
An Affordable Upper-Limb Exoskeleton Concept for Rehabilitation Applications

 ,
,  ,
, 

Abstract
:1. Introduction
State of the Art
2. Materials and Methods
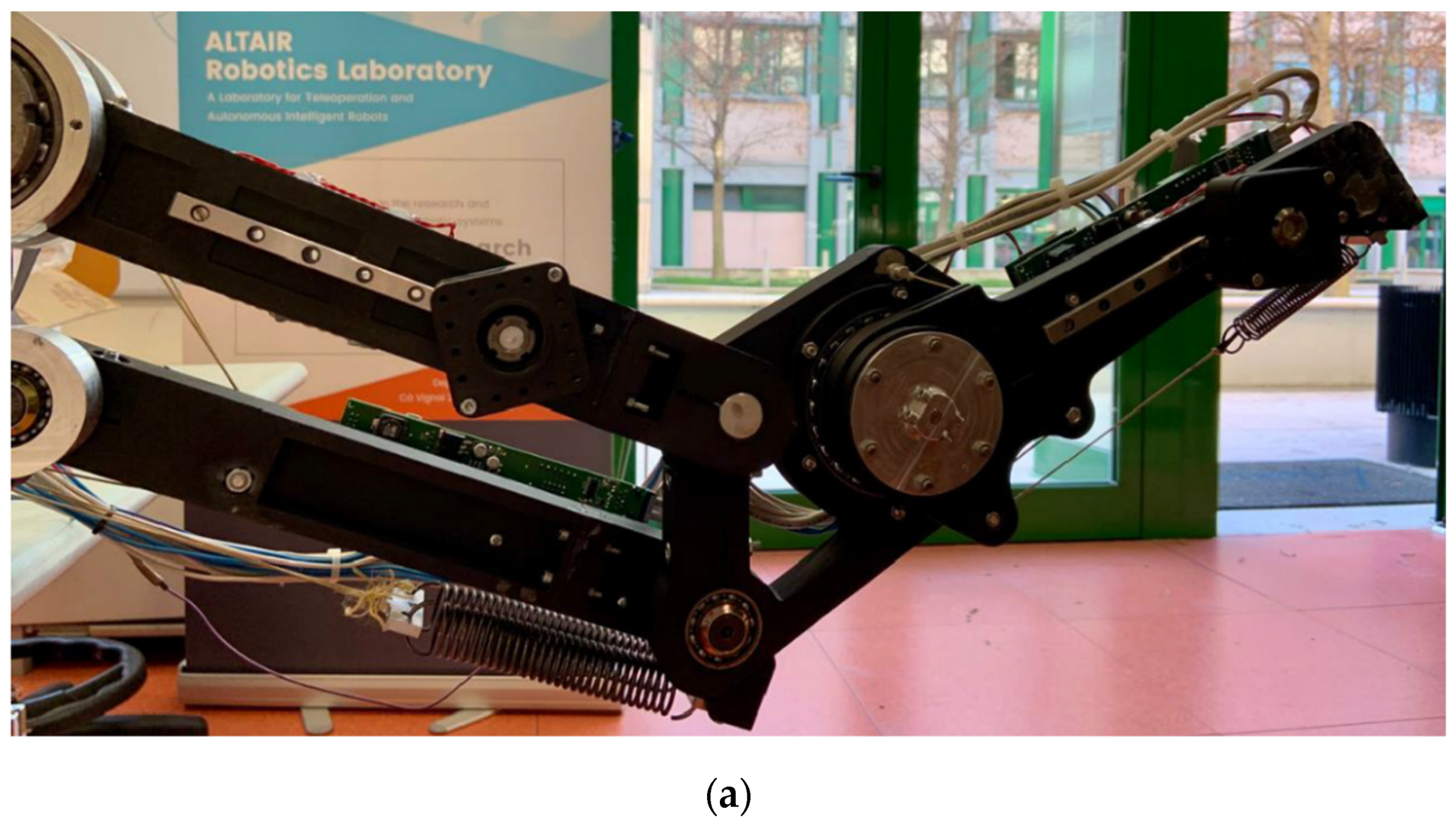
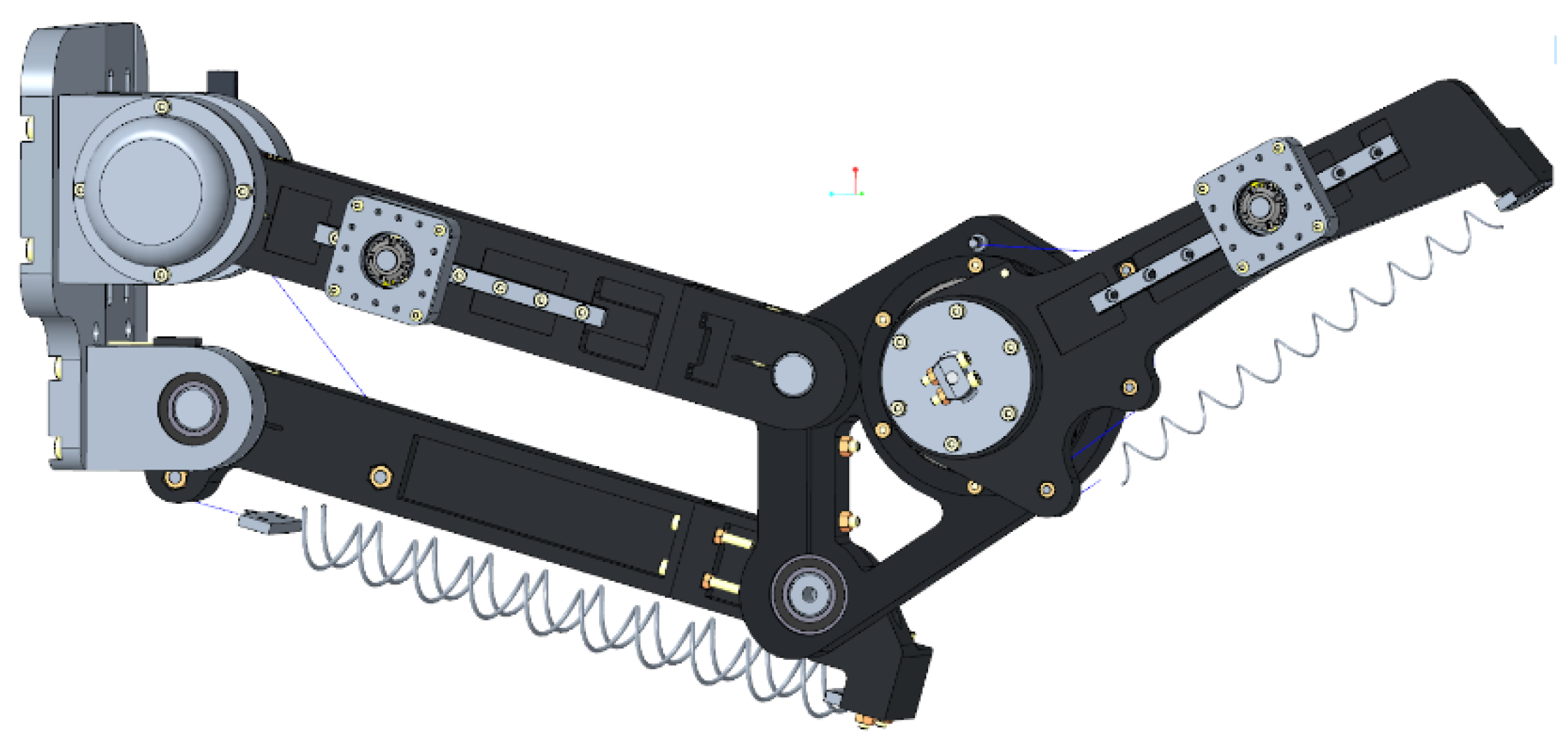
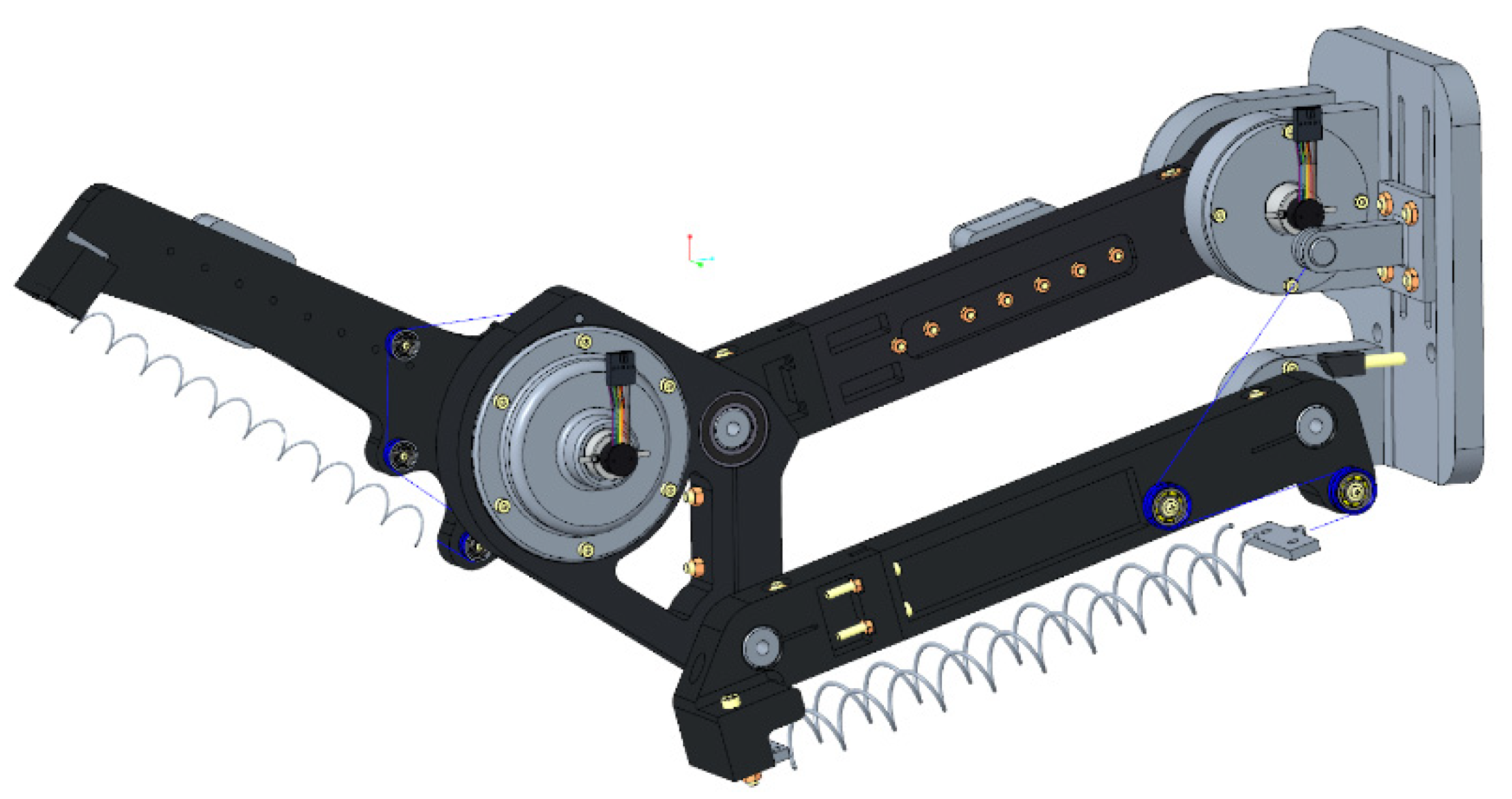
2.1. Mechanical Design and Manufacturing
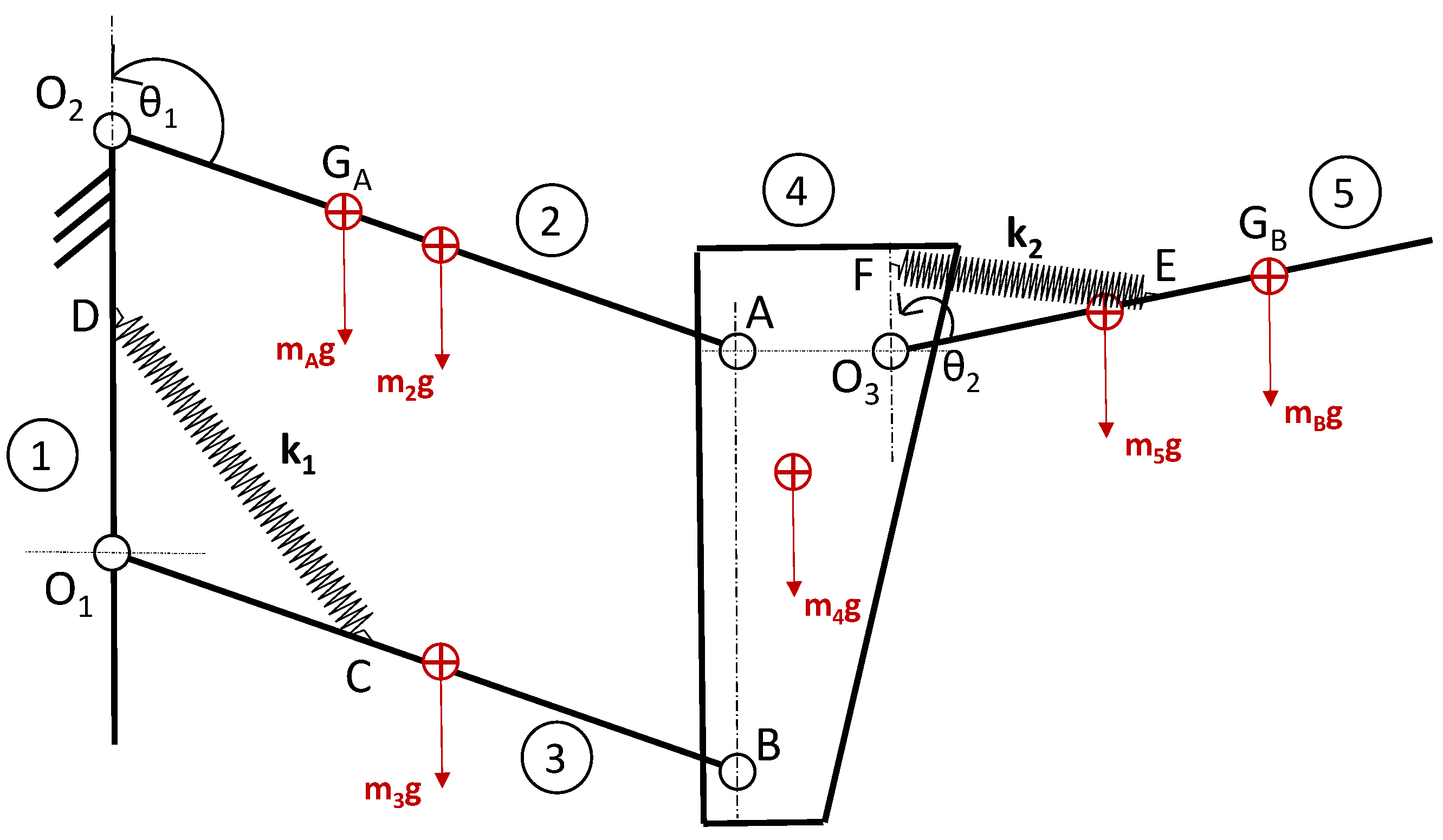
2.2. Gravity Balance Compensation
- Shoulder joint: Maxon Motor EC-90 flat (323772) with a 1:50 reducer, e.g., NLHSG-I 17–50;
- Elbow joint: Maxon Motor EC-45 flat (397172) with a 1:50 reducer, e.g., NLHSG-I 14–50.
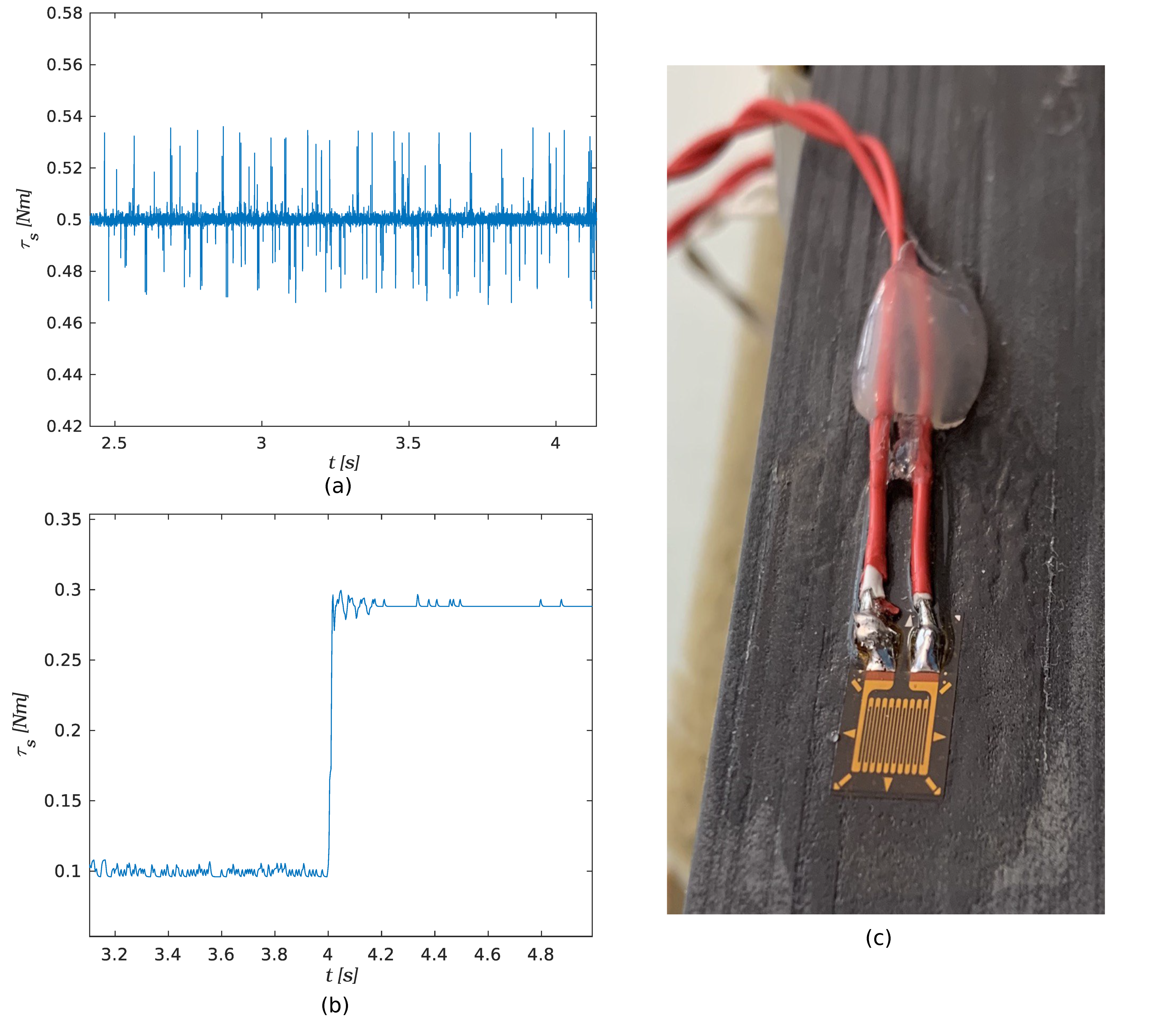
2.3. Electronics and Sensing
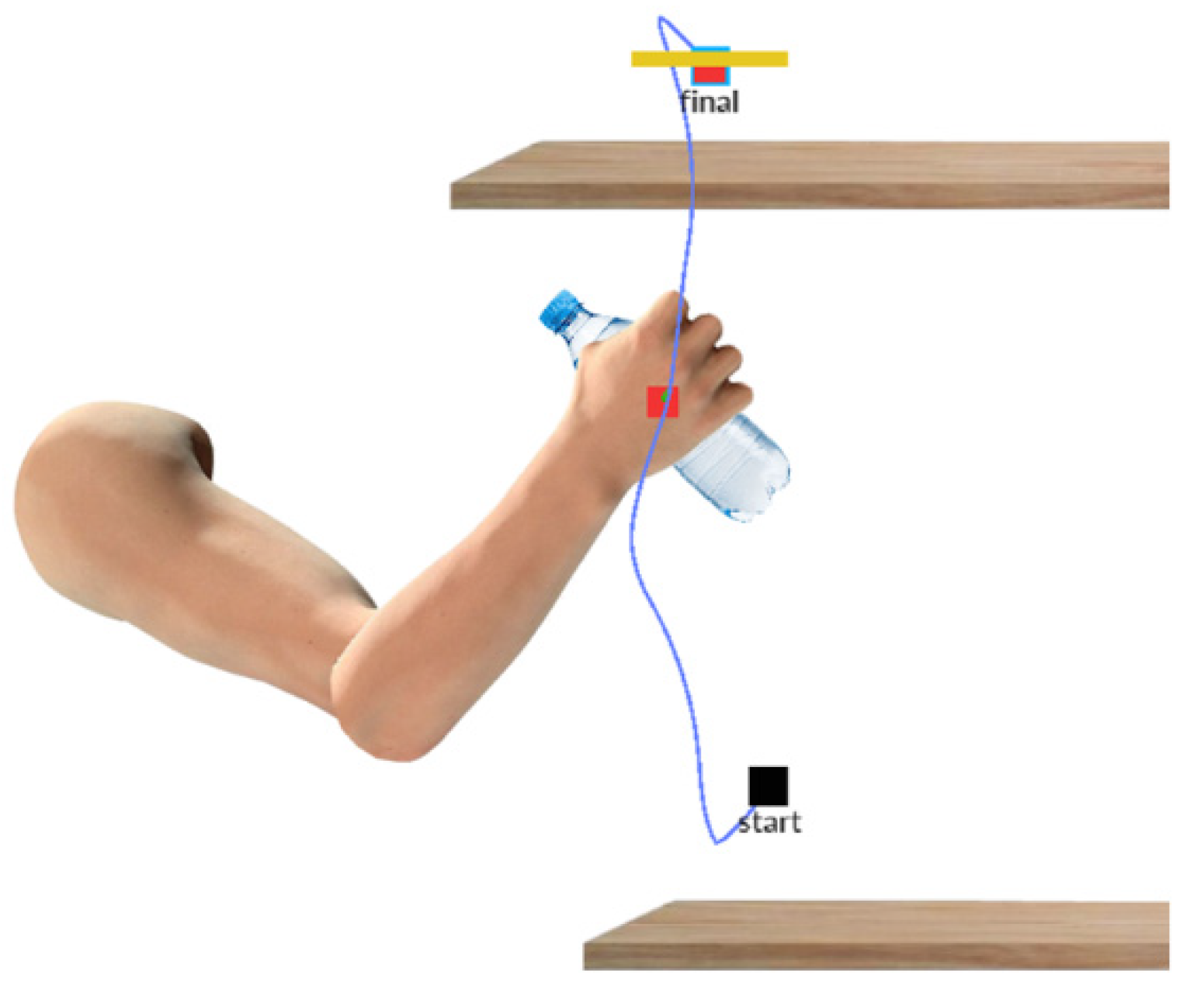
2.4. Rehabilitation Features
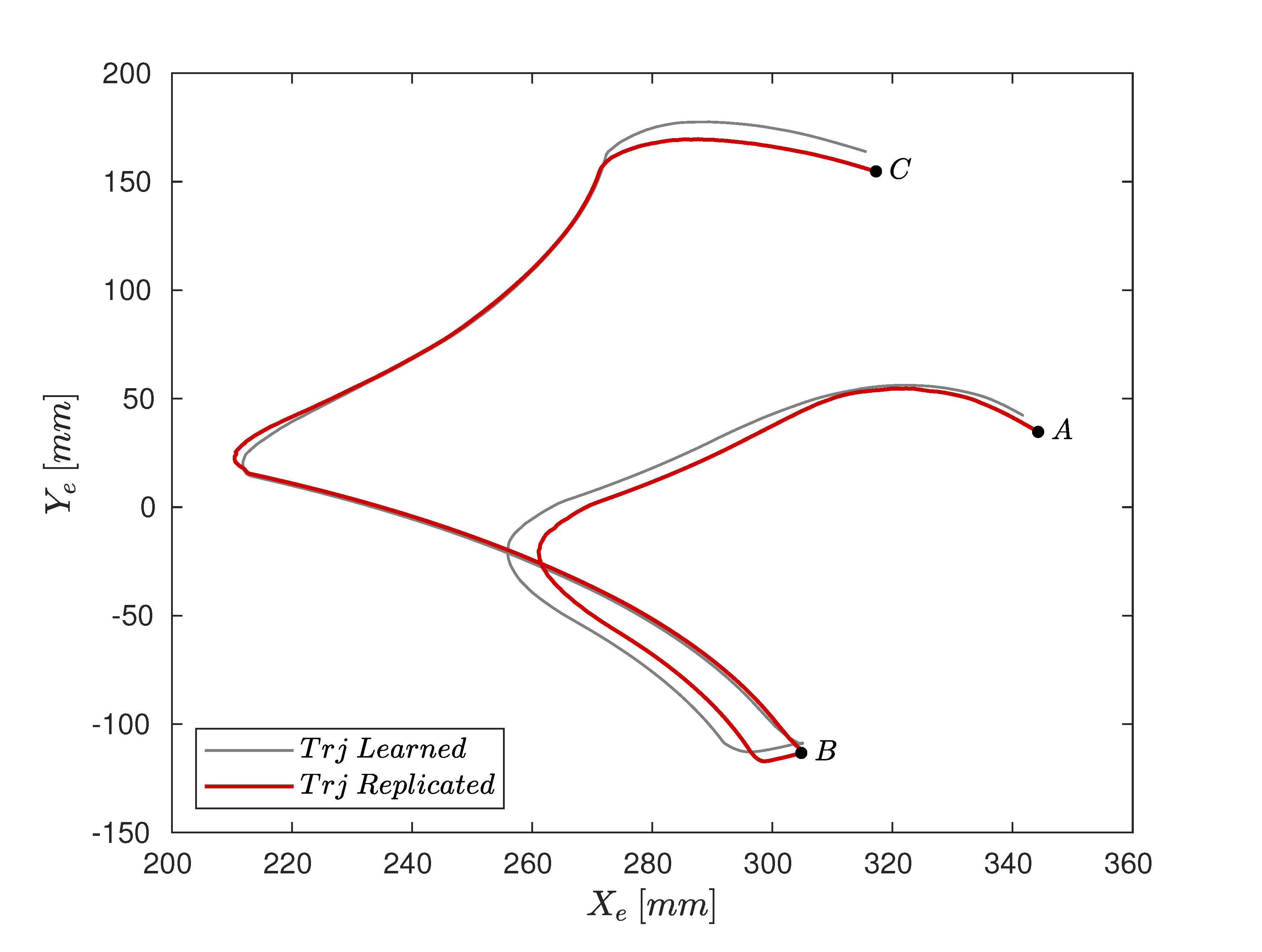
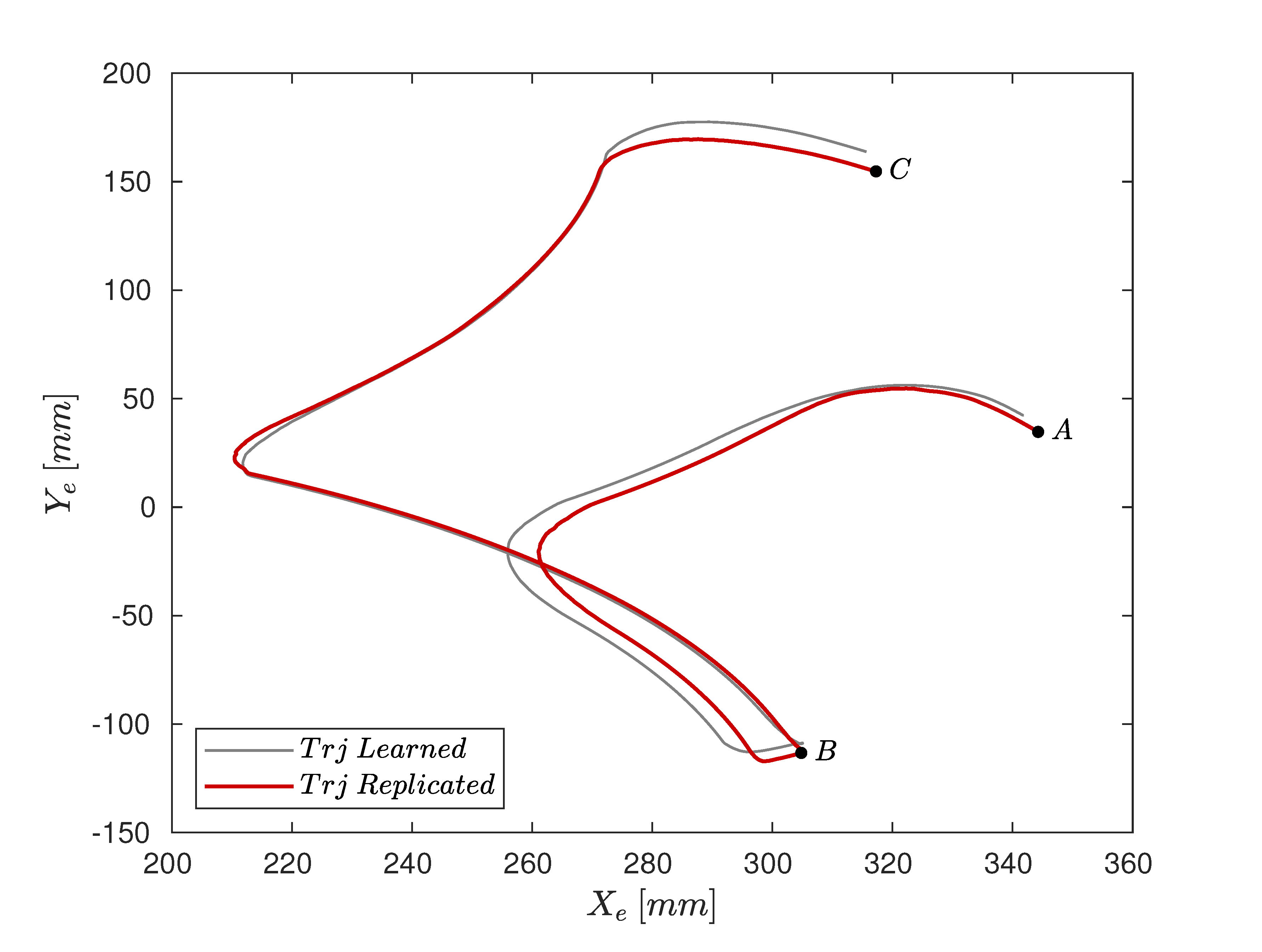
3. Experimental Results
4. Discussion
- The actual inertial parameters of human limbs;
- Bearings and motor friction;
- The inherent hysteresis of the spring behavior;
- Cable elasticity.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, S.; Nussbaum, M.A.; Esfahani, M.I.M.; Alemi, M.M.; Jia, B.; Rashedi, E. Assessing the influence of a passive, upper extremity exoskeletal vest for tasks requiring arm elevation: Part II–“Unexpected” effects on shoulder motion, balance, and spine loading. Appl. Ergon. 2018, 70, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Carmeli, E.; Peleg, S.; Bartur, G.; Elbo, E.; Vatine, J.-J. HandTutorTM enhanced hand rehabilitation after stroke—A pilot study. Physiother. Res. Int. 2011, 16, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, M.; Ingvast, J.; Wikander, J.; von Holst, H. The Soft Extra Muscle system for improving the grasping capability in neurological rehabilitation. In Proceedings of the 2012 IEEE-EMBS Conference on Biomedical Engineering and Sciences, Langkawi, Malaysia, 17–19 December 2012. [Google Scholar] [CrossRef]
