
Brain Metastasis Response to Stereotactic Radio Surgery: A Mathematical Approach

 ,
,  , ,
, ,  , , and
, , and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Mathematical Model and Methods
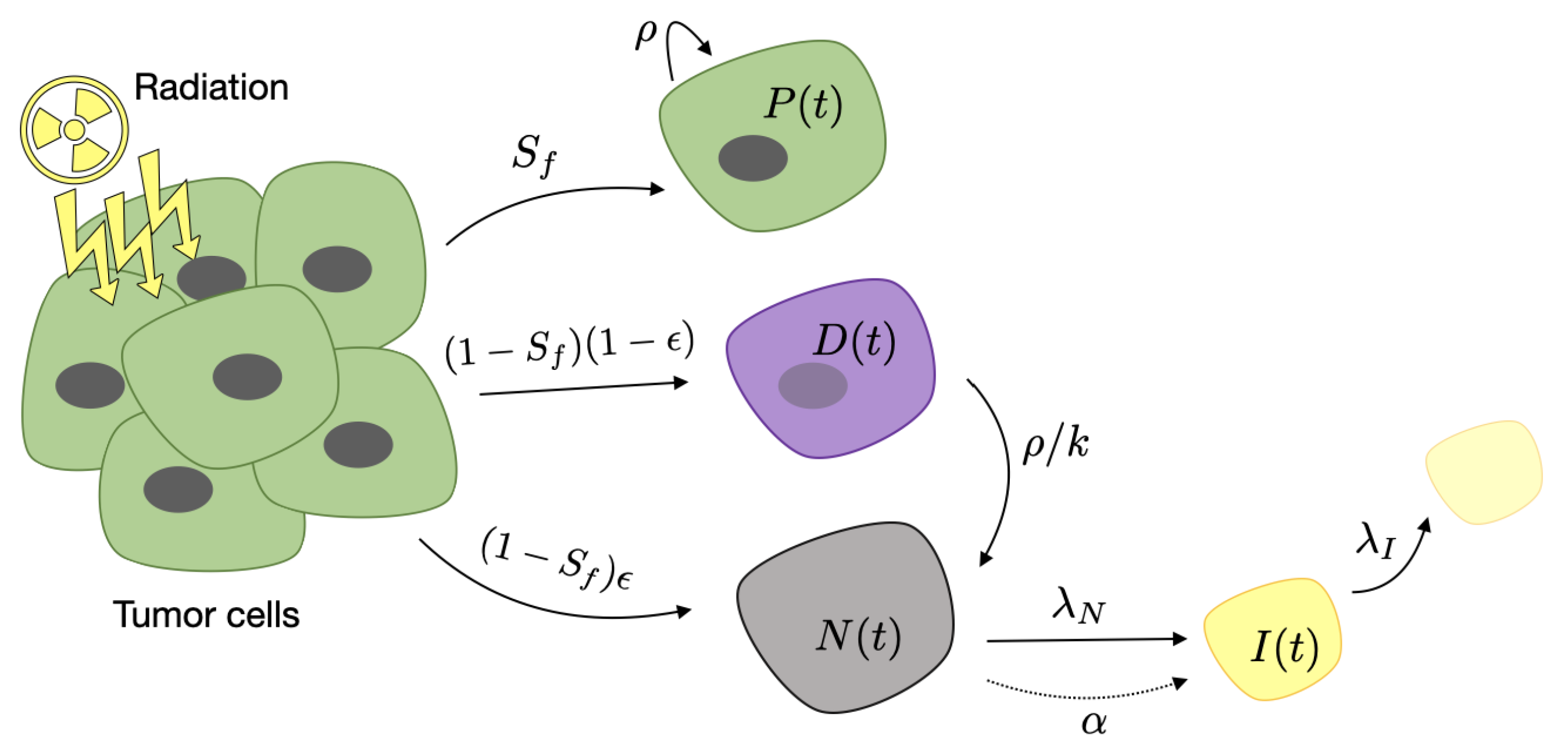
2.1. Mathematical Model of Response to Radiosurgery
2.2. Patients
2.3. Tumor Segmentation
3. Results
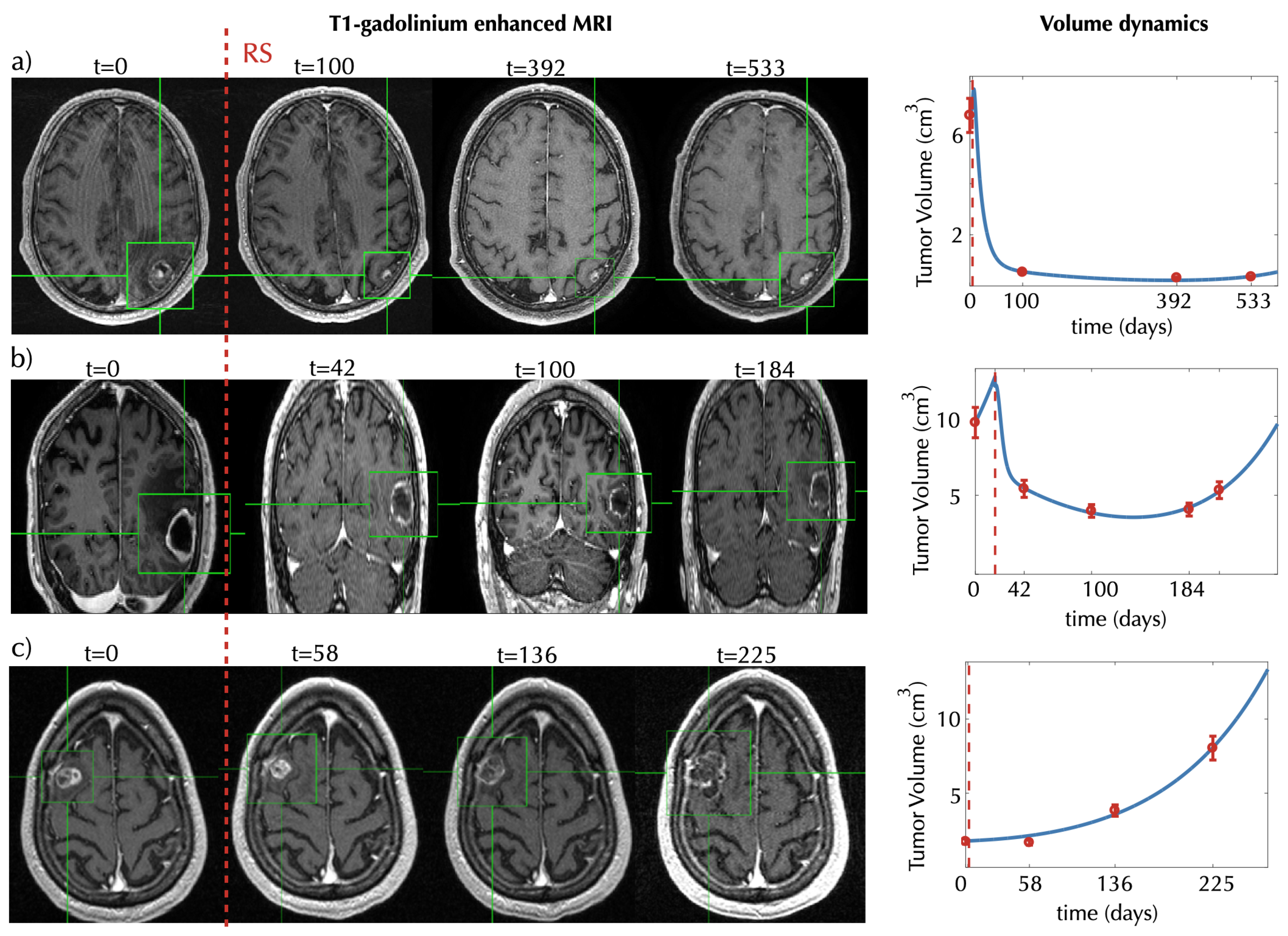
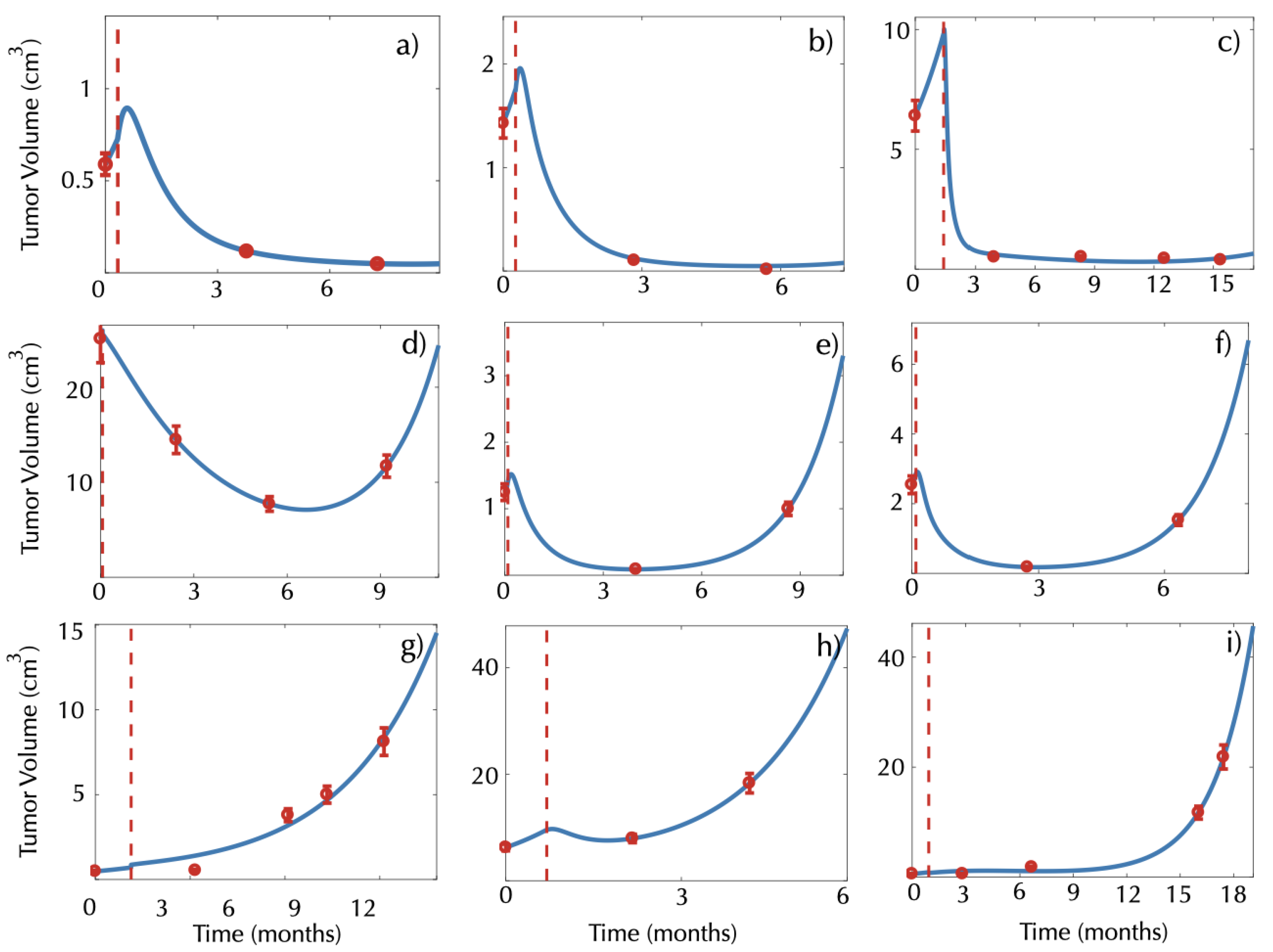
3.1. Mathematical Model Describe the Response to Radiosurgery
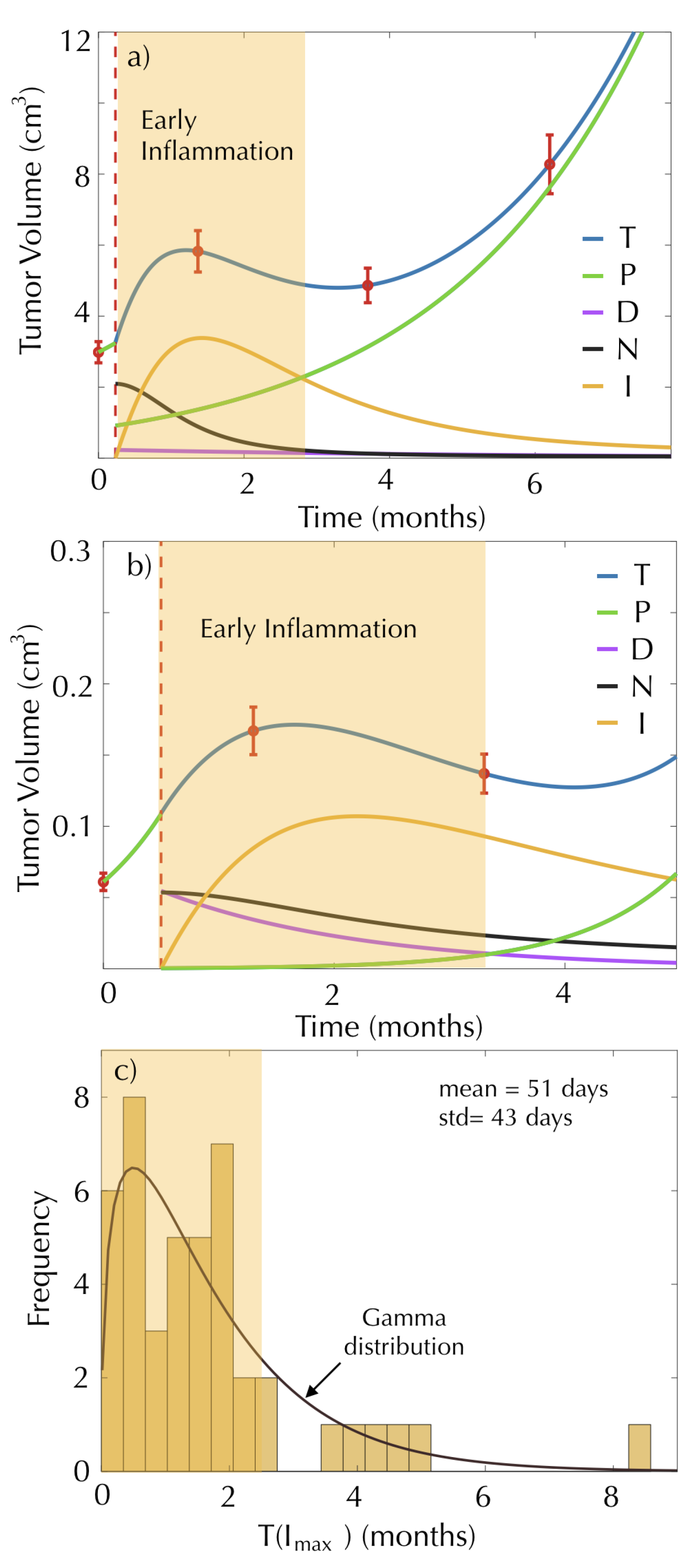
3.2. The Mathematical Model Describes the Early Inflammatory Dynamics Observed in the Post-SRS Response
3.3. Damage to Healthy Tissue Could Lead to Late Inflammatory Response and Radiation Necrosis
3.4. Time to Tumor Progression Can Be Obtained from the Mathematical Model
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BMs | Brain Metastases |
| SRS | Stereotactic Radio Surgery |
| RT | Radiation Therapy |
| MRI | Magnetic Resonance Imaging |
Appendix A

References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics. CA Cancer J. Clin. 2016, 66, 7–30. [Google Scholar] [CrossRef]
- Clairambault, J. Optimizing cancer pharmacotherapeutics using mathematical modeling and a systems biology approach. Pers. Med. 2011, 8, 271–286. [Google Scholar] [CrossRef]
- Jackson, T.; Komarova, N.; Swanson, K. Mathematical oncology: Using mathematics to enable cancer discoveries. Am. Math. Month. 2014, 121, 840–856. [Google Scholar] [CrossRef]
- Altrock, P.M.; Liu, L.L.; Michor, F. The mathematics of cancer: Integrating quantitative models. Nat. Rev. Cancer 2016, 15, 730–745. [Google Scholar] [CrossRef]
- Pérez-García, V.M.; Fitzpatrick, S.; Pérez-Romasanta, L.A.; Pesic, M.; Schucht, P.; Arana, E.; Sánchez-Gómez, P. Applied mathematics and nonlinear sciences in the war on cancer. Appl. Math. Nonlinear Sci. 2016, 1, 423–436. [Google Scholar] [CrossRef]
- Fox, B.D.; Cheung, V.J.; Patel, A.J.; Suki, D.; Rao, G. Epidemiology of metastatic brain tumors. Neurosurg. Clin. N. Am. 2011, 22, 1–6. [Google Scholar] [CrossRef]
- Venkatesan, P. SRS is non-inferior to WBRT for brain metastases. Lancet Oncol. 2018, 19, e386. [Google Scholar] [CrossRef]
- Iwata, K.; Kawasaki, K.; Shigesada, N. A dynamical model for the growth and size distribution of multiple metastatic tumors. J. Theor. Biol. 2000, 203, 177–186. [Google Scholar] [CrossRef]
- Hartung, N.; Mollard, S.; Barbolosi, D.; Benabdallah, A.; Chapuisat, G.; Henry, G.; Giacometti, S.; Iliadis, A.; Ciccolini, J.; Faivre, C.; et al. Mathematical modeling of tumor growth and metastatic spreading: Validation in tumor-bearing mice. Cancer Res. 2014, 74, 6397–6407. [Google Scholar] [CrossRef]
- Barbolosi, D.; Benabdallah, A.; Hubert, F.; Verga, F. Mathematical and numerical analysis for a model of growing metastatic tumors. Math. Biosci. 2009, 218, 1–14. [Google Scholar] [CrossRef]
