Training Needs of Manitoba Pharmacists to Increase Application of Assessment and Prescribing for Minor Ailments into Practice: A Qualitative and Quantitative Survey

Abstract
1. Introduction
2. Methods
2.1. Survey Design
2.2. Recruitment and Data Collection
2.3. Statistical Analysis
3. Results
3.1. Demographics of Survey Respondents
3.2. Assessment and Prescribing Skills for Self-Limiting Conditions in the Practice Setting
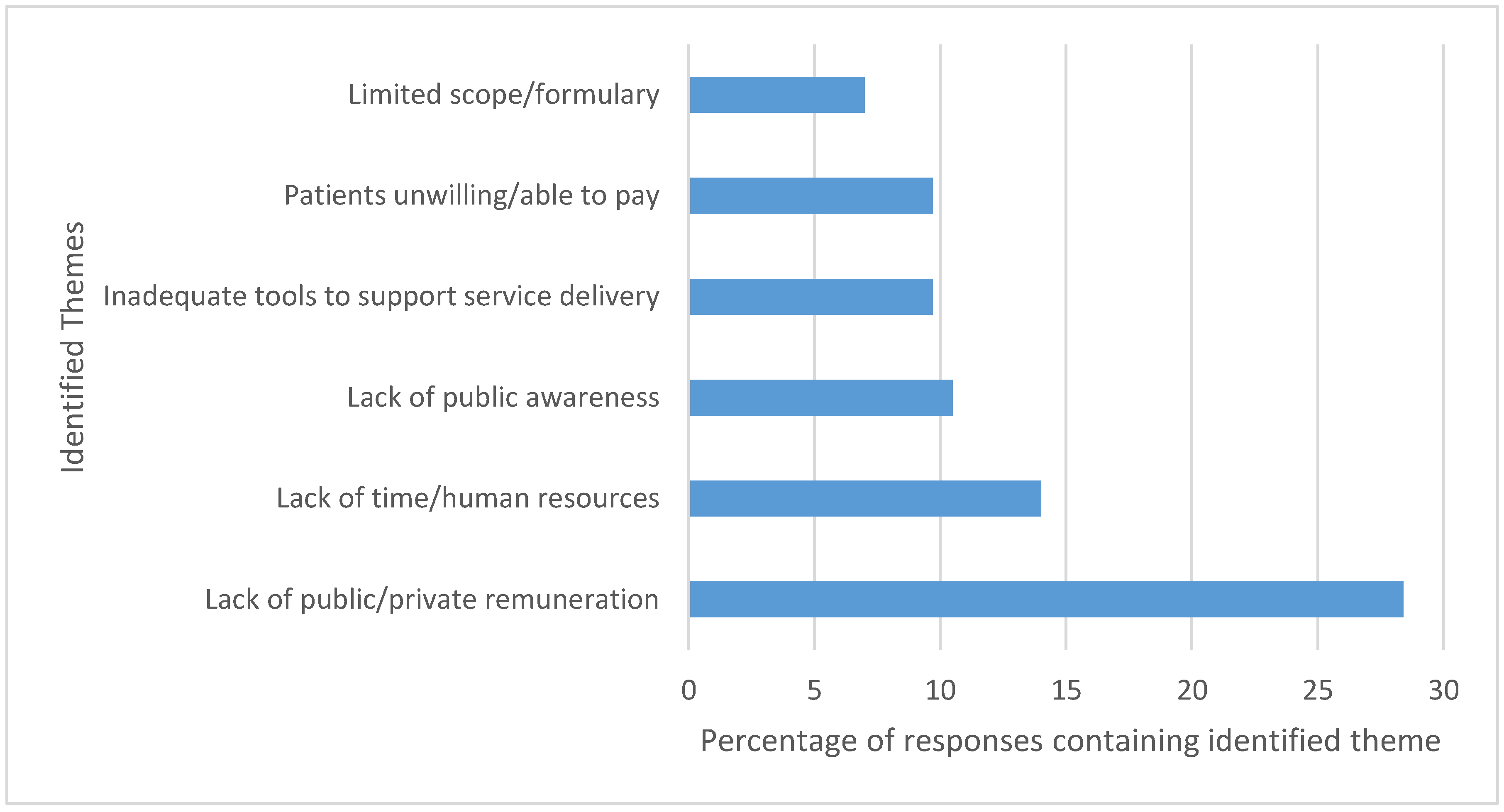
3.3. Perceived Barriers for Applying Assessment and Prescribing Skills
3.4. Preferences for Continuing Education
4. Discussion
Strengths & Limitation
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Habicht, D.; Ng, S.; Dunford, D.; Shearer, B.; Kuo, I.F. Incorporating assessment and prescribing for ambulatory ailments skills into practice: An environmental scan of continuing education for pharmacist prescribing in Canada. Can. Pharm. J. 2017, 150, 316–325. [Google Scholar] [CrossRef] [PubMed]
- College of Pharmacists of Manitoba. A guide to pharmacy practice in Manitoba. 2018. Available online: http://www.cphm.ca/uploaded/web/Legislation/Pharmacy-Practice-Guide/Guide-to-Pharmacy-Practice-Final.pdf (accessed on 4 August 2018).
- Faruquee, C.F.; Guirguis, L.M. A scoping review of research on the prescribing practice of Canadian pharmacists. Can. Pharm. J. 2015, 148, 325–348. [Google Scholar] [CrossRef] [PubMed]
- Canadian Pharmacists Association. A Review of Pharmacy Services in Canada and the Health Economic Evidence. 2016. Available online: https://www.pharmacists.ca/cpha-ca/assets/File/cpha-on-the-issues/Pharmacy%20Services%20Report%201.pdf (accessed on 4 August 2018).
- Grol, R.; Grimshaw, J. From best evidence to best practice: Effective implementation of change in patients’ care. Lancet 2003, 362, 1225–1230. [Google Scholar] [CrossRef]
- George, J.; Pfleger, D.; McCaig, D.; Bond, C.; Stewart, D. Independent prescribing by pharmacists: A study of the awareness, views and attitudes of Scottish community pharmacists. Pharm. World Sci. 2006, 28, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Pfleger, D.E.; McHattie, L.W.; Diack, H.L.; McCaig, D.J.; Stewart, D.C. Views, attitudes and self-assessed training needs of Scottish community pharmacists to public health practice and competence. Pharm. World Sci. 2008, 30, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Partin, M.R.; Powell, A.A.; Burgess, D.J.; Haggstrom, D.A.; Gravely, A.A.; Halek, K.; Bangerter, A.; Shaukat, A.; Nelson, D.B. Adding Postal Follow-Up to a Web-Based Survey of Primary Care and Gastroenterology Clinic Physician Chiefs Improved Response Rates but not Response Quality or Representativeness. Eval. Health Prof. 2015, 38, 382–403. [Google Scholar] [CrossRef] [PubMed]
