1. Introduction
Medical diagnosis is a process that directly affects people’s health and lives. One main task in medical science is to obtain an accurate diagnosis [
1]. Many scholars have conducted extensive research to find suitable methods for improving the accuracy of medical diagnosis [
2,
3,
4,
5,
6]. Medical diagnosis for critical diseases is a complex decision-making problem that contains a great deal of symptom analysis. Therefore, a doctor may find it difficult to draw firm conclusions about such diseases without the assistance of their colleagues when assessing the health problem and providing precise diagnosis [
7]. Therefore, medical diagnosis is a group decision-making (GDM) problem [
8,
9]. Two main problems in the GDM process must be solved: one is obtaining evaluation information, that is, weights and evaluation values, and the other is selecting an appropriate method for aggregating this information [
10].
In the real world, this may be difficult as people may not be able to provide accurate evaluation values in complex decision-making environments. Generally, the inherent uncertainty in patient history and current signs and symptoms may make it difficult to find the precise diagnosis [
11]. As an extension of the fuzzy set (FS) [
12], the intuitionistic fuzzy set (IFS) can better describe the complexity and fuzziness of information that contains membership, non-membership, and hesitation information [
13]. Medical diagnosis models based on FS theory have been widely investigated. Li et al. applied an approach to medical diagnosis using fuzzy soft sets [
14]. Based on the ambiguity measure and Dempster–Shafer theory of evidence, a decision-making method was presented and applied to medical diagnosis [
15]. Xiao utilized a hybrid method based on fuzzy soft sets to address medical diagnoses [
16]. Thao et al. proposed the concept of a divergence measure of picture fuzzy sets and a new multi-criteria decision-making algorithm for medical diagnosis [
17]. An algorithm for medical diagnosis using score matrices has been proposed [
18]. For a double-hierarchy hesitant fuzzy linguistic environment, Zhang et al. proposed novel correlation measures for medical diagnoses in Chinese medicine [
19]. The theory of fuzzy soft matrices has also been applied in medical diagnosis [
20]. Farhadinia developed a divergence-based medical decision-making process for COVID-19 diagnosis in a hesitant fuzzy environment [
21]. A novel algorithm for the decision-making problem of neutrosophic soft sets was proposed and applied to medical diagnosis [
22]. Considering FS theory’s inherent difficulties and the inadequacy of the parametrization tool, Molodtsov put forward the concept of the soft set [
23]. Parameterization in soft set theory is expressed with the aid of words, sentences, and other forms. It is difficult to provide preferences appropriately and accurately using soft sets in uncertain situations. Maji et al. established an intuitionistic fuzzy soft set (IFSS) that integrates the advantages of soft sets and IFSs [
24]. Evaluation values in the form of IFSSs can help achieve appropriate results closer to the actual reality because IFSSs can describe decision-makers’ positive, negative, and hesitant traits. The IFSS theory has been further developed. Fuzzy information measures, which include distance measures and fuzzy entropy [
25,
26], similarity measures [
27,
28], and correlation coefficients [
29], have been widely used in medical diagnosis, pattern recognition, cluster analysis, decision analysis, and other fields. Furthermore, the approximation ideal solution (TOPSIS method) [
29], ranking priority relation (PROMETHE) [
30], and prospect theory [
31] have been developed to deal with practical problems with intuitionistic fuzzy soft information.
