


Dynamic Surgical Prioritization: A Machine Learning and XAI-Based Strategy

 ,
,  , and
, and
Abstract
1. Introduction
2. Literature Review
Justification of the Chosen Method
- Traditional prioritization frameworks do not integrate temporal evolution and competitive dynamics among patients. By combining stochastic simulations with LightGBM, our methodology models the dynamic progression of patient conditions and incorporates competitive interactions, offering a comprehensive solution.
- Many ML models for prioritization lack interpretability, limiting their utility in clinical settings. Our integration of SHAP analysis ensures transparency and provides actionable insights into global and patient-specific contributions.
- Existing methods often ignore the interaction between dynamic variables and resource limitations. Our framework explicitly models these interactions, dynamically adjusting prioritization strategies based on evolving patient conditions and healthcare resources.
- Some studies leverage XAI to provide detailed explanations of prioritization decisions. Our approach contributes by employing SHAP to highlight the role of clinical, social, and psychological factors, fostering trust and alignment with medical guidelines.
3. Methodology
3.1. Dataset Description and Clinical Context
3.2. Foundations for Predictive Modeling
- We model the prioritization mathematically by predicting a dynamic prioritization score, , for each patient p at time t, based on their clinical, social, and psychological characteristics, represented by a feature vector , as follows:where is a feature vector consisting of dynamic () and static () variables, represents a predictive model trained to estimate , and is the set of parameters learned during model training.
- We categorize the variables into the following dynamic and static groups:
- -
- Dynamic variables () reflect changes in the patient’s condition over time, such as Sever () or Urg ().
- -
- Static variables () represent intrinsic characteristics of the patient, such as Jclin () or Tlist ().
- We represent the dataset as a matrix , where N denotes the total number of patients, and n represents the number of features.where represents the complete feature vector for patient p, comprising dynamic variables , which evolve over time (e.g., Sever, Urg) and have dimension h, and static variables , which remain fixed (e.g., Opat, Diag) with dimension r. The dynamic variables exist in an h-dimensional real-valued space (), while static variables exist in an r-dimensional real-valued space ().In Equation (3), Z represents the dataset matrix containing features and the physicians’ prioritization scores (Pscore) for all patients. Each row corresponds to a specific patient p, where are the characteristics n (including dynamic and static variables), and is the prioritization score assigned by the physician for patient p. The dataset includes N patients, with , where accounts for the n features and the Pscore.
- We model the evolution of dynamic variables over time. The state of a dynamic variable at time is given bywhere represents the observed change between time t and . This approach allows us to capture how dynamic variables evolve over time, reflecting changes in patient conditions.
- To standardize variable scales and mitigate biases in model training, we normalize variables using Min–Max scaling [47,48], as follows:where and represent the observed minimum and maximum values of variable v. This normalization ensures that all variables are on a comparable scale, improving the stability and performance of our model.
3.3. LightGBM Model: A Strategy to Prioritize Patients on the Surgical Waiting List
- LightGBM constructs decision trees using gradient boosting, which optimizes predictive performance by minimizing a specified loss function [52,53]. The loss function used during training is given bywhere each predicted prioritization score, , reflecting dynamic conditions over time, is modeled as a function of patient-specific features (), with the observed static physician-assigned score () serving as the benchmark for evaluation as follows:where is the feature vector for patient p at time t, which includes both static and updated dynamic variables, and represents the set of hyperparameters defining the model configuration. By incorporating static and dynamic variables into the feature vector, we ensure that the model accounts for both intrinsic patient characteristics and evolving clinical conditions. This configuration enables us to accurately predict while maintaining flexibility and interpretability in the model design.
3.4. Dynamic Evolution of Prioritizations and Stochastic Simulation
- Dynamic variables evolve over time, representing changes in patient conditions. We model these variables using discrete time steps, reflecting temporal intervals. Let represent the set of dynamic variables for patient p at time t. The state of these variables at the next time step, , is modeled aswhere represents the growth rate, and is stochastic noise [58]. The noise term follows a Gaussian distribution as follows:where is the standard deviation of variable v.
- We adjust growth rates based on competition as follows:where represents the initial growth rate of the dynamic variable v for patient p at time t, and denotes the contribution of variable v to the prioritization score of another patient at the same time t. The term is the cumulative contribution of variable v to the prioritization scores of all patients other than p. Similarly, represents the total contribution of variable v to the prioritization scores of all patients at time t. The competitive adjustment term,allows us to quantify the relative impact of other patients on the growth rate of patient p. If other patients exhibit high contributions to variable v, this reduces the relative weight of for patient p, thereby incorporating competitive dynamics into the prioritization model.
- At each time step, we recalculate as follows:The prioritization score of patient p at time t is dynamically estimated using the trained predictive model (), which incorporates static and updated dynamic variables from the characteristic vector . The model parameters () are learned during training, allowing to reflect evolving patient conditions and ensuring adaptability to temporal changes in clinical needs.