- Gregory, P.A.M.; Teixeira, B.; Austin, Z. What does it take to change practice? Perspectives of pharmacists in Ontario. Can. Pharm. J. 2018, 151, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Houle, S.K.D.; Grindrod, K.A.; Chatterley, T.; Tsuyuki, R.T. Paying pharmacists for patient care: A systematic review of remunerated pharmacy clinical care services. Can. Pharm. J. 2014, 147, 209–232. [Google Scholar] [CrossRef] [PubMed]
- McCullough, K.B.; Formea, C.M.; Berg, K.D.; Burzynski, J.A.; Cunningham, J.L.; Ou, N.N.; Rudis, M.I.; Stollings, J.L.; Nicholson, W.T. Assessment of the pharmacogenomics educational needs of pharmacists. Am. J. Pharm. Educ. 2011, 75, 51. [Google Scholar] [CrossRef] [PubMed]
- Kibicho, J.; Pinkerton, S.D.; Owczarzak, J. Community-Based Pharmacists’ Needs for HIV-Related Training and Experience. J. Pharm. Pract. 2014, 27, 369–378. [Google Scholar] [CrossRef] [PubMed]
- Maio, V.; Belazi, D.; Goldfarb, N.I.; Phillips, A.L.; Crawford, A.G. Use and effectiveness of pharmacy continuing-education materials. Am. J. Health Syst. Pharm. 2003, 60, 1644–1649. [Google Scholar] [PubMed]
- Hasan, S. Continuing education needs assessment of pharmacists in the United Arab Emirates. Pharm. World Sci. 2009, 31, 670–676. [Google Scholar] [CrossRef] [PubMed]
- Bascom, C.S.; Rosenthal, M.M.; Houle, S.K.D. Are pharmacists ready for a greater role in travel health? An evaluation of the knowledge and confidence in providing travel health advice of pharmacists practicing in a community pharmacy chain in Alberta, Canada. J. Travel Med. 2015, 22, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Amery, J.; Lapwood, S. A study into the educational needs of children’s hospice doctors: A descriptive quantitative and qualitative survey. Palliat. Med. 2004, 18, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Awad, N.I.; Bridgeman, M.B. Continuing-education program planning: Tips for assessing staff educational needs. Am. J. Health Syst. Pharm. 2014, 71, 1616–1619. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Johnson, T.P.; Wislar, J.S. Response rates and nonresponse errors in surveys. JAMA 2012, 307, 1805–1806. [Google Scholar] [CrossRef] [PubMed]
- Dillman, D. Mail and Internet Surverys: The Tailored Design Method, 2nd ed.; John Wiley & Sons: Hoboken, NJ, USA, 2007. [Google Scholar]