- Barbolosi, D.; Summer, I.; Meille, C.; Serre, R.; Kelly, A.; Zerdoud, S.; Bournaud, C.; Schvartz, C.; Toubeau, M.; Toubert, M.E.; et al. Modeling therapeutic response to radioiodine in metastatic thyroid cancer: A proof-of-concept study for individualized medicine. Oncotarget 2017, 8, 39167–39176. [Google Scholar] [CrossRef]
- Mollard, S.; Ciccolini, J.; Imbs, D.C.; El Cheikh, R.; Barbolosi, D.; Benzekry, S. Model driven optimization of antiangiogenics + cytotoxics combination: Application to breast cancer mice treated with bevacizumab + paclitaxel doublet leads to reduced tumor growth and fewer metastasis. Oncotarget 2017, 8, 23087–23098. [Google Scholar] [CrossRef]
- Bilous, M.; Serdjebi, C.; Boyer, A.; Tomasini, P.; Pouypoudat, C.; Barbolosi, D.; Barlesi, F.; Chomy, F.; Benzekry, S. Quantitative mathematical modeling of clinical brain metastasis dynamics in non-small cell lung cancer. Sci. Rep. 2019, 9, 13018. [Google Scholar] [CrossRef]
- Brodland, G.W.; Veldhuis, J.H. The mechanics of metastasis: Insights from a computational model. PLoS ONE 2012, 7, e44281. [Google Scholar] [CrossRef]
- Chen, L.L.; Blumm, N.; Christakis, N.A.; Barabási, A.L.; Deisboeck, T.S. Cancer metastasis networks and the prediction of progression patterns. Br. J. Cancer 2009, 101, 749–758. [Google Scholar] [CrossRef] [PubMed]
- Newton, P.K.; Mason, J.; Bethel, K.; Bazhenova, L.; Nieva, J.; Norton, L.; Kuhn, P. Spreaders and sponges define metastasis in lung cancer: A Markov chain Monte Carlo mathematical model. Cancer Res. 2013, 73, 2760–2769. [Google Scholar] [CrossRef]
- Scott, J.G.; Basanta, D.; Anderson, A.R.; Gerlee, P. A mathematical model of tumour self-seeding reveals secondary metastatic deposits as drivers of primary tumour growth. J. R. Soc. Interface 2013, 10, 20130011. [Google Scholar] [CrossRef]
- Newton, P.K.; Mason, J.; Bethel, K.; Bazhenova, L.A.; Nieva, J.; Kuhn, P. A stochastic Markov chain model to describe lung cancer growth and metastasis. PLoS ONE 2012, 7, e34637. [Google Scholar] [CrossRef]
- Diego, D.; Calvo, G.F.; Pérez-García, V.M. Modeling the connection between primary and metastatic tumors. J. Math. Biol. 2013, 67, 657–692. [Google Scholar] [CrossRef]
- Haeno, H.; Gonen, M.; Davis, M.B.; Herman, J.M.; Iacobuzio-Donahue, C.A.; Michor, F. Computational modeling of pancreatic cancer reveals kinetics of metastasis suggesting optimum treatment strategies. Cell 2012, 148, 362–375. [Google Scholar] [CrossRef]
- Watanabe, Y.; Dahlman, E.L.; Leder, K.Z.; Hui, S.K. A mathematical model of tumor growth and its response to single irradiation. Theor. Biol. Med. Model. 2016, 13, 6. [Google Scholar] [CrossRef]
- Dehghan, M.; Narimani, N. Radial basis function-generated finite difference scheme for simulating the brain cancer growth model under radiotherapy in various types of computational domains. Comput. Methods Programs Biomed. 2020, 195, 105641. [Google Scholar] [CrossRef]