3.5. SHAP-Based Interpretability for LightGBM Model
- The importance of each variable over time was quantified using the mean absolute Shapley value [28,59], defined aswhere represents the global importance of variable v across all patients at time t, N is the total number of patients, and denotes the Shapley value of v for patient p at time t. This metric captures the average absolute contribution of each variable to the dynamic prioritization scores , offering critical insights into its influence at specific time points.
- We analyzed variable interactions using the following joint Shapley value formula:where represents the combined contribution of variables and to the prioritization score for patient p at time t. Here, and are the individual contributions of and , while captures their joint contribution. This formula quantifies the interactions between variables, revealing synergies or redundancies that influence the dynamic predictions of the model [60].
- We decomposed , the prioritization score of patient p at time t, as follows:where represents the baseline prediction, corresponding to the mean across all patients, and quantifies the contribution of variable v to for patient p at time t. This decomposition enables transparency by explaining the specific factors influencing , ensuring interpretability in the context of dynamic patient conditions.
4. Results
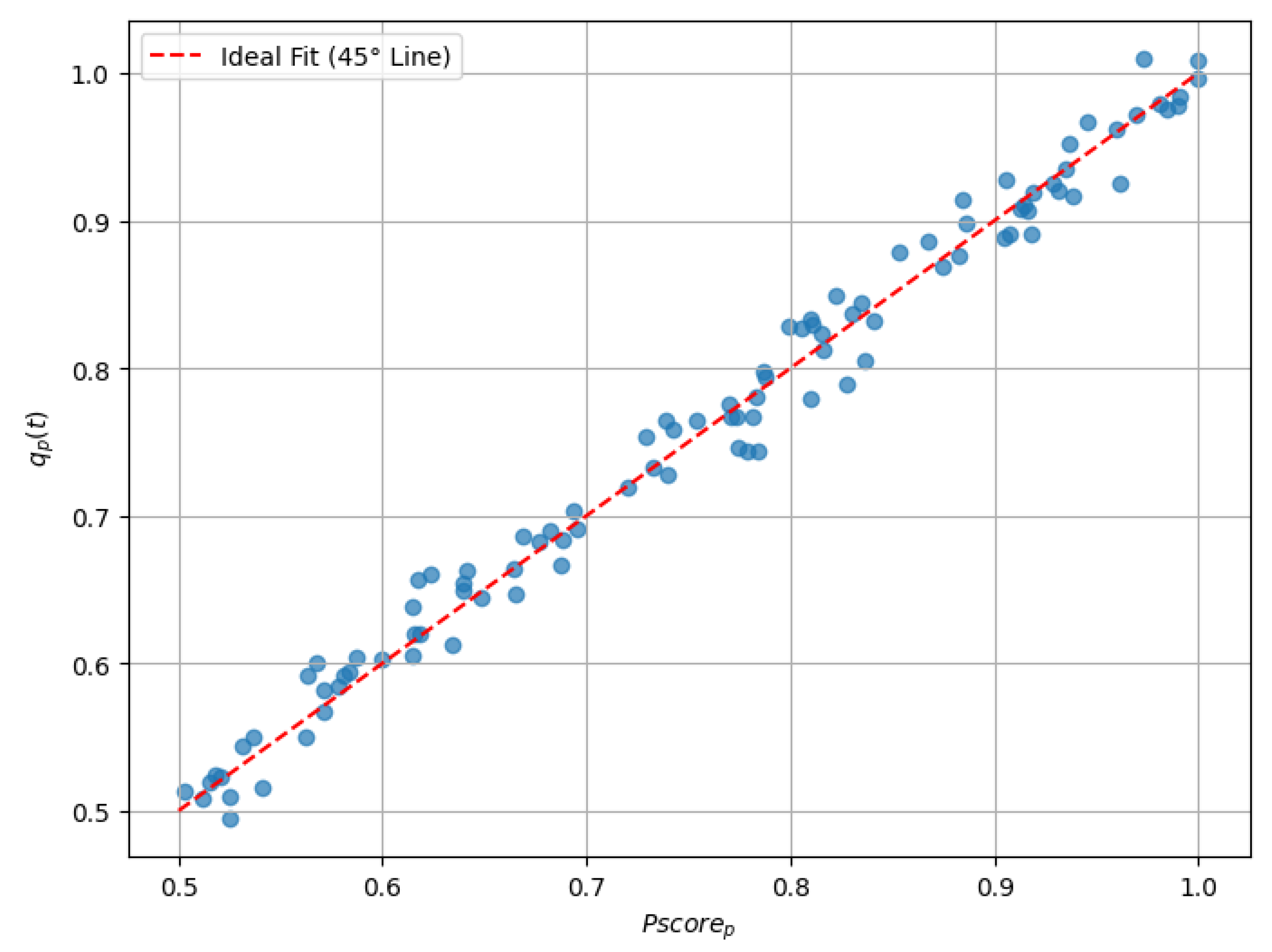
4.1. Performance Evaluation of the LightGBM Predictive Model
4.2. Sensitivity Analysis of Stochastic Simulation Parameters
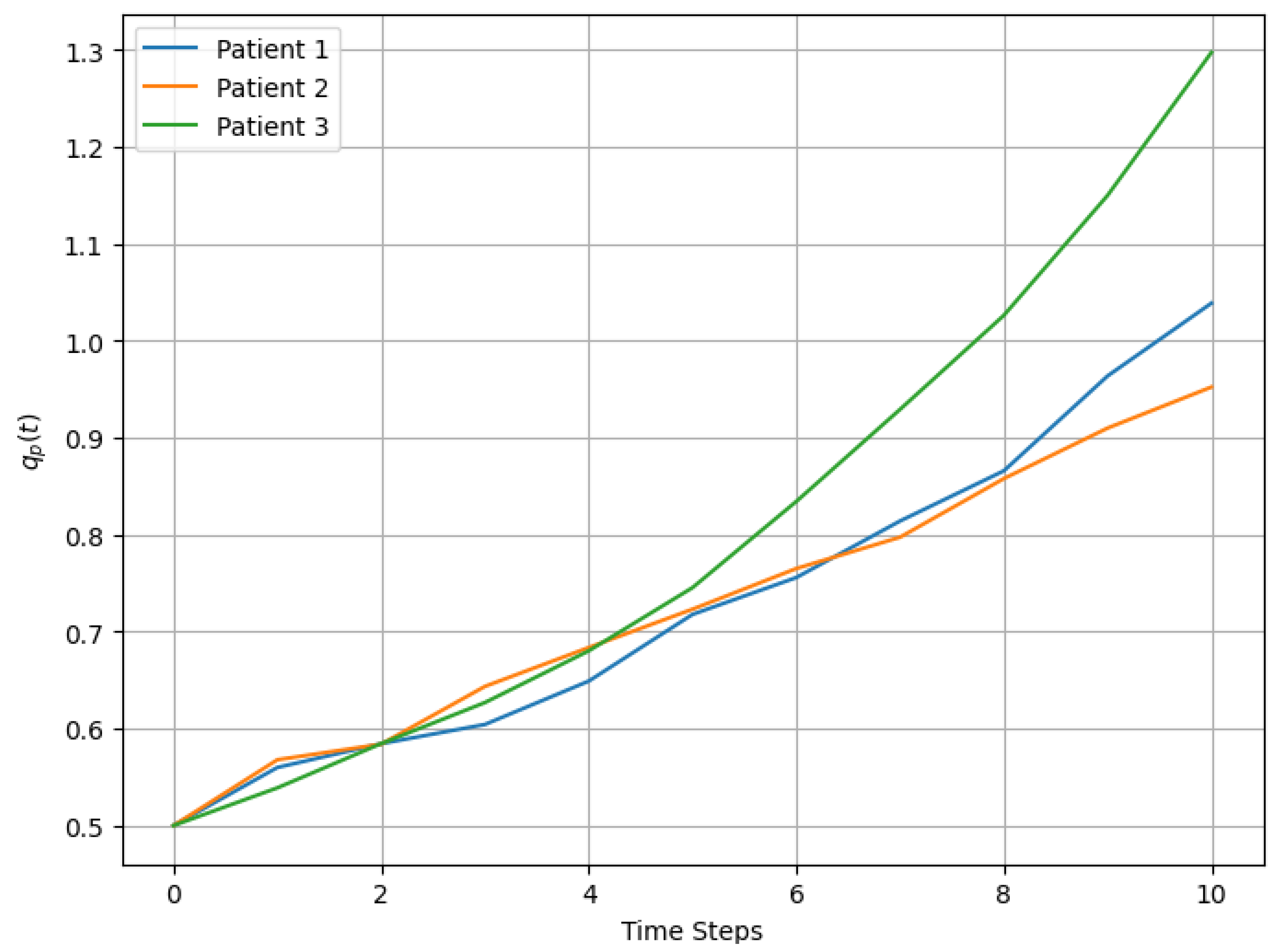
4.3. Analysis of Prioritization Dynamics Through Stochastic Simulations
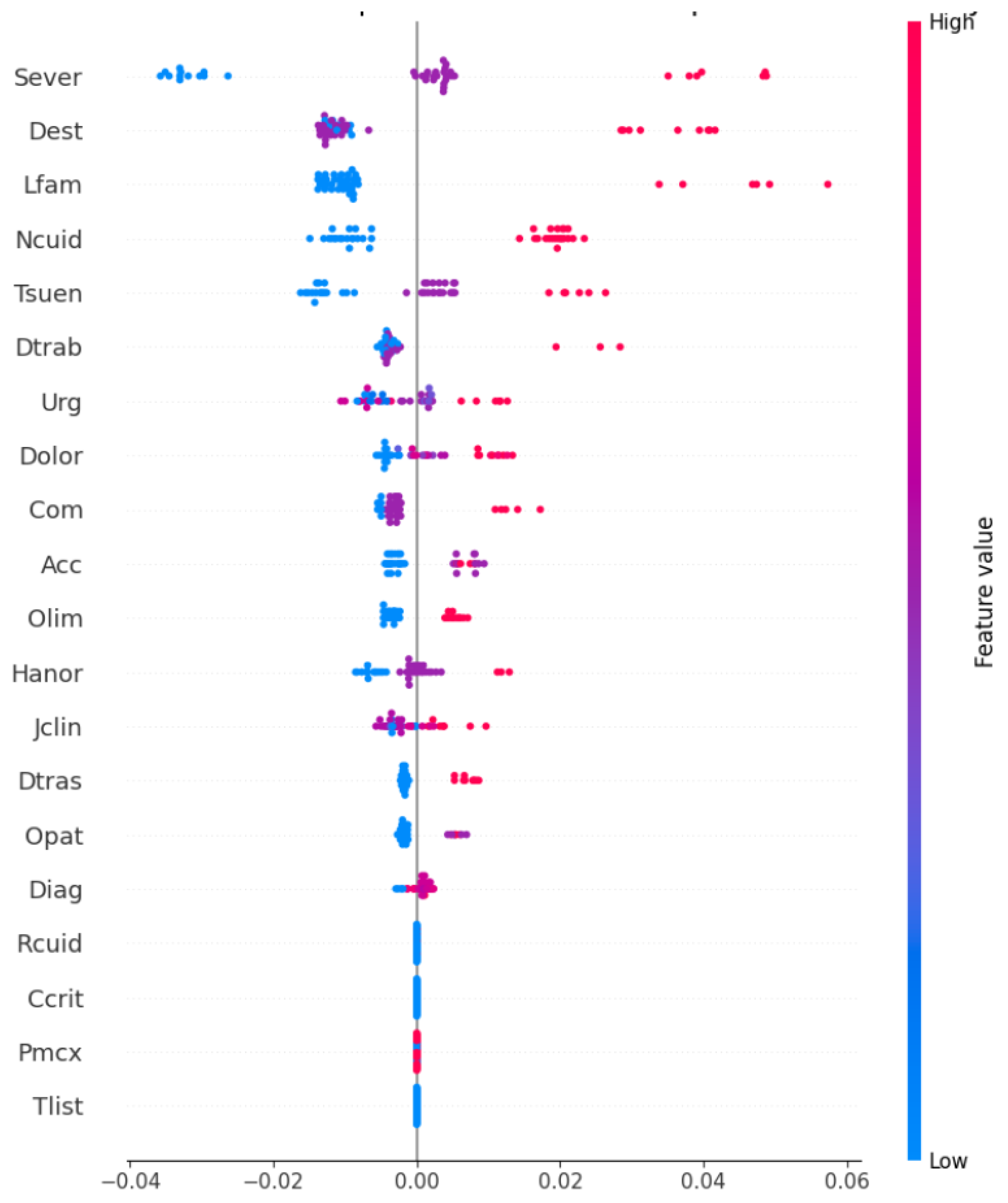
4.4. Insights from SHAP-Based Interpretability of the LightGBM Model
4.5. Impact of Dynamic Prioritization on Waiting Time Management
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Silva-Aravena, F.; Álvarez-Miranda, E.; Astudillo, C.A.; González-Martínez, L.; Ledezma, J.G. Patients’ prioritization on surgical waiting lists: A decision support system. Mathematics 2021, 9, 1097. [Google Scholar] [CrossRef]
- García-Corchero, J.D.; Jiménez-Rubio, D. Waiting times in healthcare: Equal treatment for equal need? Int. J. Equity Health 2022, 21, 184. [Google Scholar] [CrossRef] [PubMed]
- Rana, H.; Umer, M.; Hassan, U.; Asgher, U.; Silva-Aravena, F.; Ehsan, N. Application of fuzzy TOPSIS for prioritization of patients on elective surgeries waiting list—A novel multi-criteria decision-making approach. Decis. Mak. Appl. Manag. Eng. 2023, 6, 603–630. [Google Scholar] [CrossRef]
- Rahimi, S.A.; Jamshidi, A.; Ruiz, A.; Aït-Kadi, D. A new dynamic integrated framework for surgical patients’ prioritization considering risks and uncertainties. Decis. Support Syst. 2016, 88, 112–120. [Google Scholar] [CrossRef]