- Bianchi, M.; Fanelli, F.; Conti, R.; Governi, L.; Meli, E.; Ridolfi, A.; Rindi, A.; Vannetti, F.; Allotta, B. Design and Motion Analysis of a Wearable and Portable Hand Exoskeleton. Biosyst. Biorobotics 2016, 16, 373–377. [Google Scholar] [CrossRef]
- Kim, B.; Deshpande, A.D. An upper-body rehabilitation exoskeleton Harmony with an anatomical shoulder mechanism: Design, modeling, control, and performance evaluation. Int. J. Robot. Res. 2017, 36, 414–435. [Google Scholar] [CrossRef]
- Christensen, S.; Bai, S. Kinematic Analysis and Design of a Novel Shoulder Exoskeleton Using a Double Parallelogram Linkage. J. Mech. Robot. 2018, 10, 041008. [Google Scholar] [CrossRef]
- Bütefisch, C.; Hummelsheim, H.; Denzler, P.; Mauritz, K.-H. Repetitive training of isolated movements improves the outcome of motor rehabilitation of the centrally paretic hand. J. Neurol. Sci. 1995, 130, 59–68. [Google Scholar] [CrossRef]
- Feys, H.M.; De Weerdt, W.J.; Selz, B.E.; Steck, G.A.C.; Spichiger, R.; Vereeck, L.; Putman, K.; Van Hoydonck, G.A. Effect of a Therapeutic Intervention for the Hemiplegic Upper Limb in the Acute Phase After Stroke. Stroke 1998, 29, 785–792. [Google Scholar] [CrossRef]
- Van Der Lee, J.H.; Wagenaar, R.C.; Lankhorst, G.J.; Vogelaar, T.W.; Devillé, W.L.; Bouter, L. Forced use of the upper extremity in chronic stroke patients: Results from a single-blind randomized clinical trial. Stroke 1999, 30, 2369–2375. [Google Scholar] [CrossRef]