- Leder, K.; Pitter, K.; Laplant, Q.; Hambardzumyan, D.; Ross, B.D.; Chan, T.A.; Holland, E.C.; Michor, F. Mathematical modeling of PDGF-driven glioblastoma reveals optimized radiation dosing schedules. Cell 2014, 156, 603–616. [Google Scholar] [CrossRef]
- Eikenberry, S.E.; Kuang, Y. Virtual glioblastoma: Growth, migration and treatment in a three-dimensional model. Cell Prolif. 2009, 42, 511–528. [Google Scholar] [CrossRef]
- Rockne, R.; Alvord, E.C., Jr.; Rockhill, J.K.; Swanson, K.R. A mathematical model for brain tumor response to radiation therapy. J. Math. Biol. 2009, 59, 561. [Google Scholar] [CrossRef]
- Rockne, R.; Rockhill, J.; Mrugala, M.; Spence, M.; Kalet, I.; Hendrickson, K.; Lai, A.; Cloughesy, T.; Alvord, C.; Swanson, K. Predicting the efficacy of radiotherapy in individual glioblastoma patients in vivo: A mathematical modeling approach. Phys. Med. Biol. 2010, 55, 3271–3285. [Google Scholar] [CrossRef] [PubMed]
- Nazari, A.J.; Sardari, D.; Vali, A.R.; Maghooli, K. Computer implementation of a new therapeutic model for GBM tumor. Comput. Math. Methods Med. 2014, 2014, 481935. [Google Scholar] [CrossRef]
- Martínez-González, A.; Durán-Prado, M.; Calvo, G.F.; Alcain, F.J.; Pérez-Romasanta, L.A.; Pérez-García, V.M. Combined therapies of antithrombotics and antioxidants delay in silico brain tumour progression. Math. Med. Biol. 2015, 32, 239–262. [Google Scholar] [CrossRef] [PubMed]
- Yu, V.Y.; Nguyen, D.; Pajonk, F.; Kupelian, P.; Kaprealian, T.; Selch, M.; Low, D.A.; Sheng, K. Incorporating cancer stem cells in radiation therapy treatment response modeling and the implication in glioblastoma multiforme treatment resistance. Int. J. Radiat. Oncol. Biol. Phys. 2015, 91, 866–875. [Google Scholar] [CrossRef]
- Borasi, G.; Nahum, A. Modelling the radiotherapy effect in the reaction-diffusion equation. Eur. J. Med. Phys. 2016, 32, 1175–1179. [Google Scholar] [CrossRef]
- Chakwizira, A.; Ahlstedt, J.; Redebrandt, H.N.; Ceberg, C. Mathematical modelling of the synergistic combination of radiotherapy and indoleamine-2,3-dioxygenase (IDO) inhibitory immunotherapy against glioblastoma. Br. J. Radiol. 2018, 91, 1087. [Google Scholar] [CrossRef]
- Hawkins-Daarud, A.; Rockne, R.; Corwin, D.; Anderson, A.R.A.; Kinahan, P.; Swanson, K.R. In silico analysis suggests differential response to bevacizumab and radiation combination therapy in newly diagnosed glioblastoma. J. R. Soc. Interface 2015, 12, 20150388. [Google Scholar] [CrossRef]
- Ribba, B.; Kaloshi, G.; Peyre, M.; Ricard, D.; Calvez, V.; Tod, M.; Cajavec-Bernard, B.; Idbaih, A.; Psimaras, D.; Dainese, L.; et al. A tumor growth inhibition model for low-grade glioma treated with chemotherapy or radiotherapy. Clin. Cancer Res. 2012, 15, 5071–5080. [Google Scholar] [CrossRef]
