
Development of a Social Play Evaluation Tool for Preschool Children



Abstract
1. Introduction
2. Methods
2.1. Design
2.2. Participants
2.3. Procedures
2.4. Data Analysis
3. Results
3.1. Step 1. CFA
3.2. Step 2. Rasch Analysis
3.2.1. Item and Person Fit
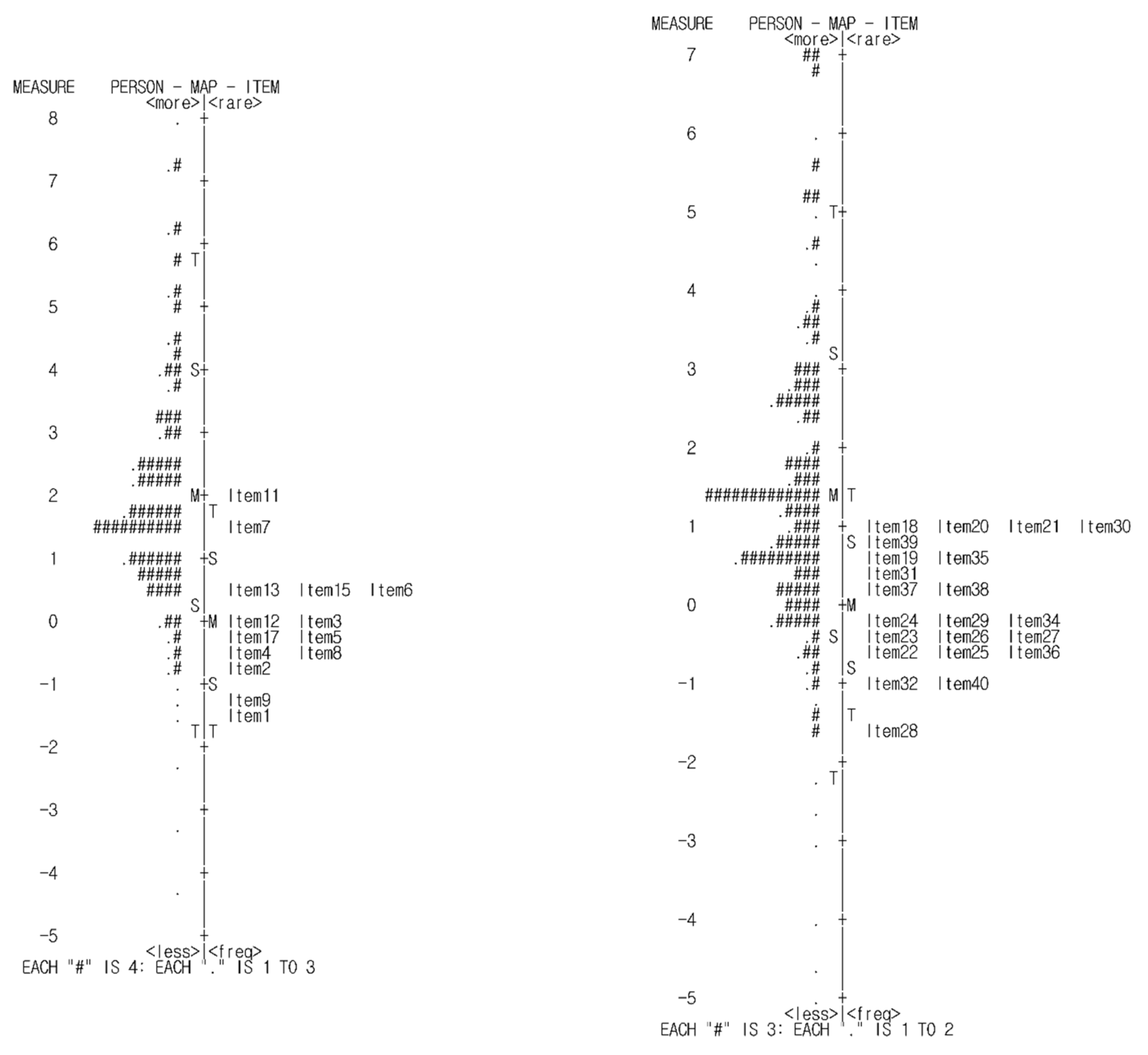
3.2.2. Item Difficulty and Person-Item Match
3.2.3. Rating Scale Analysis
3.2.4. Precision
3.3. Step 3. Known-Groups Validity
4. Discussion
4.1. Limitations
4.2. Future Lines of Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Scoring Sheets

{kind=link}
{kind=link}
| Item | Associative Play | Never | Rarely | Sometimes | Always |
|---|---|---|---|---|---|
| 1 | The child prefers to play with other children in a group | ||||
| 2 | The child plays by interacting with another child, such as by asking questions | ||||
| 3 | The child plays and sing or dances with other children in the group. | ||||
| 4 | The child talk with other children about the story of the play activity | ||||
| 5 | The child plays with other children by lending and borrowing toys | ||||
| 6 | The child share, lend, and order toys while preoccupied with their own play activities | ||||
| 7 | The child plays and exchanges toys with other children, although the story of the play is unstructured | ||||
| 8 | The child tells the parent or caregiver the story of the play with another child | ||||
| 9 | The child engages in the play of other children | ||||
| 10 | The child notices and wants to engage with a child who likes the same style of play | ||||
| 11 | The child pay attention to other children’s play activities and engages in many conversations. | ||||
| 12 | The child can offer his (or her) toy to another child | ||||
| 13 | The child tries to recruit another child who would participate in the group | ||||
| 14 | The child kind of tries to control another child with whom he/she |
| Item | Cooperative Play | Never | Rarely | Sometimes | Always |
|---|---|---|---|---|---|
| 1 | The child engages in role play with other children, creating various scenarios (e.g., hospital, teacher) | ||||
| 2 | The child can compose a play environment with other children (e.g., bringing toys, clearing obstacles, etc.) | ||||
| 3 | The child participates in the activity by selecting and sharing roles with other children in “pretend” play situations (e.g., role play) | ||||
| 4 | The child remembers previous play with other children and is able to continue it the next time they meet | ||||
| 5 | The child engage in play activities with rules | ||||
| 6 | The child can play given roles in the process of play with other children | ||||
| 7 | The child can help other children in need during play | ||||
| 8 | The child play with three or more children without constant supervision | ||||
| 9 | The child play cooperatively with other children to complete objects or structures | ||||
| 10 | The child can play to achieve competitive goals | ||||
| 11 | The child explain the rules of play to other children | ||||
| 12 | The child can transform one play into another | ||||
