
Cervical Precancerous Lesion Image Enhancement Based on Retinex and Histogram Equalization

Abstract
:1. Introduction
- This paper introduces the channel peak ratio and average brightness into the quantization formula of retinex, effectively improving the issue of color distortion in the multi-scale retinex (MSR) algorithm when processing cervical precancerous lesion images. The improved MSR achieves the preliminary goal of image enhancement in a simple and efficient manner.
- This paper selectively applies the contrast-limited adaptive histogram equalization (CLAHE) algorithm to the blue and green channels, which contain more detailed information, to improve the contrast between lesion areas and the background without excessive enhancement.
- Based on the characteristics of cervical precancerous lesion images, this paper selectively adopts a pixel-based dynamic weighted fusion strategy to fuse the enhanced image with the original image. This approach effectively preserves details while reducing the amplification of noise during the image enhancement process.
2. Related Work
3. Methods
3.1. Enhancement Based on the Improved MSR
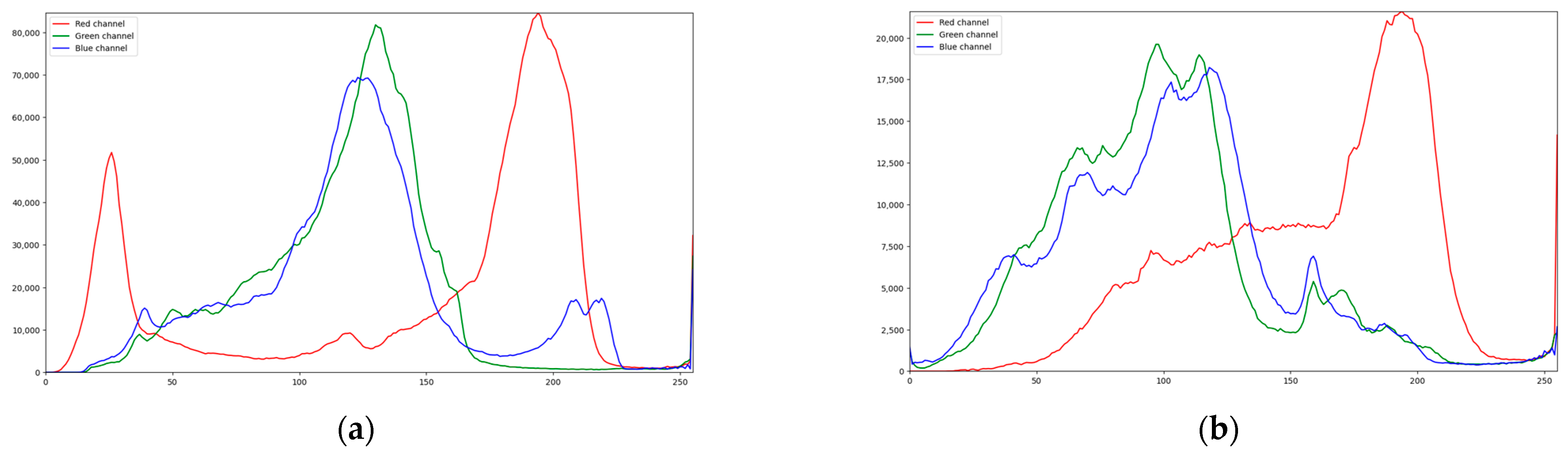
3.2. Enhancement Based on CLAHE
- The input image is divided into nonoverlapping subblocks, each of which contains pixels;
- Compute the histogram of the subblocks;
- Set the clipping threshold;
- For each subblock, use the excess pixels from the previous step to reallocate;
- Each subblock is histogram-equalized;
- The bilinear interpolation method is used to reconstruct the pixels.
