
Social and Individual Factors Predicting Students’ Resilience: A Multigroup Structural Equation Model

 ,
,  ,
,  , and
, and
Abstract
:1. Introduction
1.1. Resilience Outcomes at School
1.2. Impact of the COVID-19 Pandemic on Resilience Outcomes
1.3. Social Support as Key Factor for Mental Health
1.4. Current Study
Hypotheses
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures
2.2.1. Symptoms of Anxiety and Depression
2.2.2. The Four Social Indicators
Two Teacher Indicators
Two Family Support Indicators
2.2.3. Two Individual Indicators
2.2.4. The Dependent Variable
2.2.5. Sociodemographic Indicators
2.3. Analytic Strategy
3. Results
3.1. Analytic Step 1: Intercorrelations and Descriptive Statistics of the Applied Measures
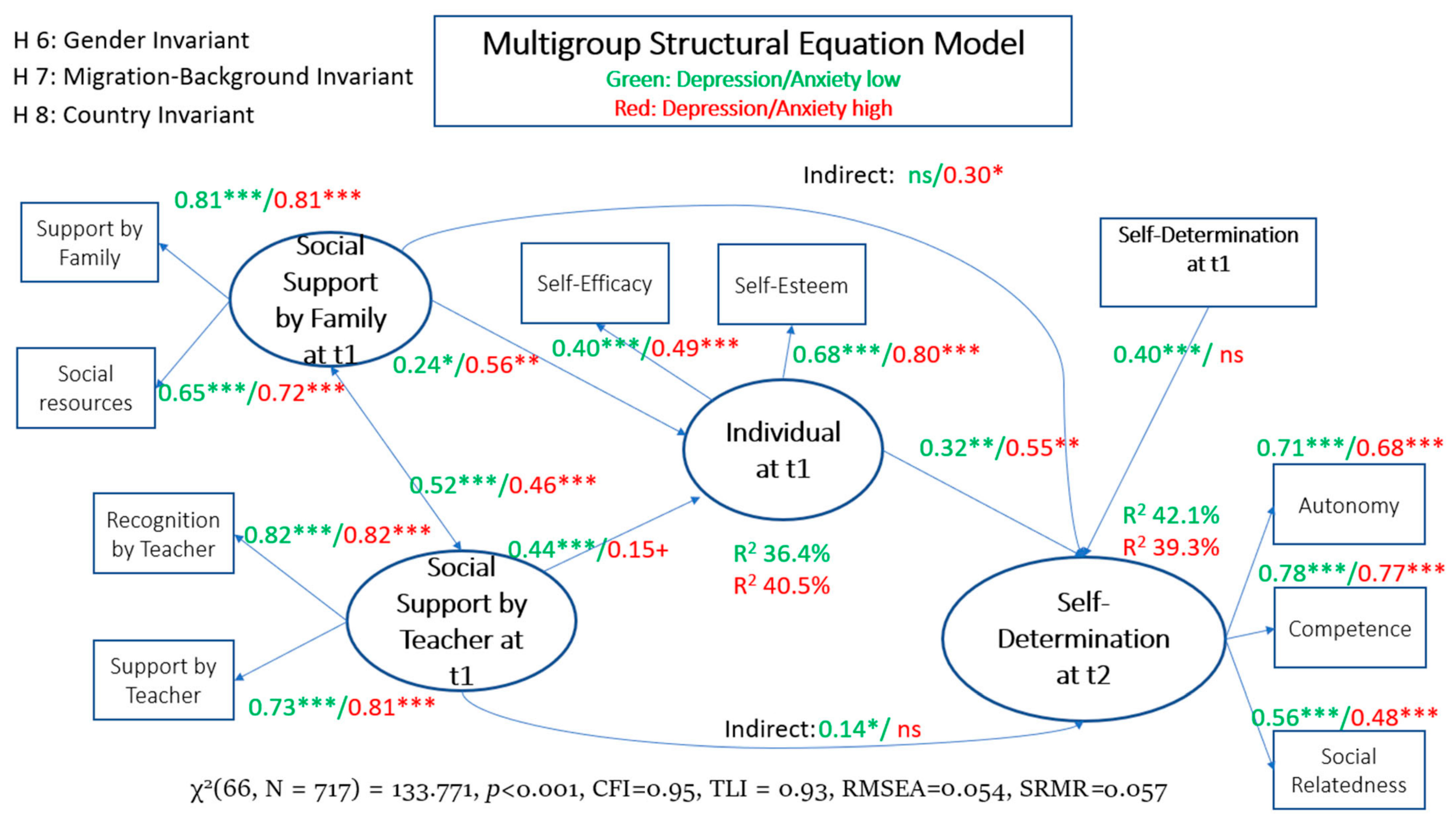
3.2. Analytic Step 3: Testing for Longitudinal Effects Using Structural Equation Modeling
Invariance Testing for Country, Gender, and Migration Background
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Masten, A.S. Global perspectives on resilience in children and youth. Child Dev. 2014, 85, 6–20. [Google Scholar] [CrossRef] [PubMed]
- Rutter, M. Resilience as a dynamic concept. Dev. Psychopathol. 2021, 24, 335–344. [Google Scholar] [CrossRef] [PubMed]
- Masten, A.S. Resilience of children in disasters: A multisystem perspective. Int. J. Psychol. 2021, 56, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, D.; Sarkar, M. Psychological resilience: A review and critique of definitions, concepts, and theory. Eur. Psychol. 2013, 18, 12–23. [Google Scholar] [CrossRef]
- Masten, A.S. Ordinary magic: Resilience processes in development. Am. Psychol. 2001, 56, 227–238. [Google Scholar] [CrossRef] [PubMed]
- Windle, G.; Bennett, K.M.; Noyes, J. A methodological review of resilience measurement scales. Health Qual. Life Outcomes 2011, 9, 8. [Google Scholar] [CrossRef] [PubMed]
- Graber, R.; Turner, R.; Madill, A. Best friends and better coping: Facilitating psychological resilience through boys’ and girls’ closest friendships. Br. J. Psychol. 2016, 107, 338–358. [Google Scholar] [CrossRef] [PubMed]
- Liebenberg, L.; Joubert, N. A comprehensive review of core resilience elements and indicators: Findings of relevance to children and youth. Int. J. Child Adolesc. Resil. 2020, 6, 8–18. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Self-Determination Theory: Basic Psychological Needs in Motivation, Development, and Wellness; Guilford Publications: New York, NY, USA, 2017; ISBN 978-1-4625-2876-9. [Google Scholar]
- Ryan, R.M.; Deci, E.L.; Vansteenkiste, M. Autonomy and autonomy disturbances in self-development and psychopathology: Research on motivation, attachment, and clinical process. Dev. Psychopathol. 2016, 1, 385–438. [Google Scholar]
- Evans, P. Self-determination theory: An approach to motivation in music education. Music. Sci. 2015, 19, 65–83. [Google Scholar] [CrossRef]
- Vansteenkiste, M.; Niemiec, C.P.; Soenens, B. The development of the five mini-theories of self-determination theory: An historical overview, emerging trends, and future direction. In The Decade Ahead: Theoretical Perspectives on Motivation and Achievement; Urdan, T.C., Karabenick, S.A., Eds.; Emerald Group Publishing Limited: Bingley, UK, 2010; pp. 105–165. ISBN 978-0-85724-111-5. [Google Scholar]
