
The Secondary Use of Data to Support Medication Safety in the Hospital Setting: A Systematic Review and Narrative Synthesis


Abstract
1. Introduction
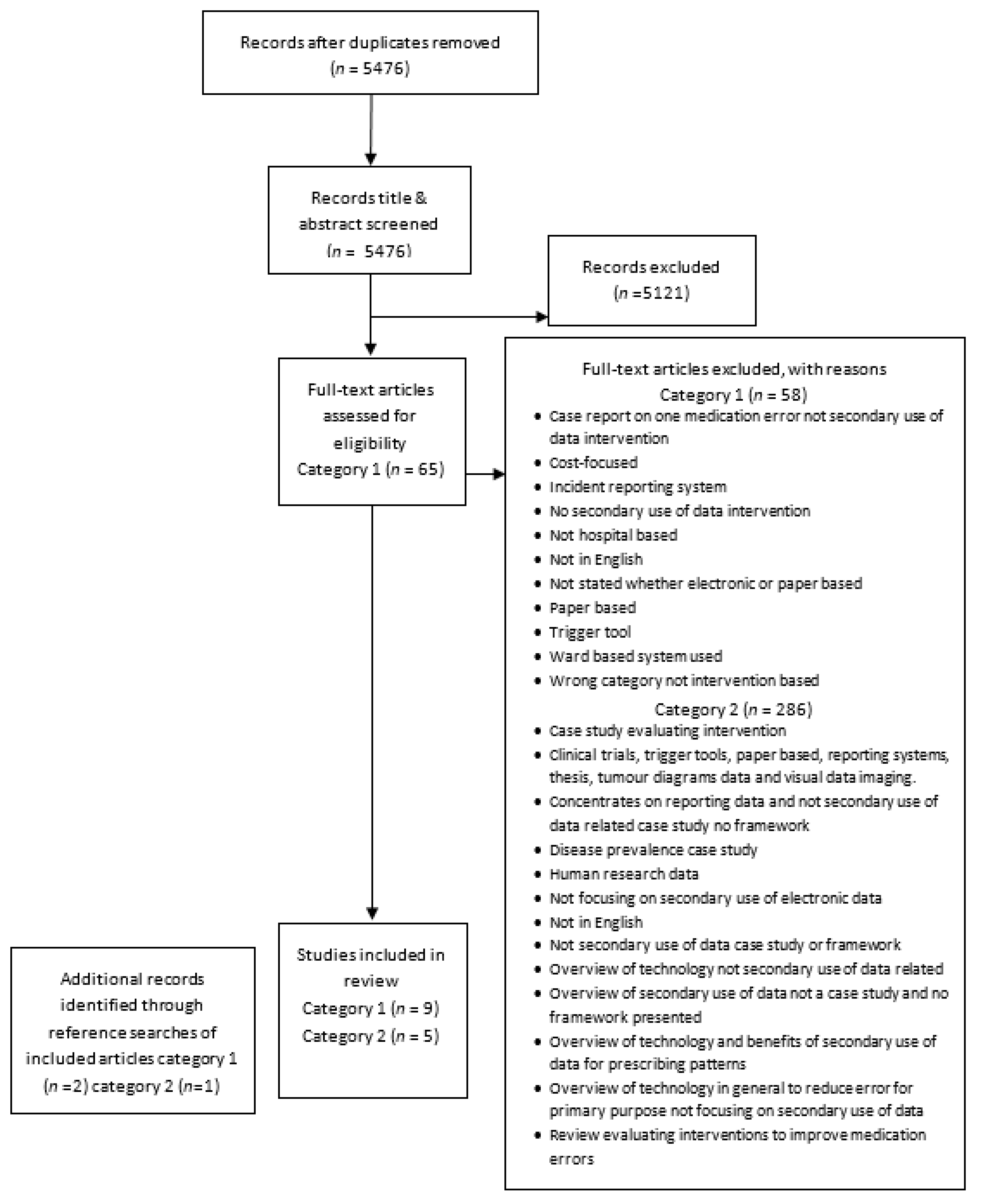
2. Materials and Methods
2.1. Search Strategy
2.2. Definitions
- ‘Secondary use of electronic prescribing/pharmacy data’: the reuse of clinical and/or operational data from an EP or EHP system for purposes other than direct patient care or the original purpose for which the data were used.
- ‘Intervention based on secondary use of electronic prescribing/pharmacy data’ (‘SUD intervention’): The reuse of the data from an EP or EHP system for secondary purpose(s) with the intent of changing or improving a process, either alone or in combination with other intervention(s). The actual implementation of an electronic system was not considered an intervention in this context.