- Mohammed, K.; Zaidan, A.; Zaidan, B.; Albahri, O.S.; Alsalem, M.; Albahri, A.S.; Hadi, A.; Hashim, M. Real-time remote-health monitoring systems: A review on patients prioritisation for multiple-chronic diseases, taxonomy analysis, concerns and solution procedure. J. Med. Syst. 2019, 43, 1–21. [Google Scholar] [CrossRef]
- Ahmed, A.; He, L.; Chou, C.a.; Hamasha, M.M. A prediction-optimization approach to surgery prioritization in operating room scheduling. J. Ind. Prod. Eng. 2022, 39, 399–413. [Google Scholar] [CrossRef]
- Keyvanshokooh, E.; Kazemian, P.; Fattahi, M.; Van Oyen, M.P. Coordinated and priority-based surgical care: An integrated distributionally robust stochastic optimization approach. Prod. Oper. Manag. 2022, 31, 1510–1535. [Google Scholar] [CrossRef]
- Bamaarouf, S.; Jawab, F.; Frichi, Y. Elective surgery prioritization criteria and tools: A literature review. In Proceedings of the 2024 IEEE 15th International Colloquium on Logistics and Supply Chain Management (LOGISTIQUA), Sousse, Tunisia, 2–4 May 2024; IEEE: Piscataway, NJ, USA, 2024; pp. 1–6. [Google Scholar]
- Silva-Aravena, F.; Álvarez-Miranda, E.; Astudillo, C.A.; González-Martínez, L.; Ledezma, J.G. On the data to know the prioritization and vulnerability of patients on surgical waiting lists. Data Brief 2020, 29, 105310. [Google Scholar] [CrossRef]
- Skillings, J.L.; Lewandowski, A.N. Team-based biopsychosocial care in solid organ transplantation. J. Clin. Psychol. Med. Settings 2015, 22, 113–121. [Google Scholar] [CrossRef]
- Silva-Aravena, F.; Morales, J. Dynamic surgical waiting list methodology: A networking approach. Mathematics 2022, 10, 2307. [Google Scholar] [CrossRef]
- Stitini, O.; Ouakasse, F.; Rakrak, S.; Kaloun, S.; Bencharef, O. Combining IoMT and XAI for Enhanced Triage Optimization: An MQTT Broker Approach with Contextual Recommendations for Improved Patient Priority Management in Healthcare. Int. Online Biomed. Eng. 2024, 20, 145. [Google Scholar] [CrossRef]
- Silva-Aravena, F.; Delafuente, H.N.; Astudillo, C.A. A novel strategy to classify chronic patients at risk: A hybrid machine learning approach. Mathematics 2022, 10, 3053. [Google Scholar] [CrossRef]
- Kim, S.Y.; Kim, D.H.; Kim, M.J.; Ko, H.J.; Jeong, O.R. XAI-Based Clinical Decision Support Systems: A Systematic Review. Appl. Sci. 2024, 14, 6638. [Google Scholar] [CrossRef]
- Cutillo, C.M.; Sharma, K.R.; Foschini, L.; Kundu, S.; Mackintosh, M.; Mandl, K.D.; MI in Healthcare Workshop Working Group. Machine intelligence in healthcare—Perspectives on trustworthiness, explainability, usability, and transparency. Npj Digit. Med. 2020, 3, 47. [Google Scholar] [CrossRef]