- Badoual, M.; Gerin, C.; Derouler, C.; Grammaticos, B.; Llitjos, J.F.; Oppenheim, C.; Varlet, P.; Pallud, J. Oedema-based model for diffuse low-grade gliomas: Application to clinical cases under radiotherapy. Cell Prolif. 2014, 47, 369–380. [Google Scholar] [CrossRef]
- Pérez-García, V.M.; Bogdanska, M.; Martínez-González, A.; Belmonte-Beitia, J.; Schucht, P.; Pérez-Romasanta, L.A. Delay effects in the response of low-grade gliomas to radiotherapy: A mathematical model and its therapeutical implications. Math. Biol. Med. 2015, 32, 307–329. [Google Scholar] [CrossRef]
- Galochkina, T.; Bratus, A.; Pérez-García, V.M. Optimal radiotherapy protocol for low-grade gliomas: Insights from a mathematical model. Math. Biosci. 2015, 267, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Henares-Molina, A.; Benzekry, S.; Lara, P.C.; García-Rojo, M.; Pérez-García, V.M.; Martínez-González, A. Non-standard radiotherapy fractionations delay the time to malignant transformation of low-grade gliomas. PLoS ONE 2017, 12, e0178552. [Google Scholar] [CrossRef] [PubMed]
- Pérez-García, V.M.; Pérez-Romasanta, L.A. Extreme protraction for low-grade gliomas: Theoretical proof of concept of a novel therapeutical strategy. Math. Med. Biol. 2016, 33, 253–271. [Google Scholar] [CrossRef] [PubMed]
- Sperduto, P.W.; Kased, N.; Roberge, D.; Xu, Z.; Shanley, R.; Luo, X.; Sneed, P.K.; Chao, S.T.; Weil, R.J.; Suh, J.; et al. Summary report on the graded prognostic assessment: An accurate and facile diagnosis- specific tool to estimate survival for patients with brain metastases. J. Clin. Oncol. 2012, 30, 419–425. [Google Scholar] [CrossRef]
- Swanson, K.R.; Harpold, H.L.P.; Peacock, D.L.; Rockne, R.; Pennington, C.; Kilbride, L.; Grant, R.; Wardlaw, J.M.; Alvord, E.C., Jr. Velocity of radial expansion of contrast-enhancing gliomas and the effectiveness of radiotherapy in individual patients: A proof of principle. Clin. Oncol. 2008, 20, 301–308. [Google Scholar] [CrossRef]
- Wang, C.H.; Rockhill, J.K.; Mrugala, M.; Peacock, D.L.; Lai, A.; Jusenius, K.; Wardlaw, J.M.; Cloughesy, T.; Spence, A.; Rockne, R.; et al. Prognostic significance of growth kinetics in newly diagnosed glioblastomas revealed by combining serial imaging with a novel biomathematical model. Cancer Res. 2009, 69, 9133–9140. [Google Scholar] [CrossRef]
- Pérez-Beteta, J.; Molina-García, D.; Martínez-González, A.; Henares-Molina, A.; Amo-Salas, M.; Luque, B.; Arregui, E.; Calvo, M.; Borrás, J.M.; Martino, J.; et al. Morphological MRI-based features provide pretreatment and post-surgery survival prediction in glioblastoma. Eur. Radiol. 2019, 29, 1968–1977. [Google Scholar] [CrossRef]
- Pérez-Beteta, J.; Molina, D.; Villena, M.; Rodríguez, M.J.; Velásquez, C.; Martino, J.; Meléndez-Asensio, B.; Rodríguez de Lope, Á.; Morcillo, R.; Sepúlveda, J.M.; et al. Morphologic features on MR imaging classify multifocal glioblastomas in different prognostic groups. Am. J. Neuro-Radiol. 2019, 40, 634–640. [Google Scholar] [CrossRef]