3.3. Enhancement Based on Multi-Scale Detail Boosting
3.4. Enhancement Based on Dynamic Weighted Fusion
4. Experimental Results and Discussion
4.1. Experimental Setup
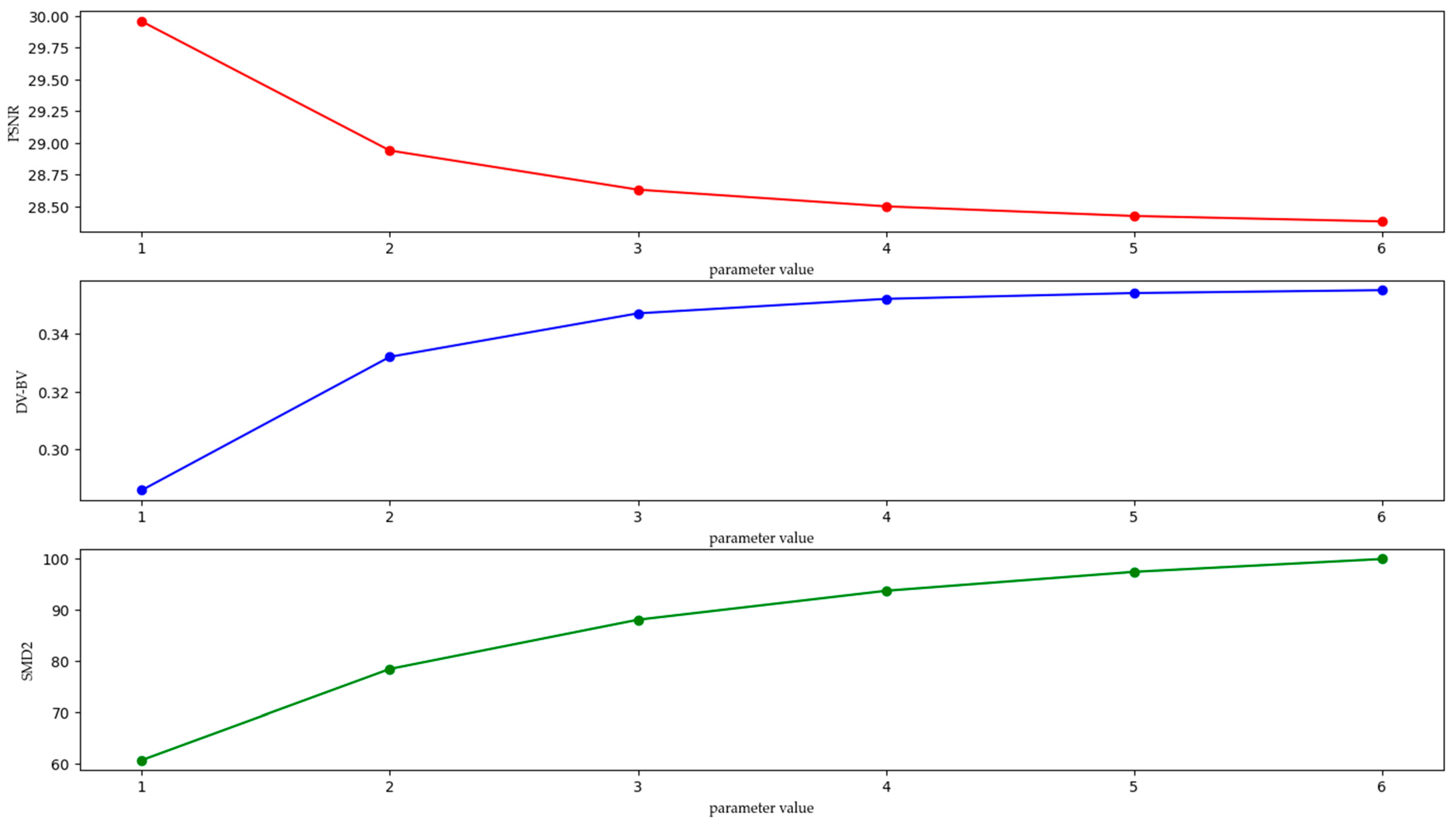
4.2. Selection of Parameters Involved in the Algorithm
4.2.1. Parameter
4.2.2. Parameter
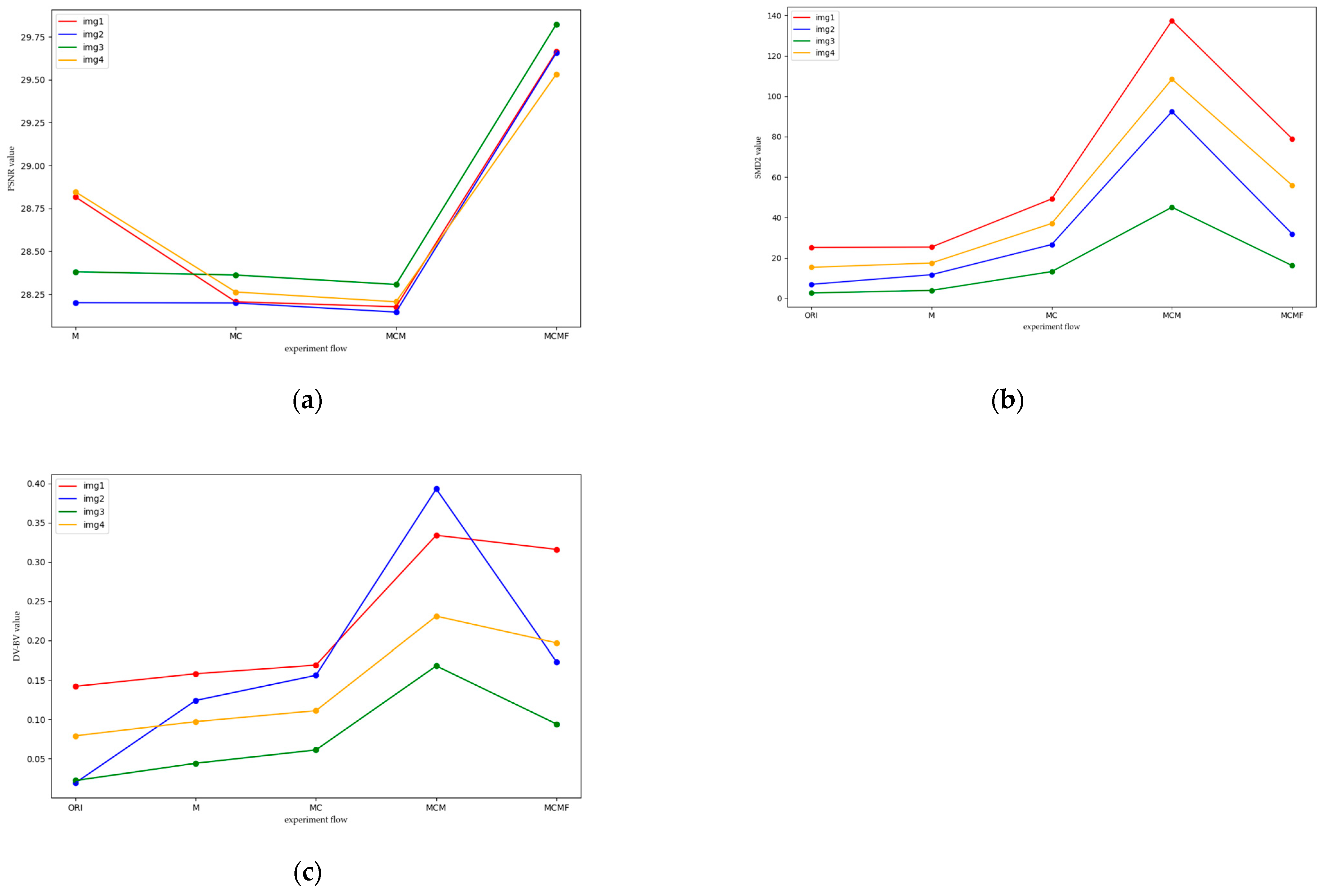
4.3. Subjective and Objective Evaluation
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brisson, M.; Drolet, M. Global elimination of cervical cancer as a public health problem. Lancet Oncol. 2019, 20, 319–321. [Google Scholar] [CrossRef] [PubMed]
- Herfs, M.; Vargas, S.O.; Yamamoto, Y.; Howitt, B.E.; Nucci, M.R.; Hornick, J.L.; McKeon, F.D.; Xian, W.; Crum, C.P. A novel blueprint for ‘top down’ differentiation defines the cervical squamocolumnar junction during development, reproductive life, and neoplasia. J. Pathol. 2013, 229, 460–468. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.J.; Werner, C.L.; Darragh, T.M.; Guido, R.S.; Mathews, C.; Moscicki, A.-B.; Mitchell, M.M.; Schiffman, M.; Wentzensen, N.; Massad, L.S.; et al. ASCCP Colposcopy Standards: Role of Colposcopy, Benefits, Potential Harms, and Terminology for Colposcopic Practice. J. Low. Genit. Tract Dis. 2017, 21, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Singh, K.; Kapoor, R. Image enhancement using Exposure based Sub Image Histogram Equalization. Pattern Recognit. Lett. 2014, 36, 10–14. [Google Scholar] [CrossRef]
- Al-Ameen, Z.; Sulong, G.; Rehman, A.; Al-Dhelaan, A.; Saba, T.; Al-Rodhaan, M. An innovative technique for contrast enhancement of computed tomography images using normalized gamma-corrected contrast-limited adaptive histogram equalization. Eurasip J. Adv. Signal Process. 2015, 2015, 32. [Google Scholar] [CrossRef]
- Chang, Y.-T.; Wang, J.-T.; Yang, W.-H.; Chen, X.-W. Contrast enhancement in palm bone image using quad-histogram equalization. In Proceedings of the 2014 International Symposium on Computer, Consumer and Control (IS3C), Taichung, Taiwan, 10–12 June 2014; pp. 1091–1094. [Google Scholar] [CrossRef]
- Joseph, J.; Periyasamy, R. A fully customized enhancement scheme for controlling brightness error and contrast in magnetic resonance images. Biomed. Signal Process. Control 2018, 39, 271–283. [Google Scholar] [CrossRef]
