
Measuring Outcomes for Children with Cerebral Palsy Who Use Gait Trainers


Abstract
:
1. Introduction
2. Materials and Methods
3. Results
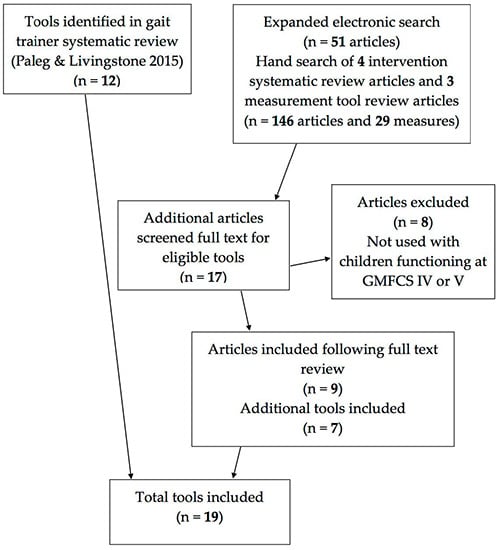
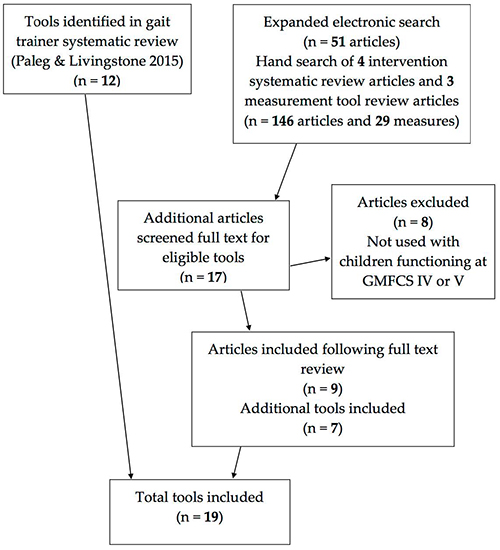
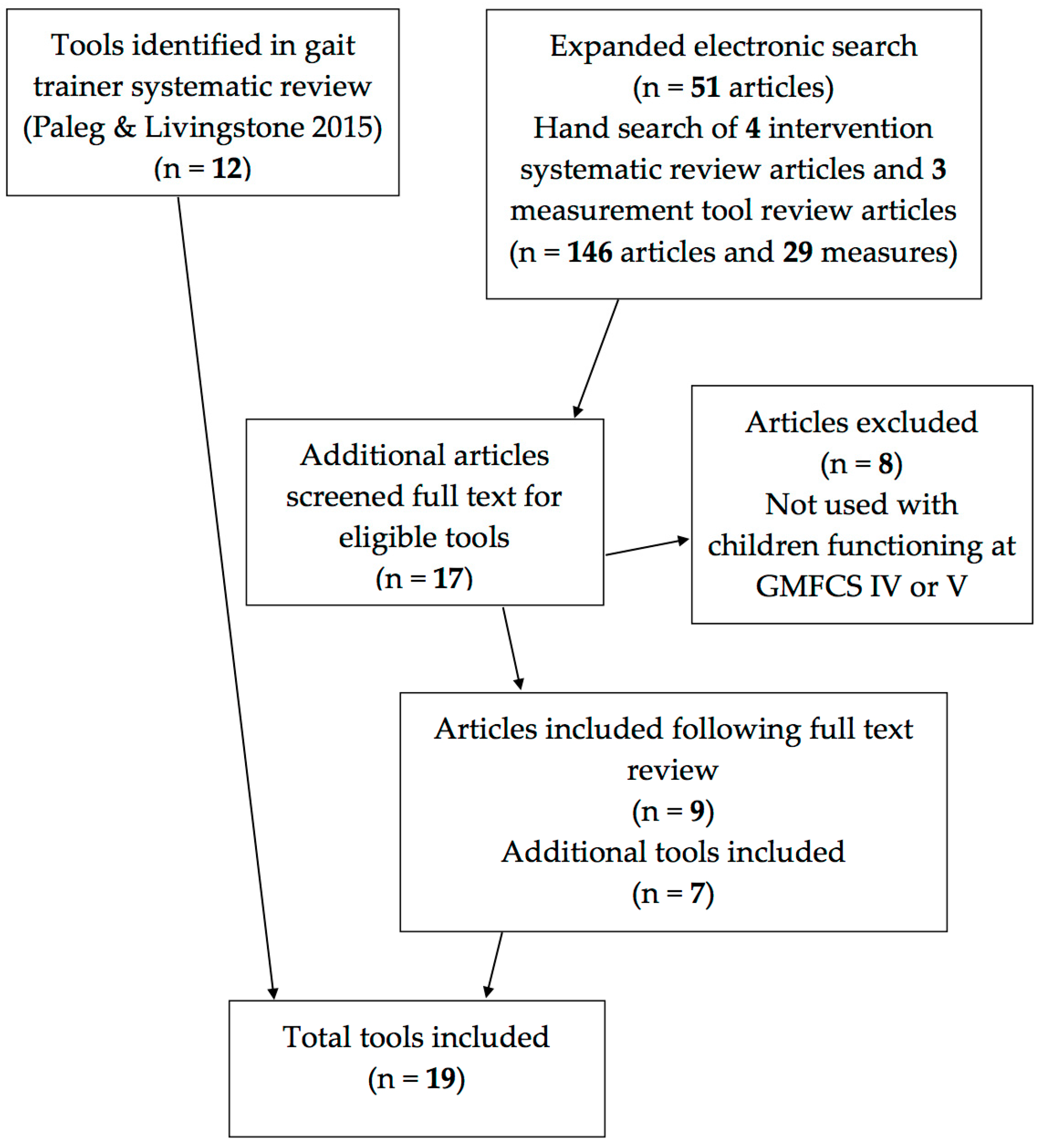
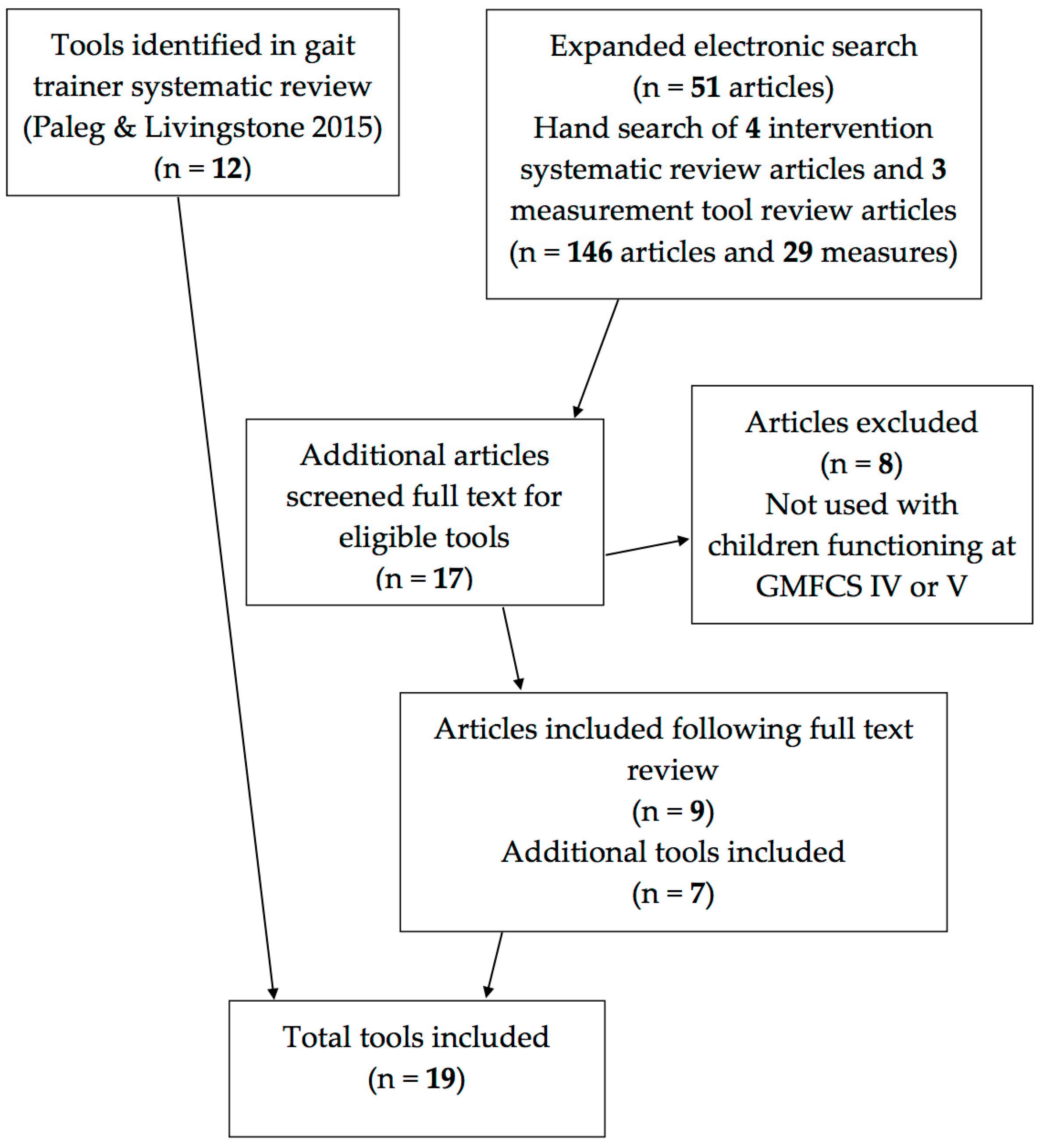
3.1. Tool Identification
3.2. Tool Characteristics
3.3. Reliability
3.4. Validity
3.5. Responsiveness and Sensitivity to Change
3.6. Clinical Utility
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
Abbreviations
| COPM | Canadian Occupational Performance Measure |
| CP | Cerebral Palsy |
| DMA | Directional Mobility Assessment |
| EASE | Early Activity Scale for Endurance |
| GAS | Goal Attainment Scaling |
| GMFCS | Gross Motor Function Classification System |
| GMFM | Gross Motor Function Measure |
| ICF | International Classification of Functioning, Disability and Health |
| MATCH | Matching Assistive Technology and Child |
| PAMS | Physical Abilities Mobility Scale |
| PEDI | Pediatric Evaluation of Disability Inventory |
| QUEST 2.0 | Quebec User Evaluation of Satisfaction with Technology |
| SFA | School Function Assessment |
| SWAPS | Supported Walker Ambulation Scale |
| TDMMT | Top Down Motor Milestone Test |
| Wee FIM | Functional Independence Measure for Children |
Appendix A. Studies Providing Evidence for Use of Additional Tools to Measure Outcomes of Motor Interventions with Children at GMFCS IV and V

{kind=link}
{kind=link}
| Study | Design | Intervention | Participants & Sample | Clinical Tools |
|---|---|---|---|---|
| Benedict et al., 1999 [86] | Cross-sectional | Assistive Technology | 21 families; 19 CP, 2 metabolic; 2–4 years; 1 PWC user (GMFCS IV) | PEDI [29] QUEST 2.0 [46] |
| Bottos et al., 2001 [61] | Case series | Power Mobility | 25 children with CP, (GMFCS IV or V) 3–8 years | COPM [42] |
| Malouin et al., 1997 [47] | Tool development | NA | 3 expert PT’s 9 children with CP 1.3–2.3 years. GMFCS levels unclear—4 quadriplegic | SWAPS [47] |
| Mattern-Baxter et al., 2009 [77] | Cohort without control | Treadmill training | 6 children with CP 2.5–3.9 years Including 2 at GMFCS IV | 6-min walk test [41] 10-m walk test [26,27] PEDI [29] GMFM-66 [73] |
| Meyer-Heim et al., 2009 [80] | Single Subject Research Design | Robot-assisted treadmill training | 22 children with CP mean 8.6 years (4.6–11.7 years). Including 4 at GMFCS IV | 6 min walk test [41] 10 m walk test [26,27] GMFM-66 [73] |
| Reid et al., 1999 [60] | Single Subject Research Design | Rigid pelvic stabilizer | 6 children with CP GMFCS IV; 8–12 years. Rated with caregiver | COPM [42] |
| Steenbeek et al., 2011 [65] | Methodological | Multi-disciplinary rehabilitation | 23 children with CP GMFCS I–V 2–13 years. Included 5 at GMFCS V and 4 at GMFCS IV | GAS [44] PEDI [29] GMFM-66 [73] |
| Tefft et al., 2011 [75] | Cohort without control | Power Mobility | Parents of 23 children; 18–72 mos. 13 CP (GMFCS IV or V), 10 other | MATCH [45] QUEST 2.0 [46] |
| Westcott-McCoy et al., 2012 [43] | Tool development | Not Appropriate | 69 children GMFCS IV and 92 GMFCS V—Construct validity 8 children GMFCS V—Test-retest reliability study 13 children GMFCS I and 1 GMFCS II—convergent reliability with 6 min walk test | EASE [43] 6-min walk test [41] |
References
- Hanna, S.E.; Bartlett, D.J.; Rivard, L.M.; Russell, D.J. Reference curves for the Gross Motor Function Measure: Percentiles for clinical description and tracking over time among children with cerebral palsy. Phys. Ther. 2008, 88, 596–607. [Google Scholar] [CrossRef] [PubMed]
- Dayanidhi, S.; Dykstra, P.B.; Lyubasyuk, V.; McKay, B.R.; Chambers, H.G.; Lieber, R.L. Reduced satellite cell number in situ in muscular contractures from children with cerebral palsy. J. Orthop. Res. 2015, 33, 1039–1045. [Google Scholar] [CrossRef] [PubMed]