- Guo, L.L.; Guo, L.Y.; Li, J.; Gu, Y.W.; Wang, J.Y.; Cui, Y.; Qian, Q.; Chen, T.; Jiang, R.; Zheng, S. Characteristics and Admission Preferences of Pediatric Emergency Patients and Their Waiting Time Prediction Using Electronic Medical Record Data: Retrospective Comparative Analysis. J. Med. Internet Res. 2023, 25, e49605. [Google Scholar] [CrossRef]
- Yu, Z.; Ashrafi, N.; Li, H.; Alaei, K.; Pishgar, M. Prediction of 30-day mortality for ICU patients with Sepsis-3. Bmc Med. Inform. Decis. Mak. 2024, 24, 223. [Google Scholar] [CrossRef]
- Rathnayake, D.; Clarke, M.; Jayasinghe, V. Patient prioritisation methods to shorten waiting times for elective surgery: A systematic review of how to improve access to surgery. PLoS ONE 2021, 16, e0256578. [Google Scholar] [CrossRef]
- Adeniran, I.A.; Efunniyi, C.P.; Osundare, O.S.; Abhulimen, A.O. Data-driven decision-making in healthcare: Improving patient outcomes through predictive modeling. Eng. Sci. Technol. J. 2024, 5, 59–67. [Google Scholar]
- Bakker, M.; Tsui, K.L. Dynamic resource allocation for efficient patient scheduling: A data-driven approach. J. Syst. Sci. Syst. Eng. 2017, 26, 448–462. [Google Scholar] [CrossRef]
- Morales, J.; Silva-Aravena, F.; Saez, P. Reducing Waiting Times to Improve Patient Satisfaction: A Hybrid Strategy for Decision Support Management. Mathematics 2024, 12, 3743. [Google Scholar] [CrossRef]
- Asif, S.; Wenhui, Y.; ur Rehman, S.; ul ain, Q.; Amjad, K.; Yueyang, Y.; Jinhai, S.; Awais, M. Advancements and Prospects of Machine Learning in Medical Diagnostics: Unveiling the Future of Diagnostic Precision. Arch. Comput. Methods Eng. 2024, 1–31. [Google Scholar] [CrossRef]
- Li, L. Application of Machine learning and data mining in Medicine: Opportunities and considerations. In Machine Learning and Data Mining Annual Volume 2023; IntechOpen Limited: London, UK, 2023. [Google Scholar]
- Nasarian, E.; Alizadehsani, R.; Acharya, U.R.; Tsui, K.L. Designing interpretable ML system to enhance trust in healthcare: A systematic review to proposed responsible clinician-AI-collaboration framework. Inf. Fusion 2024, 108, 102412. [Google Scholar] [CrossRef]
- Fahimullah, M.; Ahvar, S.; Agarwal, M.; Trocan, M. Machine learning-based solutions for resource management in fog computing. Multimed. Tools Appl. 2024, 83, 23019–23045. [Google Scholar] [CrossRef]
- Yasin, P.; Yimit, Y.; Cai, X.; Aimaiti, A.; Sheng, W.; Mamat, M.; Nijiati, M. Machine learning-enabled prediction of prolonged length of stay in hospital after surgery for tuberculosis spondylitis patients with unbalanced data: A novel approach using explainable artificial intelligence (XAI). Eur. J. Med. Res. 2024, 29, 383. [Google Scholar] [CrossRef]
- Khanna, V.V.; Chadaga, K.; Sampathila, N.; Prabhu, S.; Chadaga, R. A machine learning and explainable artificial intelligence triage-prediction system for COVID-19. Decis. Anal. J. 2023, 7, 100246. [Google Scholar] [CrossRef]