| 13 | When a child is given an unwanted role in play, the child can express his (or her) opinion | ||||
| 14 | The child can change their roles in play for other children | ||||
| 15 | The child understand the rules of fair play | ||||
| 16 | The child compete against other teams in a game with rules | ||||
| 17 | The child can work with other children to create new ways of playing or rules | ||||
| 18 | The child try to conform to their own and other children’s opinions when making play choices | ||||
| 19 | The child form teams to play in groups | ||||
| 20 | The child share roles in play to complete the outcome | ||||
| 21 | The child can set goals for play activities within a group and play proceeds systematically | ||||
| 22 | The child organizes play, such as assigning work to different people within a group |
References
- Meyer, A. The philosophy of occupational therapy. Arch. Occup. Ther. 1922, 1, 1–10. [Google Scholar] [CrossRef]
- Alessandrini, N.A. Play-A child’s world. Am. J. Occup. Ther. 1949, 3, 9–12. [Google Scholar]
- Reilly, M. Play as Exploratory Learning; SAGE Publications: Beverly Hills, CA, USA, 1974. [Google Scholar]
- Bundy, A. Play and playfulness: What to look for. Play. Occup. Ther. Child. 1997, 52–66. [Google Scholar]
- Henry, A. Assessment of Play and Leisure in children and adolescents. In Play in Occupational Therapy for Children; Mosby: St. Louis, MO, USA, 2008; pp. 95–125. [Google Scholar] [CrossRef]
- Canadian Association of Occupational Therapists. Practice paper: Occupational therapy and children’s play. Can. J. Occup. Ther. 1996, 63, 1–9. [Google Scholar] [CrossRef]
- Rodger, S.; Ziviani, J. Play-based occupational therapy. Int. J. Disabil. Dev. Educ. 1999, 46, 337–365. [Google Scholar] [CrossRef]
- Parham, L.D.; Fazio, L.S. Play in Occupational Therapy for Children; Mosby: St. Louis, MO, USA, 1997. [Google Scholar]
- Lee, S.H.; Hong, C.R.; Park, H.Y. Current trend in use of occupational therapy assessment tool by pediatric occupational therapist. J. Korean Acad. Sens. Integr. 2018, 16, 23–33. [Google Scholar]
- Stagnitti, K. Understanding play: The implications for play assessment. Aust. Occup. Ther. J. 2004, 51, 3–12. [Google Scholar] [CrossRef]
- Lee, S.A.; Choi, J.S. Play awareness of occupational therapists with using the sensory integration approach. J. Korean Acad. Sens. Integr. 2004, 2, 43–52. [Google Scholar]
- Couch, K.J.; Dietz, J.C.; Kanny, E.M. The role of play in pediatric occupational therapy. Am. J. Occup. Ther. 1998, 52, 111–117. [Google Scholar] [CrossRef]
- Kuhaneck, H.M.; Tanta, K.J.; Coombs, A.K.; Pannone, H. A survey of pediatric occupational therapists’ use of play. J. Occup. Ther. Sch. Early Interv. 2013, 6, 213–227. [Google Scholar] [CrossRef]
- Moore, A.; Lynch, H. Play and play occupation: A survey of pediatric occupational therapy practice in Ireland. Ir. J. Occup. Ther. 2018, 46, 59–72. [Google Scholar] [CrossRef]
- Bailey, D.B., Jr.; Wolery, M. Assessing Infants and Preschoolers with Handicaps; Merrill Publishing, Co.: Princeton, NJ, USA, 1989. [Google Scholar]