- Medway, R.L.; Fulton, J. When More Gets You Less: A Meta-Analysis of the Effect of Concurrent Web Options on Mail Survey Response Rates. Public Opin. Q. 2012, 76, 733–746. [Google Scholar] [CrossRef]
- Koo, M.; Skinner, H. Challenges of internet recruitment: A case study with disappointing results. J. Med. Int. Res. 2005, 7, e6. [Google Scholar] [CrossRef] [PubMed]
- Jain, C.L.; Wyatt, C.M.; Burke, R.; Sepkowitz, K.; Begier, E.M. Knowledge of the Centers for Disease Control and Prevention’s 2006 routine HIV testing recommendations among New York City internal medicine residents. AIDS Patient Care STDS 2009, 23, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Kramer, M.; Schmalenberg, C.; Brewer, B.B.; Verran, J.A.; Keller-Unger, J. Accurate assessment of clinical nurses’ work environments: Response rate needed. Res. Nurs. Health 2009, 32, 229–240. [Google Scholar] [CrossRef] [PubMed]
- Torghele, K.; Buyum, A.; Dubruiel, N.; Augustine, J.; Houlihan, C.; Alperin, M.; Miner, K.R. Logic Model Use in Developing a Survey Instrument for Program Evaluation: Emergency Preparedness Summits for Schools of Nursing in Georgia. Public Health Nurs. 2007, 24, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Petrovčič, A.; Petrič, G.; Lozar Manfreda, K. The effect of email invitation elements on response rate in a web survey within an online community. Comput. Hum. Behav. 2016, 56, 320–329. [Google Scholar] [CrossRef]
- Zillmann, D.; Schmitz, A.; Skopek, J.; Blossfeld, H.-P. Survey topic and unit nonresponse. Qual. Quant. 2014, 48, 2069–2088. [Google Scholar] [CrossRef]
- De Valck, K.D.; Langerak, F.; Verhoef, P.C.; Verlegh, P.W.J. Satisfaction with Virtual Communities of Interest: Effect on Members’ Visit Frequency*. Br. J. Manag. 2007, 18, 241–256. [Google Scholar] [CrossRef]
- Isenor, J.E.; Minard, L.V.; Stewart, S.A.; Curran, J.A.; Deal, H.; Rodrigues, G.; Sketris, I.S. Identification of the relationship between barriers and facilitators of pharmacist prescribing and self-reported prescribing activity using the theoretical domains framework. Res. Soc. Adm. Pharm. 2017. [Google Scholar] [CrossRef] [PubMed]
- Guirguis, L.M.; Hughes, C.A.; Makowsky, M.J.; Sadowski, C.A.; Schindel, T.J.; Yuksel, N.; Faruquee, C.F. Development and validation of a survey instrument to measure factors that influence pharmacist adoption of prescribing in Alberta, Canada. Pharm. Pract. 2018, 16, 1068. [Google Scholar] [CrossRef] [PubMed]
- Tsuyuki, R.T.; Beahm, N.P.; Okada, H.; Al Hamarneh, Y.N. Pharmacists as accessible primary health care providers: Review of the evidence. Can. Pharm. J. 2018, 151, 4–5. [Google Scholar] [CrossRef] [PubMed]