- Ryan, R.M.; Deci, E.L. Supporting autonomy, competence, and relatedness: The coaching process from a self-determination theory perspective. In Professional Coaching: Principles and Practice; English, S., Sabatine, J.M., Brownell, P., Eds.; Springer: New York, NY, USA, 2019; pp. 231–245. ISBN 978-0-8261-8008-7. [Google Scholar]
- Vansteenkiste, M.; Ryan, R.M.; Soenens, B. Basic psychological need theory: Advancements, critical themes, and future directions. Motiv. Emot. 2020, 44, 1–31. [Google Scholar] [CrossRef]
- Ungar, M. Pathways to resilience among children in child welfare, corrections, mental health and educational settings: Navigation and negotiation. Child Youth Care Forum 2005, 34, 423–444. [Google Scholar] [CrossRef]
- Niemiec, C.P.; Ryan, R.M. Autonomy, competence, and relatedness in the classroom: Applying self-determination theory to educational practice. Theory Res. Educ. 2009, 7, 133–144. [Google Scholar] [CrossRef]
- Tian, L.; Chen, H.; Huebner, E.S. The longitudinal relationships between basic psychological needs satisfaction at school and school-related subjective well-being in adolescents. Soc. Indic. Res. 2014, 119, 353–372. [Google Scholar] [CrossRef]
- Henning, G.; Bjalkebring, P.; Stenling, A.; Thorvaldsson, V.; Johansson, B.; Lindwall, M. Changes in within and between-person associations between basic psychological need satisfaction and well-being after retirement. J. Res. Pers. 2019, 79, 151–160. [Google Scholar] [CrossRef]
- Mabbe, E.; Soenens, B.; Vansteenkiste, M.; Van Leeuwen, K. Do personality traits moderate relations between psychologically controlling parenting and problem behavior in adolescents? J. Pers. 2016, 84, 381–392. [Google Scholar] [CrossRef] [PubMed]
- Benita, M.; Benis-Weisman, M.; Matos, L.; Torres, C. Integrative and suppressive emotion regulation diferentially predict well-being through basic need satisfaction and frustration: A test of three countries. Motiv. Emot. 2020, 44, 67–81. [Google Scholar] [CrossRef]
- La Guardia, J.G.; Ryan, R.M. What adolescents need: A self-determination theory perspective on development within families, school, and society. In Academic Motivation of Adolescents; Pajares, F., Urdan, T., Eds.; Information Book Publishing: Greenwich, CT, USA, 2002; pp. 193–219. ISBN 1-931576-62-9. [Google Scholar]
- Wehmeyer, M.L.; Shogren, K.A. The development of self-determination during adolescence. In Development of Self-Determination through the Life-Course; Wehmeyer, M.L., Shogren, K.A., Little, T.D., Lopez, S.J., Eds.; Springer: Dordrecht, The Netherlands, 2017; pp. 89–98. ISBN 978-94-024-1040-2. [Google Scholar]
- UNESCO. COVID-19 Impact on Education. Available online: https://en.unesco.org/covid19/educationresponse (accessed on 25 September 2023).
- UNESCO. Nurturing the Social and Emotional Wellbeing of Children and Young People during Crises. UNESCO COVID19 Education Response. Available online: https://unesdoc.unesco.org/ark:/48223/pf0000373271 (accessed on 25 September 2023).