- Fantuzzo, J.; Coolahan, K.; Mendez, J.; McDermott, P.; Sutton-Smith, B. Contextually-relevant validation of peer play constructs with African American Head Start children: Penn interactive play scale. Early Child. Res. Q. 1998, 13, 411–431. [Google Scholar] [CrossRef]
- Han, J.Y.; Yim, D.S. Korean brief parent report measures of language development in children with vocabulary delay. JSLHD 2018, 27, 69–84. [Google Scholar]
- Thal, D.; Jackson-Maldonado, D.; Acosta, D. Validity of a parent-report measure of vocabulary and grammar for Spanish-speaking toddlers. J. Speech Lang. Hear. Res. 2000, 43, 1087–1100. [Google Scholar] [CrossRef]
- Choi, H.Y.; Shin, H.Y. Validation of the Penn interactive peer play scale for Korean children. Korean J. Child Stud. 2008, 29, 303–318. [Google Scholar]
- Parten, M.B. Social participation among pre-school children. J Abnorm. Psychol. 1932, 27, 243–269. [Google Scholar] [CrossRef]
- The Korean Society of Occupational Therapy for Child and School. Pediatric Occupational Therapy; Gyechuk Munwhasa: Seoul, Korea, 2012. [Google Scholar]
- Farran, D.C.; Son-Yarbrough, W. I funded preschools as a developmental context for children’s play and verbal behaviors. Early Child. Res. Q. 2001, 16, 245–262. [Google Scholar] [CrossRef]
- Lillvist, A. Observations of social competence of children in need of special support based on traditional disability categories versus a functional approach. Early Child Dev. Care 2010, 180, 1129–1142. [Google Scholar] [CrossRef]
- Sjöman, M.; Granlund, M.; Almqvist, L. Interaction processes as a mediating factor between children’s externalized behaviour difficulties and engagement in preschool. Early Child Dev. Care 2016, 186, 1649–1663. [Google Scholar] [CrossRef]
- Shin, E.S.; Kim, M.S.; Shin, D.J.; Lee, J.H.; Choi, S.R. Play and Young Children; Ewha Womans University Press: Seoul, Korea, 2002. [Google Scholar]
- Kim, S.J. Sequential Transition Patterns of Social Play According to the Children’s Social Competence. Master’s Thesis, Ewha Womans University, Seoul, Korea, 2003. [Google Scholar]
- Pellegrini, A.D.; Perlmutter, J.C. Classroom contextual effects on children’s play. Dev. Psychol. 1989, 25, 289–296. [Google Scholar] [CrossRef]
- Rubin, K.H.; Maioni, T.L.; Hornung, M. Free play behaviors in middle-and lower-class preschoolers: Parten and Piaget revisited. Child Dev. 1976, 47, 414–419. [Google Scholar] [CrossRef]
- Smilansky, S. The Effects of Sociodramatic Play on Disadvantaged Preschool Children; John Wiley & Sons: New York, NY, USA, 1968. [Google Scholar]
- Park, S.H. Development of an Occupational Therapy Program to Improve School Readiness in Preschool Children with Disabilities. Ph.D. Thesis, Honam University, Gwangju, Korea, 2018. [Google Scholar]
- Shin, M.K. Development and Validation of a Sensory Processing Evaluation Tool for Preschool Children Based on the Sensory Environment of Home. Ph.D. Thesis, Yonsei University, Seoul, Korea, 2019. [Google Scholar]
- Lee, S.H.; Jung, M.Y.; Yoo, E.Y.; Hong, I.; Kim, J.R.; Park, H.Y. Developing Social Play Evaluation Items for Preschool Children: A Delphi Study. Ther. Sci. Rehabil. 2021, 10, 97–110. [Google Scholar] [CrossRef]