- Barreca, S.; Wolf, S.L.; Fasoli, S.; Bohannon, R. Treatment Interventions for the Paretic Upper Limb of Stroke Survivors: A Critical Review. Neurorehabilit. Neural Repair 2003, 17, 220–226. [Google Scholar] [CrossRef]
- Frisoli, A.; Salsedo, F.; Bergamasco, M.; Rossi, B.; Carboncini, M.C. A force-feedback exoskeleton for upper-limb rehabilitation in virtual reality. Appl. Bionics Biomech. 2009, 6, 115–126. [Google Scholar] [CrossRef] [Green Version]
- Tsagarakis, N.; Caldwell, D.G. Development and Control of a ‘Soft-Actuated’ Exoskeleton for Use in Physiotherapy and Training. Auton. Robot. 2003, 15, 21–33. [Google Scholar] [CrossRef]
- Nef, T.; Riener, R. ARMin-Design of a Novel Arm Rehabilitation Robot. In Proceedings of the 2005 IEEE 9th International Conference on Rehabilitation Robotics, Chicago, IL, USA, 28 June–1 July 2005; Volume 2005. [Google Scholar] [CrossRef]
- Perry, J.C.; Rosen, J.; Burns, S. Upper-Limb Powered Exoskeleton Design. IEEE/ASME Trans. Mechatron. 2007, 12, 408–417. [Google Scholar] [CrossRef]
- Carignan, C.R.; Naylor, M.P.; Roderick, S.N. Controlling shoulder impedance in a rehabilitation arm exoskeleton. In Proceedings of the 2008 IEEE International Conference on Robotics and Automation, Pasadena, CA, USA, 19–23 May 2008. [Google Scholar] [CrossRef]
- Reinkensmeyer, D.J.; Kahn, L.E.; Averbuch, M.; McKenna-Cole, A.; Schmit, B.D.; Rymer, W.Z. Understanding and treating arm movement impairment after chronic brain injury: Progress with the ARM guide. J. Rehabil. Res. Dev. 2000, 37, 653–662. [Google Scholar] [PubMed]
- Jack, D.; Boian, R.; Merians, A.; Tremaine, M.; Burdea, G.; Adamovich, S.; Recce, M.; Poizner, H. Virtual reality-enhanced stroke rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2001, 9, 308–318. [Google Scholar] [CrossRef] [PubMed]