- Silva-Aravena, F.; Núñez Delafuente, H.; Gutiérrez-Bahamondes, J.H.; Morales, J. A hybrid algorithm of ml and xai to prevent breast cancer: A strategy to support decision making. Cancers 2023, 15, 2443. [Google Scholar] [CrossRef]
- Bhandari, M.; Yogarajah, P.; Kavitha, M.S.; Condell, J. Exploring the capabilities of a lightweight CNN model in accurately identifying renal abnormalities: Cysts, stones, and tumors, using LIME and SHAP. Appl. Sci. 2023, 13, 3125. [Google Scholar] [CrossRef]
- Gaur, L.; Bhandari, M.; Razdan, T.; Mallik, S.; Zhao, Z. Explanation-driven deep learning model for prediction of brain tumour status using MRI image data. Front. Genet. 2022, 13, 822666. [Google Scholar] [CrossRef]
- Rane, N.; Choudhary, S.; Rane, J. Explainable Artificial Intelligence (XAI) in healthcare: Interpretable Models for Clinical Decision Support. SSRN 2023, 4637897. [Google Scholar] [CrossRef]
- Frichi, Y.; Aboueljinane, L.; Jawab, F. Using discrete-event simulation to assess an AHP-based dynamic patient prioritisation policy for elective surgery. J. Simul. 2023, 19, 39–63. [Google Scholar] [CrossRef]
- Antoniadi, A.M.; Du, Y.; Guendouz, Y.; Wei, L.; Mazo, C.; Becker, B.A.; Mooney, C. Current challenges and future opportunities for XAI in machine learning-based clinical decision support systems: A systematic review. Appl. Sci. 2021, 11, 5088. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Shaw, S.; Wherton, J.; Vijayaraghavan, S.; Morris, J.; Bhattacharya, S.; Hanson, P.; Campbell-Richards, D.; Ramoutar, S.; Collard, A.; et al. Real-world implementation of video outpatient consultations at macro, meso, and micro levels: Mixed-method study. J. Med. Internet Res. 2018, 20, e150. [Google Scholar] [CrossRef] [PubMed]
- Kislov, R.; Checkland, K.; Wilson, P.M.; Howard, S.J. ‘Real-world’priority setting for service improvement in English primary care: A decentred approach. Public Manag. Rev. 2023, 25, 150–174. [Google Scholar] [CrossRef]
- Kundu, S.; Bhattacharya, A.; Chandan, V.; Radhakrishnan, N.; Adetola, V.; Vrabie, D. A Stochastic Multi-Criteria Decision-Making Algorithm for Dynamic Load Prioritization in Grid-Interactive Efficient Buildings. Asme Lett. Dyn. Syst. Control 2021, 1, 031014. [Google Scholar] [CrossRef]
- Feng, W.H.; Lou, Z.; Kong, N.; Wan, H. A multiobjective stochastic genetic algorithm for the pareto-optimal prioritization scheme design of real-time healthcare resource allocation. Oper. Res. Health Care 2017, 15, 32–42. [Google Scholar] [CrossRef]
- Zion, G.D.; Tripathy, B. Pattern Prediction on Uncertain Big Datasets using Combined Light GBM and LSTM Model. Int. J. Adv. Soft Comput. Its Appl. 2023, 15, 288–310. [Google Scholar]
