Implementation of a Teaching Electronic Medical Record within Didactic Instruction Using a Drug Information Question Assignment


Abstract
1. Introduction
2. Materials and Methods
2.1. Research Setting
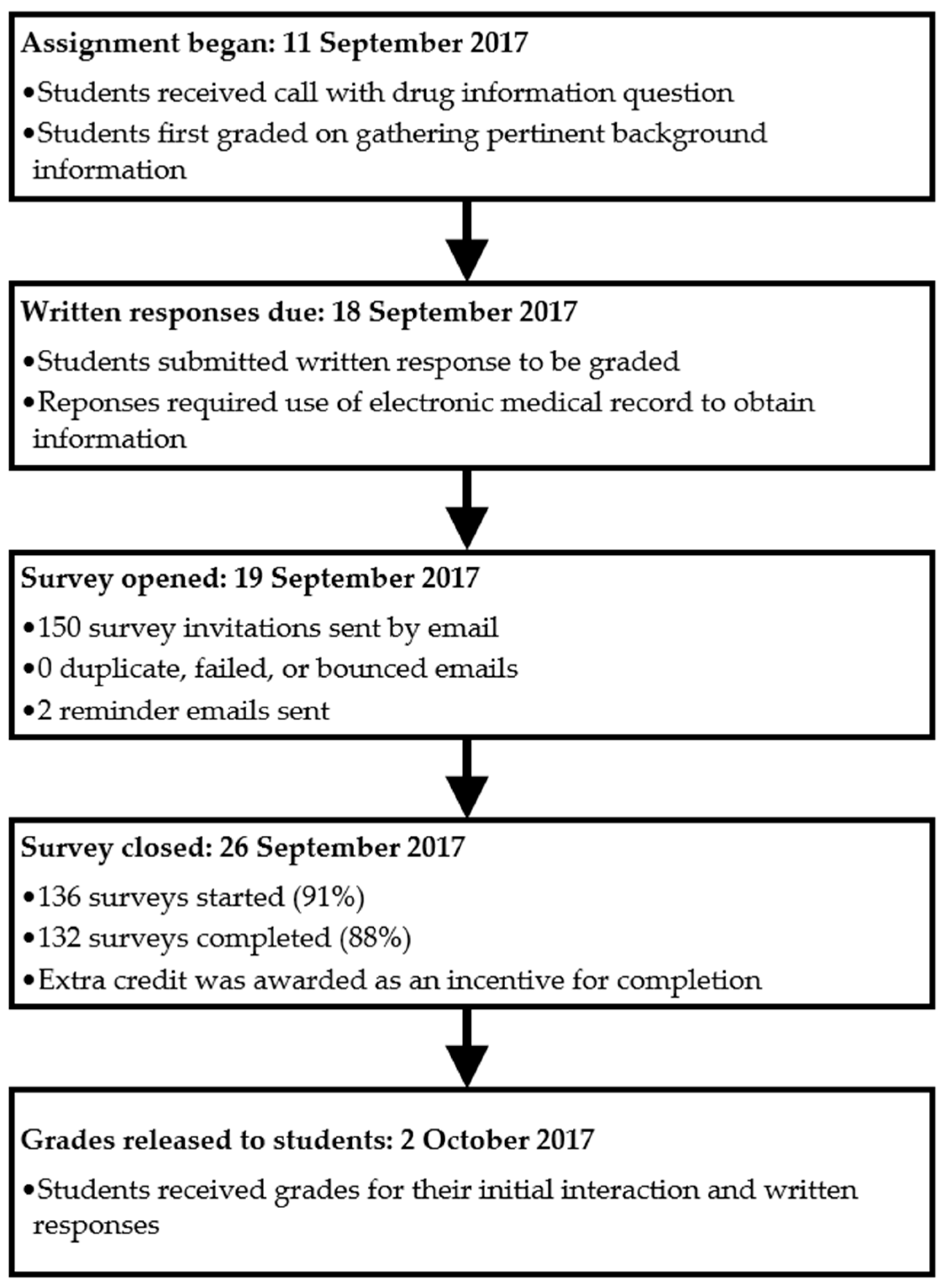
2.2. Implementation of Teaching EMR
2.3. Assessment of Student Perceptions
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Example Drug Information Question Given to Students by an Instructor
- •
- Name: Faye Dugan
- •
- MRN: 3938703891, 45 year old female
- •
- Height/Weight: 5 feet 7 inches; 136 pounds
- •
- Temperature: 98.9 degrees Fahrenheit
- •
- Blood Pressure: 132/62 mmHg
- •
- Oxygen Saturation: 99%
- •
- Pulse: 88 bpm
- •
- Respiratory Rate: 19 breathes per minute
- •
- Pain Score: 2
- •
- Renal Function Labs: “I don’t know” (student would need to locate in EMR)
- •
- Liver Function Labs: “I don’t know” (student would need to locate in EMR)
- •
- Required Background Questions for Students to Ask for Full Credit:
- •
- What is the indication for naltrexone? (pathological gambling)
- •
- What is the patient’s age and weight? (age as above, student to locate weight in EMR)
- •
- What is the status of the patient’s renal and hepatic function? “I don’t know” (in EMR)
- •
- What are the patient’s current medical problems? (provide PMH as above)
- •
- What other medications is the patient taking right now? (as above)
- •
- What are the doses of the patient’s current medications? “I don’t know” (in EMR)
- •
- Does the patient take any OTC or herbal medications? “I don’t know” (in EMR)
- •
- Does the patient have any allergies? “I don’t know” (in EMR)
References
- Accreditation Council for Pharmacy Education. Accreditation Standards and Key Elements for the Professional Program in Pharmacy Leading to Doctor of Pharmacy Degree. Available online: https://www.acpe-accredit.org/pdf/Standards2016Final.pdf (accessed on 16 March 2020).
