Validation of a Drug-Related Problem Classification System for the Intermediate and Long-Term Care Setting in Singapore


Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participant Recruitment
2.2. Data Collection
2.3. Outcome Measures and Data Analysis
3. Results
3.1. Participants’ Demographics
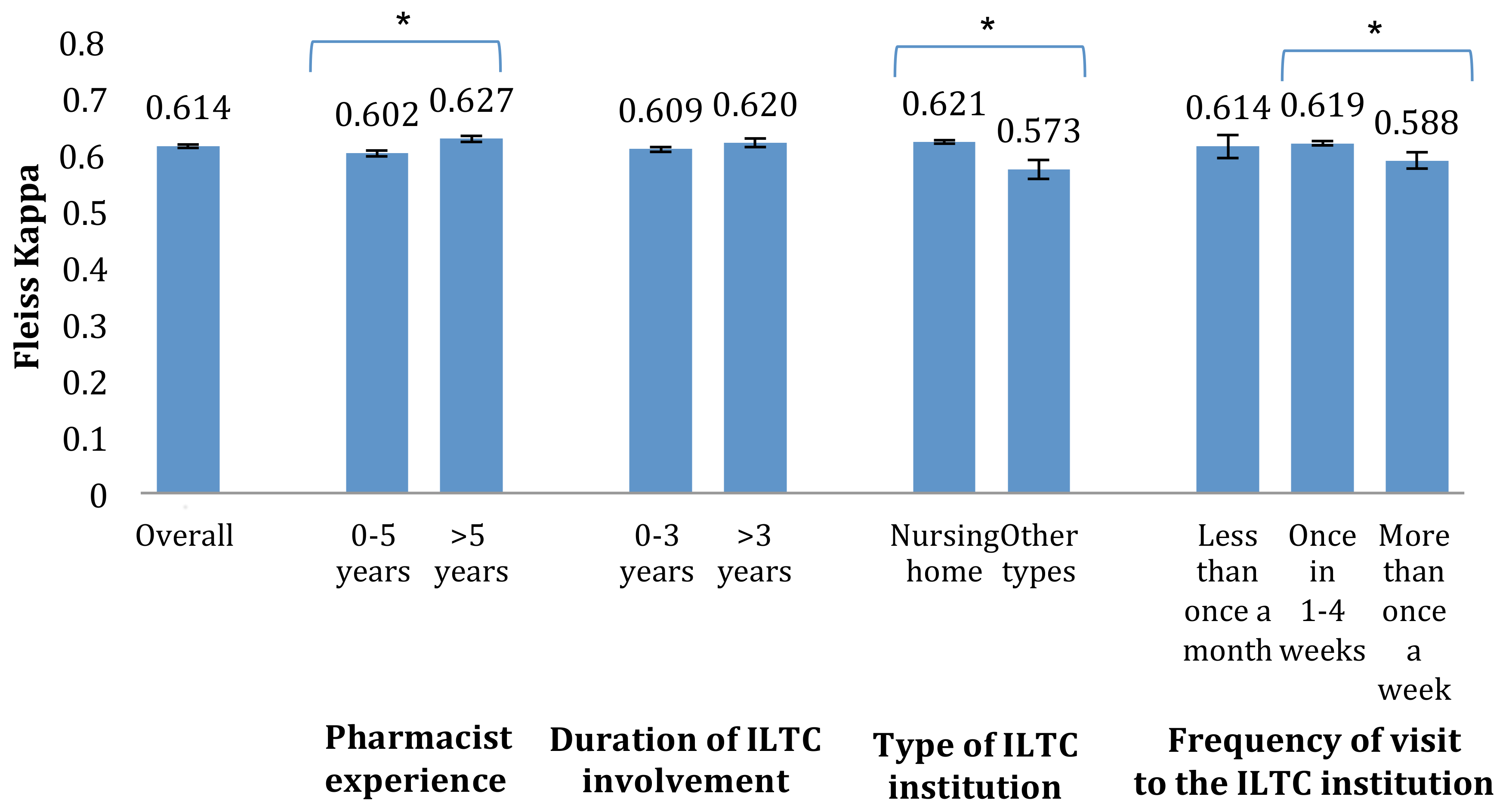
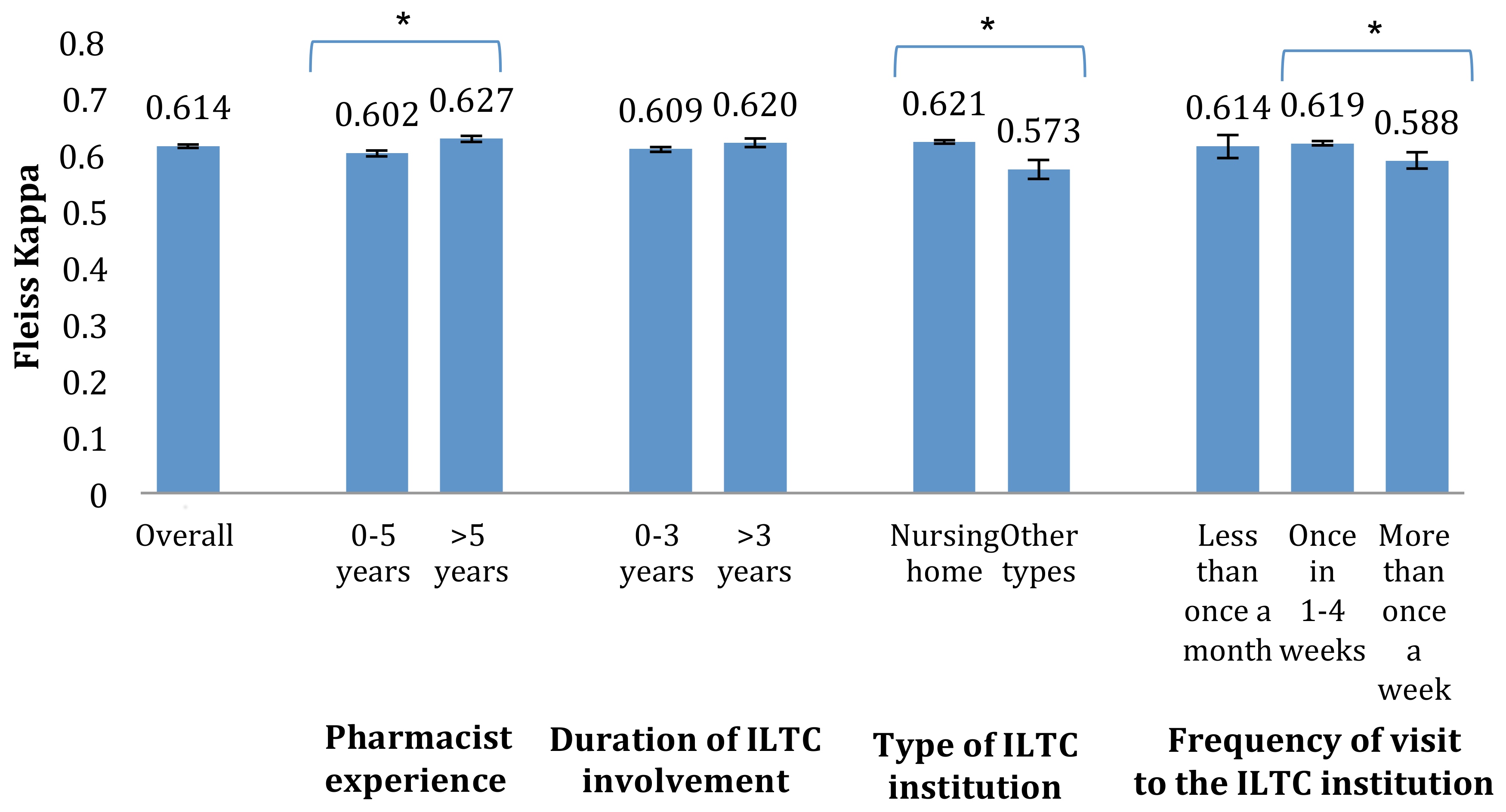
3.2. Inter-Rater Reliability
3.3. Users’ Perceived Usability
4. Discussion
4.1. Inter-Rater Reliability
4.2. Users’ Perception of Usability
4.3. Limitations and Future Work
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pharmaceutical Care Network Europe. Pharmaceutical Care Network Europe Classification for Drug Related Problems V7. Available online: http://www.pcne.org/upload/files/152_PCNE_classification_V7-0.pdf (accessed on 20 August 2018).