- Palisano, R.; Rosenbaum, P.; Walter, S.; Russell, D.; Wood, E.; Galuppi, B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev. Med. Child Neurol. 1997, 39, 214–223. [Google Scholar] [CrossRef] [PubMed]
- Low, S.A.; McCoy, S.W.; Beling, J.; Adams, J. Pediatric physical therapists’ use of support walkers for children with disabilities: A nationwide survey. Pediatr. Phys. Ther. 2011, 23, 381–389. [Google Scholar] [CrossRef] [PubMed]
- Paleg, G.; Livingstone, R. Outcomes of gait trainer use in home and school settings for children with motor impairments: A systematic review. Clin. Rehabil. 2015, 28, 1077–1091. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. International Classification of Functioning, Disability & Health (ICF); World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- World Health Organization. International Classification of Functioning, Disability and Health—Children and Youth; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Chung, J.; Evans, J.; Lee, C.; Rabbani, Y.; Roxborough, L.; Harris, S.R. Effectiveness of adaptive seating on sitting posture and postural control in children with cerebral palsy. Pediatr. Phys. Ther. 2008, 20, 303–317. [Google Scholar] [CrossRef] [PubMed]
- Livingstone, R.; Field, D. Systematic review of power mobility outcomes for infants, children and adolescents with mobility limitations. Clin. Rehabil. 2014, 28, 954–964. [Google Scholar] [CrossRef] [PubMed]
- Houwen, S.; Van der Putten, A.; Vlaskamp, C. A systematic review of the effects of motor interventions to improve motor, cognitive, and/or social functioning in people with severe or profound intellectual disabilities. Res. Dev. Disabil. 2014, 35, 2093–2116. [Google Scholar] [CrossRef] [PubMed]
- Zwicker, J.G.; Mayson, T.A. Effectiveness of treadmill training in children with motor impairments: An overview of systematic reviews. Pediatr. Phys. Ther. 2010, 22, 361–377. [Google Scholar] [CrossRef] [PubMed]
- Sakzewski, L.; Boyd, R.; Ziviani, J. Clinimetric properties of participation measures for 5 to 13 year old children with cerebral palsy: A systematic review. Dev. Med. Child Neurol. 2007, 49, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Field, D.; Livingstone, R. Clinical tools that measure sitting posture, seated postural control or functional abilities in children with motor impairments: A systematic review. Clin. Rehabil. 2013, 27, 994–1004. [Google Scholar] [CrossRef] [PubMed]
- Field, D.A.; Miller, W.C.; Ryan, S.E.; Jarus, T.; Abundo, A. Measuring participation for children and youth with power mobility needs: A systematic review of potential health measurement tools. Arch. Phys. Med. Rehabil. 2015, 97, 462–477. [Google Scholar] [CrossRef] [PubMed]
- Law, M. Outcome Measures Rating Form Guidelines. Available online: http://www.canchild.ca/en/canchildresources.resources.measguid.pdf (accessed on 7 May 2016).
- Barnes, S.B.; Whinnery, K.W. Effects of Functional Mobility Skills Training for Young Students with Physical Disabilities. Except. Child. 2002, 68, 313–324. [Google Scholar] [CrossRef]
- Eisenberg, S.; Zuk, L.; Carmeli, E.; Katz-Leurer, M. Contribution of stepping while standing to function and secondary conditions among children with cerebral palsy. Pediatr. Phys. Ther. 2009, 21, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Farrell, E.; Naber, E.; Geigle, P. Description of a multifaceted rehabilitation program including overground gait training for a child with cerebral palsy: A case report. Physiother. Theory Pract. 2010, 26, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Lancioni, G.; Nirbhay, N.; O’Reilly, F.; Campodonico, F.; Oliva, O.; Vigo, C. Promoting walker-assisted step responses by an adolescent with multiple disabilities through automatically delivered stimulation. J. Vis. Impair. Blind 2005, 99, 109–113. [Google Scholar]