- The Office of the National Coordinator for Health Information Technology (ONC). Law, Regulation, and Policy. Available online: https://www.healthit.gov/topic/laws-regulation-and-policy (accessed on 16 March 2020).
- US Centers for Medicare & Medicaid Services. Promoting Interoperability (PI). Available online: https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/ (accessed on 16 March 2020).
- US Department of Health and Human Services. Standards for the Electronic Health Record Technology Incentive Program. 42 CFR 495. Available online: https://www.ecfr.gov/cgi-bin/text-idx?SID=daf746912b0362d08add1fe2d7356c79&mc=true&node=pt42.5.495&rgn=div5#se42.5.495_12 (accessed on 16 March 2020).
- Henry, J.; Pylypchuk, Y.; Searcy, T.; Patel, V. Adoption of Electronic Health Record Systems Among US non-Federal Acute Care Hospitals: 2008–2015. ONC Data Brief, no.35. Office of the National Coordinator for Health Information Technology: Washington DC. Available online: https://dashboard.healthit.gov/evaluations/data-briefs/non-federal-acute-care-hospital-ehr-adoption-2008–2015.php (accessed on 16 March 2020).
- Joint Commission of Pharmacy Practitioners. The Pharmacists’ Patient Care Process. Available online: https://jcpp.net/patient-care-process/ (accessed on 16 March 2020).
- Ehrenstein, V.; Kharrazi, H.; Lehmann, H.; Taylor, C.O. Chapter 4: Obtaining data from electronic health records. In Tools and Technologies for Registry Interoperability, Registries for Evaluating Patient Outcomes: A User’s Guide, 3rd ed.; Gliklich, R.E., Leavy, M.B., Dreyer, N.A., Eds.; Addendum 2; Agency for Healthcare Research and Quality: Rockville, ME, USA, 2019. Available online: https://www.ncbi.nlm.nih.gov/books/NBK551878/ (accessed on 16 March 2020).