- Massey, S.C.; White, H.; Whitmire, P.; Doyle, T.; Johnston, S.K.; Singleton, K.W.; Jackson, P.R.; Hawkins-Daarud, A.; Bendok, B.R.; Porter, A.B.; et al. Image-based metric of invasiveness predicts response to adjuvant temozolomide for primary glioblastoma. PLoS ONE 2020, 15, e0230492. [Google Scholar] [CrossRef]
- Pérez-Beteta, J.; Molina-García, D.; Ortiz-Alhambra, J.A.; Fernández-Romero, A.; Luque, B.; Arregui, E.; Calvo, M.; Borrás, J.M.; Meléndez, B.; Rodríguez de Lope, Á.; et al. Tumor surface regularity at MR imaging predicts survival and response to surgery in patients with glioblastoma. Radiology 2018, 288, 218–225. [Google Scholar] [CrossRef]
- Amelot, A.; Deroulers, C.; Badoual, M.; Polivka, M.; Adle-Biassette, H.; Houdart, E.; Carpentier, A.F.; Froelich, S.; Mandonnet, E. Surgical decision making from image-based biophysical modeling of glioblastoma: Not ready for primetime. Neurosurgery 2017, 80, 793–799. [Google Scholar] [CrossRef]
- Pérez-García, V.M.; Calvo, G.F.; Bosque, J.J.; León-Triana, O.; Jiménez, J.; Pérez-Beteta, J.; Belmonte-Beitia, J.; Valiente, M.; Zhu, L.; García-Gómez, P.; et al. Universal scaling laws rule explosive growth in human cancers. Nat. Phys. 2020, 16, 1232–1237. [Google Scholar] [CrossRef]
- Joiner., M.C.; Van der Kogel, A.J. Basic Clinical Radiobiology; CRC Press: Boca Raton, FL, USA, 2018. [Google Scholar]
- Lorenzo, G.; Pérez-García, V.M.; Mariño, A.; Pérez-Romasanta, L.A.; Reali, A.; Gomez, H. Mechanistic modelling of prostate- specific antigen dynamics shows potential for personalized prediction of radiation therapy outcome. J. R. Soc. Interface 2019, 16, 20190195. [Google Scholar] [CrossRef]
- Kim, M.S.; Kim, W.; Park, I.H.; Kim, H.J.; Lee, E.; Jung, J.H.; Cho, L.C.; Song, C.W. Radiobiological mechanisms of stereotactic body radiation therapy and stereotactic radiation surgery. Radiat. Oncol. J. 2015, 33, 265–275. [Google Scholar] [CrossRef]
- Brown, J.M.; Carlson, D.J.; Brenner, D.J. The tumor radiobiology of SRS and SBRT: Are more than the 5 Rs involved? Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 254–262. [Google Scholar] [CrossRef]
- Rock, K.L.; Kono, H. The inflammatory response to cell death. Annu. Rev. Pathol. 2008, 3, 99–126. [Google Scholar] [CrossRef]
- Berghoff, A.S.; Lassmann, H.; Preusser, M.; Höftberger, R. Characterization of the inflammatory response to solid cancer metastases in the human brain. Clin. Exp. Metastasis 2013, 30, 69–81. [Google Scholar] [CrossRef]
- Jiang, J.; Wu, L.; Yuan, F.; Ji, J.; Lin, X.; Yang, W.; Wu, J.; Shi, M.; Yang, H.; Ma, Y.; et al. Characterization of the immune microenvironment in brain metastases from different solid tumors. Cancer Med. 2020, 9, 2299–2308. [Google Scholar] [CrossRef]