- Magson, N.R.; Freeman, J.Y.; Rapee, R.M.; Richardson, C.E.; Oar, E.L.; Fardouly, J. Risk and protective factors for prospective changes in adolescent mental health during the COVID-19 pandemic. J. Youth Adolesc. 2021, 50, 44–57. [Google Scholar] [CrossRef]
- Nearchou, F.; Flinn, C.; Niland, R.; Subramaniam, S.S.; Hennessy, E. Exploring the impact of COVID-19 on mental health outcomes in children and adolescents: A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 8479. [Google Scholar] [CrossRef]
- Prati, G.; Mancini, A.D. The psychological impact of COVID-19 pandemic lockdowns: A review and meta-analysis of longitudinal studies and natural experiments. Psychol. Med. 2021, 51, 201–211. [Google Scholar] [CrossRef]
- Lampropoulou, A.; Georgakakou-Koutsonikou, N.; Hatzichristou, C.; Roussos, P. Student Adaptation, Loneliness and Mental Health Profiles during the Second Wave of the Pandemic COVID-19. Educ. Sci. 2023, 13, 644. [Google Scholar] [CrossRef]
- Zhou, J.; Jiang, S.; Zhu, X.; Huebner, E.S.; Tian, L. Profiles and transitions of dual-factor mental health among Chinese early adolescents: The predictive roles of perceived psychological need satisfaction and stress in school. J. Youth Adolesc. 2020, 49, 2090–2108. [Google Scholar] [CrossRef] [PubMed]
- Ravens-Sieberer, U.; Kaman, A.; Erhart, M.; Devine, J.; Schlack, R.; Otto, C. Impact of the COVID-19 pandemic on quality of life and mental health in children and adolescents in Germany. Eur. Child Adolesc. Psychiatry 2022, 31, 879–889. [Google Scholar] [CrossRef] [PubMed]
- Pieh, C.; Dale, R.; Jesser, A.; Probst, T.; Plener, P.L.; Humer, E. The impact of migration status on adolescents’ mental health during COVID-19. Healthcare 2022, 10, 176. [Google Scholar] [CrossRef] [PubMed]
- Ertanir, B.; Kassis, W.; Garrote, A. Longitudinal changes in Swiss adolescent’s mental health outcomes from before and during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2021, 18, 12734. [Google Scholar] [CrossRef]
- Ravens-Sieberer, U.; Kaman, A.; Erhart, M.; Otto, C.; Devine, J.; Löffler, C.; Hurrelmann, K.; Bullinger, M.; Barkmann, C.; Siegel, N.A.; et al. Quality of life and mental health in children and adolescents during the first year of the COVID-19 pandemic: Results of a two-wave nationwide population-based study. Eur. Child Adolesc. Psychiatry 2021, 32, 575–588. [Google Scholar] [CrossRef]
- Mohler-Kuo, M.; Dzemaili, S.; Foster, S.; Werlen, L.; Walitza, S. Stress and mental health among children/adolescents, their parents, and young adults during the first COVID-19 lockdown in Switzerland. Int. J. Environ. Res. Public Health 2021, 18, 4668. [Google Scholar] [CrossRef]
- Theuring, S.; Kern, M.; Hommes, F.; Mall, M.A.; Seybold, J.; Mockenhaupt, F.P.; Glatz, T.; Kurth, T. Generalized anxiety disorder in Berlin school children after the third COVID-19 wave in Germany: A cohort study between June and September 2021. Child Adolesc. Psychiatry Ment. Health 2023, 17, 1. [Google Scholar] [CrossRef]
- Raccanello, D.; Rocca, E.; Vicentini, G.; Brondino, M. Eighteen Months of COVID-19 Pandemic Through the Lenses of Self or Others: A Meta-Analysis on Children and Adolescents’ Mental Health. Child Youth Care Forum 2022, 52, 737–760. [Google Scholar] [CrossRef]
- Elgersma, I.H.; Hart, R.K.; Straiton, M.L.; Hauge, L.J.; Reneflot, A. Migrant background and the impact of the COVID-19 pandemic on mental healthcare consultations among children and adolescents in Norway: A nationwide registry study. BMC Health Serv. Res. 2023, 23, 718. [Google Scholar] [CrossRef]
- Cameranesi, M.; Adisaputri, G.; Jefferies, P.; Ungar, M. Resilience-promoting interventions for children and youth experiencing chronic stress in rural contexts: A convergent segregated mixed methods systematic review. Health Sci. Rev. 2023, 7, 100090. [Google Scholar] [CrossRef]
- Racine, N.; McArthur, B.A.; Cooke, J.E.; Eirich, R.; Zhu, J.; Madigan, S. Global prevalence of depressive and anxiety symptoms in children and adolescents during COVID-19: A meta-analysis. JAMA Pediatr. 2021, 175, 1142–1150. [Google Scholar] [CrossRef] [PubMed]
- Masten, A.S.; Motti-Stefanidi, F. Multisystem resilience for children and youth in disaster: Reflections in the context of COVID-19. Advers. Resil. Sci. 2020, 1, 95–106. [Google Scholar] [CrossRef] [PubMed]
- Bronfenbrenner, U. Ecology of the family as a context for human development: Research perspectives. Dev. Psychol. 1986, 22, 723. [Google Scholar] [CrossRef]
- Ungar, M. The social ecology of resilience: Addressing contextual and cultural ambiguity of a nascent construct. Am. J. Orthopsychiatry 2011, 81, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Dollete, S.; Phillips, M. Understanding girls’ circle as an intervention on perceived social support, body image, self-efficacy, locus of control and self-esteem. J. Psychol. 2004, 90, 204–215. [Google Scholar]
- Bronfenbrenner, U.; Morris, P.A. The bio-ecological model of human development. In Handbook of Child Psychology: Theoretical Models of Human Development, 6th ed.; Damon, W., Lerne, R.M., Eds.; Wiley: Hoboken, NJ, USA, 2006; Volume 1, pp. 793–828. ISBN 978-047-014-765-8. [Google Scholar]