2.3. Study Selection
2.4. Screening Process, Data Extraction, and Analysis
3. Results
3.1. Overview of Included Literature
3.2. Definitions of SUD Employed in the Literature

{kind=link}
{kind=link}
| Author(s) | Title | Country | Type of Study: | Factors to Consider When Reusing Data: |
|---|---|---|---|---|
| Bain et al., 1997 [3] | Routinely collected data in national and regional databases—an under-used resource | UK | Narrative literature review | Consists of 5 main stages to consider:
|
| Danciu et al., 2014 [34] | Secondary use of clinical data: The Vanderbilt approach | USA | Reflection on a case study | 9 factors to consider:
|
| Galster, 2012 [35] | Why is clinical information not reused? | Denmark | Systematic literature review | 4 major barriers identified resulting in lack of clinical data reuse:
|
| Holzer and Gall, 2011 [36] | Utilizing IHE-based [Integrating the Healthcare Enterprise] Electronic Health Record Systems for Secondary use | Austria | Systematic literature review | Requirements for secondary use of data from electronic health records:
|
| Safran et al., 2007 [33] | Toward a national framework for the secondary use of health data | USA | Qualitative work—discussion between experts. | 5 recommendations:
|
3.3. Interventions Based on SUD in Hospitals (Interventional Studies)
3.3.1. Types of EP Systems and the Data Used
3.3.2. Types of Intervention Based on Secondary Use of Data
3.3.3. Secondary Users of Electronic Data
3.3.4. Effectiveness of Secondary Use Interventions
3.3.5. Limitations of Included Studies
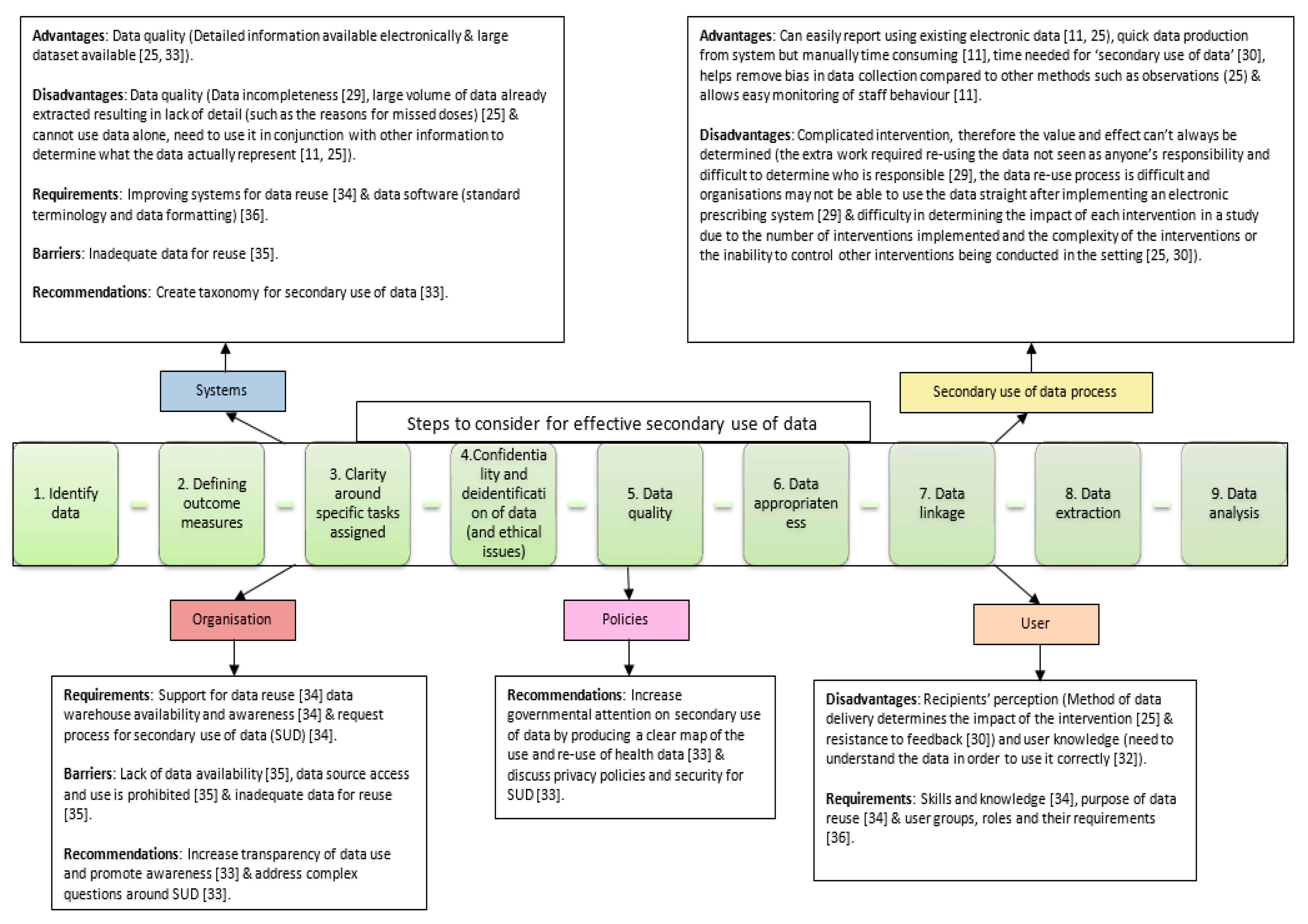
3.4. Factors Influencing Secondary Use of Data in Healthcare (Interventional and Non-Interventional Studies)
4. Discussion
4.1. Summary of Main Findings
4.2. Comparison to Previous Literature
4.3. Implications for Practice
4.4. Implications for Research
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bradley, E.H.; Holmboe, E.S.; A Mattera, J.; A Roumanis, S.; Radford, M.; Krumholz, H.M. Data feedback efforts in quality improvement: Lessons learned from US hospitals. Qual. Saf. Health Care 2004, 13, 26–31. [Google Scholar] [CrossRef]
- Department Of Health. Health and Social Care Information Centre: Collecting Data. Department Of Health, 2013. Available online: http://www.hscic.gov.uk/datasets (accessed on 10 January 2014).