- Lancioni, G.E.; Singh, N.N.; O’Reilly, M.F.; Sigafoos, J.; Oliva, D.; Scalini, L.; Castagnaro, F.; Di Bari, M. Promoting foot-leg movements in children with multiple disabilities through the use of support devices and technology for regulating contingent stimulation. Cogn. Process. 2007, 8, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Lancioni, G.E.; Singh, N.N.; O’Reilly, M.F.; Sigafoos, J.; Oliva, D.; Piazzolla, G.; Pidala, S.; Smaldone, A.; Manfredi, F. Automatically Delivered Stimulation for Walker-Assisted Step Responses: Measuring its Effects in Persons with Multiple Disabilities. J. Dev. Phys. Disabil. 2007, 19, 1–13. [Google Scholar] [CrossRef]
- Van der Putten, A.; Vlaskamp, C.; Reynders, K.; Nakken, H. Children with profound intellectual and multiple disabilities: The effects of functional movement activities. Clin. Rehabil. 2005, 19, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Willoughby, K.L.; Dodd, K.J.; Shields, N.; Foley, S. Efficacy of partial body weight-supported treadmill training compared with overground walking practice for children with cerebral palsy: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2010, 91, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Wright, F.V.; Belbin, G.; Slack, M.; Jutai, J. An evaluation of the David Hart Walker Orthosis: A new assistive device for children with Cerebral Palsy. Physiother. Can. 1999, 51, 280–291. [Google Scholar]
- Wright, F.V.; Jutai, J.W. Evaluation of the longer-term use of the David Hart Walker Orthosis by children with cerebral palsy: A 3-year prospective evaluation. Disabil. Rehabil. Assist. Technol. 2006, 1, 155–166. [Google Scholar] [CrossRef] [PubMed]
- Evans, M.D.; Goldie, P.A.; Hill, K.D. Systematic and random error in repeated measurements of temporal and distance parameters of gait after stroke. Arch. Phys. Med. Rehabil. 1997, 78, 725–729. [Google Scholar] [CrossRef]
- Pirpiris, M.; Wilkinson, A.J.; Rodda, J.; Nguyen, T.C.; Baker, R.J.; Nattrass, G.R.; Graham, H.K. Walking speed in children and young adults with neuromuscular disease: Comparison between two assessment methods. J. Pediatr. Orthop. 2003, 23, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Russell, D.; Rosenbaum, P.; Cadman, D.; Gowland, C.; Hardy, S.; Jarvis, S. The Gross Motor Function Measure: A means to evaluate the effects of physical therapy. Dev. Med. Child Neurol. 1989, 31, 341–352. [Google Scholar] [CrossRef] [PubMed]
- Haley, S.; Coster, W.; Ludlow, L. Pediatric Evaluation of Disability Inventory: Development, Standardization and Administration Manual; New England Medical Center Publications: Boston, MA, USA, 1992. [Google Scholar]
- Suskauer, S.; Slomine, B.; Salorio, C.; Bradley, E.; Madigan, L.; Sesma, H.; Christensen, J. The physical abilities and mobility scale. J. Head Trauma Rehabil. 2006, 21, 420–420. [Google Scholar] [CrossRef]
- Coster, W.; Deeney, T.; Haltiwanger, J.; Haley, S. School Function Assessment (SFA) User’s Manual; PsychCorp: San Antonio, TX, USA, 1998. [Google Scholar]
- Lancioni, G.E.; Singh, N.N.; O’Reilly, M.F.; Sigafoos, J.; Oliva, D.; Campodonico, F.; Buono, S. Walker devices and microswitch technology to enhance assisted indoor ambulation by persons with multiple disabilities: Three single-case studies. Res. Dev. Disabil. 2013, 34, 2191–2199. [Google Scholar] [CrossRef] [PubMed]
- Van der Putten, A.; Vlaskamp, C.; Reynders, K.; Nakken, H. Movement skill assessment in children with profound multiple disabilities: A psychometric analysis of the Top Down Motor Milestone Test. Clin. Rehabil. 2005, 19, 635–643. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.C.; Bode, R.K.; Granger, C.V.; Heinemann, A.W. Psychometric Properties and Developmental Differences in Children’s ADL Item Hierarchy. Am. J. Phys. Med. Rehabil. 2005, 84, 671–679. [Google Scholar] [CrossRef] [PubMed]
- Uniform Data System for Medical Rehabilitation: WeeFIM System Clinical Guide, 5th ed.; University of Buffalo: New York, NY, USA, 1998.