- Ioannou, M.; Kassianos, A.P.; Symeou, M. Coping with depressive symptoms in young adults: Perceived social support protects against depressive symptoms only under moderate levels of stress. Front. Psychol. 2019, 9, 2780. [Google Scholar] [CrossRef]
- Stice, E.; Ragan, J.; Randall, P. Prospective relations between social support and depression: Differential direction of effects for parent and peer support? J. Abnorm. Psychol. 2004, 113, 155–159. [Google Scholar] [CrossRef]
- Gariepy, G.; Honkaniemi, H.; Quesnel-Vallee, A. Social support and protection from depression: Systematic review of current findings in Western countries. Br. J. Psychiatry 2016, 209, 284–293. [Google Scholar] [CrossRef]
- Fox, J.K.; Sital, M.; Halpern, L.F.; Ryan, J.L. Elucidating the Roles of Maternal Overcontrol and Warmth in the Development of Childhood Anxiety and Depression: A Moderated Mediation Framework. Child Psychiatry Hum. Dev. 2023, 54, 609–622. [Google Scholar] [CrossRef]
- Yap, M.B.H.; Pilkington, P.D.; Ryan, S.M.; Jorm, A.F. Parental factors associated with depression and anxiety in young people: A systematic review and meta-analysis. J. Affect. Disord. 2014, 156, 8–23. [Google Scholar] [CrossRef] [PubMed]
- Rueger, S.Y.; Malecki, C.K.; Pyun, Y.; Aycock, C.; Coyle, S. A meta-analytic review of the association between perceived social support and depression in childhood and adolescence. Psychol. Bull. 2016, 142, 1017. [Google Scholar] [CrossRef] [PubMed]
- Honneth, A. The Struggle for Recognition: The Moral Grammar of Social Conflicts; The MIT Press: Cambridge, MA, USA, 1996; ISBN 0-262-58147-7. [Google Scholar]
- Graham, A.; Powell, M.A.; Truscott, J. Facilitating student well-being: Relationships do matter. Educ. Res. 2016, 58, 366–383. [Google Scholar] [CrossRef]
- Graham, A.; Powell, M.A.; Thomas, N.; Anderson, D. Reframing ‘well-being’ in schools: The potential of recognition. Camb. J. Educ. 2017, 47, 439–455. [Google Scholar] [CrossRef]
- Graham, A.; Anderson, D.; Truscott, J.; Simmons, C.; Thomas, N.P.; Cashmore, J.; Bessell, S. Exploring the associations between student participation, wellbeing and recognition at school. Camb. J. Educ. 2022, 52, 453–472. [Google Scholar] [CrossRef]
- Colarossi, L.G.; Eccles, J.S. Differential effects of support providers on adolescents’ mental health. Soc. Work Res. 2003, 27, 19–30. [Google Scholar] [CrossRef]
- Reddy, R.; Rhodes, J.E.; Mulhall, P. The influence of teacher support on student adjustment in the middle school years: A latent growth curve study. Dev. Psychopathol. 2003, 15, 119–138. [Google Scholar] [CrossRef] [PubMed]
- Pössel, P.; Burton, S.M.; Cauley, B.; Sawyer, M.G.; Spence, S.H.; Sheffield, J. Associations between social support from family, friends, and teachers and depressive symptoms in adolescents. J. Youth Adolesc. 2018, 47, 398–412. [Google Scholar] [CrossRef]
- Kelly, K.M.; Malecki, C.K. Social support, depression, and anxiety in female adolescents: Associations and profiles. Child Youth Care Forum 2022, 51, 85–109. [Google Scholar] [CrossRef]
- Auerbach, R.P.; Bigda-Peyton, J.S.; Eberhart, N.K.; Webb, C.A.; Ho, M.-H.R. Conceptualizing the prospective relationship between social support, stress, and depressive symptoms among adolescents. Res. Child Adolesc. Psychopathol. 2011, 39, 475–487. [Google Scholar] [CrossRef]
- Hoferichter, F.; Kulakow, S.; Raufelder, D. How teacher and classmate support relate to students’ stress and academic achievement. Front. Psychol. 2022, 13, 992497. [Google Scholar] [CrossRef] [PubMed]
- Dueggeli, A.; Kassis, M.; Kassis, W. Navigation and negotiation towards school success at upper secondary school: The interplay of structural and procedural risk and protective factors for resilience pathways. Educ. Sci. 2021, 11, 395. [Google Scholar] [CrossRef]
- Theron, L.; van Rensburg, A. Resilience over time: Learning from school-attending adolescents living in conditions of structural inequality. J. Adolesc. 2018, 67, 167–178. [Google Scholar] [CrossRef] [PubMed]
- Pyszczynski, T.; Greenberg, J.; Solomon, S.; Arndt, J.; Schimel, J. Why do people need? A theoretical and empirical review. Psychol. Bull. 2004, 130, 435–468. [Google Scholar] [CrossRef] [PubMed]
- Çelik, E.; Süler, M.; Söylemez, A.; Koçak, L. The Mediating Role of Time Attitude in the Relationship between Self-Esteem and Resilience in High School Students. J. Pedagog. Res. 2023, 7, 82–102. [Google Scholar] [CrossRef]
- Kong, F.; Zhao, J.; You, X. Self-esteem as mediator and moderator of the relationship between social support and subjective well-being among Chinese university students. Soc. Indic. Res. 2013, 112, 151–161. [Google Scholar] [CrossRef]
- Poudel, A.; Gurung, B.; Khanal, G.P. Perceived social support and psychological wellbeing among Nepalese adolescents: The mediating role of self-esteem. BMC Psychol. 2020, 8, 43. [Google Scholar] [CrossRef]