- Frenzel, J.E. Using electronic medical records to teach patient-centered care. Am. J. Pharm. Educ. 2010, 74, 71. [Google Scholar] [CrossRef] [PubMed]
- Hincapie, A.L.; Cutler, T.W.; Fingado, A.R. Incorporating health information technology and pharmacy informatics in a pharmacy professional didactic curriculum-with a team-based learning approach. Am. J. Pharm. Educ. 2016, 80, 107. [Google Scholar] [CrossRef] [PubMed]
- Kirwin, J.L.; DiVall, M.V.; Guerra, C.; Brown, T. A simulated hospital pharmacy module using an electronic medical record in a pharmaceutical care skills laboratory course. Am. J. Pharm. Educ. 2013, 77, 62. [Google Scholar] [CrossRef] [PubMed]
- Ray, S.; Bellone, J.; Zupec, N.; Bartelme, K. Retention of students’ ability to incorporate a computer into simulated patient encounters. Am. J. Pharm. Educ. 2018, 82, 6748. [Google Scholar] [CrossRef] [PubMed]
- Wisniewski, J.N.; Wisniewski, C.S.; Jones, E.P.; Van Cuyk, M.P. Incorporation of a mock drug information telephone call exercise in a health-systems pharmacy laboratory. Curr. Pharm. Teach. Learn 2020, 12, 450–458. [Google Scholar] [CrossRef] [PubMed]
- VanLangen, K.; Wellman, G. Trends in electronic health record usage among US colleges of pharmacy. Curr. Phar. Teach. Learn 2018, 10, 566–570. [Google Scholar] [CrossRef] [PubMed]
- Clauson, K.A.; Breeden, E.A.; Fingado, A.R.; Kaing, C.L.; Flynn, A.J.; Cutler, T.W. A progress report on the state of pharmacy informatics education in US pharmacy schools and colleges. Am. J. Pharm. Educ. 2018, 82, 6332. [Google Scholar] [CrossRef] [PubMed]
- Flynn, A.J. The current state of pharmacy informatics education in professional programs at US colleges of pharmacy. Am. J. Pharm. Educ. 2005, 69, 66. [Google Scholar] [CrossRef][Green Version]
- Fox, B.I.; Karcher, R.B.; Flynn, A.; Mitchell, S. Pharmacy informatics syllabi in doctor of pharmacy programs in the US. Am. J. Pharm. Educ. 2008, 72, 89. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Cook, D.A.; Artino, A.R. Motivation to learn: An overview of contemporary theories. Med. Educ. 2016, 50, 997–1014. [Google Scholar] [CrossRef] [PubMed]
- Dweck, S.A. Self-Theories: Their Role in Motivation, Personality, and Development; Psychology Press: Hove, UK, 2000. [Google Scholar]
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Calis, K.A.; Anderson, D.W.; Auth, D.A.; Mays, D.A.; Turcasso, N.M.; Meyer, C.C.; Young, L.R. Quality of pharmacotherapy consultations provided by drug information centers in the United States. Pharmacotherapy 2000, 20, 830–836. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, M.; Parkman, H.P.; Shafit, M.A.; Abell, T.L.; Gerson, L. Clinical guideline: Management of gastroparesis. Am. J. Gastroenterol. 2013, 108, 18–37. [Google Scholar] [CrossRef] [PubMed]
- Ghaibi, S.; Ipema, H.; Gabay, M. ASHP guidelines on the pharmacist’s role in providing drug information. Am. J. Health Syst. Pharm. 2015, 72, 573–577. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Respondents n = 38, n (%) | |
|---|---|
| Previous exposure to EMR practice setting a | |
| Hospital | 19 (50) |
| Ambulatory Care Office | 3 (7.9) |
| Academic | 1 (2.6) |
| Community Based System | 20 (52.6) |
| Managed Care Pharmacy | 1 (2.6) |
| Prefer not to say | 1 (2.6) |
| Previous exposure to EMR practice type a | |
| Paid job or internship outside of IPPE | 22 (57.9) |
| IPPE | 20 (52.6) |
| Academic | 3 (7.9) |
| Volunteer work outside of IPPE | 3 (7.9) |
| Type of EMRs exposure a | |
| Cerner | 11 (28.9) |
| Epic | 5 (13.2) |
| Allscripts (Sunrise Clinical Manager) | 3 (7.9) |
| NextGen | 1 (2.6) |
| Athena | 1 (2.6) |
| eClinicalWorks | 2 (5.3) |
| McKesson | 4 (10.5) |
| Others, not specified | 5 (13.2) |
| Unknown | 9 (23.7) |