- Tedla, J.S.; Ganesan, S.; Katragadda, S. Inter-rater reliability of the Top Down Motor Milestone Test: A cross-sectional study. Clin. Rehabil. 2009, 23, 725–729. [Google Scholar] [CrossRef] [PubMed]
- Thompson, P.; Beath, T.; Bell, J.; Jacobson, G.; Phair, T.; Salbach, N.M.; Wright, F.V. Test-retest reliability of the 10-metre fast walk test and 6-minute walk test in ambulatory school-aged children with cerebral palsy. Dev. Med. Child Neurol. 2008, 50, 370–376. [Google Scholar] [CrossRef] [PubMed]
- Graser, J.V.; Letsch, C.; Van Hedel, H.J.A. Reliability of timed walking tests and temporo-spatial gait parameters in youths with neurological gait disorders. BMC Neurol. 2016, 16, 15. [Google Scholar] [CrossRef] [PubMed]
- Trovato, M.K.; Bradley, E.; Slomine, B.S.; Salorio, C.F.; Christensen, J.R.; Suskauer, S.J. Physical abilities and mobility scale: Reliability and validity in children receiving inpatient rehabilitation for acquired brain injury. Arch. Phys. Med. Rehabil. 2013, 94, 1335–1341. [Google Scholar] [CrossRef] [PubMed]
- Kuenzle, C.; Brunner, R. The effects of the Norsk Funktion-walking orthosis on the walking ability of children with cerebal palsy and severe gait impairment. J. Prosthet. Orthot. 2009, 21, 138–144. [Google Scholar] [CrossRef]
- Maher, C.; Williams, L.; Olds, T. The six-minute walk test for children with cerebral palsy. Int. J. Rehabil. Res. 2008, 31, 185–188. [Google Scholar] [CrossRef] [PubMed]
- Law, M.; Baptiste, S.; Carswell, A.; McColl, M.; Polatajko, H.; Pollock, N. Canadian Occupational Performance Measure, 2nd ed.; Canadian Association of Occupational Therapists: Toronto, ON, Canada, 1994. [Google Scholar]
- Westcott McCoy, S.; Yocum, A.; Bartlett, D.J.; Mendoza, J.; Jeffries, L.; Chiarello, L.; Palisano, R.J. Development of the Early Activity Scale for Endurance for children with cerebral palsy. Pediatr. Phys. Ther. 2012, 24, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Kiresuk, T.; Smith, A.; Cardillo, J. Goal Attainment Scaling: Application, Theory and Measurement; Lawrence Erlbaum Associates: Hillscale, NJ, USA, 1994. [Google Scholar]
- Scherer, M. Matching Assistive Technology & Child (MATCH. A Process and Series of Assessments for Selecting and Evaluating Technologies Used by Infants and Young Children; The Institute for Matching Person & Technology: Webster, NY, USA, 1998. [Google Scholar]
- Demers, L.; Weiss-Lambrou, R.; Ska, B. The Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST Version 2.0), 2000. Available online: http://www.midss.ie/sites/default/files/questmanual_final_electronic20version_0.pdf (accessed on 7 May 2016).
- Malouin, F.; Richards, C.; Menier, C.; Dumas, F.; Marcoux, S. Supported walker ambulation performance scale (SWAPS): Development of an outcome measure of locomotor status in children with cerebral palsy. Pediatr. Phys. Ther. 1997, 9, 48–53. [Google Scholar] [CrossRef]
- Dodd, K.J. Partial body-weight-supported treadmill training can improve walking in children with cerebral palsy: A clinical controlled trial. Dev. Med. Child Neurol. 2007, 49, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Ko, J.; Kim, M. Reliability and responsiveness of the gross motor function measure-88 in children with cerebral palsy. Phys. Ther. 2013, 93, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Wright, F.; Boschen, K. Use of the Pediatric Evaluation of Disability Inventory to detect change in functional status in children with cerebral palsy. Physiother. Can. 1996, 48 (Suppl. 2), 1–6. [Google Scholar]
- Nichols, D.; Case-Smith, J. Reliability and Validity of the Pediatric Evaluation of Disability Inventory. Pediatr. Phys. Ther. 1996, 8, 15–24. [Google Scholar] [CrossRef]
- Iyer, L.V.; Haley, S.M.; Watkins, M.P.; Dumas, H.M. Establishing minimal clinically important differences for scores on the pediatric evaluation of disability inventory for inpatient rehabilitation. Phys. Ther. 2003, 83, 888–898. [Google Scholar] [PubMed]
- Wright, F.V.; Boschen, K.; Jutai, J. Exploring the comparative responsiveness of a core set of outcome measures in a school-based conductive education programme. Child Care Health Dev. 2005, 31, 291–302. [Google Scholar] [CrossRef] [PubMed]
- Wright, F.; Liu, G.; Milne, F. Reliability of the measurement of time-distance parameters of gait: A comparison in children with juvenile rheumatoid arthritis and children with cerebral palsy. Physiother. Can. 1999, 15, 191–200. [Google Scholar]
- Nsenga Leunkeu, A.; Shephard, R.J.; Ahmaidi, S. Six-minute walk test in children with cerebral palsy gross motor function classification system levels I and II: Reproducibility, validity, and training effects. Arch. Phys. Med. Rehabil. 2012, 93, 2333–2339. [Google Scholar] [CrossRef] [PubMed]
- Cusick, A.; Lannin, N.A.; Lowe, K. Adapting the Canadian Occupational Performance Measure for use in a paediatric clinical trial. Disabil. Rehabil. 2007, 29, 761–766. [Google Scholar] [CrossRef] [PubMed]
- Verkerk, G.J.Q.; Wolf, M.J.M.; Louwers, A.M.; Meester-Delver, A.; Nollet, F. The reproducibility and validity of the Canadian Occupational Performance Measure in parents of children with disabilities. Clin. Rehabil. 2006, 20, 980–988. [Google Scholar] [CrossRef] [PubMed]
- Wallen, M.A.; Ziviani, J.M. Canadian Occupational Performance Measure: Impact of blinded parent-proxy ratings on outcome. Can. J. Occup. Ther. 2012, 79, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Cusick, A.; McIntyre, S.; Novak, I.; Lannin, N.; Lowe, K. A comparison of goal attainment scaling and the Canadian Occupational Performance Measure for paediatric rehabilitation research. Pediatr. Rehabil. 2006, 9, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Reid, D.; Rigby, P.; Ryan, S. Functional impact of a rigid pelvic stabilizer on children with cerebral palsy who use wheelchairs: users’ and caregivers’ perceptions. Pediatr. Rehabil. 1999, 3, 101–118. [Google Scholar] [PubMed]
- Bottos, M.; Bolcati, C.; Sciuto, L.; Ruggeri, C.; Feliciangeli, A. Powered wheelchairs and independence in young children with tetraplegia. Dev. Med. Child Neurol. 2001, 43, 769–777. [Google Scholar] [CrossRef] [PubMed]
- Carswell, A.; McColl, M.A.; Baptiste, S.; Law, M.; Polatajko, H.; Pollock, N. The Canadian Occupational Performance Measure: A research and clinical literature review. Can. J. Occup. Ther. 2004, 71, 210–222. [Google Scholar] [CrossRef] [PubMed]
- Steenbeek, D.; Ketelaar, M.; Lindeman, E.; Galama, K.; Gorter, J.W. Interrater Reliability of Goal Attainment Scaling in Rehabilitation of Children With Cerebral Palsy. Arch. Phys. Med. Rehabil. 2010, 91, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Law, L.S.H.; Dai, M.O.; Siu, A. Applicability of goal attainment scaling in the evaluation of gross motor changes in children with cerebral palsy. Hong Kong Physiother. J. 2004, 22, 22–28. [Google Scholar] [CrossRef]