- Tian, L.; Liu, B.; Huang, S.; Huebner, E.S. Perceived social support and school well-being among Chinese early and middle adolescents: The mediational role of self-esteem. Soc. Indic. Res. 2013, 113, 991–1008. [Google Scholar] [CrossRef]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef]
- Kassis, W.; Govaris, C.; Chouvati, R.; Sidler, P.; Janousch, C.; Ertanir, B. Identification and Comparison of School Well-Being Patterns of Migrant and Native Lower Secondary-School Students in Greece and Switzerland: A Multigroup Latent Profile Analysis Approach. Int. J. Educ. Res. 2021, 110, 43. [Google Scholar] [CrossRef]
- Schwarzer, R.; Warner, L.M. Perceived self-efficacy and its relationship to resilience. In Resilience in Children, Adolescents, and Adults: Translating Research into Practice; Prince-Embury, S., Saklofske, D.H., Eds.; Springer: New York, NY, USA, 2012; pp. 139–150. ISBN 978-1-4614-4939-3. [Google Scholar]
- Zeng, W.; Wu, X.; Xu, Y.; Wu, J.; Zeng, Y.; Shao, J.; Huang, D.; Zhu, Z. The impact of general self-efficacy on psychological resilience during the COVID-19 pandemic: The mediating role of posttraumatic growth and the moderating role of deliberate rumination. Front. Psychol. 2021, 12, 684354. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Yu, H. Contribution of social support to home-quarantined Chinese college students’ well-being during the COVID-19 pandemic: The mediating role of online learning self-efficacy and moderating role of anxiety. Soc. Psychol. Educ. 2021, 24, 1643–1662. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, N.; Ryan, R.M. A self-determination theory approach to understanding stress incursion and responses. Stress Health 2011, 27, 4–17. [Google Scholar] [CrossRef]
- Kavvadas, D.; Kavvada, A.; Karachrysafi, S.; Papaliagkas, V.; Cheristanidis, S.; Chatzidimitriou, M.; Papamitsou, T. Stress, anxiety and depression prevalence among greek university students during COVID-19 pandemic: A two-year survey. J. Clin. Med. 2022, 11, 4263. [Google Scholar] [CrossRef] [PubMed]
- Voltmer, E.; Köslich-Strumann, S.; Walther, A.; Kasem, M.; Obst, K.; Kötter, T. The impact of the COVID-19 pandemic on stress, mental health and coping behavior in German University students–a longitudinal study before and after the onset of the pandemic. BMC Public Health 2021, 21, 1385. [Google Scholar] [CrossRef] [PubMed]
- Foster, S.; Estévez-Lamorte, N.; Walitza, S.; Dzemaili, S.; Mohler-Kuo, M. Perceived stress, coping strategies, and mental health status among adolescents during the COVID-19 pandemic in Switzerland: A longitudinal study. Eur. Child Adolesc. Psychiatry 2023, 32, 937–949. [Google Scholar] [CrossRef] [PubMed]
- Breaux, R.; Dvorsky, M.R.; Marsh, N.P.; Green, C.D.; Cash, A.R.; Shroff, D.M.; Buchen, N.; Langberg, J.M.; Becker, S.P. Prospective impact of COVID-19 on mental health functioning in adolescents with and without ADHD: Protective role of emotion regulation abilities. J. Child Psychol. Psychiatry 2021, 62, 1132–1139. [Google Scholar] [CrossRef]
- Garagiola, E.R.; Lam, Q.; Wachsmuth, L.S.; Tan, T.Y.; Ghali, S.; Asafo, S.; Swarna, M. Adolescent Resilience during the COVID-19 Pandemic: A Review of the Impact of the Pandemic on Developmental Milestones. Behav. Sci. 2022, 12, 220. [Google Scholar] [CrossRef]
- Zhu, Q.; Cheong, Y.; Wang, C.; Sun, C. The roles of resilience, peer relationship, teacher–student relationship on student mental health difficulties during COVID-19. Sch. Psychol. 2022, 37, 62–74. [Google Scholar] [CrossRef]
- Costa, S.; Canale, N.; Mioni, G.; Cellini, N. Maintaining social support while social distancing: The longitudinal benefit of basic psychological needs for symptoms of anxiety during the COVID-19 outbreak. J. Appl. Soc. Psychol. 2022, 52, 439–448. [Google Scholar] [CrossRef]
- Vermote, B.; Waterschoot, J.; Morbée, S.; der Kaap-Deeder, V.; Schrooyen, C.; Soenens, B.; Ryan, R.; Vansteenkiste, M. Do psychological needs play a role in times of uncertainty? Associations with well-being during the COVID-19 crisis. J. Happiness Stud. 2022, 23, 257–283. [Google Scholar] [CrossRef] [PubMed]
- Derogatis, L.R.; Lipman, R.S.; Rickels, K.; Uhlenhuth, E.H.; Covi, L. The Hopkins Symptom Checklist (HSCL): A self-report symptom inventory. Behav. Sci. 1974, 19, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Veijola, J.; Jokelainen, J.; Läksy, K.; Kantojärvi, L.; Kokkonen, P.; Järvelin, M.R.; Joukamaa, M. The Hopkins Symptom Checklist-25 in screening DSM-III-R axis-I disorders. Nord. J. Psychiatry 2003, 57, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Sandanger, I.; Moum, T.; Ingebrigtsen, G.; Dalgard, O.S.; Sørensen, T.; Bruusgaard, D. Concordance between symptom screening and diagnostic procedure: The Hopkins Symptom Checklist-25 and the Composite International Diagnostic Interview I. Soc. Psychiatry Psychiatr. Epidemiol. 1998, 33, 345–354. [Google Scholar] [CrossRef] [PubMed]
- Böhm-Kasper, O.; Fritzsche, S.; Krappidel, A.; Siebholz, S. Skalenhandbuch zum Schülerfragebogen aus dem Projekt Politische Orientierung bei Schülern im Rahmen schulischer Anerkennungsbeziehungen. Available online: http://wcms.uzi.uni-halle.de/download.php?down=998&elem=1010879 (accessed on 23 September 2022).