- Kudo, Y.; Haymaker, C.; Zhang, J.; Reuben, A.; Duose, D.Y.; Fujimoto, J.; Roy-Chowdhuri, S.; Solis Soto, L.M.; Dejima, H.; Parra, E.R.; et al. Suppressed immune microenvironment and repertoire in brain metastases from patients with resected non-small-cell lung cancer. Ann. Oncol. 2019, 30, 1521–1530. [Google Scholar] [CrossRef]
- Vellayappan, B.; Tan, C.L.; Yong, C.; Khor, L.K.; Koh, W.Y.; Yeo, T.T.; Detsky, J.; Lo, S.; Sahgal, A. Diagnosis and management of radiation necrosis in patients with brain metastases. Front. Oncol. 2018, 8, 395. [Google Scholar] [CrossRef]
- Kohutek, Z.A.; Yamada, Y.; Chan, T.A.; Brennan, C.W.; Tabar, V.; Gutin, P.H.; Yang, T.J.; Rosenblum, M.K.; Ballangrud, Å.; Young, R.J.; et al. Long-term risk of radionecrosis and imaging changes after stereotactic radiosurgery for brain metastases. J. Neurooncol. 2015, 125, 149–156. [Google Scholar] [CrossRef]
- Donovan, E.K.; Parpia, S.; Greenspoon, J.N. Incidence of radionecrosis in single-fraction radiosurgery compared with fractionated radiotherapy in the treatment of brain metastasis. Curr. Oncol. 2019, 26, e328–e333. [Google Scholar] [CrossRef]
- Liu, Y.; Ye, G.; Huang, L.; Zhang, C.; Sheng, Y.; Wu, B.; Han, L.; Wu, C.; Dong, B.; Qi, Y. Single-cell transcriptome analysis demonstrates inter-patient and intra-tumor heterogeneity in primary and metastatic lung adenocarcinoma. Aging 2020, 12, 21559–21581. [Google Scholar] [CrossRef]
- Shih, D.J.H.; Nayyar, N.; Bihun, I.; Dagogo-Jack, I.; Gill, C.M.; Aquilanti, E.; Bertalan, M.; Kaplan, A.; D’Andrea, M.R.; Chukwueke, U.; et al. Genomic characterization of human brain metastases identifies drivers of metastatic lung adenocarcinoma. Nat Genet 2020, 52, 371–377. [Google Scholar] [CrossRef]
- Perus, L.J.M.; Walsh, L.A. Microenvironmental heterogeneity in brain malignancies. Front. Immunol. 2019, 10, 2294. [Google Scholar] [CrossRef]
- Akimoto, T.; Hunter, N.R.; Buchmiller, L.; Mason, K.; Ang, K.K.; Milas, L. Inverse relationship between epidermal growth factor receptor expression and radiocurability of murine carcinomas. Clin. Cancer Res. 1999, 5, 2884–2890. [Google Scholar]
- Choi, S.H.; Yang, H.; Lee, S.H.; Ki, J.H.; Nam, D.H.; Yoo, H.Y. TopBP1 and Claspin contribute to the radioresistance of lung cancer brain metastases. Mol. Cancer. 2014, 13, 211. [Google Scholar] [CrossRef]
- Stella, G.M.; Corino, A.; Berzero, G.; Kolling, S.; Filippi, A.R.; Benvenuti, S. Brain metastases from lung cancer: Is MET an actionable target? Cancers 2019, 11, 271. [Google Scholar] [CrossRef]
- Duregon, E.; Senetta, R.; Pittaro, A.; Verdun di Cantogno, L.; Stella, G.; De Blasi, P.; Zorzetto, M.; Mantovani, C.; Papotti, M.; Cassoni, P. CAVEOLIN-1 expression in brain metastasis from lung cancer predicts worse outcome and radioresistance, irrespective of tumor histotype. Oncotarget 2015, 6, 29626–29636. [Google Scholar] [CrossRef][Green Version]
- Soffietti, R.; Ahluwalia, M.; Lin, N.; Rudà, R. Management of brain metastases according to molecular subtypes. Nat. Rev. Neurol. 2020, 16, 557–574. [Google Scholar] [CrossRef]