- Bain, M.R.S.; Chalmers, J.W.T.; Brewster, D.H. Routinely collected data in national and regional databases—An under-used resource. J. Public Health Med. 1997, 19, 413–418. [Google Scholar] [CrossRef]
- Lowrance, W. Learning from experience: Privacy and the secondary use of data in health research. J. Health Serv. Res. Policy 2003, 8 (Suppl. 1), 2–7. [Google Scholar] [CrossRef] [PubMed]
- Safran, C. Reuse of clinical data. Yearb. Med. Inf. 2014, 9, 52–54. [Google Scholar] [CrossRef][Green Version]
- van der Veer, S.N.; de Keizer, N.F.; Ravelli, A.C.; Tenkink, S.; Jager, K.J. Improving quality of care. A systematic review on how medical registries provide information feedback to health care providers. Int. J. Med. Inform. 2010, 79, 305–323. [Google Scholar]
- PricewaterhouseCoopers. Transforming healthcare through secondary use of health data. Dallas PriceWaterhouseCoopers 2009, 1–40. [Google Scholar]
- Suffolk Mental Health Partnership NHS Trust. Access to Patient Identifiable Data for Secondary Use Policy. Policy. Suffolk Mental Health Partnership NHS Trust, UK, 2011 28/03/2011. Available online: https://www.nsft.nhs.uk/ (accessed on 7 August 2015).
- Hyppönen, H.; Saranto, K.; Vuokko, R.; Mäkelä-Bengs, P.; Doupi, P.; Lindqvist, M.; Mäkelä, M. Impacts of structuring the electronic health record: A systematic review protocol and results of previous reviews. Int. J. Med. Inform. 2014, 83, 159–169. [Google Scholar] [CrossRef] [PubMed]
- de Bruin, J.S.; Seeling, W.; Schuh, C. Data use and effectiveness in electronic surveillance of healthcare associated infections in the 21st century: A systematic review. J. Am. Med Inform. Assoc. 2014, 21, 942–951. [Google Scholar] [CrossRef] [PubMed]
- Dixon-Woods, M.; Redwood, S.; Leslie, M.; Minion, J.; Martin, G.P.; Coleman, J.J. Improving quality and safety of care using technovigilance: An ethnographic case study of secondary use of data from an electronic prescribing and decision support system. Milbank Q. 2013, 91, 424–454. [Google Scholar] [CrossRef] [PubMed]
- Teich, J.M.; Merchia, P.R.; Schmiz, J.L.; Kuperman, G.J.; Spurr, C.D.; Bates, D.W. Effects of computerized physician order entry on prescribing practices. Arch. Intern. Med. 2000, 160, 2741–2747. [Google Scholar] [CrossRef]
- Barcoding Inc. Barcoding in Hospitals, Heath Care Systems, and Pharmacy 2015. Available online: http://www.barcoding.com/hospital-acute-care-facility-data-capture-solutions.shtml (accessed on 7 August 2015).
- Cummings, K. “Smart” Infusion Pumps Are Selectively Intelligent FDA.gov 2015. Available online: http://www.fda.gov/MedicalDevices/Safety/AlertsandNotices/TipsandArticlesonDeviceSafety/ucm245160.htm (accessed on 7 August 2015).
- Balogun, A. Safer Care Trigger Tools—NHS Institute for Innovation and Improvement Institute.nhs.uk 2015. Available online: http://www.institute.nhs.uk/safer_care/safer_care/trigger_tool_portal.html (accessed on 7 August 2015).