- Ernst, F.R.; Grizzle, A.J. Drug-related morbidity and mortality: Updating the cost-of-illness model. J. Am. Pharm. Assoc. 2001, 41, 192–199. [Google Scholar] [CrossRef]
- Cipolle, R.J.; Strand, L.; Morley, P. Pharmaceutical Care Practice: The Patient-Centered Approach to Medication Management, 3rd ed.; McGraw-Hill Education: New York, NY, USA, 2012; pp. 141–182. [Google Scholar]
- Van Mil, J.W.; Westerlund, L.O.; Hersberger, K.E.; Schaefer, M.A. Drug-related problem classification systems. Ann. Pharmacother. 2004, 38, 859–867. [Google Scholar] [CrossRef] [PubMed]
- Chia, H.S.; Ho, J.A.; Lim, B.D. Pharmacist review and its impact on Singapore nursing homes. Singap. Med. J. 2015, 56, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Hohmann, C.; Eickhoff, C.; Klotz, J.M.; Schulz, M.; Radziwill, R. Development of a classification system for drug-related problems in the hospital setting (APS-Doc) and assessment of the inter-rater reliability. J. Clin. Pharm. Ther. 2012, 37, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.; Peterson, G.M.; Tenni, P.C.; Bindoff, I.K.; Stafford, A.C. Document: A system for classifying drug-related problems in community pharmacy. Int. J. Clin. Pharm. 2012, 34, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Silva, C.; Ramalho, C.; Luz, I.; Monteiro, J.; Fresco, P. Drug-related problems in institutionalized, polymedicated elderly patients: Opportunities for pharmacist intervention. Int. J. Clin. Pharm. 2015, 37, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Basger, B.J.; Moles, R.J.; Chen, T.F. Application of drug-related problem (DRP) classification systems: A review of the literature. Eur. J. Clin. Pharmacol. 2014, 70, 799–815. [Google Scholar] [CrossRef] [PubMed]
- Hepler, C.D.; Strand, L.M. Opportunities and responsibilities in pharmaceutical care. Am. J. Hosp. Pharm. 1990, 47, 533–543. [Google Scholar] [PubMed]
- Ministry of Social and Family Development. Committee on Ageing Issues: Report on the Ageing Population 2006. Available online: https://www.msf.gov.sg/publications/Pages/Report-of-the-Committee-on-Ageing-Issues-2006.aspx (accessed on 25 August 2018).
- Pharmaceutical Society of Singapore. PSS ILTC Pharmacist Workgroup Inaugural Management Meeting. Available online: http://www.pss.org.sg/whats-happening/e-bulletin/issue-no-121-pss-e-bulletin-august-2016/pss-iltc-pharmacist-workgroup#.WJxqmm997IV (accessed on 11 January 2016).