- Palanisamy, G.; Ponnusamy, P.; Gopi, V.P. An improved luminosity and contrast enhancement framework for feature preservation in color fundus images. Signal Image Video Process. 2019, 13, 719–726. [Google Scholar] [CrossRef]
- Pizer, S.M.; Johnston, R.E.; Ericksen, J.P.; Yankaskas, B.C.; Muller, K.E. Contrast-limited adaptive histogram equalization: Speed and effectiveness. In Proceedings of the First Conference on Visualization in Biomedical Computing, Atlanta, GA, USA, 22–25 May 1990; pp. 337–345. [Google Scholar]
- Thirumala, K.; Pal, S.; Jain, T.; Umarikar, A.C. A classification method for multiple power quality disturbances using EWT based adaptive filtering and multiclass SVM. Neurocomputing 2019, 334, 265–274. [Google Scholar] [CrossRef]
- Oh, J.; Hwang, H. Feature Enhancement of Medical Images using Morphology-Based Homomorphic Filter and Differential Evolution Algorithm. Int. J. Control Autom. Syst. 2010, 8, 857–861. [Google Scholar] [CrossRef]
- Ajam, A.; Abd Aziz, A.; Asirvadam, V.S.; Izhar, L.I.; Muda, S. Cerebral Vessel Enhancement Using Bilateral and Hessian-Based Filter. In Proceedings of the 6th International Conference on Intelligent and Advanced Systems (ICIAS), Kuala Lumpur, Malaysia, 15–17 August 2016. [Google Scholar]
- Bhonsle, D.; Bagga, J.; Mishra, S.; Sahu, C.; Sahu, V.; Mishra, A. Reduction of Gaussian noise from Computed Tomography Images using Optimized Bilateral Filter by Enhanced Grasshopper Algorithm. In Proceedings of the 2nd IEEE International Conference on Advances in Electrical, Computing, Communication and Sustainable Technologies (IEEE ICAECT), Bhilai, India, 21–22 April 2022. [Google Scholar]
- Dhivyaprabha, T.T.; Jayashree, G.; Subashini, P. Medical Image Denoising Using Synergistic Fibroblast Optimization Based Weighted Median Filter. In Proceedings of the 2nd International Conference on Advances in Electronics, Computers and Communications (ICAECC), Bengaluru, India, 9–10 February 2018. [Google Scholar]
- Chen, C.; Zhang, J. Improved multi-scale Retinex enhancement algorithm of medical X ray images. Comput. Eng. Appl. 2015, 51, 191–195, 226. [Google Scholar] [CrossRef]
- Daway, E.G.; Abdulameer, F.S.; Daway, H.G. X-ray image enhancement using retinex algorithm based on color restoration. J. Eng. Sci. Technol. 2022, 17, 1276–1286. [Google Scholar]