Aggregation of information and preferences in the GDM process is important. Various aggregation operators, which are mathematical tools for combining information, have been constructed to combine decision information in different situations. To express information more clearly and elaborately, Seikh and Mandal defined the p,q-quasirung orthopair fuzzy set and proposed its weighted averaging and geometric aggregation operators [
32]. Arora and Garg developed some intuitionistic fuzzy soft prioritized and robust aggregation operators for decision-making problems [
33,
34]. Garg and Arora proposed an intuitionistic fuzzy soft Bonferroni mean operator for integrating the different preferences [
35]. Subsequently, Hu et al. proposed a weighted intuitionistic fuzzy soft Bonferroni mean operator to solve the group medical diagnosis problem [
36]. In group medical diagnosis problems, the symptoms of a disease, which are described by certain parameters, usually interact with one another. Doctors also interact with each other when providing evaluation information. Hence, the interrelation between multi-input arguments, including different attributes or different experts, should be considered. To synthesize the comprehensive value of each parameter and identify the relationship between individual arguments, the Maclaurin symmetric mean (MSM) operator [
37] and BM operator [
38] were applied to the IFSS [
35,
39]. In the general case of the BM and MSM operators, the Muirhead mean (MM) operator can capture the intrinsic relationships between any number of arguments based on parameter variation [
40]. It can reduce the influence of relevant factors on the ranking results by eliminating the overlapping influence of non-orthogonal terms [
41]. MM operators have been found to be suitable for solving practical decision-making problems as they provide reasonable and effective fusing information. Hong et al. applied the MM operator to aggregate hesitant fuzzy information [
42]. A series of hesitant fuzzy linguistic MM operators has been proposed [
43,
44]. Zhu utilized the proposed Pythagorean fuzzy MM operators to solve multiple-criteria GDM problems [
45]. Wang studied financial investment risk appraisal models based on interval number MM operators [
46]. Novel operators were developed by applying the MM operator to interval-valued linear Diophantine fuzzy data [
47].
Generally, aggregation operators are formed using operations in various fuzzy environments. The majority of operations are algebraic, Einstein, Hamacher, etc. Based on the Archimedean t-norm, the generalized MSM aggregation operators of the IFSS, which could reflect the interrelation between the input arrangements, were given [
39]. Seikh and Mandal [
48] proposed intuitionistic fuzzy Dombi operators that prioritize variability with information operations. The Archimedean t-conorms and t-norm operations presented in a q-rung orthopair fuzzy environment have been extended and applied to MADM issues [
49]. The algebraic product and sum are the most common operations used to model intersections and unions; however, they are not unique. As another typical case of strict Archimedes
t-norms and Archimedean
t-conorms, the Einstein
t-norm and
t-conorm also have the best approximations for the sum and product. Du established aggregation operators on q-rung orthopair fuzzy values based on the Einstein operational laws [
50]. Using Einstein operations, Wang and Liu [
51] developed intuitionistic fuzzy aggregation operators. To overcome the shortcomings of the Einstein operations of the IFSs described in [
51], Garg redefined the Einstein norms and conorms of the IFSs and presented a class of intuitionistic fuzzy interactive geometric operators [
52]. Einstein operations were also applied to Pythagorean fuzzy sets [
53]. Based on the new Einstein interactive operational rules for the intuitionistic fuzzy numbers, Liu and Wang presented the intuitionistic fuzzy Einstein interactive weighted averaging operators [
54]. Arora [
55] provided the Einstein operation for IFSSs and presented the corresponding operators. Inspired by these ideas, this study extends the MM operator to IFSSs to capture the interrelation between arguments for a group medical diagnosis based on Einstein norms [
55].
Similarly, the weights of decision-makers must be considered in GDM problems. Different decision-makers have different levels of knowledge and ability; therefore, they contribute different expertise and have different importance. The weight information of the decision-makers directly affects the accuracy of the overall GDM results [
56,
57,
58]. Therefore, numerous scholars have focused more on mining and studying weight information. Different approaches have been studied to obtain weight information by considering objective or subjective factors. The subjective weights can reflect people’s preferences; therefore, the decision-making results may be very subjective and random. The objective weights depend on strong mathematical theory and can avoid the arbitrariness of decision-making results; thus, they cannot reflect the willingness of people. In this study, similarity measures of IFSSs and the comparison matrices constructed by doctors’ grades are used to obtain the objective and subjective weights of doctors, respectively. Subsequently, doctors’ comprehensive weights are obtained by combining subjective and objective factors. Moreover, considering the complexity of GDM and the knowledge limitation of decision-makers, some may not provide complete evaluation information. Das et al. utilized probabilistic weight and distance information to estimate the missing or unknown information in incomplete fuzzy soft sets [
59]. Based on the methods in [
60,
61], a minimum-trust discount coefficient model was designed to estimate the missing values in an IFSS [
62]. Qin and Ma presented a filling approach for incomplete information using the data analysis approaches of interval-valued fuzzy soft sets [
63]. Qin et al. presented a method to fill in the missing information by fully considering and employing the characteristics of the interval-valued IFSS itself [
64]. Ma et al. proposed a K-nearest neighbors data filling algorithm for the incomplete interval-valued fuzzy soft sets[
65]. Therefore, it is very necessary to study the situations where group medical diagnosis problems involve incomplete information.