- Steenbeek, D.; Gorter, J.W.; Ketelaar, M.; Galama, K.; Lindeman, E. Responsiveness of Goal Attainment Scaling in comparison to two standardized measures in outcome evaluation of children with cerebral palsy. Clin. Rehabil. 2011, 25, 1128–1139. [Google Scholar] [CrossRef] [PubMed]
- Demers, L.; Weiss-Lambrou, R.; Ska, B. Item analysis of the Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST). Assist. Technol. 2000, 12, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Demers, L.; Weiss-lambrou, R.; Ska, B. The Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST 2.0): An overview and recent progress. Technol. Disabil. 2002, 14, 101–105. [Google Scholar]
- Kurz, M.J.; Stuberg, W.; Dejong, S.; Arpin, D.J. Overground body-weight-supported gait training for children and youth with neuromuscular impairments. Phys. Occup. Ther. Pediatr. 2013, 33, 353–365. [Google Scholar] [CrossRef] [PubMed]
- Stuberg, W.; DeJong, S.; Kelly, M. Gait training using partial body weight support during over ground walking in individuals with developmental disabilities. Pediatr. Phys. Ther. 2004, 16, 65–66. [Google Scholar]
- Watson, M.J. Refining the ten-metre walking test for use with neurologically impaired people. Physiother 2002, 88, 386–397. [Google Scholar] [CrossRef]
- Haley, S.M.; Coster, W.I.; Kao, Y.C.; Dumas, H.M.; Fragala-Pinkham, M.A.; Kramer, J.M.; Ludlow, L.H.; Moed, R. Lessons from use of the Pediatric Evaluation of Disability Inventory: Where do we go from here? Pediatr. Phys. Ther. 2010, 22, 69–75. [Google Scholar] [CrossRef] [PubMed]
- SCIRE Project. Available online: http://www.scireproject.com/outcome-measures-new/10-m-walking-test-10-mwt# (accessed on 26 July 2016).
- Russell, D.; Rosenbaum, P.; Avery, L.; Lane, M. The Gross Motor Function Measure (GMFM-66 and GMFM-88) User’s Manual; Cambridge University Press: Cambridege, UK, 2002. [Google Scholar]
- Steenbeek, D.; Ketelaar, M.; Galama, K.; Gorter, J.W. Goal attainment scaling in paediatric rehabilitation: A report on the clinical training of an interdisciplinary team. Child Care Health Dev. 2008, 34, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Tefft, D.; Guerette, P.; Furumasu, J. The impact of early powered mobility on parental stress, negative emotions, and family social interactions. Phys. Occup. Ther. Pediatr. 2011, 31, 4–15. [Google Scholar] [CrossRef] [PubMed]
- Palisano, R.J.; Chiarello, L.A.; King, G.A.; Novak, I.; Stoner, T.; Fiss, A. Participation-based therapy for children with physical disabilities. Disabil. Rehabil. 2012, 34, 1041–1052. [Google Scholar] [CrossRef] [PubMed]
- Mattern-Baxter, K.; Bellamy, S.; Mansoor, J.K. Effects of intensive locomotor treadmill training on young children with cerebral palsy. Pediatr. Phys. Ther. 2009, 21, 308–318. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.; McEwen, I.; Neas, B. Effects of power wheelchairs on the development and function of young children with severe motor impairments. Pediatr. Phys. Ther. 2012, 24, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Gibson, B.E.; Teachman, G.; Wright, V.; Fehlings, D.; Young, N.L.; McKeever, P. Children’s and parents’ beliefs regarding the value of walking: Rehabilitation implications for children with cerebral palsy. Child Care Health Dev. 2012, 38, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Meyer-Heim, A.; Ammann-Reiffer, C.; Schmartz, A.; Schaefer, J.; Sennhauser, F.H.; Heinen, F.; Knecht, B.; Dabrowski, E.; Borggraefe, I. Improvement of walking abilities after robotic-assisted locomotion training in children with cerebral palsy. Arch. Dis. Child 2009, 94, 615–620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richards, C.L.; Malouin, F.; Dumas, F.; Marcoux, S.; Lepage, C.; Menier, C. Early and intensive treadmill locomotor training for young children with cerebral palsy: A feasibility study. Pediatr. Phys. Ther. 1997, 9, 158–165. [Google Scholar] [CrossRef]
- Drouin, L.M.; Malouin, F.; Richards, C.L.; Marcoux, S. Correlation between the gross motor function measure scores and gait spatiotemporal measures in children with neurological impairments. Dev. Med. Child Neurol. 1996, 38, 1007–1019. [Google Scholar] [CrossRef] [PubMed]
- Carty, C.P.; Walsh, H.P.J.; Gillett, J.G.; Phillips, T.; Edwards, J.M.; Boyd, R.N. The effect of femoral derotation osteotomy on transverse plane hip and pelvic kinematics in children with cerebral palsy: A systematic review and meta-analysis. Gait Posture 2014, 40, 333–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schroeder, A.S.; Homburg, M.; Warken, B.; Auffermann, H.; Koerte, I.; Berweck, S.; Jahn, K.; Heinen, F.; Borggraefe, I. Prospective controlled cohort study to evaluate changes of function, activity and participation in patients with bilateral spastic cerebral palsy after Robot-enhanced repetitive treadmill therapy. Eur. J. Paediatr. Neurol. 2014, 18, 502–510. [Google Scholar] [CrossRef] [PubMed]
- Scherer, M.J.; Craddock, G. Matching Person & Technology ({MPT}) assessment process. Technol. Disabil. 2002, 14, 125–132. [Google Scholar]
- Benedict, R.; Lee, J.; Marrujo, S.; Farel, A. Assistive devices as an early childhood intervention: Evaluating outcomes. Technol. Disabil. 1999, 11, 79–90. [Google Scholar]
- Novak, I.; McIntyre, S.; Morgan, C.; Campbell, L.; Dark, L.; Morton, N.; Stumbles, E.; Wilson, S.; Goldsmith, S. A systematic review of interventions for children with cerebral palsy: state of the evidence. Dev. Med. Child Neurol. 2002, 55, 885–910. [Google Scholar] [CrossRef] [PubMed]
- Amman-Reiffer, C.; Bastiaenen, C.H.G.; De Bie, R.A.; Van Hedel, H.J.A. Measurement properties of gait-related outcomes in youth with neuromuscular diagnoses: A systematic review. Phys. Ther. 2014, 94, 1067–1082. [Google Scholar] [CrossRef] [PubMed]
- Himoru, N.; Hirokazu, A.; Nishibu, H.; Seino, T.; Mori, M. Easy to use clinical measures of walking ability in children and adolescents with cerebral palsy: A systematic review. Disabil. Rehabil. 2016. [Google Scholar] [CrossRef] [PubMed]
- Streiner, D.L.; Norman, G.R.; Cairney, J. Health Measurement Scales: A Practical Guide to Their Development and Use; Oxford University Press: Oxford, UK, 2014. [Google Scholar]
- Andresen, E.M. Criteria for assessing the tools of disability outcomes research. Arch. Phys. Med. Rehabil. 2000, 81, S15–S20. [Google Scholar] [CrossRef] [PubMed]