- Stewart, J.; Yeh, S.-C.; Jung, Y.; Yoon, H.; Whitford, M.; Chen, S.-Y.; Li, L.; McLaughlin, M.; Rizzo, A.; Winstein, C. Pilot Trial Results from a Virtual Reality System Designed to Enhance Recovery of Skilled Arm and Hand Movements after Stroke. In Proceedings of the 2006 International Workshop on Virtual Rehabilitation, New York, NY, USA, 29–30 August 2006. [Google Scholar] [CrossRef]
- Cardoso, L.; Da Costa, R.; Piovesana, A.; Costa, M.; Penna, L.; Crispin, A.; Carvalho, J.; Ferreira, H.; Lopes, M.; Brandao, G.; et al. Using Virtual Environments for Stroke Rehabilitation. Phys. Med. Rehabil. Clin. N. Am. 2006, 1–5. [Google Scholar] [CrossRef]
- Gull, M.A.; Bai, S.; Bak, T. A Review on Design of Upper Limb Exoskeletons. Robotics 2020, 9, 16. [Google Scholar] [CrossRef] [Green Version]
- Maciejasz, P.; Eschweiler, J.; Gerlach-Hahn, K.; Jansen-Troy, A.; Leonhardt, S. A survey on robotic devices for upper limb rehabilitation. J. Neuroeng. Rehabilitation 2014, 11, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krebs, H.I.; Hogan, N.; Aisen, M.L.; Volpe, B.T. Robot-aided neurorehabilitation. IEEE Trans. Rehabil. Eng. 1998, 6, 75–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoone, M.; van Os, P.; Campagne, A. Robot-mediated Active Rehabilitation (ACRE) A user trial. In Proceedings of the 2007 IEEE 10th International Conference on Rehabilitation Robotics, Noordwijk, The Netherlands, 13–15 June 2007. [Google Scholar] [CrossRef]