- Huang, Y.; Liu, Z.; Zhao, Z. Enhancement of Ultrasonic Liver Images Based on Multi-Scale Retinex Model. J. Data Acquis. Process. 2013, 28, 597–601. [Google Scholar]
- Qin, Y.; Luo, F.; Li, M. A Medical Image Enhancement Method Based on Improved Multi-Scale Retinex Algorithm. J. Med. Imaging Health Inform. 2020, 10, 152–157. [Google Scholar] [CrossRef]
- Wang, W.B.; Zhou, L.J.; Fei, L. An improved algorithm based on retinex theory for x-ray medical image. Adv. Mater. Res. 2013, 772, 233–238. [Google Scholar] [CrossRef]
- Eilimnur, A.; Abdurusul, O.; Turghunjan; Abdukirim, T. An algorithm of medical image enhancement based on dyadic wavelet transform. Comput. Appl. Chem. 2012, 29, 951–954. [Google Scholar]
- Masud, M.; Sikder, N.; Nahid, A.-A.; Bairagi, A.K.; AlZain, M.A. A Machine Learning Approach to Diagnosing Lung and Colon Cancer Using a Deep Learning-Based Classification Framework. Sensors 2021, 21, 748. [Google Scholar] [CrossRef]
- Gupta, R.; Pachauri, R.; Singh, A. Despeckling of Ultrasound Images Using Modified Local Statistics Mean Variance Filter. CMES-Comput. Model. Eng. Sci. 2018, 114, 19–32. [Google Scholar] [CrossRef]
- Povoroznyuk, A.I.; Filatova, A.E.; Kozak, L.M.; Ignashchuk, O.V.; Kotyra, A.; Orshubekov, N.; Smailova, S.; Karnakova, G. Grayscale morphological filter based on local statistics. In Proceedings of the Conference on Photonics Applications in Astronomy, Communications, Industry, and High Energy Physics Experiments, Wilga, Poland, 28 May–6 June 2017. [Google Scholar]
- Zhao, F.; Zhao, J.; Zhao, W.; Qu, F.; Sui, L. Local region statistics combining multi-parameter intensity fitting module for medical image segmentation with intensity inhomogeneity and complex composition. Opt. Laser Technol. 2016, 82, 17–27. [Google Scholar] [CrossRef]
- Guo, J.; Wang, H.; Xue, X.; Li, M.; Ma, Z. Real-time classification on oral ulcer images with residual network and image enhancement. IET Image Process. 2022, 16, 641–646. [Google Scholar] [CrossRef]
- Ma, Y.; Liu, J.; Liu, Y.; Fu, H.; Hu, Y.; Cheng, J.; Qi, H.; Wu, Y.; Zhang, J.; Zhao, Y. Structure and Illumination Constrained GAN for Medical Image Enhancement. IEEE Trans. Med. Imaging 2021, 40, 3955–3967. [Google Scholar] [CrossRef]