- Ahmed, K.A.; Berglund, A.E.; Welsh, E.A.; Naghavi, A.O.; Kim, Y.; Yu, M.; Robinson, T.J.; Eschrich, S.A.; Johnstone, P.A.S.; Torres-Roca, J.F. The radiosensitivity of brain metastases based upon primary histology utilizing a multigene index of tumor radiosensitivity. Neuro Oncol. 2017, 19, 1145–1146. [Google Scholar] [CrossRef]
- Smart, D.; Garcia-Glaessner, A.; Palmieri, D.; Wong-Goodrich, S.J.; Kramp, T.; Gril, B.; Shukla, S.; Lyle, T.; Hua, E.; Cameron, H.A.; et al. Analysis of radiation therapy in a model of triple-negative breast cancer brain metastasis. Clin. Exp. Metastasis 2015, 32, 717–727. [Google Scholar] [CrossRef]
- Voglstaetter, M.; Thomsen, A.R.; Nouvel, J.; Koch, A.; Jank, P.; Navarro, E.G.; Gainey-Schleicher, T.; Khanduri, R.; Groß, A.; Rossner, F.; et al. Tspan8 is expressed in breast cancer and regulates E-cadherin/catenin signalling and metastasis accompanied by increased circulating extracellular vesicles. J. Pathol. 2019, 248, 421–437. [Google Scholar] [CrossRef]
- Wingrove, E.; Liu, Z.Z.; Patel, K.D.; Arnal-Estapé, A.; Cai, W.L.; Melnick, M.A.; Politi, K.; Monteiro, C.; Zhu, L.; Valiente, M.; et al. Transcriptomic hallmarks of tumor plasticity and stromal interactions in brain metastasis. Cell Rep. 2019, 27, 1277–1292.e7. [Google Scholar] [CrossRef]
- Toma-Dasu, I.; Dasu, A. Modelling Tumour Oxygenation, Reoxygenation and Implications on Treatment. Comput. Math. Methods Med. 2013, 141087. [Google Scholar] [CrossRef]
- Rockne, R.C.; Trister, A.D.; Jacobs, J.; Hawkins-Daarud, A.J.; Nean, M.L.; Hendrickson, K.; Mrugala, M.M.; Rockhill, J.K.; Kinahan, P.; Krohn, K.A.; et al. A patient-specific computational model of hypoxia-modulated radiation resistance in glioblastoma using 18F-FMISO-PET. J. R. Soc. Interface 2015, 12, 20141174. [Google Scholar] [CrossRef] [PubMed]
- Lewin, T.D.; Maini, P.K.; Moros, E.G.; Enderling, H.; Byrne, H.M. The evolution of tumour composition during fractionated radiotherapy: Implications for outcome. Bull. Math. Biol. 2018, 80, 1207–1235. [Google Scholar] [CrossRef]
- Kuznetsov, M.; Kolobov, A. Optimization of dose fractionation for radiotherapy of a solid tumor with account of oxygen effect and proliferative heterogeneity. Mathematics 2020, 8, 1204. [Google Scholar] [CrossRef]
- Hessel, F.; Petersen, C.; Zips, D.; Krause, M.; Pfitzmann, D.; Thames, H.D.; Baumann, M. Impact of increased cell loss on the repopulation rate during fractionated irradiation in human FaDu squamous cell carcinoma growing in nude mice. Int. J. Radiat. Biol. 2003, 79, 479–486. [Google Scholar] [CrossRef]
- Hanin, L.; Rose, J. Suppression of metastasis by primary tumor and ac- celeration of metastasis following primary tumor resection: A natural law? Bull. Math. Biol. 2018, 80, 519–539. [Google Scholar] [CrossRef]