- Kosar, L.; Hu, N.; Lix, L.M.; Shevchuk, Y.; Teare, G.F.; Champagne, A.; Blackburn, D.F. Uptake of the Medication Assessment Program in Saskatchewan: Tracking claims during the first year. Can. Pharm. J. 2018, 151, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Weglicki, R.S.; Reynolds, J.; Rivers, P.H. Continuing professional development needs of nursing and allied health professionals with responsibility for prescribing. Nurse Educ. Today 2015, 35, 227–231. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, M.M.; Holmes, E.R. The Professional Culture of Community Pharmacy and the Provision of MTM Services. Pharmacy 2018, 6. [Google Scholar] [CrossRef] [PubMed]
- Henkel, P.J.; Marvanova, M. Maintaining Vitality: Pharmacists’ Continuing Professional Education Decision-Making in the Upper Midwest. Pharmacy 2018, 6. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Overall (n = 162) | Self-Study Completed (n = 115) | Self-Study in Progress (n = 9) | Self-study not Started but Plan to Initiate (n = 23) | No Plans to Start Self-Study (n = 15) | |
|---|---|---|---|---|---|
| Number of years practicing as pharmacist | |||||
| <6 years | 36 (22.2%) | 29 (25.2%) | 1 (11.1%) | 5 (21.7%) | 1 (6.7%) |
| 6–15 years | 52 (32.1%) | 33 (28.7%) | 2 (22.2%) | 7 (30.4%) | 10 (66.7%) |
| >15 years | 74 (45.7%) | 53 (46.1%) | 6 (66.7%) | 11 (47.8%) | 4 (26.7%) |
| Employment status | |||||
| Full time | 122 (75.3%) | 94 (81.7%) | 5 (55.6%) | 14 (60.9%) | 9 (60.0%) |
| Part time | 27 (16.7%) | 16 (13.9%) | 3 (33.3%) | 4 (17.4%) | 4 (26.7%) |
| Casual or on leave | 12 (7.4%) | 4 (3.4%) | 1 (11.1%) | 5 (21.7%) | 2 (13.3%) |
| Primary area of employment | |||||
| Retail/community | 147 (90.7%) | 111 (96.5%) | 6 (66.7%) | 20 (87.0%) | 10 (66.7%) |
| Hospital | 8 (4.9%) | 1 (0.9%) | 1 (11.1%) | 1 (4.3%) | 5 (33.3%) |
| Government or academia | 3 (1.9%) | 2 (1.8%) | 1 (11.1%) | 0 | 0 |
| Other | 3 (1.9%) | 1 (0.9%) | 1 (11.1%) | 1 (4.3%) | 0 |
| Location of employment by health region | |||||
| Winnipeg (Churchill) | 85 (52.5%) | 55 (47.8%) | 6 (66.7%) | 12 (52.2%) | 1 (6.7%) |
| Interlake Eastern | 16 (9.9%) | 12 (10.4%) | 1 (11.1%) | 3 (13.0%) | 0 |
| Northern | 5 (3.1%) | 3 (2.6%) | 0 | 1 (4.3%) | 1 (6.7%) |
| Prairie Mountain Health | 25 (15.4%) | 19 (16.5%) | 1 (11.1%) | 4 (17.4%) | 1 (6.7%) |
| Southern Health-Sante Sud | 22 (13.6%) | 20 (17.4%) | 0 | 2 (8.7%) | 12 (80.0%) |
| Self-Study Completed (n = 115) | Self-Study in Progress/Plan to Initiate (n = 32) | No Plans to Start Self-Study (n = 15) | |
|---|---|---|---|