- Spencer, S.J.; Klein, J.; Minakata, K.; Le, V.; Bobrow, J.E.; Reinkensmeyer, D.J. A low cost parallel robot and trajectory optimization method for wrist and forearm rehabilitation using the Wii. In Proceedings of the 2008 2nd IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics, Scottsdale, AZ, USA, 19–22 October 2008. [Google Scholar] [CrossRef]
- Krebs, H.I.; Ferraro, M.; Buerger, S.P.; Newbery, M.J.; Makiyama, A.; Sandmann, M.; Lynch, D.; Volpe, B.T.; Hogan, N. Rehabilitation robotics: Pilot trial of a spatial extension for MIT-Manus. J. Neuroeng. Rehabil. 2004, 1, 5. [Google Scholar] [CrossRef] [Green Version]
- Rosati, G.; Gallina, P.; Masiero, S. Design, Implementation and Clinical Tests of a Wire-Based Robot for Neurorehabilitation. IEEE Trans. Neural Syst. Rehabilitation Eng. 2007, 15, 560–569. [Google Scholar] [CrossRef] [PubMed]
- Beer, R.F.; Naujokas, C.; Bachrach, B.; Mayhew, D. Development and evaluation of a gravity compensated training environment for robotic rehabilitation of post-stroke reaching. In Proceedings of the 2008 2nd IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics, Scottsdale, AZ, USA, 19–22 October 2008. [Google Scholar] [CrossRef]
- Bessler, J.; Prange-Lasonder, G.B.; Schaake, L.; Saenz, J.F.; Bidard, C.; Fassi, I.; Valori, M.; Lassen, A.B.; Buurke, J.H. Safety Assessment of Rehabilitation Robots: A Review Identifying Safety Skills and Current Knowledge Gaps. Front. Robot. AI 2021, 8. [Google Scholar] [CrossRef] [PubMed]
- Calanca, A.; Dimo, E.; Palazzi, E.; Ferro, R.; Vicario, R.; Murr, N.; Meneghetti, M.; Costanzi, D.; Luzi, L.; Vertechy, R.; et al. Toward Personal Affordable Exoskeletons with Force Control Capabilities. In Proceedings of the 14th PErvasive Technologies Related to Assistive Environments Conference, Corfu, Greece, 29 June 2021. [Google Scholar] [CrossRef]