- Franssen, L.C.; Lorenzi, T.; Burgess, A.E.F.; Chaplain, M.A.J. A mathematical framework for modelling the metastatic spread of cancer. Bull. Math. Biol. 2019, 81, 1965–2010. [Google Scholar] [CrossRef]
- Hanin, L.; Zaider, M. A mechanistic description of radiation-induced damage to normal tissue and its healing kinetics. Phys. Med. Biol. 2013, 58, 825–839. [Google Scholar] [CrossRef] [PubMed]
- Essig, M.; Waschkies, M.; Wenz, F.; Debus, J.; Hentrich, H.R.; Knopp, M.V. Assessment of brain metastases with dynamic susceptibility-weighted contrast-enhanced MR imaging: Initial results. Radiology 2003, 228, 193–199. [Google Scholar] [CrossRef]
- Barajas, R.F.; Chang, J.S.; Sneed, P.K.; Segal, M.R.; McDermott, M.W.; Cha, S. Distinguishing recurrent intra-axial metastatic tumor from radiation necrosis following gamma knife radiosurgery using dynamic susceptibility-weighted contrast-enhanced perfusion MR imaging. AJNR Am. J. Neuroradiol. 2009, 30, 367–372. [Google Scholar] [CrossRef]
- Salkeld, A.L.; Hau, E.K.C.; Nahar, N.; Sykes, J.R.; Wang, W.; Thwaites, D.I. Changes in brain metastasis during radiosurgical planning. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, 727–733. [Google Scholar] [CrossRef]
- Garcia, M.A.; Anwar, M.; Yu, Y.; Duriseti, S.; Merritt, B.; Nakamura, J.; Hess, C.; Theodosopoulos, P.V.; McDermott, M.; Sneed, P.K.; et al. Brain metastasis growth on preradiosurgical magnetic resonance imaging. Pract. Radiat. Oncol. 2018, 8, e369–e376. [Google Scholar] [CrossRef] [PubMed]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
León-Triana, O.; Pérez-Beteta , J.; Albillo, D.; Ortiz de Mendivil, A.; Pérez-Romasanta, L.; González-Del Portillo, E.; Llorente, M.; Carballo, N.; Arana, E.; Pérez-García, V.M. Brain Metastasis Response to Stereotactic Radio Surgery: A Mathematical Approach. Mathematics 2021, 9, 716. https://doi.org/10.3390/math9070716
León-Triana O, Pérez-Beteta J, Albillo D, Ortiz de Mendivil A, Pérez-Romasanta L, González-Del Portillo E, Llorente M, Carballo N, Arana E, Pérez-García VM. Brain Metastasis Response to Stereotactic Radio Surgery: A Mathematical Approach. Mathematics. 2021; 9(7):716. https://doi.org/10.3390/math9070716
Chicago/Turabian StyleLeón-Triana, Odelaisy, Julián Pérez-Beteta , David Albillo, Ana Ortiz de Mendivil, Luis Pérez-Romasanta, Elisabet González-Del Portillo, Manuel Llorente, Natalia Carballo, Estanislao Arana, and Víctor M. Pérez-García. 2021. "Brain Metastasis Response to Stereotactic Radio Surgery: A Mathematical Approach" Mathematics 9, no. 7: 716. https://doi.org/10.3390/math9070716
APA StyleLeón-Triana, O., Pérez-Beteta , J., Albillo, D., Ortiz de Mendivil, A., Pérez-Romasanta, L., González-Del Portillo, E., Llorente, M., Carballo, N., Arana, E., & Pérez-García, V. M. (2021). Brain Metastasis Response to Stereotactic Radio Surgery: A Mathematical Approach. Mathematics, 9(7), 716. https://doi.org/10.3390/math9070716