- Xia, K.; Zhou, Q.; Jiang, Y.; Chen, B.; Gu, X. Deep residual neural network based image enhancement algorithm for low dose CT images. Multimed. Tools Appl. 2022, 81, 36007–36030. [Google Scholar] [CrossRef]
- Kaur, M.; Kaur, J.; Kaur, J. Survey of Contrast Enhancement Techniques based on Histogram Equalization. Int. J. Adv. Comput. Sci. Appl. 2011, 2, 137–141. [Google Scholar] [CrossRef]
- Chang, Y.; Jung, C.; Ke, P.; Song, H.; Hwang, J. Automatic Contrast-Limited Adaptive Histogram Equalization With Dual Gamma Correction. IEEE Access 2018, 6, 11782–11792. [Google Scholar] [CrossRef]
- Subramani, B.; Veluchamy, M. Fuzzy Gray Level Difference Histogram Equalization for Medical Image Enhancement. J. Med. Syst. 2020, 44, 103. [Google Scholar] [CrossRef] [PubMed]
- Land, E.H.; McCann, J.J. Lightness and retinex theory. J. Opt. Soc. Am. 1971, 61, 1–11. [Google Scholar] [CrossRef]
- Land, E.H. An alternative technique for the computation of the designator in the retinex theory of color-vision. Proc. Natl. Acad. Sci. USA 1986, 83, 3078–3080. [Google Scholar] [CrossRef]
- Rahman, Z.U.; Jobson, D.J.; Woodell, G.A. A multiscale retinex for color rendition and dynamic range compression. In Proceedings of the Conference on Applications of Digital Image Processing XIX, Denver, CO, USA, 7–9 August 1996; pp. 183–191. [Google Scholar]
- Rahman, Z.U.; Jobson, D.J.; Woodell, G.A. Retinex processing for automatic image enhancement. In Proceedings of the Conference on Human Vision and Electronic Imaging VII, San Jose, CA, USA, 21–24 January 2002; pp. 390–401. [Google Scholar]
- Fu, X.; Zeng, D.; Huang, Y.; Zhang, X.-P.; Ding, X. A weighted variational model for simultaneous reflectance and illumination estimation. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Seattle, WA, USA, 27–30 June 2016; pp. 2782–2790. [Google Scholar]
- Wang, D.; Yan, W.; Zhu, T.; Xie, Y.; Song, H.; Hu, X. An Adaptive Correction Algorithm for Non-Uniform Illumination Panoramic Images Based on the Improved Bilateral Gamma Function. In Proceedings of the International Conference on Digital Image Computing—Techniques and Applications (DICTA), Sydney, Australia, 29 November–1 December 2017; pp. 878–883. [Google Scholar]