Based on the considerations above, it is crucial to present a GDM model for a medical diagnosis problem with incomplete intuitionistic fuzzy soft information. The remainder of this paper is structured as follows:
Section 2 introduces some basic concepts and theories related to IFSSs and the MM mean operator. Subsequently, to identify the interrelation of the arguments, we propose an intuitionistic fuzzy soft weighted MM operator and its dual weighted MM operator based on the Einstein operations in
Section 3. Meanwhile, some properties of these presented operators are studied. In
Section 4, we propose a model for solving group medical diagnosis problems with incomplete intuitionistic fuzzy soft information based on the novel operators.
Section 5 presents a numerical example and analyzes the results to illustrate the validity, rationality, and flexibility of the proposed model. The conclusion of this paper is in
Section 6.
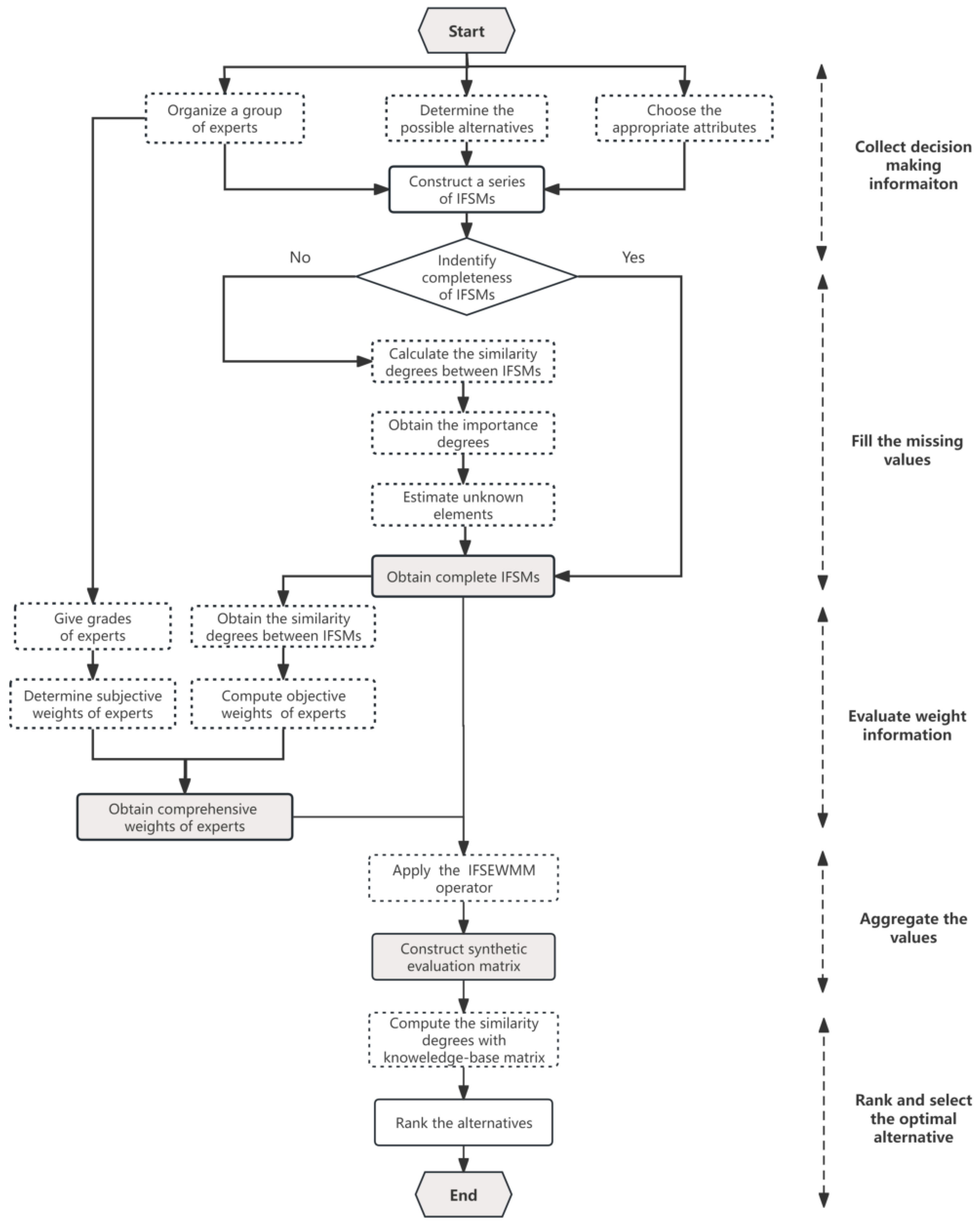
4. Group Medical Diagnosis Model with Incomplete Intuitionistic Fuzzy Soft Information
In a group medical diagnosis problem, m possible alternatives with respect to n parameters of symptoms are evaluated by q doctors . Suppose that the weight of doctor is completely unknown. The evaluation value of with respect to is an IFSN given by the doctor . These values can be constructed as a series of IFSMs . After fruitful discussions among the corresponding medical experts, a medical knowledge-base is expressed in terms of , which consists of a set of diseases and the related set of symptoms concerned with a specific disease.