| Approximate length of time working with EMRs | |
| <2 weeks | 5 (13.2) |
| ≥2 weeks, but <1 month | 3 (7.9) |
| ≥1 month, but <1 year | 18 (47.4) |
| ≥1 year | 11 (28.9) |
| Prefer not to say | 1 (2.6) |
| Statement | Pre Assignment | Post Assignment | |||
|---|---|---|---|---|---|
| Mean (SD) Median | Agreed or Strongly Agreed, n (%) | Mean (SD) Median | Agreed or Strongly Agreed, n (%) | p Value a | |
| I am confident in my ability to look up and obtain patient specific information from an electronic medical record (EMR). (n = 132, 128) | 3.49 (1.04) 4 | 27 (20.5) | 2.09 (0.70) 2 | 106 (82.8) | <0.001 |
| Access to an EMR is useful for completing the drug information question assignment. (n = 132, 131) | 2.08 (0.78) 2 | 95 (71.9) | 1.63 (0.81) 1 | 120 (91.6) | <0.001 |
| Access to patient information in an EMR is necessary to provide appropriate responses to drug information questions in pharmacy practice. (n = 132, 131) | 2.02 (0.75) 2 | 102 (77.2) | 1.44 (0.58) 1 | 130 (99.3) | <0.001 |
| Using the teaching EMR to complete the drug information assignment will improve or has improved my knowledge of EMR systems. (n = 132, 130) | 2.30 (0.79) 2 | 81 (61.4) | 1.70 (0.80) 2 | 116 (89.3) | <0.001 |
| Using the teaching EMR to complete the drug information assignment will improve or has improved my confidence in using EMR systems. (n = 131, 130) | 2.34 (0.76) 2 | 76 (58.0) | 1.84 (0.81) 2 | 110 (84.7) | <0.001 |
| Student pharmacists should be exposed to EMRs during classroom coursework. (n = 131, 131) | 1.87 (0.80) 2 | 105 (80.2) | 1.42 (0.67) 1 | 127 (96.9) | <0.001 |
| The teaching EMR used is easy to learn and easy to navigate. (n = 131, 130) | 3.09 (0.84) 3 | 28 (21.4) | 2.60 (0.99) 2 | 67 (51.6) | <0.001 |
| The teaching EMR used to complete the drug information assignment will improve my performance during upcoming IPPE and APPE rotations. (n = 132, 131) | 2.33 (0.74) 2 | 78 (59.1) | 1.98 (0.78) 2 | 104 (79.4) | <0.001 |
| Access to the teaching EMR for the drug information assignment will improve or has improved my verbal score. (n = 131, 130) | 3.05 (0.72) 3 | 24 (18.3) | 2.93 (0.90) 3 | 38 (29.3) | 0.03 |
| Access to the teaching EMR for the drug information assignment will improve or has improved my written score. (n = 132, 131) | 4.71 (3.08) 2 | 67 (50.8) | 3.05 (2.70) 2 | 99 (75.5) | <0.001 |
| The integration of the teaching EMR within the drug information course will enhance or has enhanced my overall learning experience. (n = 132, 131) | 2.23 (0.75) 2 | 88 (66.7) | 1.84 (0.73) 2 | 114 (87.1) | <0.001 |
| It is an expectation that pharmacy graduates are ready to appropriately use health information tools, including EMRs. (n = 132, 130) | 1.95 (0.79) 2 | 103 (78.0) | 1.62 (0.80) 1 | 116 (89.3) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wasynczuk, J.; Sheehan, A.H. Implementation of a Teaching Electronic Medical Record within Didactic Instruction Using a Drug Information Question Assignment. Pharmacy 2021, 9, 35. https://doi.org/10.3390/pharmacy9010035
Wasynczuk J, Sheehan AH. Implementation of a Teaching Electronic Medical Record within Didactic Instruction Using a Drug Information Question Assignment. Pharmacy. 2021; 9(1):35. https://doi.org/10.3390/pharmacy9010035
Chicago/Turabian StyleWasynczuk, Jacqueline, and Amy H. Sheehan. 2021. "Implementation of a Teaching Electronic Medical Record within Didactic Instruction Using a Drug Information Question Assignment" Pharmacy 9, no. 1: 35. https://doi.org/10.3390/pharmacy9010035
APA StyleWasynczuk, J., & Sheehan, A. H. (2021). Implementation of a Teaching Electronic Medical Record within Didactic Instruction Using a Drug Information Question Assignment. Pharmacy, 9(1), 35. https://doi.org/10.3390/pharmacy9010035