- Health Quality & Safety Commission. Global Trigger Tools: A Review of the Evidence; Institute of Healthcare Improvement: Wellington, New Zealand, 2013. [Google Scholar]
- Ohashi, K.; Dalleur, O.; Dykes, P.C.; Bates, D.W. Benefits and risks of using smart pumps to reduce medication error rates: A systematic review. Drug Saf. 2014, 37, 1011–1020. [Google Scholar] [CrossRef] [PubMed]
- Voshall, B.; Piscotty, R.; Lawrence, J.; Targosz, M. Barcode medication administration work-arounds: A systematic review and implications for nurse executives. J. Nurs. Adm. 2013, 43, 530–535. [Google Scholar] [CrossRef]
- Uman, L. Systematic reviews and meta-analyses. J. Can. Acad. Child Adolesc. Psychiatry 2011, 20, 57–59. [Google Scholar]
- Popay, J.; Roberts, H.; Sowden, A.; Petticrew, M.; Arai, L.; Rodgers, M.; Britten, N.; Roen, K.; Duffy, S. Guidance on the conduct of narrative synthesis in systematic reviews. In A Product from the ESRC Methods Programme; Institute of Health Research: Lancaster, UK, 2006. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Wong, G.; Greenhalgh, T.; Westhorp, G.; Buckingham, J.; Pawson, R. RAMESES publication standards: Meta-narrative reviews. BMC Med. 2013, 11, 20. [Google Scholar]
- Aslam, S.; Emmanuel, P. Formulating a researchable question: A critical step for facilitating good clinical research. Indian J. Sex. Transm. Dis. 2010, 31, 47–50. [Google Scholar] [CrossRef]
- Sim, I.; Gorman, P.; Greenes, R.A.; Haynes, R.B.; Kaplan, B.; Lehmann, H.; Tang, P.C. Clinical decision support systems for the practice of evidence-based medicine. J. Am. Med. Inf. Assoc. 2001, 8, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Coleman, J.J.; Hodson, J.; Brooks, H.L.; Rosser, D. Missed medication doses in hospitalised patients: A descriptive account of quality improvement measures and time series analysis. Int. J. Qual. Health Care 2013, 25, 564–572. [Google Scholar] [CrossRef]
- Coleman, J.J.; Hodson, J.; Ferner, R.E. Deriving dose limits for warnings in electronic prescribing systems: Statistical analysis of prescription data at university hospital Birmingham, UK. Drug Saf. 2012, 35, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Rosser, D.; Cowley, N.J.; Ray, D.; Nightingale, P.G.; Jones, T.; Moore, J.; Coleman, J.J. Quality improvement programme, focusing on error reduction: A single center naturalistic study. J. R. Soc. Med. Short Rep. 2012, 3, 1–7. [Google Scholar] [CrossRef]
- Griffith, D.N.W.; Robinson, M. Prescribing practice and policy for hypnotics: A model of pharmacy audit. Age Ageing 1996, 25, 490–492. [Google Scholar] [CrossRef][Green Version]
- Morrison, C.; Jones, M.; Jones, R.; Vuylsteke, A. ‘You can’t just hit a button’: An ethnographic study of strategies to repurpose data from advanced clinical information systems for clinical process improvement. BMC Med. 2013, 11, 1–8. [Google Scholar] [CrossRef]
- Sullivan, K.M.; Suh, S.; Monk, H.; Chuo, J. Personalised performance feedback reduces narcotic prescription errors in a NICU. BMJ Qual. Saf. 2013, 22, 256–262. [Google Scholar] [CrossRef][Green Version]
- Finnerty, M.; Altmansberger, R.; Bopp, J.; Carpinello, S.; Docherty, J.P.; Fisher, W.; Jensen, P.; Krishnan, P.; Mittleman, M.; Olfson, M.; et al. Using state administrative and pharmacy data bases to develop a clinical decision support tool for schizophrenia guidelines. Schizophr. Bull. 2002, 28, 85–94. [Google Scholar] [CrossRef][Green Version]
- Nelson, N.C.; Evans, R.S.; Samore, M.H.; Gardner, R.M. Detection and prevention of medication errors using real-time bedside nurse charting. J. Am. Med. Inform. Assoc. 2005, 12, 390–397. [Google Scholar] [CrossRef]
- Safran, C.; Bloomrosen, M.; Hammond, W.E.; Labkoff, S.; Markel-Fox, S.; Tang, P.C.; Detmer, D.E. Toward a national framework for the secondary use of health data: An American Medical Informatics Association White Paper. J. Am. Med Inform. Assoc. 2007, 14, 1–9. [Google Scholar] [CrossRef]
- Danciu, I.; Cowan, J.D.; Basford, M.; Wang, X.; Saip, A.; Osgood, S.; Shirey-Rice, J.; Kirby, J.; Harris, P.A. Secondary use of clinical data: The Vanderbilt approach. J. Biomed. Inform. 2014, 52, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Galster, G. Why is clinical information not reused? In Studies in Health Technology and Informatics; PMID: Aalborg, Denmark, 2012; Volume 180, pp. 624–628. [Google Scholar]
- Holzer, K.; Gall, W. Utilizing IHE-based Electronic Health Record systems for secondary use. Methods Inf. Med. 2011, 50, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Medical Research Council. Developing and Evaluating Complex Interventions: New Guidance; Medical Research Council: London, UK, 2006. [Google Scholar]
- El Emam, K.; Jonker, E.; Arbuckle, L.; Malin, B. A Systematic Review of Re-Identification Attacks on Health Data. PLoS ONE 2011, 6, e28071. [Google Scholar] [CrossRef] [PubMed]
- Weiskopf, N.G.; Hripcsak, G.; Swaminathan, S.; Weng, C. Defining and measuring completeness of electronic health records for secondary use. J. Biomed. Inform. 2013, 46, 830–836. [Google Scholar] [CrossRef]