| Encountered barriers in applying assessment and prescribing skills for minor ailments | |||
| Yes | 96 (83.5%) | -- | -- |
| No | 19 (16.5%) | -- | -- |
| Anticipated encountering barriers in applying assessment and prescribing skills for minor ailments | |||
| Yes | -- | 20 (62.5%) | -- |
| No | -- | 12 (37.5%) | -- |
| Identified barriers to taking on expanded role of applying assessment and prescribing skills for minor ailments | |||
| Yes | -- | -- | 14 (93.3%) |
| No | -- | -- | 1 (0.06%) |
| Specific barriers identified (n, %) | |||
| Lack of sufficient revenue attached to expanded role | 68 (26.2%) | 14 (29.8%) | 10 (66.7%) |
| Lack of training in expanded role | 11 (4.2%) | 1 (2.1%) | -- |
| Lack of confidence in skills | 25 (9.6%) | 4 (8.5%) | 0 |
| Clinical uncertainty | 12 (4.6%) | 0 | 1 (6.7%) |
| Lack of time at work | 61 (23.5%) | 15 (31.9%) | 8 (53.3%) |
| Lack of performance feedback | 2 (0.8%) | 2 (4.3%) | -- |
| Lack of motivation to take on new responsibilities | 10 (3.8%) | 3 (6.4%) | 7 (46.7%) |
| Lack of support from management | 14 (5.4%) | 4 (8.5%) | 4 (26.7%) |
| Lack of patients presenting with minor ailments | 31 (11.9%) | 2 (4.3%) | -- |
| Lack of satisfaction with current training and certification program | -- | -- | 2 (13.3%) |
| Irrelevant to practice | -- | -- | 4 (26.7%) |
| Other | 26 (10.0%) | 2 (4.3%) | 2 (13.3%) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shearer, B.; Ng, S.; Dunford, D.; Kuo, I.F. Training Needs of Manitoba Pharmacists to Increase Application of Assessment and Prescribing for Minor Ailments into Practice: A Qualitative and Quantitative Survey. Pharmacy 2018, 6, 82. https://doi.org/10.3390/pharmacy6030082
Shearer B, Ng S, Dunford D, Kuo IF. Training Needs of Manitoba Pharmacists to Increase Application of Assessment and Prescribing for Minor Ailments into Practice: A Qualitative and Quantitative Survey. Pharmacy. 2018; 6(3):82. https://doi.org/10.3390/pharmacy6030082
Chicago/Turabian StyleShearer, Brenna, Sheila Ng, Drena Dunford, and I Fan Kuo. 2018. "Training Needs of Manitoba Pharmacists to Increase Application of Assessment and Prescribing for Minor Ailments into Practice: A Qualitative and Quantitative Survey" Pharmacy 6, no. 3: 82. https://doi.org/10.3390/pharmacy6030082
APA StyleShearer, B., Ng, S., Dunford, D., & Kuo, I. F. (2018). Training Needs of Manitoba Pharmacists to Increase Application of Assessment and Prescribing for Minor Ailments into Practice: A Qualitative and Quantitative Survey. Pharmacy, 6(3), 82. https://doi.org/10.3390/pharmacy6030082