- Wang, L.; Wu, B.; Wang, X.; Zhu, Q.; Xu, K. Endoscopic image luminance enhancement based on the inverse square law for illuminance and retinex. Int. J. Med. Robot. Comput. Assist. Surg. 2022, 18, e2396. [Google Scholar] [CrossRef]
- Yang, Y.; Su, Z.; Sun, L. Medical image enhancement algorithm based on wavelet transform. Electron. Lett. 2010, 46, 120–121. [Google Scholar] [CrossRef]
- Xia, K.-j.; Wang, J.-q.; Cai, J. A novel medical image enhancement algorithm based on improvement correction strategy in wavelet transform domain. Clust. Comput.-J. Netw. Softw. Tools Appl. 2019, 22, 10969–10977. [Google Scholar] [CrossRef]
- Li, Q.; Yang, X.; Wu, W.; Liu, K.; Jeon, G. Multi-Focus Image Fusion Method for Vision Sensor Systems via Dictionary Learning with Guided Filter. Sensors 2018, 18, 2143. [Google Scholar] [CrossRef]
- Chen, J.; Zhang, L.; Lu, L.; Li, Q.; Hu, M.; Yang, X. A novel medical image fusion method based on Rolling Guidance Filtering. Internet Things 2021, 14, 100172. [Google Scholar] [CrossRef]
- Daniel, E.; Anitha, J. Optimum wavelet based masking for the contrast enhancement of medical images using enhanced cuckoo search algorithm. Comput. Biol. Med. 2016, 71, 149–155. [Google Scholar] [CrossRef]
- Zhou, Y.; Ye, J.; Du, Y.; Sheykhahmad, F.R. New Improved Optimized Method for Medical Image Enhancement Based on Modified Shark Smell Optimization Algorithm. Sens. Imaging 2020, 21, 20. [Google Scholar] [CrossRef]
- An, Z.; Xu, C.; Qian, K.; Han, J.; Tan, W.; Wang, D.; Fang, Q. EIEN: Endoscopic Image Enhancement Network Based on Retinex Theory. Sensors 2022, 22, 5464. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Gong, X.; Liu, D.; Cheng, Y.; Fang, C.; Shen, X.; Yang, J.; Zhou, P.; Wang, Z. EnlightenGAN: Deep Light Enhancement without Paired Supervision arXiv. IEEE Trans. Image Process. 2021, 30, 2340–2349. [Google Scholar]
- Fan, J.; Liu, J.; Xie, S.; Zhou, C.; Wu, Y. Cervical lesion image enhancement based on conditional entropy generative adversarial network framework. Methods 2022, 203, 523–532. [Google Scholar] [CrossRef]
- Jiang, H.; Zhang, K.; Yuan, B.; Wang, L. A vascular enhancement algorithm for endoscope image. Opto-Electron. Eng. 2019, 46, 180167-1. [Google Scholar]