- Weiskopf, N.G.; Weng, C. Methods and dimensions of electronic health record data quality assessment: Enabling reuse for clinical research. J. Am. Med. Inform. Assoc. 2013, 20, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.; Cresswell, K.; Mozaffar, H.; Sheikh, A. A systematic assessment of review to promoting the appropriate use of antibiotics through hospital electronic prescribing systems. Int. J. Pharm. Pract. 2016, 25, 5–17. [Google Scholar]
- Cornford, T.; Doukidis, G.; Forster, D. Experience with a Structure, Process and Outcome Framework for Evaluating an Information-System. Omega-Int. J. Manag. Sci. 1994, 22, 491–504. [Google Scholar] [CrossRef]
- Micallef, C.; Chaudhry, N.T.; Holmes, A.H.; Hopkins, S.; Benn, J.; Franklin, B.D. The secondary use of data from hospital electronic prescribing and pharmacy systems to support quality and safety of antimicrobial use: A systematic review. J. Antimicrob. Chemother. Submitt. Publ. October. 2017, 72, 1880–1885. [Google Scholar] [CrossRef] [PubMed]


| Search Strategy 1 | Search Strategy 2 | |
|---|---|---|
| Facets used | 3 facets: (a) electronic databases AND (b) medication safety AND (c) [hospital or (quality or safety)] | 1 facet: (Secondary$ us$ or reus$ or epurpose$) adj6 (data$ or information$ or record$) |
| Databases used for MeSH terms (date search conducted): | Excerpta Medical DataBASE (EMBASE) [15 August 2014], Medline [4 August 2014], and Cumulative Index to Nursing and Allied Health Literature (CINAHL) [4 August 2014]. | No MeSH terms used for search strategy 2 |
| Databases used for keywords (date search conducted): | EMBASE, Medline, IPA and CINAHL [19 March 2018]. | EMBASE, Medline, IPA, and CINAHL [19 March 2018]. |
| Search restriction criteria: | Title and abstract | Title search only |
| Filters applied (e.g., date, language, or publication type): | None | None |
| Author(s) and Reference | Country and Type of Hospital Setting | Aim(s) of Study and Study Design to Evaluate Secondary Use of Data (SUD) Intervention | Secondary Use of Data Intervention(s) | |||
|---|---|---|---|---|---|---|
| Electronic System(s) from Which Data Were Used for SUD Intervention and Types of Data Used for the Intervention(s) | Method of Applying Data in Practice i.e., Data Are Included in Intervention and Applied in Context. | Clinical Setting and End Users | Outcome Measure(s) for Evaluation | |||
| Coleman et al., 2012 [26] | UK—type of hospital not specified | Producing upper dose limits using existing data to reduce inappropriate prescribing. Quantitative study, formula testing using retrospective data analysis | Electronic prescribing system (system not specified). 100 most frequently used drugs that were prescribed more than 100 times. | Production of upper dose limits on the electronic prescribing system. | Clinical setting not specified End user: Piloted by clinical pharmacologists | Sensitivity and specificity of the limits applied to each medication and views of piloting clinical pharmacologists. From the 28 drug form combinations available, the 86th percentile of dose gave a mean sensitivity of 95.3% and mean specificity of 97.9%. |
| Coleman et al., 2013 [25] | UK—Large NHS Foundation Trust | To investigate the rates of overdue doses following the implementation of electronic prescribing. Quantitative Multi-intervention study, retrospective time series analysis of weekly dose administration data. | Electronic prescribing system (Prescribing information and communications systems [PICS]) and administrative data. Overdue medication doses. | Pause function for electronic prescribing implemented, clinical dashboards produced fed back live data to end users, visual indicators and care omission meetings (for feedback) and National Patient Safety Agency rapid response. | Clinical setting: Hospital wide End users: clinical staff and managers (including board members) | Omitted doses for antibiotics and non-antibiotics. Clinical dashboards: reductions of 0.60 (95% CI = 0.26, 0.95) and 0.41 percentage points (95% CI = 0.11, 0.70) Pausing prescriptions: 0.49 percentage points (95% CI = 0.18, 0.80) and -0.28 percentage points (95% CI = −0.50, −0.07) Executive-led overdue doses root cause analysis (RCA) meetings: reductions of 0.83 (95% CI = 0.50, 1.17) and 0.97 (95% CI = 0.61, 1.32) percentage points Visual indicator for overdue doses did not result in a significant decrease in missed antibiotics or non-antibiotic doses. |
| Dixon-Woods et al., 2013 [11] | UK—Large NHS acute care hospital. | To improve missed doses, measure performance and overall improve quality and safety. To define the use of electronic data to generate quality and safety interventions. Qualitative Ethnographic case study | Electronic prescribing system (Hospital electronic prescribing and decision support system: ePDSS). Missed medication doses, time taken from writing antibiotic prescription to administration of first dose, venous thromboembolism risk assessment completion rates, completion of clinical observations, rates of specific infections. | The raw data from ePDSS were used with regular feedback to clinical teams (with improvement suggestions when needed via conversations, emails and meetings), dashboard displays, and support for individuals whose performance was of concern, care omission meetings, and automated emails. | Clinical setting: Two wards, the pharmacy department, and one specialist clinical unit End users: clinical teams in the areas | Qualitative interviews and opinions of staff members. Secondary use of data and feedback mechanisms not successful alone therefore RCA monthly meetings organised which were perceived to be successful. |