- Hertel, S.; Hochweber, J.; Mildner, D.; Steinert, B.; Jude, N. PISA 2009 Skalenhandbuch; Waxmann: New York, NY, USA, 2014; ISBN 978-3-8309-3112-6. [Google Scholar]
- Hjemdal, O.; Friborg, O.; Stiles, T.C.; Martinussen, M.; Rosenvinge, J.H. A new scale for adolescent resilience: Grasping the central protective resources behind healthy development. Meas. Eval. Couns. Dev. 2006, 39, 84–96. [Google Scholar] [CrossRef]
- Rosenberg, M. Society and Adolescent Self-Image; Princeton University Press: Rahway, NJ, USA, 1965. [Google Scholar]
- Schwarzer, R.; Jerusalem, M. Generalized self-efficacy scale. In Measures in Health Psychology: A User’s Portfolio. Causal and Control; Weinman, J., Wright, S., Johnston, M., Eds.; NFER-NELSON: Windsor, UK, 1995; pp. 35–37. [Google Scholar]
- Deci, E.L.; Ryan, R.M. The Theory. Available online: https://selfdeterminationtheory.org/the-theory/ (accessed on 23 September 2022).
- Mollica, R.F.; Wyshak, G.; Lavelle, J. The psychosocial impact of war trauma and torture on Southeast Asian refugees. Am. J. Psychiatry 1987, 144, 1567–1572. [Google Scholar] [CrossRef] [PubMed]
- Winokur, A.; Winokur, D.F.; Rickels, K.; Cox, D.S. Symptoms of Emotional Distress in a Family Planning Service: Stability over a Four-Week Period. Br. J. Psychiatry 1984, 144, 395–399. [Google Scholar] [CrossRef] [PubMed]
- Glaesmer, H.; Braehler, E.; Grande, G.; Hinz, A.; Petermann, F.; Romppel, M. The German Version of the Hopkins Symptoms Checklist-25 (HSCL-25)—Factorial structure, psychometric properties, and population-based norms. Compr. Psychiatry 2014, 55, 396–403. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling; Guilford Publications: New York, NY, USA, 2023; ISBN 978-1-4625-5191-0. [Google Scholar]
- Xia, Y.; Yang, Y. RMSEA, CFI, and TLI in structural equation modeling with ordered categorical data: The story they tell depends on the estimation methods. Behav. Res. Methods 2019, 51, 409–428. [Google Scholar] [CrossRef]
- Chen, F.F. Sensitivity of Goodness of Fit Indexes to Lack of Measurement Invariance. Struct. Equ. Model. 2007, 14, 464–504. [Google Scholar] [CrossRef]
- Hayduk, L.A. Structural Equation Modeling with LISREL: Essentials and Advances; The John Hopkins University Press: Baltimore, MD, USA, 1987; ISBN 0-8018-3478-3. [Google Scholar]
- Cheung, G.W.; Rensvold, R.B. Evaluating goodness-of-fit indexes for testing measurement invariance. Struct. Equ. Model. 2002, 9, 233–255. [Google Scholar] [CrossRef]
- Graupensperger, S.; Calhoun, B.H.; Fleming, C.; Rhew, I.C.; Lee, C.M. Mental Health and Well-Being Trends Through the First Year-and-a-Half of the COVID-19 Pandemic: Results from a Longitudinal Study of Young Adults in the USA. Prev. Sci. 2022, 23, 853–864. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Xu, Q. Family support as a protective factor for attitudes toward social distancing and in preserving positive mental health during the COVID-19 pandemic. J. Health Psychol. 2022, 27, 858–867. [Google Scholar] [CrossRef] [PubMed]
- Mariani, R.; Renzi, A.; Di Trani, M.; Trabucchi, G.; Danskin, K.; Tambelli, R. The impact of coping strategies and perceived family support on depressive and anxious symptomatology during the coronavirus pandemic (COVID-19) lockdown. Front. Psychiatry 2020, 11, 587724. [Google Scholar] [CrossRef] [PubMed]
- Vasiou, A.; Andriopoulou, P. University students’ mental health and affect during COVID-19 lockdown in Greece: The role of social support and inclusion of others in the self. Psychol. J. Hell. Psychol. Soc. 2023, 28, 253–263. [Google Scholar] [CrossRef]
- Hong, J.C.; Lee, Y.F.; Ye, J.H. Procrastination predicts online self-regulated learning and online learning ineffectiveness during the coronavirus lockdown. Pers. Individ. Differ. 2021, 174, 110673. [Google Scholar] [CrossRef] [PubMed]