- Kim, Y.; Koh, Y.J.; Lee, C.; Kim, S.; Kim, C.-S. Dark image enhancement based on pairwise target contrast and multi-scale detail boosting. In Proceedings of the IEEE International Conference on Image Processing (ICIP), Quebec City, QC, Canada, 27–30 September 2015; pp. 1404–1408. [Google Scholar]
- Li, K.; Xu, C.; Feng, B.; Liu, H.R. Brightness and Contrast Adjustment-Based Endoscopic Image Enhancement Technique. J. Small Microcomput. Syst. 2022, 43, 2375–2380. [Google Scholar] [CrossRef]
- An, Z.; Xu, C.; Feng, B.; Han, J. Endoscopic Image Enhancement Algorithm Based on Luminance Correction and Fusion Channel Prior. Comput. Sci. 2023, 50 (Suppl. S1), 298–304. [Google Scholar]
- Zhu, Y.; Xu, C.; Feng, B.; Fang, S. Research on Endoscopic Image Enhancement Algorithm Based on Contrast Fusion. In Proceedings of the 2021 IEEE 6th International Conference on Signal and Image Processing (ICSIP), Nanjing, China, 22–24 October 2021; pp. 210–215. [Google Scholar]



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Source Images | MSR | MSRCR | IESVE | LCLCP | IECF | CLAHE | Proposed |
|---|---|---|---|---|---|---|---|
| Img1 | 28.824 | 28.595 | 29.658 | 28.059 | 27.328 | 29.299 | 29.664 |
| Img2 | 28.070 | 28.122 | 29.656 | 28.627 | 27.344 | 29.621 | 29.657 |
| Img3 | 28.529 | 28.504 | 30.546 | 27.695 | 27.445 | 29.699 | 29.824 |
| Img4 | 28.807 | 28.147 | 29.240 | 28.280 | 27.343 | 28.865 | 29.532 |
| Source Images | MSR | MSRCR | IESVE | LCLCP | IECF | CLAHE | Proposed |
|---|---|---|---|---|---|---|---|
| Img1 | 0.174 | 0.131 | 0.181 | 0.105 | 0.233 | 0.180 | 0.316 |
| Img2 | 0.130 | 0.120 | 0.043 | 0.035 | 0.059 | 0.046 | 0.323 |
| Img3 | 0.049 | 0.041 | 0.033 | 0.023 | 0.048 | 0.031 | 0.094 |
| Img4 | 0.108 | 0.070 | 0.108 | 0.058 | 0.138 | 0.106 | 0.197 |
| Source Images | MSR | MSRCR | IESVE | LCLCP | IECF | CLAHE | Proposed |
|---|---|---|---|---|---|---|---|
| Img1 | 25.738 | 61.539 | 41.769 | 50.971 | 62.629 | 46.705 | 78.928 |
| Img2 | 10.175 | 30.501 | 18.665 | 24.588 | 31.315 | 22.238 | 31.880 |
| Img3 | 3.949 | 14.920 | 6.343 | 10.843 | 9.660 | 7.119 | 16.197 |
| Img4 | 17.970 | 44.097 | 26.738 | 34.052 | 43.119 | 30.112 | 55.879 |
| Source Images | MSR | MSRCR | IESVE | LCLCP | IECF | CLAHE | Proposed |
|---|---|---|---|---|---|---|---|