- Terwee, C.B.; Prinsen, C.A.C.; Ricci Garotti, M.G.; Suman, A.; De Vet, H.C.W.; Mokkink, L.B. The quality of systematic reviews of health-related outcome measurement instruments. Qual. Life Res. 2016, 25, 767–779. [Google Scholar] [CrossRef] [PubMed]
- Mokkink, L.B.; Terwee, C.B.; Stratford, P.W.; Alonso, J.; Patrick, D.L.; Riphagen, I.; Knol, D.L.; Bouter, L.M.; DeVet, H.C.W. Evaluation of the methodological quality of systematic reviews of health status measurement instruments. Qual. Life Res. 2009, 18, 313–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuhrer, M.J.; Jutai, J.W.; DeRuyter, F.A. A framework for the conceptual modelling of assistive technology device outcomes. Disabil. Rehabil. 2003, 25, 1243–1251. [Google Scholar] [CrossRef] [PubMed]
| Description | Reliability | Validity | Sensitivity and Responsiveness |
|---|---|---|---|
| Clinical Tools Used in Gait Trainer Intervention Studies | |||
| 10-m walk test [26,27] Participant observation capacity measure. Time taken to walk the middle 10 m of a 14-m walkway measured with a stopwatch. Walking speed calculated by dividing time by distance. | Adequate test-retest reliability GMFCS III—ICC 0.78 (95% CI 45–93), SEM 6.4 s [37] Excellent test-retest reliability at preferred speed GMFCS II and III: ICC 0.90 (95% CI 0.8–0.95) SEM 3.61 s [38] | Face and Content Validity: More appropriate for evaluating gait kinematics than speed with GMFCS I–III [27] Used to measure self-selected walking speed in children with GMFCS IV and V [23] | MDC95 in children functioning at GMFCS III 17.7 s [37] SRD in children functioning at GMFCS II and III—10 s [38] |
| Poor for GMFCS IV and V | Poor for GMFCS IV and V | Poor for GMFCS IV and V | |
| 10 min walk test [27] Participant observation capacity measure. Distance walked in 10 min is recorded. Studies including children with CP used a 20-m oval track marked at 1-m intervals [23,27,48]. | Good test-retest reliability in children with neuromuscular conditions including CP GMFCS III ICC > 0.91 95% CI [27] | Face and Content Validity: Measure of community walking ability for children with CP [27] Feasible for some children GMFCS IV and V using walkers and gait trainers [23] | |
| Poor for GMFCS IV and V | Poor for GMFCS IV and V | Not established | |
| DMA [24,25] Participant observation capacity measure. Measures ability to maneuver gait trainer. 11 items on 5 point scale indicating full, partial or inability to complete. | Convergent Validity: moderate correlation between DMA and GMFM dimension E. r = 0.59 p = 0.007 [25] | ||
| Not established | Adequate | Not established | |
| GMFM-88 [28] Participant observation capacity measure. Criterion-referenced, evaluative measure for children with CP. 5 dimensions: A lying and rolling; B crawling and kneeling; C sitting; D standing; and E walking, running and jumping. | Intra-rater and inter-rater reliability reported to be excellent in multiple studies. ICC > 0.95 at all GMFCS levels [49] | Reported to have excellent face, content and construct validity in multiple studies. | Responsive to change in children with CP [28]. Regardless of GMFCS level [49] |
| Excellent | Excellent | Excellent | |
| Indices of happiness/affect [19,21] Participant observation capacity measure. Count incidences of alertness, smiling or positive affect within a set time period from video recording | Mean agreement of 92% [21] and 94% [19] between two raters 20% of sessions. | ||
| Adequate | Not established | Not established | |
| PAMS [30] Participant observation capacity measure. Evaluative measure of gross motor function. Each item rated on a 5 point scale 1 = no tolerance—5 = complete tolerance of an activity. | High inter-rater reliability—ICC 0.99 for children with BI [39] | Internal consistency—0.97 [30] Validated for children with Acquired BI. Criterion validity with WeeFIM mobility scale [39] | |
| Poor for CP | Poor for CP | Not established | |
| PEDI [29] Performance measure involving structured parent interview. Measures functional abilities and caregiver assistance in self-care, mobility and social function. | Good reliability in CP [50,51] | Good validity in children with CP reported in multiple studies. | MCID—between 6 and 15 points or an 11% change on all scales [52] |
| Excellent | Excellent | Adequate | |
| SFA Travel subscale [31] Performance measure involving parent or caregiver report. Criterion referenced judgment-based questionnaire with 3 domains. The travel subscale is part of the Activity domain. Rated on 4-point scale: 1 (does not perform) to 4 (consistently performs). | Good test-retest reliability for Activity domain 0.8–0.99 [23]. Inter-rater reliability ICC 0.73 for Activity performance subscale [12]. | Content validity from expert panel and factor analysis. Discriminative validity: Detects differences between children with/without CP [12]. Activity domain difficult for children with CP [53]. | |
| Adequate | Adequate | Not established | |
| Step/leg movement counting [16,20,21,32] Participant observation capacity measure. Involves counting number of independent steps or leg movements within a set time period. | Inter-rater reliability checks completed at least twice with each child—100% agreement [16]. Mean agreement of 96% [20] or >90% [32] between two raters 20% trials. | ||
| Adequate | Not established | Not established | |
| Step length and velocity footprint analysis [24,25] Participant observation capacity measure. Step length is analyzed from footprint analysis taken from pressure sensitive paper. | Good inter-rater reliability in school-aged children with CP (ICC > 70) [54] Excellent test-retest reliability for children GMFCS I-III ICC = 0.86 SEM 0.14 m/s [54] | Face validity: Used with children using hands-free gait trainers in two studies [24,25] | |
| Poor | Poor | Not established | |
| Top Down Motor Milestone Test (TDMMT) [33] Performance measure completed by school and therapy team. Assesses sitting, standing and walking skills in individuals with severe and profound multiple disabilities. | Test-retest reliability mean 0.8 range—0.54 to 0.9. Item test reliability 0.97 range—0.58–1.0. Strong internal consistency —cronbach’s alpha 0.95 [33] Test-retest reliability individual subtests—kappa 0.74–0.96 Pooled kappa—0.88 SEM 0.06 p < 0.01 [36] | Construct validity: Factor analysis did not confirm the three underlying factors of standing, sitting and walking but only one or two factors. Suggests a uni-dimensional theoretical construct | |
| Adequate | Poor | Not established | |