- Zhou, F.; Hu, S.; Du, X.; Wan, X.; Lu, Z.; Wu, J. Lidom: A Disease Risk Prediction Model Based on LightGBM Applied to Nursing Homes. Electronics 2023, 12, 1009. [Google Scholar] [CrossRef]
- Saito, H.; Yoshimura, H.; Tanaka, K.; Kimura, H.; Watanabe, K.; Tsubokura, M.; Ejiri, H.; Zhao, T.; Ozaki, A.; Kazama, S.; et al. Predicting CKD progression using time-series clustering and light gradient boosting machines. Sci. Rep. 2024, 14, 1723. [Google Scholar] [CrossRef]
- Malik, S.; Rathee, P. Enhancing COVID-19 Diagnosis Accuracy and Transparency with Explainable Artificial Intelligence (XAI) Techniques. Comput. Sci. 2024, 5, 806. [Google Scholar] [CrossRef]
- Sadeghi, Z.; Alizadehsani, R.; CIFCI, M.A.; Kausar, S.; Rehman, R.; Mahanta, P.; Bora, P.K.; Almasri, A.; Alkhawaldeh, R.S.; Hussain, S.; et al. A review of Explainable Artificial Intelligence in healthcare. Comput. Electr. Eng. 2024, 118, 109370. [Google Scholar] [CrossRef]
- Li, J.; Luo, L.; Wu, X.; Liao, C.; Liao, H.; Shen, W. Prioritizing the elective surgery patient admission in a Chinese public tertiary hospital using the hesitant fuzzy linguistic ORESTE method. Appl. Soft Comput. 2019, 78, 407–419. [Google Scholar] [CrossRef]
- Silva-Aravena, F.; Gutiérrez-Bahamondes, J.H.; Núñez Delafuente, H.; Toledo-Molina, R.M. An intelligent system for patients’ well-being: A multi-criteria decision-making approach. Mathematics 2022, 10, 3956. [Google Scholar] [CrossRef]
- Raza, A.; Eid, F.; Montero, E.C.; Noya, I.D.; Ashraf, I. Enhanced interpretable thyroid disease diagnosis by leveraging synthetic oversampling and machine learning models. BMC Med. Inform. Decis. Mak. 2024, 24, 364. [Google Scholar] [CrossRef] [PubMed]
- Powers, J.; McGree, J.M.; Grieve, D.; Aseervatham, R.; Ryan, S.; Corry, P. Managing surgical waiting lists through dynamic priority scoring. Health Care Manag. Sci. 2023, 26, 533–557. [Google Scholar] [CrossRef]
- Cao, X.H.; Stojkovic, I.; Obradovic, Z. A robust data scaling algorithm to improve classification accuracies in biomedical data. BMC Bioinform. 2016, 17, 359. [Google Scholar] [CrossRef]
- Henderi, H.; Wahyuningsih, T.; Rahwanto, E. Comparison of Min-Max normalization and Z-Score Normalization in the K-nearest neighbor (kNN) Algorithm to Test the Accuracy of Types of Breast Cancer. Int. J. Inform. Inf. Syst. 2021, 4, 13–20. [Google Scholar] [CrossRef]
- Liu, S.; Lu, C. An Active SearchTime Tuning Model Based on the Optimally Weighted LightGBM Algorithm. In Proceedings of the Journal of Physics: Conference Series, Shanghai, China, 26–28 August 2022; IOP Publishing: Bristol, UK, 2022; Volume 2383, p. 012149. [Google Scholar]