- Basger, B.J.; Moles, R.J.; Chen, T.F. Development of an aggregated system for classifying causes of drug-related problems. Ann. Pharmacother. 2015, 49, 405–418. [Google Scholar] [CrossRef] [PubMed]
- AbuRuz, S.M.; Bulatova, N.R.; Yousef, A.M. Validation of a comprehensive classification tool for treatment-related problems. Pharm. World Sci. 2006, 28, 222–232. [Google Scholar] [CrossRef] [PubMed]
- Eichenberger, P.M.; Lampert, M.L.; Kahmann, I.V.; van Mil, J.F.; Hersberger, K.E. Classification of drug-related problems with new prescriptions using a modified PCNE classification system. Pharm. World Sci. 2010, 32, 362–372. [Google Scholar] [CrossRef] [PubMed]
- Maes, K.A.; Tremp, R.M.; Hersberger, K.E.; Lampert, M.L. Demonstrating the clinical pharmacist’s activity: Validation of an intervention oriented classification system. Int. J. Clin. Pharm. 2015, 37, 1162–1171. [Google Scholar] [CrossRef] [PubMed]
- Fleiss, J.L. Measuring nominal scale agreement among many raters. Psychol. Bull. 1971, 76, 378–382. [Google Scholar] [CrossRef]
- IBM. Stats Fleiss Kappa. Available online: https://www.ibm.com/developerworks/community/files/app#/file/48234a16-fb14-4bee-8c18-570319c57108 (accessed on 19 December 2016).
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| No. | Main Categories | Subcategories | Remarks |
|---|---|---|---|
| 1 | Indication | (a) Drug use without indication | Patient is taking a drug without a valid medical indication |
| (b) Untreated indication | Patient has medical problem that requires drug therapy but is not receiving medication for that indication Examples: • Conditions where patients are in need of prophylaxis or premedications but are not receiving them • Combination therapy required for synergistic effect but only one drug is used, e.g., antibiotics, chemotherapy | ||
| (c) Therapeutic duplication | Inappropriate duplication of therapeutic group or active ingredients | ||
| 2 | Improper drug selection | (a) Contraindication | Patient has contraindications to the drug prescribed |
| (b) More cost-effective drug available | Similarly effective alternative is available at a cheaper price | ||
| 3 | Dosage | (a) Drug dose is too low | Dosage regimen is not individualized for a specific patient, taking into consideration the appropriate drug, disease, and patient-specific information Examples: • Dosage regimen adjustment for patients with renal/hepatic impairment • Dose adjustment when switching between formulations, e.g., phenytoin tablets and syrup, controlled release to immediate release formulation |
| (b) Drug dose is too high | |||
| (c) Dosage regimen not frequent enough | |||
| (d) Dosage regimen too frequent | |||
| 4 | Duration | (a) Duration of treatment too short | Patient is prescribed a drug for a duration that is clinically inappropriate |
| (b) Duration of treatment too long | |||
| 5 | Drug form | (a) Inappropriate formulation/drug form | Formulation/drug form is not individualized to patient, e.g., sustained release medication given to patient with nasogastric tube |
| (b) Inappropriate change in brand | Different preparations of the same drug may not be bioequivalent. For drugs that have a narrow therapeutic window, switch in brands can affect clinical outcomes, e.g., levothyroxine | ||
| 6 | Adverse drug reaction | (a) ADR (nonallergic) | Consistent with pharmacologic actions of the drug, occur commonly, are usually dose dependent, and are fairly predictable |
| (b) ADR (allergic) | Allergic or idiosyncratic reactions that are independent of drug pharmacology. Rare, not dose related, and cannot be predicted. (To be differentiated from wrong drug used where patient has been experiencing allergic reactions for a period of time versus ADR, where patient is taking medication for first time and experiences allergic reaction) | ||
| 7 | Drug interaction | (a) Drug–drug interaction | E.g., Clarithromycin and simvastatin |