- Brown, T.A. Confirmatory Factor Analysis for Applied Research; Guilford Publications: New York, NY, USA, 2015. [Google Scholar]
- Linacre, J.M. Sample size and item calibration stability. Rasch Meas. Trans. 1994, 7, 328. [Google Scholar]
- Reeve, B.B.; Hays, R.D.; Bjorner, J.B.; Cook, K.F.; Crane, P.K.; Teresi, J.A.; Thissen, D.; Revicki, D.A.; Weiss, D.J.; Hambleton, R.K.; et al. Psychometric evaluation and calibration of health-related quality of life item banks: Plans for the Patient-Reported Outcomes Measurement Information System (PROMIS). Med. Care. 2007, 45, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Bentler, P.M. Comparative fit indexes in structural models. Psychol. Bull. 1990, 107, 238. [Google Scholar] [CrossRef]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Modeling A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Bond, T.G.; Fox, C.M. Applying the Rasch Model: Fundamental Measurement in the Human Science, 3rd ed.; Psychology Press: New York, NY, USA, 2015. [Google Scholar]
- Wright, B.D. Reasonable mean-square fit values. Rasch Meas. Trans. 1994, 2, 370. [Google Scholar]
- Bond, T.G.; Fox, C.M. Applying the Rasch Model: Fundamental Measurement in the Human Science, 2nd ed.; Psychology Press: New York, NY, USA, 2007. [Google Scholar]
- Wright, B. Number of person or item strata (4G+ 1)/3. Rasch Meas. Trans. 2002, 16, 888. [Google Scholar]
- Lunz, M.E.; Stahl, J.A. The effect of rater severity on person ability measure: A Rasch model analysis. Am. J. Occup. Ther. 1993, 47, 311–317. [Google Scholar] [CrossRef][Green Version]
- Cho, E.O. A Study of Children’s Playfulness and Play Behavior According to Their Temperament. Master’s Thesis, Su-won University, Suwon, Korea, 2002. [Google Scholar]
- Linacre, J.M. Optimizing rating scale category effectiveness. J. Appl. Meas. 2002, 3, 85–106. [Google Scholar]
- Choi, H.Y. Validation of The Parent Version of Penn Interactive Peer Play Scale for Young Children. J. Korean Home Econ. Assoc. 2010, 48, 133–141. [Google Scholar] [CrossRef]
- Suh, M.O. A validation of the Korean version of the Social Skill Rating System for preschool level (K-SSRS: Teacher and Parent Forms). J. Early Child Educ. 2004, 24, 223–424. [Google Scholar]
- Prieto, L.; Alonso, J.; Lamarca, R. Classical test theory versus Rasch analysis for quality of life questionnaire reduction. Health Qual. Life Outcomes 2003, 1, 1–13. [Google Scholar]
- Coplan, R.J.; Rubin, K.H. Exploring and assessing nonsocial play in the preschool: The development and validation of the Preschool Play Behavior Scale. Soc. Dev. 1998, 7, 72–91. [Google Scholar] [CrossRef]
- Lee, S.Y. The Impact of Group Sensory Integrative Intervention for Motor Skills and Play Behaviors of the Children with Autism Spectrum Disorder. Master’s Thesis, Daegu University, Gyeongbuk, Korea, 2013. [Google Scholar]
- Squire, J.K.; Nickel, R.; Bricker, D. Use of parent-completed developmental questionnaires for child-find and screening. Infants Young Child. 1990, 3, 46–57. [Google Scholar] [CrossRef]