- Qiuqian, W.; GaoMin; KeZhu, Z.; Chenchen. A light gradient boosting machine learning-based approach for predicting clinical data breast cancer. Multiscale Multidiscip. Model. Exp. Des. 2025, 8, 75. [Google Scholar] [CrossRef]
- Kanber, B.M.; Smadi, A.A.; Noaman, N.F.; Liu, B.; Gou, S.; Alsmadi, M.K. LightGBM: A Leading Force in Breast Cancer Diagnosis Through Machine Learning and Image Processing. IEEE Access 2024, 237, 121618. [Google Scholar] [CrossRef]
- Rufo, D.D.; Debelee, T.G.; Ibenthal, A.; Negera, W.G. Diagnosis of diabetes mellitus using gradient boosting machine (LightGBM). Diagnostics 2021, 11, 1714. [Google Scholar] [CrossRef]
- Yang, H.; Chen, Z.; Yang, H.; Tian, M. Predicting coronary heart disease using an improved LightGBM model: Performance analysis and comparison. IEEE Access 2023, 11, 23366–23380. [Google Scholar] [CrossRef]
- Zeng, X. Length of stay prediction model of indoor patients based on light gradient boosting machine. Comput. Intell. Neurosci. 2022, 2022, 9517029. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Jin, N.; Dogani, A.; Yang, Y.; Zhang, M.; Gu, X. Enhancing LightGBM for Industrial Fault Warning: An Innovative Hybrid Algorithm. Processes 2024, 12, 221. [Google Scholar] [CrossRef]
- Altenbuchinger, M.; Weihs, A.; Quackenbush, J.; Grabe, H.J.; Zacharias, H.U. Gaussian and Mixed Graphical Models as (multi-) omics data analysis tools. Biochim. Biophys. Acta (BBA)-Gene Regul. Mech. 2020, 1863, 194418. [Google Scholar] [CrossRef] [PubMed]
- Bakhshaei, K.; Salavatidezfouli, S.; Stabile, G.; Rozza, G. Stochastic Parameter Prediction in Cardiovascular Problems. arXiv 2024, arXiv:2411.18089. [Google Scholar]
- Heo, J.; Lee, H.B.; Kim, S.; Lee, J.; Kim, K.J.; Yang, E.; Hwang, S.J. Uncertainty-aware attention for reliable interpretation and prediction. Adv. Neural Inf. Process. Syst. 2018, 31. [Google Scholar]
- Bloch, L.; Friedrich, C.M.; Initiative, A.D.N. Data analysis with Shapley values for automatic subject selection in Alzheimer’s disease data sets using interpretable machine learning. Alzheimer’S Res. Ther. 2021, 13, 155. [Google Scholar] [CrossRef]
- Yu, Q.; Hou, Z.; Wang, Z. Predictive modeling of preoperative acute heart failure in older adults with hypertension: A dual perspective of SHAP values and interaction analysis. BMC Med. Inform. Decis. Mak. 2024, 24, 329. [Google Scholar] [CrossRef]
- Dobbin, K.K.; Simon, R.M. Optimally splitting cases for training and testing high dimensional classifiers. BMC Med. Genom. 2011, 4, 31. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Variable | Definition |
|---|---|---|
| 1 | Sever (*) | Severity |
| 2 | Urg (*) | Urgency |
| 3 | Jclin | Maximum waiting time |
| 4 | Tsuen (*) | Sleep disorder |
| 5 | Tlist | Time on list |
| 6 | Pmcx(*) | Expected improvement due to surgery |
| 7 | Dest(*) | Capacity to study |