| (b) Drug–food interaction | E.g., Dairy products and levothyroxine | ||
| (c) Drug–lab interaction | E.g., Anaemia and HbA1c results | ||
| (d) Drug–disease interaction | Clinically significant interaction between patient’s pre-existing medical conditions and drug prescribed | ||
| 8 | Others | (a) Lab monitoring | • Lack of routine lab monitoring, which is required for adjustment of drug dose, monitoring of side effects etc., e.g., random blood glucose, HbA1C, LFTs, lipid Panel, renal panel • Lab monitoring not performed at an interval that is clinically appropriate |
| (b) RMR—related | E.g., illegibility, ambiguity, clarification of drug order, incomplete information, and lack of doctor’s signature at RMR, lack of nurses’ signature to sign on/off medication, lack of nurses’ signature to indicate medications served, inappropriate use of legends | ||
| (c) Expired medication/inappropriate storage | • Patient given expired medication or medication that have not been stored properly • Patient misses dose as a result of expired or inappropriately stored medication | ||
| (d) Nonavailability of medication | • Patient or family unable to afford medication, thus drug not made available • Drug prescribed is not available in Singapore or exemption medication or unable to be supplied to the institution • Inability to get the medication in time | ||
| (e) Others—please state reason | Any unique/additional cases of DRPs that do not fall under any of the categories above • Please kindly specify the reason for putting it in this category and/or describe the DRP |
| Demographic Factors | N | % |
|---|---|---|
| Age | ||
| 21–30 years old | 22 | 66.7 |
| 31–50 years old | 11 | 33.3 |
| Gender | ||
| Male | 9 | 27.3 |
| Female | 24 | 72.7 |
| Working experience as a pharmacist | ||
| 0–5years | 18 | 54.5 |
| >5 years | 15 | 45.5 |
| Duration of involvement in ILTC sector | ||
| 0–3 years | 22 | 66.7 |
| >3 years | 11 | 33.3 |
| Type of ILTC institution | ||
| Nursing home | 27 | 81.8 |
| Others * | 6 | 18.2 |
| Frequency of visit to the ILTC institution | ||
| Less than once a month | 5 | 15.2 |
| Once in 1–4 weeks | 21 | 63.6 |
| More than once a week | 7 | 21.2 |
| Positive Ratings a | Neutral Ratings | Negative Ratings b | |
|---|---|---|---|
| n (%) | |||
| The DRP classification system allows me to choose the correct DRP category for the cases | 29 (87.9) | 3 (9.1) | 1 (3.0) |
| The classification system is comprehensive | 23 (69.7) | 7 (21.2) | 3 (9.1) |
| The classification system is easy to use | 24 (72.7) | 5 (15.2) | 4 (12.1) |
| I am able to categorise the different types of DRPs efficiently by using the classification system | 23 (69.7) | 7 (21.2) | 3 (9.1) |
| I will use such a classification system in future | 23 (69.7) | 6 (18.2) | 4 (12.1) |
| In general, I am satisfied with the classification system | 24 (72.7) | 8 (24.3) | 1 (3.0) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, X.Y.; Yeo, Q.Q.; Kng, G.L.L.; Chung, W.L.; Yap, K.Z. Validation of a Drug-Related Problem Classification System for the Intermediate and Long-Term Care Setting in Singapore. Pharmacy 2018, 6, 109. https://doi.org/10.3390/pharmacy6040109
Lim XY, Yeo QQ, Kng GLL, Chung WL, Yap KZ. Validation of a Drug-Related Problem Classification System for the Intermediate and Long-Term Care Setting in Singapore. Pharmacy. 2018; 6(4):109. https://doi.org/10.3390/pharmacy6040109
Chicago/Turabian StyleLim, Xin Yan, Quan Qi Yeo, Grace Li Lin Kng, Wing Lam Chung, and Kai Zhen Yap. 2018. "Validation of a Drug-Related Problem Classification System for the Intermediate and Long-Term Care Setting in Singapore" Pharmacy 6, no. 4: 109. https://doi.org/10.3390/pharmacy6040109
APA StyleLim, X. Y., Yeo, Q. Q., Kng, G. L. L., Chung, W. L., & Yap, K. Z. (2018). Validation of a Drug-Related Problem Classification System for the Intermediate and Long-Term Care Setting in Singapore. Pharmacy, 6(4), 109. https://doi.org/10.3390/pharmacy6040109