| Finnerty et al., 2002 [31] | USA—26 state psychiatric hospitals. | To use existing data to improve delivery of care for patients suffering from schizophrenia and improving adherence to guidelines. Qualitative intervention study | Electronic pharmacy database (system not specified). Daily dosage of prescribed drugs, and duration. Other demographics were obtained from administrative databases. | Use of existing electronic data to produce reports for individuals. Adherence measures confirmed using existing data and feedback from individuals. Reports presented to each clinician as feedback and illustrating deviation from recommendations by guidelines. | Clinical setting: Across all participating hospitals End users: Clinicians | Feedback from key stakeholders (clinicians) obtained. Guidelines implemented were successful; work was undertaken with end-users to ensure data are useful and met their clinical needs. Feedback from end-users was incorporated to improve data presented however there was lack of detail around how this was conducted. |
| Griffith and Robinson, 1996 [28] | UK—General district hospital. | To determine the scale of hypnotic prescribing and implement interventions to improve prescribing habits. Quantitative intervention study, uncontrolled before and after design. | Electronic pharmacy system (system not specified). Volume of hypnotics dispensed. | Survey sent to GP to confirm use of hypnotics upon discharge and discharge summaries examined. Electronic data and manual survey data found influenced the production of an in-house policy. Electronic data helped monitor and feedback was provided at audit meetings. | Clinical setting: Hospital (all wards with elderly patient, and 100 patients selected at random) End users: not specified (potentially clinicians prescribing) | Assessed the number of hypnotics prescribed during the first day of admission and the number of patients on hypnotics post discharge using survey for evaluation. Prescribing of temazepam reduced from 60% to 25% (n = 100) and ward issue reduced from 2392 to 734 tablets. |
| Morrison et al., 2013 [29] | UK—5 intensive care units (ICUs) across England. | To determine how 5 intensive care units (ICUs) use data effectively for direct clinical care and clinical process improvement. To analyse the methods employed by ICUs to use data effectively for clinical process improvement and direct clinical care. Qualitative Ethnographic case study. | 5 Clinical information systems (Innovian (Draeger), Metavision with purchased database (iMDsoft), Metavision with own database (iMDsoft), QS (General Electric) and Carevue (Philips)). Data type not specified. | Complex intervention, no clear indication how data are being used other than for audit purposes (i.e., number of inappropriate drugs prescribed) or direct clinical care. Data quality for re-use was focused upon and initiatives used to improve this by 11 mechanisms, one of which was: using the data from the systems to improve data entry via providing positive feedback to individuals. | Clinical setting: Five ICU units End users: allied health professionals, healthcare assistant, nurses, clinical lean, consultant, local customizer, specialist registrar, senior house officer, dietician, pharmacists, and physiotherapist. | Qualitative interviews and opinions of staff members. Data had been successfully used for secondary purposes in ICUs; however, the purpose of the secondary data was not clearly stated. Difficulties experienced by the ICUs in using data for secondary purposes included: lack of primary data entry, missing information, and data quality were considered to be poor, requiring individuals to cross check information. |
| Nelson et al., 2005 [32] | USA—25-bed tertiary care hospital | To measure real time medication administration charting practice to improve current practice with a complex intervention to reduce error rates in administration. Quantitative intervention study, controlled before and after design. | Electronic prescribing and pharmacy system (Health Evaluation through Logical Processing: HELP system). Medication charting data and medication event reports used in conjunction. Data included: room number, patient identifier, terminal identifiers, medication name, dose, route, time of administration, computer system, charting time, reason for early or late administration, and nurse’s name. | Educational sessions on medication charting policies, error detection methods and prevention using decision support and real-time medication charting were discussed and reported back to staff. Staff then set their own target for improving real time charting. Weekly feedback was provided using real-time charting rates via posters in staff room. Poster slogans and the minutes for meetings presented to staff regularly (during morning and afternoon presentation sessions). Staff had freedom to ask any questions to investigators. | Clinical setting: Two surgical nursing units End users: all staff members | Percentage of real time charting rates calculated per day and due to awareness of the limitation of this data measure bedside charting rates were used as a second outcome measure. 