| WeeFIM [34,35] Performance Measure—structured interview with parents. 18-item assessment used to determine level of assistance needed in self-care and mobility tasks. Items rated on 7 point scale from 1 (total dependence) to 7 (independent). | Reported to be reliable (0.94) in the pediatric inpatient population [34] | Face and Content Validity: Valid for inpatient population [34] Discriminative Validity: Detects significant change in mobility level with/without gait trainer and previous aid [40] | Not sensitive to changes in non-ambulatory children [18] |
| Poor for GMFCS IV and V | Poor for GMFCS IV and V | Not established | |
| Tools used with children at GMFCS IV and V with other interventions | |||
| 6-min walk test [41] Participant observation capacity measure. Measures distance walked at preferred or fastest speed over 6-min time period. Assistive devices can be used. Time measured with stopwatch. Measuring wheel used to record distance. Walking back and forth on short straight track not recommended due to negative impact of direction changes. | Excellent test-retest reliability in GMFCS III ICC = 0.98 (95% CI 95–99), SEM 17.1 [37] Excellent test-retest reliability in GMFCS I and II ICC = 0.89 (95% CI 77–95) SEM 58.02 [38] Excellent test-retest reliability in GMFCS I–III ICC 0.98 [41] MDC95 47.4m GMFCS III [37] SRD 160.82m [38] | Construct Validity—Valid measure of cardiovascular fitness for children with CP GMFCS levels I and II [55] | |
| Poor for GMFCS IV and V | Poor for GMFCS IV and V | Not established | |
| COPM [42] Performance level individualized outcome measure—completed by child or parent proxy in semi-structured interview. Clients identify and rate importance of up to five goals in the areas of self-care, productivity and leisure. Performance and satisfaction of these goals are rated from 1–10 and difference from baseline to follow-up (change score) is used as an outcome. The manual recommends parent-proxy rating for children below 8 years of age. | Internal consistency Acceptable reliability when completed by parent proxy [56] Performance—Cronbach’s alpha 0.73 Satisfaction—Cronbach’s alpha 0.83 Inter-rater reliability 80 parents of children with disabilities including 14 with CP. Limits of agreement −2.4 to +2.3 mean performance and −2.3 to +2.6 mean satisfaction scores [57] Test-retest reliability No significant difference blinded or unblinded to previous rating of parents of 50 children hemiplegic CP [58] | Content validity: adapted for pediatrics and valid for use by parent proxy for children with hemiplegic CP [56,59] Construct and criterion validity: Valid for use with parents of children with a wide range of disabilities [57] 6 children with CP aged 8–12 years rated with caregivers present [60] Significant change in level of independence rated by parents of children with CP GMFCS IV and V following use of a power wheelchair [61] | A change of 2 points is thought to represent a clinically significant change in adult studies [62] Sensitivity to change —able to detect medium effect size in children with hemiplegic CP Performance—ES 0.78 Satisfaction—ES 0.69 [59] |
| Adequate for GMFCS IV and V | Adequate for GMFCS IV and V | Poor for GMFCS IV and V | |
| EASE [43] Performance level parent report measure. Estimates endurance for physical activity for children with CP aged 2–6 years of age. Frequency, intensity and duration of physical activity in typical environments rated on 5-point scale. Maximum score 50-higher scores = higher levels of endurance for physical activity. | Test-retest reliability Excellent-ICC (2,1) = 0.95 95%CI (0.90–0.98) Internal Consistency Good—Cronbach’s alpha 0.93 Absolute reliability SEM 2.9—at 68% CI Minimal Detectable Difference 8.0—at 95% CI—a difference of 8 points could be within measurement error | Discriminative Validity Scores differed significantly between all GMFCS levels except children at GMFCS II and III Convergent Validity Moderate correlation (rs = 0.57) between EASE and 6 min walk test for children at GMFCS I and II | |
| Adequate for GMFCS IV and V | Adequate for GMFCS IV and V | Not established | |
| MATCH [45] Personal and environmental factors parent-report measure. Parents rate statements on a 4 point likert scale from strongly agree to strongly disagree or on a 5 point likert scale from very satisfied to not satisfied at all. Statements range from satisfaction with child’s ability to use the device, go where desired, sleep-wake cycle, communication, play and social skills as well as the parent’s feelings of stress or frustration. | No reliability testing found with parents of children with CP GMFCS levels IV and V | No validity testing found with parents of children with CP GMFCS levels IV and V | |
| Poor | Poor | Not established | |
| GAS [44] Performance level individualized outcome measure completed by child and/or parent proxy. Clients select goals and rate these on a 5 point scale where 0 = expected level of achievement; +1 = somewhat more than expected; +2 = much more than expected; −1 = somewhat less than expected; −2 = much less than expected. Overall score calculated by incorporating goal outcome scores into a single aggregated T score. | Inter-rater reliability Good to excellent ICC 0.82 (95% CI 73–91) Children with CP GMFCS I–V [63] Excellent inter and intra-rater reliability in children with CP at a range of GMFCS levels ICC = 0.96 (95% CI 93–97 and 94–98, respectively) [64] | Content validity established for use with children with CP at a range of GMFCS levels [64] Convergent validity with COPM for children with hemiplegic CP [59] | Responsive to change in activity goals in children CP at all GMFCS levels [65] Likert scale GAS more sensitive than weighted GAS goals or COPM in hemiplegic CP [59]. Responsive to change in gross motor goals at a range of GMFCS levels [64] |
| Excellent for GMFCS IV and V | Adequate for GMFCS IV and V | Adequate for GMFCS IV and V | |
| QUEST 2.0 [46] Measure evaluating environmental factors completed by child and/or parent proxy. Evaluates client satisfaction with assistive technology. 8 item device scale and a 4 item services scale can be scored separately. Each item rated on 5-point scale from not satisfied at all to very satisfied. | Excellent and adequate inter-rater and intra-rater reliability with adults using mobility devices Device = 0.80 Service = 0.76 Total = 0.82 [66] Excellent test-retest reliability with adults ICC: Device = 0.82 Service = 0.82 Total = 0.91 [67] | No validity testing completed with children with CP. | |
| Poor for CP | Poor for CP | Not established | |