| Img1 | 0.062 | 0.367 | 0.042 | 0.223 | 0.108 | 0.006 | 0.255 |
| Img2 | 0.174 | 0.306 | 0.147 | 0.306 | 0.121 | 0.210 | 0.310 |
| Img3 | 0.018 | 0.858 | 0.234 | 1.031 | 0.152 | 0.359 | 1.092 |
| Img4 | 0.049 | 0.299 | 0.009 | 0.262 | 0.163 | 0.050 | 0.301 |
| Source Images | MSR | MSRCR | IESVE | LCLCP | IECF | CLAHE | Proposed |
|---|---|---|---|---|---|---|---|
| Img1 | 0.068 | 0.091 | 0.745 | 0.671 | 1.101 | 0.575 | 0.748 |
| Img2 | 0.009 | 0.036 | 1.211 | 0.960 | 1.051 | 0.856 | 1.22 |
| Img3 | 0.003 | 0.013 | 1.103 | 0.829 | 1.046 | 0.913 | 1.115 |
| Img4 | 0.068 | 0.153 | 0.975 | 0.982 | 1.076 | 0.550 | 1.080 |
| Source Images | MSR | MSRCR | IESVE | LCLCP | IECF | CLAHE | Proposed |
|---|---|---|---|---|---|---|---|
| Img1 | 1.49 | 2.117 | 38.352 | 10.451 | 7.729 | 1.03 | 3.72 |
| Img2 | 6.319 | 8.749 | 367.187 | 86.09 | 38.179 | 1.12 | 15.68 |
| Img3 | 3.726 | 5.157 | 158.426 | 38.176 | 21.502 | 1.16 | 8.85 |
| Img4 | 1.474 | 1.967 | 40.525 | 10.386 | 7.75 | 1.09 | 3.68 |
| Source Images | MSR | MSRCR | IESVE | LCLCP | IECF | CLAHE | Proposed |
|---|---|---|---|---|---|---|---|
| PSNR | 28.916 | 28.071 | 29.689 | 28.253 | 27.215 | 28.815 | 29.914 |
| DV–BV | 0.080 | 0.061 | 0.063 | 0.079 | 0.066 | 0.086 | 0.193 |
| SMD2 | 18.806 | 35.019 | 21.644 | 28.790 | 40.384 | 30.384 | 45.384 |
| CII | 0.056 | 0.374 | 0.091 | 0.606 | 0.167 | 0.406 | 0.628 |
| EQI | 0.027 | 0.076 | 0.862 | 0.813 | 0.929 | 0.797 | 0.988 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ren, Y.; Li, Z.; Xu, C. Cervical Precancerous Lesion Image Enhancement Based on Retinex and Histogram Equalization. Mathematics 2023, 11, 3689. https://doi.org/10.3390/math11173689
Ren Y, Li Z, Xu C. Cervical Precancerous Lesion Image Enhancement Based on Retinex and Histogram Equalization. Mathematics. 2023; 11(17):3689. https://doi.org/10.3390/math11173689
Chicago/Turabian StyleRen, Yuan, Zhengping Li, and Chao Xu. 2023. "Cervical Precancerous Lesion Image Enhancement Based on Retinex and Histogram Equalization" Mathematics 11, no. 17: 3689. https://doi.org/10.3390/math11173689
APA StyleRen, Y., Li, Z., & Xu, C. (2023). Cervical Precancerous Lesion Image Enhancement Based on Retinex and Histogram Equalization. Mathematics, 11(17), 3689. https://doi.org/10.3390/math11173689