8-week baseline real time charting: 59% (n = 16,372) for intervention unit and 53% (n = 18,453) for control unit. Post 12-week intervention period: 72% (n = 20,751) and 59% (n = 24,245), respectively. |
| Rosser et al., 2012 [27] | UK—type of hospital not specified. | To present multi-faceted interventions used to improve care and medication safety and how this can be linked to mortality. Quantitative multi-intervention case study, time series analysis. | Electronic prescribing system (PICS). Medication doses over a period of time and omitted doses from PICS and mortality rates from hospital episode statistics. | Ward based computer dashboards presenting information to clinical managers and frontline staff and monitoring of omitted medication doses. Care omission meetings led by Chief executive officer and use of electronic data for surveillance by executive team. | Clinical setting: Across hospital End users: clinical managers and frontline staff | Rate of missed doses and mortality. Overall, 16.2% reduction in mortality rates (p = 0.013) |
| Sullivan et al., 2013 [30] | USA—75-bed neonatal intensive care unit regional referral centre. | To report on development of feedback intervention and its effect on narcotic prescribing errors. Quantitative intervention-based study, uncontrolled before and after study design. | Electronic prescribing (system not specified). Use of electronic prescribing intervention data to determine errors linked to narcotic and in-house pharmacy reporting data. | Personalised and generalised email feedback provided to prescribers and prescriber feedback taken on board to improve systems (feedback strategy and bidirectional communication between prescriber and feedback team). | Clinical setting: Neonatal intensive care unit End users: nurse practitioners, physician assistants, and clinicians | Pharmacy interception rates on narcotics errors (reduced by 83%), number of days between errors (3.94 to 22.63 days), antibiotic errors unaffected by intervention (remained at 2.14 days) and read report function helped determine reading rates on prescriptions. |
| Recommendations for Best Practice | Avoid These Common Pitfalls |
|---|---|
| Discuss with existing organisations with similar electronic systems to consider their experiences with data reuse, if any. | Discussing data reuse opportunities only after system implementation, reducing the possibility of optimizing data reuse |
| Engage with staff and review what data your organisation would benefit from that could be used for secondary purposes, e.g., for CQUIN targets, improving prescribing habits, and meeting national standards set | Focusing solely on the primary purpose of the electronic system |
| Have a data warehouse (plus any additional hardware and software required) | Copying across existing reports from old system; additional opportunities exist when implementing a new system to improve the reporting functionality |
| Produce a policy outlining the data privacy issues and guidelines on secondary uses of data without compromising data privacy | Assuming data is always correct, without understanding the documentation processes involved with the data presented |
| Produce secondary use of data taxonomies, and standardize terminology and data formatting | Accepting the data at face value without understanding how data are being captured and its reflection of the process/tasks performed |
| Inform others in your organisation that secondary use of data opportunities exist and will be supported | |
| Implement an easier process for staff to review what data are already captured in your organization and enhance data accessibility | |
| Have a better system reporting functionality (determine the data timeliness, accuracy, validity, and completeness) | |
| Include data quality reports to improve data entry and enhance data transparency | |
| Ensure data anonymisation | |
| Have easier data extraction methods when implementing a new system | |
| Understand the caveats associated with the different data entries (i.e., knowledge of actual system usage resulting in the data produced rather than how data should be entered in theory) | |
| Have designated individuals who have clear knowledge around the strengths and weaknesses of the data collected | |
| Educate and train staff so they have the right skillset and knowledge relating to the data | |
| Engage recipients of data in order to maximise the SUD intervention impact and have a positive outcome |