| SWAPS [47] Participant observation capacity measure. Measures locomotor changes in non-independent walkers. Four dimensions: level of support; posture; quality of steps; quantity of steps. Each rated on 4 point likert scale. Support is weighted at 40% and the other dimensions at 20% each with 100% score representing independent walking. | Excellent Inter-rater reliability ICC 2.1 0.95 with lower 95% CI of 0.89 [47] | Convergent validity Moderate correlation with GMFM Spearman rho 0.68 [47] | Did not detect significant change in children at GMFCS II or III despite increased overground walking speed [68] Only marginal change in total score following overground gait training in children, four with CP GMFCS levels unclear [69] |
| Adequate for GMFCS IV and V | Adequate for GMFCS IV and V | Not established | |
| Measure (ICF) | Clinical Utility and Usefulness for Children Using Gait Trainers | Overall Utility |
|---|---|---|
| Tools suitable for use in clinical practice or research | ||
| PEDI [29] (A & P) | Appears sensitive to changes in mobility level in short-term intervention studies. Sensitivity to changes in caregiver assistance and impact on self-care and social domains require further exploration. | Excellent |
| Tools that need further development but show potential for use in clinical practice/research | ||
| COPM [42] (A & P) | Manual available for purchase. Time efficient and easy to use in OT practice. Responsiveness with children at GMFCS IV and V needs further development. | Adequate |
| GAS [44] (A & P) | Freely available. Can be time consuming and difficult to score. Training is strongly recommended prior to use in effect studies with children [74]. Reliability, validity and responsiveness for children functioning at GMFCS IV and V need further development. | Adequate |
| SWAPS [47] (A) | Freely available with scale and scoring descriptions available as an appendix to the original article [47]. Designed to measure changes in gait in children transitioning from dependent to independent walking. Limited documentation of use to measure gait changes in children at GMFCS levels IV or V. May need adaptation for use with gait trainers (Francine Malouin, personal communication 18, April 2016). | Adequate |
| TDMMT [33] (A) | Can administer a shortened set of items increasing clinical utility. Designed to be used with the Rifton gait trainer. However not all skills included can be accomplished with a gait trainer e.g., sitting skills, or higher level walking skills such as stairs. Validity and responsiveness need further development. | Adequate |
| Further development of psychometric properties needed | ||
| DMA [24,25] (A) | Not available. Not included as an appendix to the articles. Only two sample items are included in the follow-up study [25]. Reliability, validity and responsiveness for children using gait trainers need further development. | Poor |
| EASE [43] (A) | Feasible and low burden indirect measure of a child’s endurance for physical activity. Reliability, validity and responsiveness with children at GMFCS IV and V need further development. | Poor |
| Indices of happiness [19,21] (BSF) | Simple to carry out in clinical practice. | Poor |
| QUEST 2.0 [46] (EF) | Freely available. Low administrative and time burden. Reliability, validity and responsiveness for children at GMVCS levels IV and V need further development. | Poor |
| Step/leg movement counting [16,20,21,32] (A) | Simple to carry out in clinical practice. Demands full attention of assessor unless videotaped for later analysis | Poor |
| May be useful for children who are more active walkers or require less body weight support | ||
| 6-min walk test [41] (A) | Free and easy to use in clinical practice. Younger children and children with reduced cognitive abilities can be difficult to motivate to complete the test reliably [38] as can young children who use walking aids [43]. | Poor |
| 10-m walk test [26,27] (A) | Testing protocol freely available and utility with children who use gait trainers documented. Simple to set up in a school or community setting. However, reliability, validity and responsiveness not yet established for children with CP functioning at GMFCS IV and V. | Poor |
| 10 min walk test [27] (A) | Testing protocol described in Willoughby [23]. Able to be used by children who use gait trainers. Relatively simple to conduct in a school or community setting. Reliability, validity and responsiveness not yet established for children functioning at GMFCS IV and V. | Poor |
| Utility for children using gait trainers questionable | ||
| GMFM-88 [28] (A) | Only 6/14 items in domain D and 8/14 items in domain E can be completed by a child using a gait trainer [24]. May show secondary changes due to increased activity in gait trainer but does not directly assess gait trainer function. | Poor |
| MATCH [45] (EF & PF) | The entire questionnaire is extensive and too lengthy for routine use in clinical practice. Impact on the reliability and validity from non standard use e.g., administration of selected items only [75] unclear. | Poor |
| PAMS [30] (A) | Developed for an inpatient rehabilitation setting. Not validated for children with CP. Not freely available. | Poor |
| SFA [31] Travel subscale (A) | Reflects typical performance rather than based on a single trial therefore not suitable for blinded assessment. Reliability, validity and responsiveness with children at GMFCS IV and V need further development. | Poor |
| Step length and velocity footprint analysis [24,25] (A) | May be challenging to complete in the clinical settingrequires pressure sensitive paper or some type of gait recognition mat. Reliability, validity and responsiveness with children at GMFCS levels IV and V who use gait trainers need further development. | Poor |
| WeeFIM [34,35] (A) | Able to discriminate mobility function in children with and without functional mobility aids, but may not be useful for detecting change over time in children at GMFCS levels IV and V. | Poor |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Livingstone, R.; Paleg, G. Measuring Outcomes for Children with Cerebral Palsy Who Use Gait Trainers. Technologies 2016, 4, 22. https://doi.org/10.3390/technologies4030022
Livingstone R, Paleg G. Measuring Outcomes for Children with Cerebral Palsy Who Use Gait Trainers. Technologies. 2016; 4(3):22. https://doi.org/10.3390/technologies4030022
Chicago/Turabian StyleLivingstone, Roslyn, and Ginny Paleg. 2016. "Measuring Outcomes for Children with Cerebral Palsy Who Use Gait Trainers" Technologies 4, no. 3: 22. https://doi.org/10.3390/technologies4030022
APA StyleLivingstone, R., & Paleg, G. (2016). Measuring Outcomes for Children with Cerebral Palsy Who Use Gait Trainers. Technologies, 4(3), 22. https://doi.org/10.3390/technologies4030022