- Bilz, L. Werden Ängste und depressive Symptome bei Kindern und Jugendlichen in der Schule übersehen? Z. Padagog. Psychol. 2014, 28, 57–62. [Google Scholar] [CrossRef]
- Baker, J.A. Contributions of Teacher–Child Relationships to Positive School Adjustment During Elementary School. J. Sch. Psychol. 2006, 44, 211–229. [Google Scholar] [CrossRef]
- Holzer, J.; Korlat, S.; Haider, C.; Mayerhofer, M.; Pelikan, E.; Schober, B.; Spiel, C.; Toumazi, T.; Salmela-Aro, K.; Käser, U. Adolescent well-being and learning in times of COVID-19—A multi-country study of basic psychological need satisfaction, learning behavior, and the mediating roles of positive emotion and intrinsic motivation. PLoS ONE 2021, 16, e0251352. [Google Scholar] [CrossRef]
- Muca, E.; Molino, M.; Ghislieri, C.; Baratta, M.; Odore, R.; Bergero, D.; Valle, E. Relationships between psychological characteristics, academic fit and engagement with academic performance in veterinary medical students. BMC Vet. Res. 2023, 19, 132. [Google Scholar] [CrossRef]
- Masten, A.S. Ordinary Magic: Resilience in Development; The Guilford Press: New York, NY, USA, 2014; ISBN 978-1-4625-1716-9. [Google Scholar]
- Govaris, C.; Kassis, W.; Sakatzis, D.; Sarafidou, J.O.; Chouvati, R. Recognitive justice and educational inequalities: An intersectional approach involving secondary grade school students in Greece. Educ. Sci. 2021, 11, 461. [Google Scholar] [CrossRef]
- Sauerwein, M. Partizipation in der Ganztagsschule-vertiefende Analysen. Z. Erzieh. 2019, 22, 435–459. [Google Scholar] [CrossRef]
- Krane, V.; Karlsson, B.; Ness, O.; Kim, H.S. Teacher–student relationship, student mental health, and dropout from upper secondary school: A literature review. Scand. Psychol. 2016, 3, e11. [Google Scholar] [CrossRef]
- Liew, J.; Chen, Q.; Hughes, J.N. Child effortful control, teacher–student relationships, and achievement in academically at-risk children: Additive and interactive effects. Early Child. Res. Q. 2010, 25, 51–64. [Google Scholar] [CrossRef]
- Hamre, B.K.; Pianta, R.C. Early teacher–child relationships and the trajectory of children’s school outcomes through eighth grade. Child Dev. 2001, 72, 625–638. [Google Scholar] [CrossRef]
- Matsopoulos, A.; Theron, L. Resilience to COVID-19 challenges: Lessons for school psychologists serving school-attending youth with experiences of marginalization. Sch. Psychol. Int. 2023, 44, 123–134. [Google Scholar] [CrossRef]
- Goodwin, A.K.B.; Roberson, A.J.; Watson, A.; Chen, G.L.; Long, A.C.J. The Impact of COVID-19, Mental Health Distress, and School-Based Sociocultural Protective Factors among Elementary-Aged Children and their Caregivers. Sch. Psychol. Int. 2023, 44, 154–171. [Google Scholar] [CrossRef]
- Schaffer, G.E.; Power, E.M.; Fisk, A.K.; Trolian, T.L. Beyond the four walls: The evolution of school psychological services during the COVID-19 outbreak. Psychol. Sch. 2021, 58, 1246–1265. [Google Scholar] [CrossRef]
- Azevedo, J.P.; Hasan, A.; Goldemberg, D.; Geven, K.; Iqbal, S.A. Simulating the potential impacts of COVID-19 school closures on schooling and learning outcomes: A set of global estimates. World Bank Res. Obs. 2021, 36, 1–40. [Google Scholar]
- Palmer, A.N.; Small, E. COVID-19 and disconnected youth: Lessons and opportunities from OECD countries. Scand. J. Public Health 2021, 49, 779–789. [Google Scholar] [CrossRef]
- Muris, P.; Otgaar, H. Self-Esteem and Self-Compassion: A Narrative Review and Meta-Analysis on Their Links to Psychological Problems and Well-Being. Psychol. Res. Behav. Manag. 2023, 16, 2961–2975. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Wave | Sample | Gender (Female %) | Mean Age (M_age) at the Time of the Respective Wave | Age SD | No Migration Background (%) |
|---|---|---|---|---|---|