| Authors | Characteristics of Feedback That Make It Successful [1] | ||||||
|---|---|---|---|---|---|---|---|
| Data Are Valid Based on the Receivers Perspective | Credibility of Data in Organisation (for Receivers to Believe the Data Presented) | Source and Timeliness of Data | Benchmarking (Comparing Results amongst Others and Promoting Healthy Competition) | Leaders Presenting Data (Trusted Individuals Presenting Data) | Data Are Individualised (Personalised Data) | Constant Feedback (Not a One-off Account of Feedback) | |
| Coleman et al., 2013 [25] | Not stated in paper. | Not stated. | Clinical dashboard available for staff. Reports produced feeding back data and care omission meetings constructed for feedback. | Yes, against ‘acceptable rates’ set within the hospital. | Care omission meetings lead by executive members. | Directorate level emails not personalised data. | Not clear if dashboard was live (regularly accessible to user), weekly emails and monthly meetings. |
| Dixon-Woods et al., 2013 [11] | Yes data validity not questioned. | Not stated. | The raw data from ePDSS were used with regular feedback to clinical teams (with improvement suggestions when needed via conversations, emails and meetings), dashboard displays, and support for individuals whose performance was of concern, care omission meetings, and automated emails. | Against set standards within the organisation. | Executive team leading meetings. | Yes and support provided for individuals causing concern. | Monthly meetings and dashboard displays available for users. |
| Finnerty, M., et al., 2002 [31] | Receivers had opportunity to feedback on report, but nothing stated around data validity. | Receivers knew data source. | Use of existing electronic data to produce reports for individuals and monthly data collected. | Compared against guidance. | Reports produced and piloted not clear if presented by leaders. | Use of existing electronic data to produce reports for individuals. Reports presented to each clinician as feedback and illustrating deviation from recommendations by guidelines. | Input for feedback report production done twice. |
| Morrison et al., 2013 [29] | Not stated. | Not stated. | using the data from the systems to improve data entry via providing positive feedback to individuals. | Yes, positive results stated. | Senior staff. | Yes, by stating people adhering to correct data entry. | Not stated. |
| Nelson et al., 2005 [32] | Not stated. | Staff had freedom to ask any questions to investigators. | Real-time medication charting was discussed and reported back to staff. Poster slogans and the minutes for meetings presented to staff regularly (during morning and afternoon presentation sessions). | Target for improving real time charting was set by senior staff. | Not stated. | Not stated. | Weekly feedback was provided using real-time charting rates via posters in staff room. |
| Rosser et al., 2012 [27] | Not stated. | Not stated. | Ward-based computer dashboards presenting information to clinical managers and frontline staff and monitoring of omitted medication doses. | Not stated. | Care omission meetings led by Chief executive officer and use of electronic data for surveillance by executive team. | Not stated. | Clinical dashboard available to staff. |
| Sullivan et al., 2013 [30] | Not stated. | Receivers aware of feedback programme as involved in the piloting. | Dashboard using electronic data and data collected every two weeks. | General and personalised feedback available not clear statement around benchmarking performance. | Presented via email and by pharmacists. | Personalised and generalised email feedback provided to prescribers and prescriber feedback taken on board to improve systems (feedback strategy and bidirectional communication between prescriber and feedback team). | Yes, every two weeks. |
| Griffith and Robinson, 1996 [28] | Note stated. | Not stated. | Electronic pharmacy data and survey data. | Not stated. | Not stated. | Not stated. | Not stated. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chaudhry, N.T.; Franklin, B.D.; Mohammed, S.; Benn, J. The Secondary Use of Data to Support Medication Safety in the Hospital Setting: A Systematic Review and Narrative Synthesis. Pharmacy 2021, 9, 198. https://doi.org/10.3390/pharmacy9040198
Chaudhry NT, Franklin BD, Mohammed S, Benn J. The Secondary Use of Data to Support Medication Safety in the Hospital Setting: A Systematic Review and Narrative Synthesis. Pharmacy. 2021; 9(4):198. https://doi.org/10.3390/pharmacy9040198
Chicago/Turabian StyleChaudhry, Navila Talib, Bryony Dean Franklin, Salmaan Mohammed, and Jonathan Benn. 2021. "The Secondary Use of Data to Support Medication Safety in the Hospital Setting: A Systematic Review and Narrative Synthesis" Pharmacy 9, no. 4: 198. https://doi.org/10.3390/pharmacy9040198
APA StyleChaudhry, N. T., Franklin, B. D., Mohammed, S., & Benn, J. (2021). The Secondary Use of Data to Support Medication Safety in the Hospital Setting: A Systematic Review and Narrative Synthesis. Pharmacy, 9(4), 198. https://doi.org/10.3390/pharmacy9040198