- Park, J.-H.; Lee, K.-S.; Jeon, K.-H.; Kim, D.-H.; Park, H.-S. Low cost and light-weight multi-DOF exoskeleton for comprehensive upper limb rehabilitation. In Proceedings of the 2014 11th International Conference on Ubiquitous Robots and Ambient Intelligence (URAI), Kuala Lumpur, Malaysia, 12–15 November 2014; pp. 138–139. [Google Scholar] [CrossRef]
- Atia, M.G.B.; Salah, O.; Medhat, B.; Ibrahim, K. Design and analysis of low cost upper limb exoskeleton. In Proceedings of the 2017 12th International Conference on Computer Engineering and Systems (ICCES), Cairo, Egypt, 19–20 December 2017; pp. 80–84. [Google Scholar]
- Lenzo, B.; Bergamasco, M.; Salsedo, F. An Exoskeleton Structure for Physical Interaction with a Human Being; University of Surrey: Guildford, UK, 2015. [Google Scholar]
- Hsieh, H.-C.; Chen, D.-F.; Chien, L.; Lan, C.-C. Design of a Parallel Actuated Exoskeleton for Adaptive and Safe Robotic Shoulder Rehabilitation. IEEE/ASME Trans. Mechatron. 2017, 22, 2034–2045. [Google Scholar] [CrossRef]
- Hunt, J.; Lee, H.; Artemiadis, P. A Novel Shoulder Exoskeleton Robot Using Parallel Actuation and a Passive Slip Interface. J. Mech. Robot. 2017, 9, 011002. [Google Scholar] [CrossRef]
- Lenzi, T.; De Rossi, S.; Vitiello, N.; Chiri, A.; Roccella, S.; Giovacchini, F.; Vecchi, F.; Carrozza, M.C. The neuro-robotics paradigm: NEURARM, NEUROExos, HANDEXOS. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009. [Google Scholar] [CrossRef]
- Oguntosin, V.W.; Mori, Y.; Kim, H.; Nasuto, S.J.; Kawamura, S.; Hayashi, Y. Design and Validation of Exoskeleton Actuated by Soft Modules toward Neurorehabilitation—Vision-Based Control for Precise Reaching Motion of Upper Limb. Front. Neurosci. 2017, 11, 352. [Google Scholar] [CrossRef] [Green Version]