| Wave 0 | German | 47.5 | 12.67 | 0.70 | 33.0 |
| Greek | 51.7 | 12.28 | 0.82 | 54.6 | |
| Swiss | 45.9 | 12.65 | 0.68 | 34.8 | |
| Wave 1 | German | 48.5 | 13.47 | 0.66 | 28.7 |
| Greek | 53.1 | 13.12 | 1.00 | 59.2 | |
| Swiss | 46.0 | 13.60 | 0.67 | 32.4 | |
| Wave 2 | German | 47.4 | 14.48 | 0.73 | 30.9 |
| Greek | 51.0 | 14.06 | 0.89 | 57.8 | |
| Swiss | 45.5 | 14.60 | 0.72 | 32.3 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
|---|---|---|---|---|---|---|---|---|---|---|
| Hopkins Symptoms_wave1 | 1 | |||||||||
| Hopkins Symptoms_wave2 | 0.59 *** | 1 | ||||||||
| Teacher Academic Support_wave1 | −0.18 *** | −0.11 ** | 1 | |||||||
| Recognition by teacher_wave1 | −0.24 *** | −0.10 * | 0.65 *** | 1 | ||||||
| Social Resources_wave1 | −0.28 *** | −0.19 *** | 0.29 *** | 0.30 *** | 1 | |||||
| Family Support_wave1 | −0.41 *** | −0.23 *** | 0.36 *** | 0.35 *** | 0.59 *** | 1 | ||||
| Self-Esteem_wave1 | −0.66 *** | −0.42 *** | 0.33 *** | 0.31 *** | 0.38 *** | 0.39 *** | 1 | |||
| Self-Efficacy_wave1 | −0.32 *** | −0.29 *** | 0.29 *** | 0.27 *** | 0.34 *** | 0.36 *** | 0.46 *** | 1 | ||
| SDT_wave1 | −0.55 *** | −0.36 *** | 0.33 *** | 0.38 *** | 0.35 *** | 0.38 *** | 0.60 *** | 0.37 *** | 1 | |
| SDT_wave2 | −0.41 *** | −0.52 *** | 0.24 *** | 0.29 *** | 0.31 *** | 0.34 *** | 0.45 *** | 0.28 *** | 0.55 *** | 1 |
| Variables | Wave 0 | Wave 1 | Wave 1 | Wave 2 | Wave 0 | Wave 2 |
|---|---|---|---|---|---|---|
| M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | |
| Overall Sample | 1.79 (0.58) | 1.87 (0.68) ** | 1.86 (0.69) | 1.92 (0.71) * | 1.78 (0.57) | 1.92 (0.74) *** |
| Switzerland | 1.84 (0.58) | 1.90 (0.67) * | 1.90 (0.67) | 2.00 (0.70) ** | 1.86 (0.59) | 2.01 (0.69) *** |
| Germany | 1.89 (0.60) | 1.87 (0.69) | 1.80 (0.69) | 1.93 (0.73) ** | 1.80 (0.58) | 1.90 (0.72) * |
| Greece | 1.68 (0.55) | 1.83 (0.69) *** | 1.84 (0.71) | 1.84 (0.78) | 1.68 (0.53) | 1.84 (0.78) *** |
| Variables | Range | Low-Level Depression/Anxiety (n = 375) | High-Level Depression/Anxiety (n = 342) | t (df) | p | Cohen’s d |
|---|---|---|---|---|---|---|
| Teacher Academic Support_wave1 | 1–4 | 3.27 (0.59) | 3.00 (0.69) | 5.36 (688) | <0.001 | 0.31 |
| Recognition by teacher _wave1 | 1–4 | 3.31 (0.49) | 3.04 (0.61) | 6.09 (660) | <0.001 | 0.24 |
| Social Resources_wave1 | 1–5 | 4.56 (0.53) | 4.26 (0.82) | 5.76 (700) | <0.001 | 0.21 |
| Family Support_wave1 | 1–5 | 4.43 (0.55) | 3.90 (0.89) | 9.31 (691) | <0.001 | 0.33 |
| Self-Esteem_wave1 | 1–4 | 3.27 (0.45) | 2.62 (0.56) | 16.18 (663) | <0.001 | 0.53 |
| Self-Efficacy_wave1 | 1–4 | 3.08 (0.51) | 2.76 (0.62) | 7.12 (627) | <0.001 | 0.27 |
| SDT_wave1 | 1–4 | 3.00 (0.39) | 2.61 (0.39) | 12.92 (687) | <0.001 | 0.45 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kassis, W.; Vasiou, A.; Govaris, C.; Favre, C.; Aksoy, D.; Graf, U. Social and Individual Factors Predicting Students’ Resilience: A Multigroup Structural Equation Model. Educ. Sci. 2024, 14, 15. https://doi.org/10.3390/educsci14010015
Kassis W, Vasiou A, Govaris C, Favre C, Aksoy D, Graf U. Social and Individual Factors Predicting Students’ Resilience: A Multigroup Structural Equation Model. Education Sciences. 2024; 14(1):15. https://doi.org/10.3390/educsci14010015
Chicago/Turabian StyleKassis, Wassilis, Aikaterini Vasiou, Christos Govaris, Céline Favre, Dilan Aksoy, and Ulrike Graf. 2024. "Social and Individual Factors Predicting Students’ Resilience: A Multigroup Structural Equation Model" Education Sciences 14, no. 1: 15. https://doi.org/10.3390/educsci14010015
APA StyleKassis, W., Vasiou, A., Govaris, C., Favre, C., Aksoy, D., & Graf, U. (2024). Social and Individual Factors Predicting Students’ Resilience: A Multigroup Structural Equation Model. Education Sciences, 14(1), 15. https://doi.org/10.3390/educsci14010015