| 8 | Com(*) | Chances of developing comorbidities |
| 9 | Lfam(*) | Capacity of participating in family activities |
| 10 | Hanor(*) | Affected area |
| 11 | Opat | Presence of other pathologies |
| 12 | Diag | Diagnosis |
| 13 | Olim(*) | Other limitations |
| 14 | Ncuid | Need of a caregiver |
| 15 | Rcuid | Patient cares for another person |
| 16 | Dolor(*) | Pain sale |
| 17 | Dtrab | Capacity to work |
| 18 | Acc | Type of residence area |
| 19 | Dtras | Difficulty in transferring |
| 20 | Ccrit | Need for clinical bed |
| 21 | Pscore | Physician’s score, given by the health team |
| Patient | Residual | ||
|---|---|---|---|
| 1 | 0.78 | 0.76 | 0.02 |
| 2 | 0.85 | 0.87 | −0.02 |
| 3 | 0.66 | 0.68 | −0.02 |
| 4 | 0.72 | 0.73 | −0.01 |
| 5 | 0.81 | 0.79 | 0.02 |
| 6 | 0.75 | 0.74 | 0.01 |
| 7 | 0.69 | 0.67 | 0.02 |
| 8 | 0.88 | 0.86 | 0.02 |
| 9 | 0.77 | 0.76 | 0.01 |
| 10 | 0.80 | 0.82 | −0.02 |
| Patient | Sever | Urg | |
|---|---|---|---|
| Patient 1 | 0.54 | 0.52 | 0.50 |
| Patient 2 | 0.59 | 0.43 | 0.50 |
| Patient 3 | 0.55 | 0.43 | 0.50 |
| Time (t) | Sever | Urg | |
|---|---|---|---|
| 5 | 0.780 | 0.630 | 0.720 |
| 10 | 1.250 | 0.690 | 1.026 |
| Patient | Pscore | WTPs | WT(t) | Improvement (%) | ||
|---|---|---|---|---|---|---|
| 7 | 0.70 | 0.43 | 0.59 | 1.23 | 0.91 | 26.10 |
| 6 | 0.87 | 0.49 | 0.63 | 1.62 | 1.35 | 16.83 |
| 5 | 0.77 | 0.49 | 0.62 | 1.62 | 1.35 | 16.79 |
| 3 | 0.63 | 0.83 | 1.10 | 3.92 | 3.39 | 13.56 |
| 2 | 0.98 | 0.97 | 1.26 | 4.80 | 4.21 | 12.24 |
| 9 | 0.69 | 0.76 | 0.94 | 3.40 | 3.03 | 10.94 |
| 8 | 0.74 | 0.91 | 1.12 | 4.46 | 4.05 | 9.18 |
| 4 | 0.93 | 0.75 | 0.90 | 3.39 | 3.10 | 8.39 |
| 1 | 0.54 | 0.62 | 0.72 | 2.49 | 2.28 | 8.33 |
| 10 | 0.51 | 0.82 | 0.98 | 3.83 | 3.51 | 8.25 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva-Aravena, F.; Morales, J.; Jayabalan, M.; Rana, M.E.; Gutiérrez-Bahamondes, J.H. Dynamic Surgical Prioritization: A Machine Learning and XAI-Based Strategy. Technologies 2025, 13, 72. https://doi.org/10.3390/technologies13020072
Silva-Aravena F, Morales J, Jayabalan M, Rana ME, Gutiérrez-Bahamondes JH. Dynamic Surgical Prioritization: A Machine Learning and XAI-Based Strategy. Technologies. 2025; 13(2):72. https://doi.org/10.3390/technologies13020072
Chicago/Turabian StyleSilva-Aravena, Fabián, Jenny Morales, Manoj Jayabalan, Muhammad Ehsan Rana, and Jimmy H. Gutiérrez-Bahamondes. 2025. "Dynamic Surgical Prioritization: A Machine Learning and XAI-Based Strategy" Technologies 13, no. 2: 72. https://doi.org/10.3390/technologies13020072
APA StyleSilva-Aravena, F., Morales, J., Jayabalan, M., Rana, M. E., & Gutiérrez-Bahamondes, J. H. (2025). Dynamic Surgical Prioritization: A Machine Learning and XAI-Based Strategy. Technologies, 13(2), 72. https://doi.org/10.3390/technologies13020072