- Wu, Q.; Wang, X.; Du, F. Development and analysis of a gravity-balanced exoskeleton for active rehabilitation training of upper limb. Proc. Inst. Mech. Eng. Part C J. Mech. Eng. Sci. 2016, 230, 3777–3790. [Google Scholar] [CrossRef]
- Gopura, R.; Bandara, D.; Kiguchi, K.; Mann, G. Developments in hardware systems of active upper-limb exoskeleton robots: A review. Robot. Auton. Syst. 2016, 75, 203–220. [Google Scholar] [CrossRef]
- Gopura, R.A.R.C.; Kiguchi, K. Mechanical designs of active upper-limb exoskeleton robots: State-of-the-art and design difficulties. In Proceedings of the 2009 IEEE International Conference on Rehabilitation Robotics, Kyoto, Japan, 23–26 June 2009. [Google Scholar] [CrossRef]
- Proietti, T.; Crocher, V.; Roby-Brami, A.; Jarrasse, N. Upper-Limb Robotic Exoskeletons for Neurorehabilitation: A Review on Control Strategies. IEEE Rev. Biomed. Eng. 2016, 9, 4–14. [Google Scholar] [CrossRef] [Green Version]
- Lo, H.S.; Xie, S.Q. Exoskeleton robots for upper-limb rehabilitation: State of the art and future prospects. Med. Eng. Phys. 2012, 34, 261–268. [Google Scholar] [CrossRef]
- Toxiri, S.; Ortiz, J.; Masood, J.; Fernández, J.; Mateos, L.A.; Caldwell, D.G. A wearable device for reducing spinal loads during lifting tasks: Biomechanics and design concepts. In Proceedings of the 2015 IEEE International Conference on Robotics and Biomimetics (ROBIO), Zhuhai, China, 6–9 December 2015; pp. 2295–2300. [Google Scholar]
- Available online: https://harmonicdrive.de (accessed on 5 January 2022).