| Area | Item | Measure (Logits) | Infit | Outfit | ||
|---|---|---|---|---|---|---|
| MNSQ | ZSTD | MNSQ | ZSTD | |||
| Associative play | 1 | −1.38 | 0.90 | −1.23 | 0.90 | −1.02 |
| 2 | −0.69 | 1.23 | 2.34 | 1.27 | 2.31 | |
| 3 | 0.04 | 1.27 | 2.73 | 1.32 | 2.91 | |
| 4 | −0.55 | 0.81 | −2.15 | 0.75 | −2.55 | |
| 5 | −0.26 | 0.85 | −1.71 | 0.79 | −2.20 | |
| 6 | 0.31 | 0.94 | −0.65 | 0.92 | −0.81 | |
| 7 | 1.33 | 1.06 | 0.78 | 1.12 | 1.39 | |
| 8 | −0.29 | 0.65 | −4.23 | 0.60 | −4.48 | |
| 9 | −1.02 | 0.65 | −4.61 | 0.58 | −4.45 | |
| 10 | Deleted | |||||
| 11 | 1.75 | 1.26 | 3.05 | 1.34 | 3.78 | |
| 12 | −0.13 | 1.00 | 0.04 | 0.95 | −0.49 | |
| 13 | 0.53 | 1.40 | 4.04 | 1.38 | 3.60 | |
| 14 | Deleted | |||||
| 15 | 0.48 | 0.89 | −1.24 | 0.90 | −1.02 | |
| 16 | Deleted | |||||
| 17 | −0.12 | 0.98 | −0.22 | 0.95 | −0.46 | |
| Cooperative play | 18 | 0.94 | 0.92 | −0.97 | 0.94 | −0.68 |
| 19 | 0.67 | 1.15 | 1.65 | 1.16 | 1.64 | |
| 20 | 1.06 | 0.88 | −1.46 | 0.90 | −1.10 | |
| 21 | 1.07 | 0.90 | −1.26 | 0.89 | −1.19 | |
| 22 | −0.53 | 0.68 | −3.85 | 0.63 | −3.99 | |
| 23 | −0.49 | 0.94 | −0.68 | 0.88 | −1.15 | |
| 24 | −0.11 | 0.88 | −1.35 | 0.84 | −1.70 | |
| 25 | −0.60 | 0.68 | −3.95 | 0.62 | −4.18 | |
| 26 | −0.40 | 1.03 | 0.39 | 0.98 | −0.15 | |
| 27 | −0.33 | 0.91 | −0.93 | 0.89 | −1.10 | |
| 28 | −1.64 | 1.21 | 2.38 | 1.14 | 1.07 | |
| 29 | −0.27 | 1.12 | 1.29 | 1.01 | 0.17 | |
| 30 | 0.97 | 1.04 | 0.47 | 1.10 | 1.13 | |
| 31 | 0.45 | 1.10 | 1.11 | 1.02 | 0.29 | |
| 32 | −0.97 | 1.05 | 0.59 | 0.99 | −0.03 | |
| 33 | Deleted | |||||
| 34 | −0.13 | 1.16 | 1.70 | 1.18 | 1.69 | |
| 35 | 0.69 | 0.85 | −1.79 | 0.88 | −1.27 | |
| 36 | −0.53 | 1.32 | 3.21 | 1.27 | 2.42 | |
| 37 | 0.19 | 1.25 | 2.59 | 1.35 | 3.24 | |
| 38 | 0.15 | 0.85 | −1.74 | 0.89 | −1.14 | |
| 39 | 0.77 | 0.91 | −1.02 | 0.94 | −0.60 | |
| 40 | −0.97 | 1.05 | 0.57 | 0.98 | −0.11 | |
| Category | Obs. Average | Infit MNSQ | Outfit MNSQ | Structure Calibration | |
|---|---|---|---|---|---|
| Associative play | 1 | −2.01 | 1.18 | 1.30 | None |
| 2 | −0.01 | 1.02 | 1.00 | −3.64 | |
| 3 | 1.80 | 0.99 | 0.92 | −0.61 | |
| 4 | 4.57 | 0.97 | 0.95 | 4.25 | |
| Cooperative play | 1 | −4.00 | 0.81 | 0.77 | None |
| 2 | −0.41 | 1.01 | 0.98 | −4.02 | |
| 3 | 1.73 | 1.00 | 0.98 | −0.73 | |
| 4 | 5.15 | 1.01 | 0.95 | 4.75 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.-H.; Hong, I.; Park, H.Y. Development of a Social Play Evaluation Tool for Preschool Children. Healthcare 2022, 10, 102. https://doi.org/10.3390/healthcare10010102
Lee S-H, Hong I, Park HY. Development of a Social Play Evaluation Tool for Preschool Children. Healthcare. 2022; 10(1):102. https://doi.org/10.3390/healthcare10010102
Chicago/Turabian StyleLee, Sun-Hee, Ickpyo Hong, and Hae Yean Park. 2022. "Development of a Social Play Evaluation Tool for Preschool Children" Healthcare 10, no. 1: 102. https://doi.org/10.3390/healthcare10010102
APA StyleLee, S.-H., Hong, I., & Park, H. Y. (2022). Development of a Social Play Evaluation Tool for Preschool Children. Healthcare, 10(1), 102. https://doi.org/10.3390/healthcare10010102