2019, 27, 403–413. [Google Scholar] [CrossRef] [Green Version]
- Muscogiuri, G.; Van Assen, M.; Tesche, C.; De Cecco, C.N.; Chiesa, M.; Scafuri, S.; Guglielmo, M.; Baggiano, A.; Fusini, L.; Guaricci, A.I.; et al. Artificial Intelligence in Coronary Computed Tomography Angiography: From Anatomy to Prognosis. BioMed Res. Int. 2020, 2020, 6649410. [Google Scholar] [CrossRef]
- Van Hamersvelt, R.W.; Zreik, M.; Voskuil, M.; Viergever, M.A.; Išgum, I.; Leiner, T. Deep learning analysis of left ventricular myocardium in CT angiographic intermediate-degree coronary stenosis improves the diagnostic accuracy for identification of functionally significant stenosis. Eur. Radiol. 2018, 29, 2350–2359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Motwani, M.; Dey, D.; Berman, D.S.; Germano, G.; Achenbach, S.; Al-Mallah, M.; Andreini, D.; Budoff, M.J.; Cademartiri, F.; Callister, T.Q.; et al. Machine learning for prediction of all-cause mortality in patients with suspected coronary artery disease: A 5-year multicentre prospective registry analysis. Eur. Hear. J. 2016, 38, 500–507. [Google Scholar] [CrossRef] [PubMed]
- Fractional Flow Reserve—Computed Tomography: Heart Care in NJ. RWJBarnabas Health. Available online: https://www.rwjbh.org/treatment-care/heart-and-vascular-care/tests-procedures/fractional-flow-reserve-computed-tomography/ (accessed on 9 January 2022).
- Eiman Jahangir, M.D.; Fractional Flow Reserve (FFR) Measurement. Fractional Flow Reserve (FFR) Measurement. Background, Indications, Outcomes. Background, Indications, Outcomes. Medscape, 2021. Available online: https://emedicine.medscape.com/article/1839601-overview#a1 (accessed on 9 January 2022).
- Di Jiang, M.; Zhang, X.L.; Liu, H.; Tang, C.X.; Li, J.H.; Wang, Y.N.; Xu, P.P.; Zhou, C.S.; Zhou, F.; Lu, M.J.; et al. The effect of coronary calcification on diagnostic performance of machine learning–based CT-FFR: A Chinese multicenter study. Eur. Radiol. 2020, 31, 1482–1493. [Google Scholar] [CrossRef]
- Yang, S.; Koo, B.-K.; Hoshino, M.; Lee, J.M.; Murai, T.; Park, J.; Zhang, J.; Hwang, D.; Shin, E.-S.; Doh, J.-H.; et al. CT Angiographic and Plaque Predictors of Functionally Significant Coronary Disease and Outcome Using Machine Learning. JACC Cardiovasc. Imaging 2020, 14, 629–641. [Google Scholar] [CrossRef] [PubMed]
- Intravascular Ultrasound (IVUS). Cedars. Available online: https://www.cedars-sinai.org/programs/heart/clinical/womens-heart/services/ivus-intravascular-ultrasound.html (accessed on 9 January 2022).
- Using AI to Facilitate Diagnosis. Harvard-MIT Health Sciences and Technology. 2021. Available online: https://hst.mit.edu/news-events/using-ai-facilitate-diagnosis (accessed on 9 January 2022).
- Merge PACS—Overview. IBM. (n.d.). Available online: https://www.ibm.com/products/merge-pacs (accessed on 14 November 2021).
- Miller, R. IBM Buying Merge Healthcare for $1B to Bring Medical Image Analysis to Watson Health. TechCrunch. 6 August 2015. Available online: https://techcrunch.com/2015/08/06/ibm-buying-merge-healthcare-for-1b-to-bring-medical-image-analysis-to-watson-health/ (accessed on 14 November 2021).
- Shameer, K.; Johnson, K.; Glicksberg, B.; Dudley, J.T.; Sengupta, P.P. Machine learning in cardiovascular medicine: Are we there yet? Heart 2018, 104, 1156–1164. [Google Scholar] [CrossRef] [PubMed]
- Al’Aref, S.J.; Anchouche, K.; Singh, G.; Slomka, P.J.; Kolli, K.K.; Kumar, A.; Pandey, M.; Maliakal, G.; van Rosendael, A.R.; Beecy, A.N.; et al. Clinical applications of machine learning in cardiovascular disease and its relevance to cardiac imaging. Eur. Heart J. 2019, 40, 1975–1986. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Machine Learning Classification | Types of Problems Each Classification Is Used for |
|---|---|
| Supervised Learning—Uses reference data to analyze algorithms and apply the algorithms to a similar dataset [3] | Classification—Utilizes an algorithm to assign a dataset into specific categories. Specifically, draws conclusions on how specific categories in the dataset should be labeled. [4] |
| Regression—Analyzes the relationship between dependent and independent variables, particularly for making projections [4] | |
| Unsupervised Learning—Identifies hidden patterns in data without any given reference [3] | Clustering—Organizes unlabeled data based on similarities and differences [5] |
| Dimension Reduction—Reduces the number of data inputs while preserving the data integrity; applied when there is an increased number of features or dimensions in a dataset [5] |
| Pertinent Publications Related to Artificial Intelligence in the Field of Cardiovascular Imaging | Findings in Publication |
|---|---|
| Improved accuracy of myocardial perfusion single-photon emission computed tomography [SPECT] for the detection of coronary artery disease using a support vector machine algorithm | Arsajani et al. found that the accuracy of predicting CAD with an MPI device improved significantly when in adjunct with a learning algorithm [22] |
| Fully Automated Echocardiogram Interpretation in Clinical Practice | Zhang et al. determined 96% accuracy in identifying images with echocardiography [22] |
| Machine learning of clinical variables and coronary artery calcium scoring for the prediction of obstructive coronary artery disease on coronary computed tomography angiography: analysis from the CONFIRM registry | Al’Aref et al.’s results showed a significantly more accurate assessment of obstructive CAD from CT imaging using machine learning with the coronary artery calcium score [21] |
| Cardiac Imaging on the Cusp of an Artificial Intelligence Revolution | Laser et al. determined that the right ventricle reconstruction with echocardiography and cardiac MRI had more accuracy compared to the gold standard direct cardiac MRI [23] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patel, B.; Makaryus, A.N. Artificial Intelligence Advances in the World of Cardiovascular Imaging. Healthcare 2022, 10, 154. https://doi.org/10.3390/healthcare10010154
Patel B, Makaryus AN. Artificial Intelligence Advances in the World of Cardiovascular Imaging. Healthcare. 2022; 10(1):154. https://doi.org/10.3390/healthcare10010154
Chicago/Turabian StylePatel, Bhakti, and Amgad N. Makaryus. 2022. "Artificial Intelligence Advances in the World of Cardiovascular Imaging" Healthcare 10, no. 1: 154. https://doi.org/10.3390/healthcare10010154
APA StylePatel, B., & Makaryus, A. N. (2022). Artificial Intelligence Advances in the World of Cardiovascular Imaging. Healthcare, 10(1), 154. https://doi.org/10.3390/healthcare10010154