- Toxiri, S.; Calanca, A.; Ortiz, J.; Fiorini, P.; Caldwell, D.G. A Parallel-Elastic Actuator for a Torque-Controlled Back-Support Exoskeleton. IEEE Robot. Autom. Lett. 2017, 3, 492–499. [Google Scholar] [CrossRef]
- Available online: https://blackberry.qnx.com (accessed on 5 January 2022).
- Available online: https://www.windriver.com/products/vxworks (accessed on 5 January 2022).
- Mertz, L. The Next Generation of Exoskeletons: Lighter, Cheaper Devices Are in the Works. IEEE Pulse 2012, 3, 56–61. [Google Scholar] [CrossRef]
- Hamill, J.; Knutzen, K.M. Biomechanical Basis of Human Movement; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2006. [Google Scholar]
- Hart, R.J.; Patton, E.G.; Sapunkov, O. Characterization of Continuous Fiber-Reinforced Composite Materials Manufactured via Fused Filament Fabrication; Army Tank Automotive Research Development and Engineering Center: Warren, MI, USA, 2018. [Google Scholar]
- Goh, G.D.; Dikshit, V.; Nagalingam, A.P.; Goh, G.L.; Agarwala, S.; Sing, S.L.; Wei, J.; Yeong, W.Y. Characterization of mechanical properties and fracture mode of additively manufactured carbon fiber and glass fiber reinforced thermoplastics. Mater. Des. 2018, 137, 79–89. [Google Scholar] [CrossRef]
- Dutra, T.A.; Ferreira, R.T.L.; Resende, H.B.; Guimarães, A. Mechanical characterization and asymptotic homogenization of 3D-printed continuous carbon fiber-reinforced thermoplastic. J. Braz. Soc. Mech. Sci. Eng. 2019, 41, 1–15. [Google Scholar] [CrossRef]
- Ghebretinsae, F.; Mikkelsen, O.; Akessa, A.D. Strength analysis of 3D printed carbon fibre reinforced thermoplastic using experimental and numerical methods. IOP Conf. Ser. Mater. Sci. Eng. 2019, 700, 012024. [Google Scholar] [CrossRef]
- Yu, T.; Zhang, Z.; Song, S.; Bai, Y.; Wu, D. Tensile and flexural behaviors of additively manufactured continuous carbon fiber-reinforced polymer composites. Compos. Struct. 2019, 225, 111147. [Google Scholar] [CrossRef]
- Blok, L.G.; Longana, M.L.; Yu, H.; Woods, B.K.S. An investigation into 3D printing of fibre reinforced thermoplastic composites. Addit. Manuf. 2018, 22, 176–186. [Google Scholar] [CrossRef]
- Luzi, L.; Quercioli, G.; Pucci, R.; Bocchieri, G.; Vertechy, R.; Berselli, G. Additively Manufactured Continuous Fibre-Reinforced Thermoplastics for Mechanisms Subjected to Predominant Inertial Load: A Case Study. In Proceedings of the ASME 2020 Conference on Smart Materials, Adaptive Structures and Intelligent Systems, Virtual, Online, 15 September 2020. [Google Scholar] [CrossRef]
- Herder, J.L. Energy-Free Systems. Theory, Conception and Design of Statically Balanced Spring Mechanisms. Ph.D. Thesis, Delft University of Technology, Delft, The Netherlands, November 2001. [Google Scholar]
- Calanca, A.; Muradore, R.; Fiorini, P. A Review of Algorithms for Compliant Control of Stiff and Fixed-Compliance Robots. IEEE/ASME Trans. Mechatronics 2016, 21, 613–624. [Google Scholar] [CrossRef]
- Ginesi, M.; Sansonetto, N.; Fiorini, P. Overcoming some drawbacks of Dynamic Movement Primitives. Robot. Auton. Syst. 2021, 144, 103844. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Link | Length (mm) | Mass (kg) |
|---|---|---|
| 1 | 100 | - |
| 2 | 300 | 0.52 |
| 3 | 300 | 0.6 |
| 4 | - | 1.3 |
| O3A | 80 | - |
| 5 | 270 | 0.52 |
| Mechanical Properties | Onyx | CFRO |
|---|---|---|
| ρ | 1180 kg/m3 | 1400 kg/m3 1 |
| σt | 36 MPa | 986 MPa 2 |
| E | 1.4 GPa | 62.5 GPa 2 |
| σf | 81 MPa | 485 MPa 2 |
| Ef | 2.9 GPa | 41.6 GPa 2 |
| Human Parameters | |
|---|---|
| MA | 0.7 kg |
| MB | 0.8 kg |
| rA | 150 mm |
| rB | 150 mm |
| Parameters | Opt. Values (mm) |
|---|---|
| c | 85 |
| d | 85 |
| e | 80 |
| f | 60 |
| Torque Values | BMS (Nm) | UMS (Nm) | Reduction (%) |
|---|---|---|---|
| Peak at shoulder | 0.679 | 14.147 | 95 |
| Peak at elbow | 1.160 | 2.741 | 57 |
| Torque Values | BMS (Nm) | UMS (Nm) | Reduction (%) |
|---|---|---|---|
| Peak at shoulder | 1.194 | 11.603 | 89 |
| Peak at elbow | 0.304 | 1.979 | 84 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palazzi, E.; Luzi, L.; Dimo, E.; Meneghetti, M.; Vicario, R.; Luzia, R.F.; Vertechy, R.; Calanca, A. An Affordable Upper-Limb Exoskeleton Concept for Rehabilitation Applications. Technologies 2022, 10, 22. https://doi.org/10.3390/technologies10010022
Palazzi E, Luzi L, Dimo E, Meneghetti M, Vicario R, Luzia RF, Vertechy R, Calanca A. An Affordable Upper-Limb Exoskeleton Concept for Rehabilitation Applications. Technologies. 2022; 10(1):22. https://doi.org/10.3390/technologies10010022
Chicago/Turabian StylePalazzi, Emanuele, Luca Luzi, Eldison Dimo, Matteo Meneghetti, Rudy Vicario, Rafael Ferro Luzia, Rocco Vertechy, and Andrea Calanca. 2022. "An Affordable Upper-Limb Exoskeleton Concept for Rehabilitation Applications" Technologies 10, no. 1: 22. https://doi.org/10.3390/technologies10010022
APA StylePalazzi, E., Luzi, L., Dimo, E., Meneghetti, M., Vicario, R., Luzia, R. F., Vertechy, R., & Calanca, A. (2022). An Affordable Upper-Limb Exoskeleton Concept for Rehabilitation Applications. Technologies, 10(1), 22. https://doi.org/10.3390/technologies10010022