In real life, doctors have different abilities, experiences, and levels; therefore, they are always classified into different grades. Without a loss of generality, we assume that doctors can be divided into nine grades; see
Table 2 for details. Moreover, owing to the complexity of medical diagnosis problems, doctors sometimes provide incomplete evaluation values. Subsequently, we address the medical diagnosis problems step by step, which is depicted in
Figure 1.
4.1. Estimation of the Missing Values of Intuitionistic Fuzzy Soft Matrices
Let
be an IFSM with incomplete information. The elements
in
can be divided into two categories: known and missing. They are denoted, respectively, as follows:
Obviously, .
Let . denotes the set of IFSMs that help estimate the missing value .
Step 1: Calculate the degree of similarity between
and the other matrices
,
where
.
Step 2: For unknown element
, obtain the importance degree of
,
Step 3: Estimate unknown element
.
According to the method above, all missing values can be determined, and the IFSMs are complete.
4.2. Evaluation of Weight Information
Based on the merits and demerits of the subjective and objective information, we use the similarity measure of complete IFSMs and doctors’ grades to obtain the objective and subjective weights, respectively. Subsequently, both weights are organically combined as the comprehensive weights of doctors to overcome the shortcomings of the single-weight method to a certain extent.
Suppose that and are the subjective and objective weight vectors of the doctors, respectively. They are both completely unknown; , and .
After obtaining the complete IFSMs using the method described in
Section 4.1, the methodology for determining the comprehensive weights of the doctors includes the following steps:
Step 1: Calculate the subjective weight of doctor .
1.1: Use doctors’ grades to construct the preference relationship of
q doctors according to the information in
Table 2.
where
is the grade of doctor
.
1.2: Determine subjective weight
of the doctor
by the analytic hierarchy process (AHP) [
67].
Step 2: Utilize Equation (
2) to obtain the similarity degrees between
given by doctor
and the other doctor’s evaluation
.
Step 3: Compute the objective weight
of doctor
using the following formula,
Step 4: Obtain the comprehensive weight of the doctor
.
The appropriate parameter
can be chosen to describe people’s preferences for the objective and subjective weights. In the doctors’ final weights, the proportion and role of
and
will vary with the change of the parameter
in Equation (
28). Different values of
may make the weights of the doctors more elastic and produce distinct results.
4.3. Approach to Group Medical Diagnosis Problem
In this subsection, we construct a model to solve group medical diagnosis problems with incomplete IFSMs, described as follows:
Step 1: Collect relevant information regarding the group medical diagnosis problems, including sets of X and E. Simultaneously, select suitable doctors and determine their grades. Later, obtain IFSM of the doctor .
Step 2: Fill in the missing values in the IFSMs (see
Section 4.1 for more details). Thus, all IFSMs have complete information.
Step 3: According to the method in
Section 4.2, the weight vector
is determined. Based on the unity of the subjective and objective weights, the comprehensive weights consider both people’s subjective preferences for doctors and objective differences between pieces of evaluation information. This will produce a more reliable medical diagnosis.
Step 4: Adopt the IFSEWMM operator
times to aggregate the values
. Construct the synthetic evaluation matrix
, where
is the synthetic evaluation value of
with respect to
:
Step 5: Compute the similarity degrees between
and
according to Equation (
2).
where
Step 6: Based on the final ranking index, select the optimal result. The larger is, the greater the disease is.




{kind=link}
{kind=link}
{kind=link}